

Penis & scrotum
Dysplasia / carcinoma in situ
Penile intraepithelial neoplasia (PeIN)
Editorial Board Member: Debra L. Zynger, M.D.
Deputy Editor-in-Chief: Maria Tretiakova, M.D., Ph.D.


Last author update: 6 September 2022
Last staff update: 12 July 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Penile intraepithelial neoplasia
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Positive stains | Negative stains | Molecular / cytogenetics description | Molecular / cytogenetics images | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Sanchez DF, Cubilla AL. Penile intraepithelial neoplasia (PeIN). PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/penscrotumPeIN.html. Accessed April 17th, 2024.
Definition / general
- Intraepithelial neoplastic proliferation with variable degree of dysplasia, keratinization and nuclear atypia
- Penile intraepithelial neoplasia (PeIN) is classified as HPV related / dependent or HPV unrelated / independent, similar to invasive carcinomas (Am J Pathol 2001;159:1211, Semin Diagn Pathol 2015;32:198)
- Considered a precursor of penile invasive carcinoma
Essential features
- Classified as HPV related / dependent or HPV unrelated / independent
- May occur in any of the penile mucosal epithelial areas, most commonly in the glans and foreskin
- Differentiated PeIN is related to lichen sclerosus
- HPV16 is the most frequent genotype associated with PeIN
Terminology
- Synonyms are as follows: erythroplasia of Queyrat, Bowen disease, carcinoma in situ (CIS), squamous intraepithelial lesion, dysplasia (mild, moderate and severe) and bowenoid papulosis
- PeIN is the recommended nomenclature for penile precancerous lesions (Epstein: Tumors of the Prostate Gland, Seminal Vesicles, and Scrotum, 2020, Eur Urol 2016;70:93)
- PeIN refers to squamous lesions and excludes Paget disease, urothelial carcinoma in situ and malignant melanoma in situ
- Some authors stratify PeIN into grades I, II and III (Int J Urol 2019;26:353)
ICD coding
Epidemiology
- There is geographic variation in the presentation of PeIN (Hum Pathol 2012;43:190)
- Differentiated PeIN is more commonly diagnosed in countries with a high frequency of penile cancer
- HPV related PeIN is more common in countries with a low frequency of penile cancer
- In countries with a high frequency of invasive penile carcinomas (2 - 5 cases/100,000), PeIN is rarely diagnosed as a solitary lesion (Hum Pathol 2012;43:190)
- In countries in which invasive penile carcinomas are rare (≤ 1 case/100,000), PeIN is the most common penile neoplasia at clinical diagnosis
- PeIN affects patients younger than those with invasive cancers (Hum Pathol 2012;43:1020)
- Mean age is ~58 years old
- HPV related PeIN preferentially affects younger patients
- Predisposing factors: HIV / immunosuppression, lack of or delayed circumcision, inflammatory / irritative conditions (balanitis, buried penis, phimosis) (Mod Pathol 2022;35:1101)
Sites
- PeIN is most commonly found in the glans and foreskin (Histopathology 2011;58:925, Int J Urol 2019;26:353)
- Differentiated PeIN, non-HPV related, preferentially involves the foreskin inner mucosal epithelium
- ~33% of cases with PeIN are multicentric, especially the HPV related types
- PeIN may occur in the skin of the shaft of the penis
Etiology
- Undifferentiated: high risk HPV
- Differentiated: lichen sclerosus
Clinical features
- Lesions can be subclassified according to morphological features and HPV genotypes present (Am J Surg Pathol 2017;41:820)
- Non-HPV related PeIN / differentiated
- Represented by differentiated PeIN
- Squamous or simplex PeIN are synonyms
- Putative precursors of non-HPV related keratinizing squamous cell invasive carcinomas, the majority of penile cancers
- Most cases in association with invasive carcinoma and rarely as a solitary lesion
- Difficult to diagnose and underrecognized by pathologists due to only subtle histologic changes
- Foreskin is a preferential site but the glans is also involved
- Frequently associated with lichen sclerosus
- HPV related PeIN / undifferentiated
- Subclassified in basaloid, warty and warty basaloid subtypes (Epstein: Tumors of the Prostate Gland, Seminal Vesicles, and Scrotum, 2020, Eur Urol 2016;70:93)
- Bowen disease, CIS, high grade PeIN are synonyms
- In young males with multicentric lesions, it has been referred to as bowenoid papulosis (Cancer 1978;42:1890)
- More frequently multicentric than differentiated PeIN
- Putative precursors of HPV related basaloid and condylomatous (warty) invasive carcinomas or mixtures, ~33% of penile cancers (Am J Surg Pathol 2017;41:820)
- Straightforward diagnosis and well recognized by pathologists
- Glans is a preferential site but the foreskin, coronal sulcus and shaft may also be involved
- HPV16, 6 and 11 are the most commonly found genotypes (Lancet Oncol 2019;20:145, Int J Surg Pathol 2020;28:265)
- HIV positive patients are more susceptible to develop HPV related PeIN (AIDS 2006;20:1201)
- Mixed PeIN
- Coexisting non-HPV and HPV related PeIN in the same specimen
- Rarely found as solitary lesions
- Multicentric lesions may be in collision, next to each other or in separate foci
- Pathological features and HPV composition are similar in PeIN and invasive carcinomas (Int J Surg Pathol 2020;28:265)
- HPV is usually negative in differentiated PeIN and the corresponding invasive non-HPV related squamous cell carcinoma
- HPV is usually positive in PeIN and the corresponding invasive basaloid or warty invasive carcinoma
- Morphological similarity and HPV genotype composition indicate a causal relation of PeIN and corresponding invasive carcinoma
Diagnosis
- Dermatoscopy
- Biopsy
- Excision
Prognostic factors
- Frequent recurrence (48%) (Mod Pathol 2022;35:1101)
- Low rate of progression to invasive carcinoma (2%) (Mod Pathol 2022;35:1101)
Case reports
- 51 year old man with pruritic lesions on the penis, scrotum, pubis and gluteal region (JAAD Case Rep 2017;3:542)
- 68 year old man presented with phimosis (Open Access Maced J Med Sci 2017;6:61)
- 79 year old man with penile lesion involving the distal urethra (SAGE Open Med Case Rep 2020;8:2050313X20918985)
Treatment
- Local excision (Mohs surgery, glans resurfacing, glansectomy) is the most frequent approach (BJU Int 2022;129:752, Semin Diagn Pathol 2015;32:232)
- Laser therapy is associated with higher complication and recurrence rate (BJU Int 2022;129:752, Eur Urol Focus 2021 May 11 [Epub ahead of print])
- Topical agents (5-fluorouracil, imiquimod 5%)
- Local destructive methods (photodynamic therapy, cryotherapy, curettage and electrocautery)
Clinical images
AFIP images
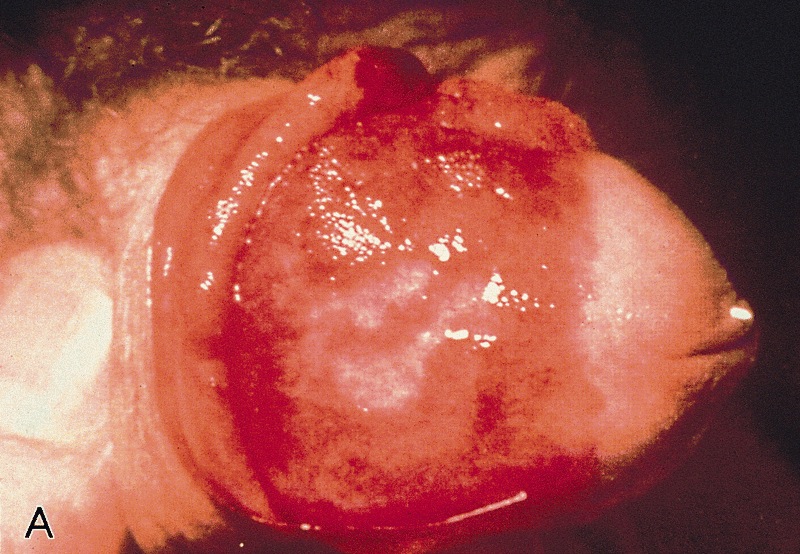
Erythroplasia of Queyrat: moist red lesion involving glans

Bowen disease
Images hosted on other servers:

Erythematous lesion in the glans


Erythroplasia of Queyrat

PeIN with lichen sclerosus

PeIN in multiple compartments
Gross description
- Non-HPV related PeIN / differentiated
- Solitary white or pink macule, plaque or slightly elevated geographical lesion
- Affects the foreskin and glans and rarely the shaft
- HPV related PeIN
- Lesions are flat or slightly elevated or papular, velvety, erythematous, dark brown or black
- Warty PeINs are granular or villous
- Borders are irregular or sharply delineated
- References: Epstein: Tumors of the Prostate Gland, Seminal Vesicles, Penis, and Scrotum, 2020, Eur Urol 2016;70:93
Microscopic (histologic) description
- Non-HPV related PeIN / differentiated
- Common features are hyperkeratosis, parakeratosis, hypergranulosis, acanthosis, elongation of rete ridges, abnormal squamous maturation and squamous cell atypia
- Prominent intercellular edematous bridges and intraepithelial keratinization
- Some histological heterogeneity: hyperplasia-like, classic and pleomorphic features
- Most common or classic feature is a keratinized maturing lesion with obvious atypical cells involving 2 or 3 basal epithelial layers
- Less common are the hyperplasia-like features, with acanthotic thickening of the epithelium and subtle basal cell atypia
- In the pleomorphic variant, there are anaplastic cells involving most of the epithelial thickness but with evident maturation or cellular keratinization
- Grading system if used can classify as follows: hyperplasia-like as grade 1, classic as grade 2, pleomorphic as grade 3
- Basaloid PeIN
- Most frequent subtype
- Uni or multicentric
- Usually, flat lesions with a broad or undulating base
- Occasionally, papillary lesions simulating urothelial tumors
- Monotonous uniform small anaplastic basaloid cell population
- Replace the full epithelial thickness
- Superficial hyper and parakeratosis often with some koilocytes is typical
- Rarely, cells are larger, spindly or pleomorphic
- High nuclear cytoplasmic ratio
- Numerous mitoses may be noted
- Starry sky pattern is not uncommon
- Warty PeIN
- Presentation as a solitary lesion is unusual (Am J Surg Pathol 2017;41:820)
- Most commonly, it is part of a multicentric lesion
- Associated with invasive warty or basaloid carcinomas
- Squamous maturing lesion
- Striking micropapillary spiking features
- Surface shows hyper and parakeratosis
- Hallmark is atypical superficial or deep pleomorphic koilocytosis
- Multinucleation, nuclei with irregular contours, perinuclear halo and dyskeratosis are common
- Warty basaloid PeIN
- Warty cells and basaloid cells in about equal proportions
- Unifocal or multicentric lesions
- May be associated with invasive basaloid or warty carcinomas
- Hyper and parakeratosis, papillary or spiking features at the upper half
- Upper half is composed of clear warty-like cells
- Lower half is composed of small, anaplastic basaloid type cells
Microscopic (histologic) images
Contributed by Alcides Chaux, M.D. and Antonio Cubilla, M.D.

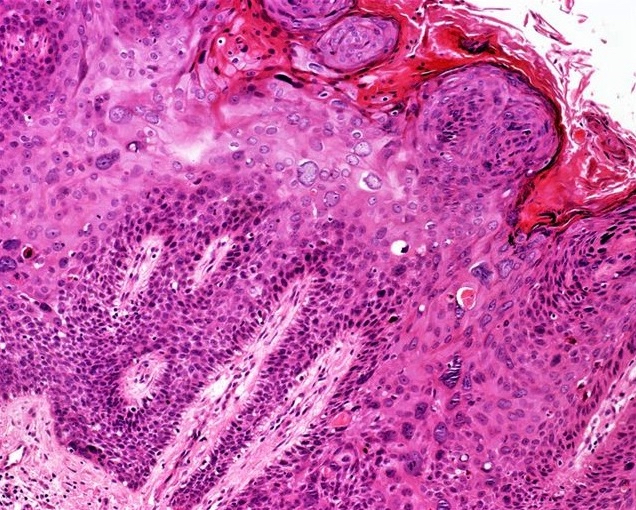
Squamous cell atypia
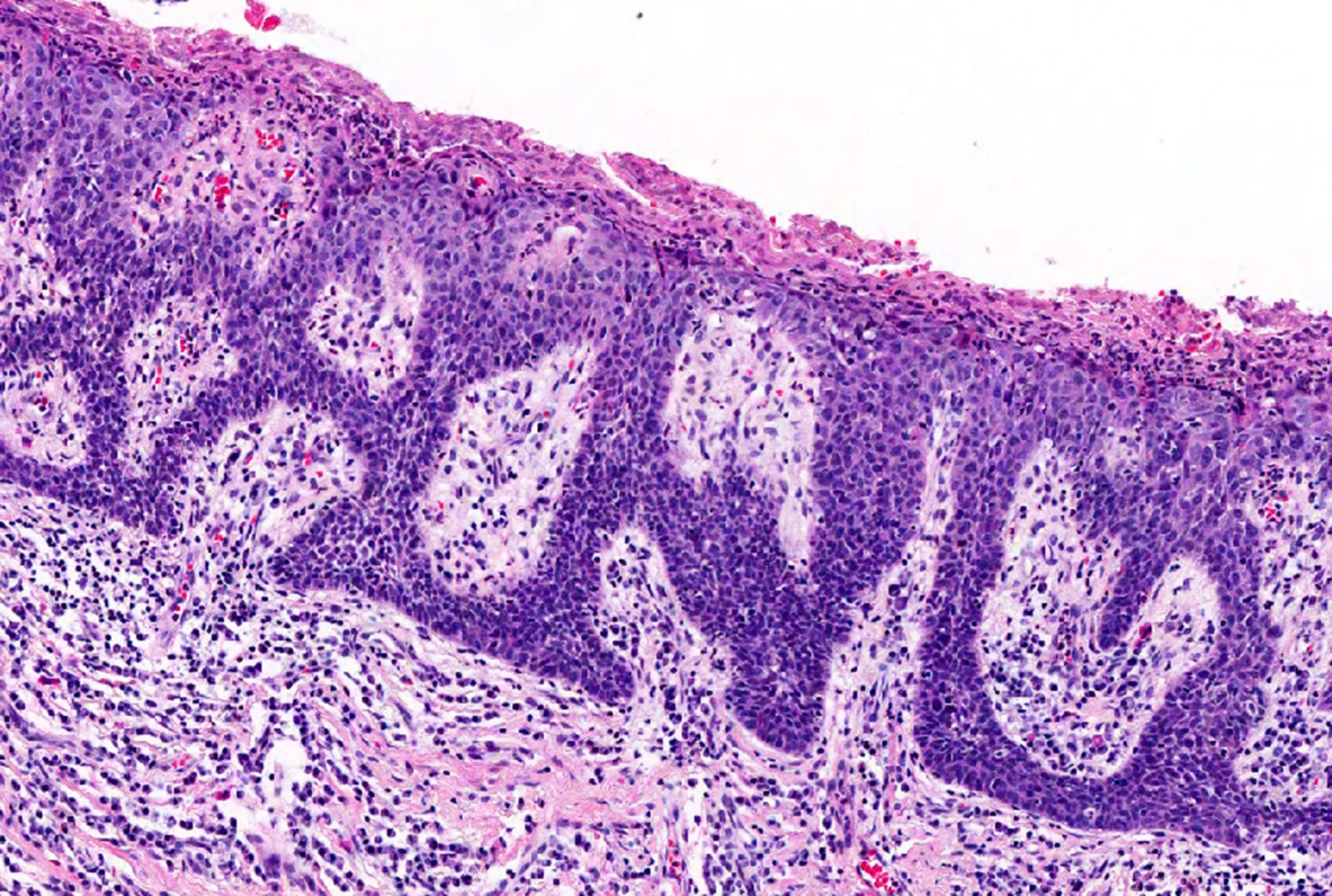
Small basaloid cells

Basaloid nonkeratinized cells
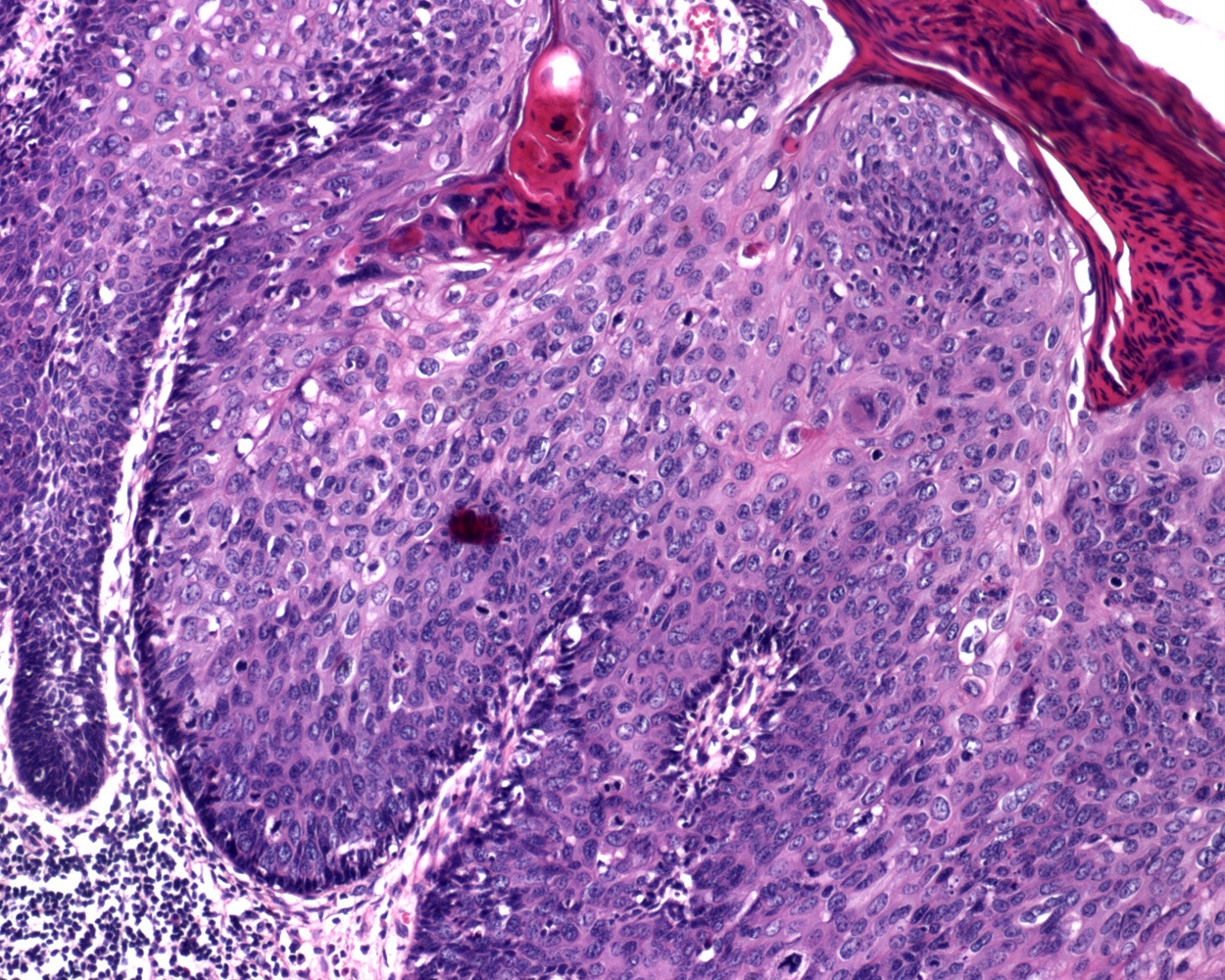
Small blue cells and koilocytes
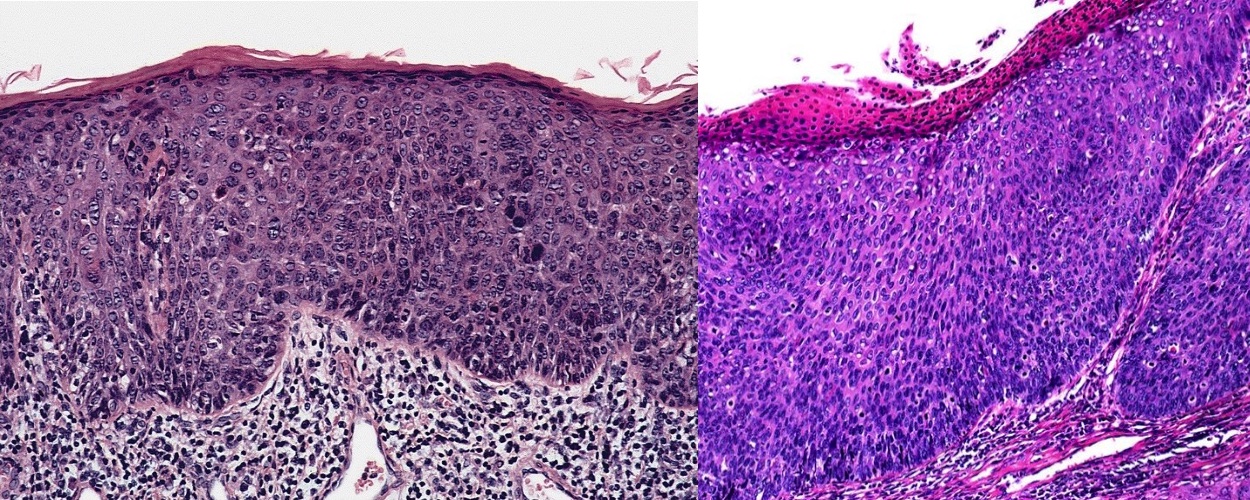
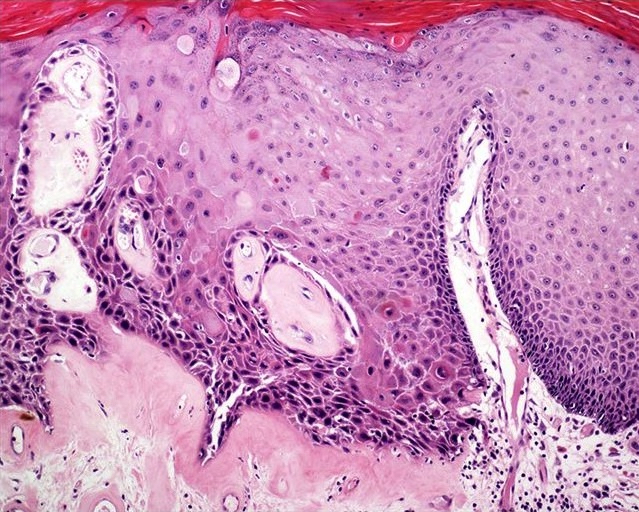
Basaloid type
Warty type
Atypical lichen sclerosus

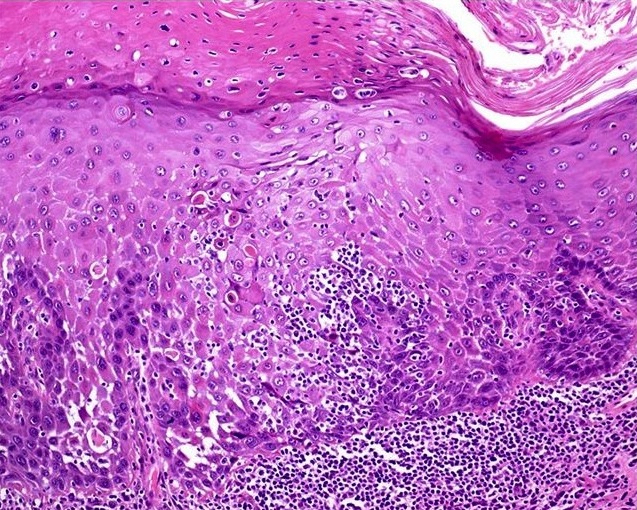
Differentiated type
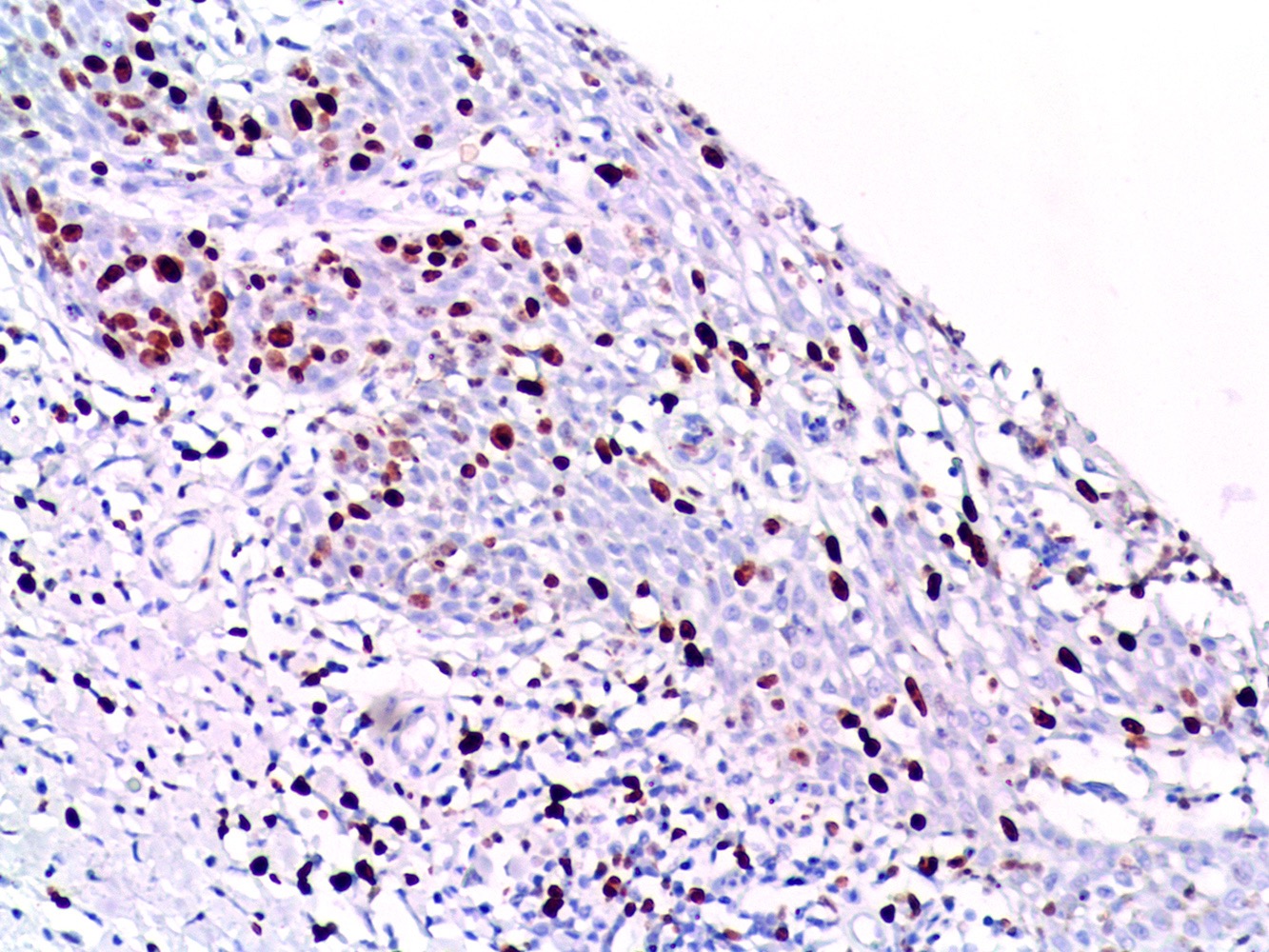
Ki67 positivity


Strong en bloc cytoplasmic and nuclear p16 immunostaining
Virtual slides
Images hosted on other servers:

Basaloid PeIN
Positive stains
- Non-HPV related PeIN / differentiated
- HPV related PeIN / undifferentiated
- Ki67: positive in most cells, full thickness
- p16: 99% positive, en bloc for basaloid PeIN and ≤ 50% of epithelial thickness in warty basaloid and warty PeIN (Am J Surg Pathol 2010;34:385, Mod Pathol 2022;35:1101)
Negative stains
- Non-HPV related PeIN / differentiated
Molecular / cytogenetics description
- HPV detection by PCR or ISH is negative in differentiated PeIN
- High risk HPV is detected in most HPV related PeIN
- HPV16 found in 67% of basaloid PeIN (Am J Surg Pathol 2017;41:820)
- Low risk HPV is present in 16% of warty PeIN (Am J Surg Pathol 2017;41:820)
- More variable HPV genotypic composition in warty PeIN
Molecular / cytogenetics images
Images hosted on other servers:

p16 and HPV ISH
Sample pathology report
- Penis, glans, biopsy:
- HPV related basaloid penile intraepithelial neoplasia (PeIN) (see comment)
- Comment: Lateral margins are involved by PeIN. High risk HPV ISH positive. p16 immunostaining is positive en bloc.
Differential diagnosis
- Non-HPV related / differentiated PeIN:
- Squamous hyperplasia:
- Condyloma acuminatum, flat type:
- HPV related PeIN (versus pleomorphic differentiated PeIN):
- HPV related PeIN:
- Urothelial carcinoma in situ (versus basaloid PeIN):
- p16 negative
- Condyloma acuminatum with atypical features (versus warty PeIN) (Int J Surg Pathol 2020;28:265):
- p16 negative
- May harbor low or high risk HPV
- Squamous cell carcinoma warty and basaloid types (versus warty and basaloid PeIN)
- Urothelial carcinoma in situ (versus basaloid PeIN):
Board review style question #1
A 55 year old man undergoes excision of a 1 cm, slow growing, erythematous plaque on the glans penis. At microscopy, the epithelium showed full thickness dysplasia, pleomorphic cells and mitoses. A representative photomicrograph is shown above. p16 immunostaining was strongly positive and Ki67 was positive in all cell layers. Which of the following statements is true regarding the depicted tumor?
- Differentiated PeIN hyperplasia-like is the diagnosis
- Distinguishing this lesion from squamous hyperplasia is difficult
- HPV16 is the most frequent genotype identified in the lesion
- It is the precursor of the most frequent invasive penile carcinoma subtype
- This neoplasia is usually related to lichen sclerosus
Board review style answer #1
C. HPV16 is the most frequent genotype identified in the lesion. This is HPV related PeIN. 67% of basaloid PeIN are positive for HPV16 genotype.
Comment Here
Reference: Penile intraepithelial neoplasia
Comment Here
Reference: Penile intraepithelial neoplasia
Board review style question #2
A 78 year old man undergoes excision of a 1 cm whitish plaque on the foreskin. At microscopy, the epithelium showed full thickness dysplasia, pleomorphic cells with ample cytoplasm and mitoses. Which of the following steps is needed for a final diagnosis?
- CD4 / CD8 for evaluating lichen sclerosus
- HMB45 immunostaining
- Ki67 for differentiating warty from basaloid PeIN
- In situ hybridization for high risk HPV
- p53 for ruling out squamous hyperplasia
Board review style answer #2
D. In situ hybridization for high risk HPV. In situ hybridization for high risk HPV is needed to confirm HPV related basaloid PeIN versus non-HPV related differentiated PeIN with pleomorphic features.
Comment Here
Reference: Penile intraepithelial neoplasia
Comment Here
Reference: Penile intraepithelial neoplasia
