
Prostate gland & seminal vesicles
Nonneoplastic
Adenosis / atypical adenomatous hyperplasia
Editorial Board Members: Maria Tretiakova, M.D., Ph.D., Bonnie Choy, M.D.

Last author update: 15 April 2021
Last staff update: 15 April 2024
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Adenosis
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Radiology description | Prognostic factors | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Magi-Galluzzi C. Adenosis / atypical adenomatous hyperplasia. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/prostateadenosis.html. Accessed April 18th, 2024.
Definition / general
- Well circumscribed, microscopic nodular proliferation of crowded, small to medium glands with pale to clear cytoplasm, a fragmented and discontinuous basal cell layer and minimal atypia; may be mistaken for low grade adenocarcinoma (Histopathology 2019;74:1036, Surg Pathol Clin 2008;1:1, J Urol 2012;188:2371)
- Found predominantly in the transition zone (1.6% of transurethral resection of the prostate [TURP], < 1% of core biopsies) in association with nodular hyperplasia (Int J Surg Pathol 2005;13:167, Surg Pathol Clin 2008;1:1)
- Frequently multifocal (Int J Surg Pathol 2005;13:167)
Essential features
- Benign lobular proliferation of small crowded glands
- Similar to prostatic adenocarcinoma; in adenosis, cells may show small or medium size nucleoli, crystalloids, intraluminal secretions, minimal infiltration and positive immunostaining for AMACR (racemase)
- In contrast to prostatic adenocarcinoma, in adenosis, glands have more pale cytoplasm, merge with adjacent benign glands, commonly have corpora amylacea (Am J Surg Pathol 1994;18:863, Surg Pathol Clin 2008;1:1)
- Basal cells can be identified on H&E slides or with immunohistochemistry for p63, cytokeratin 5/6 or HMWCK (Pathology 2013;45:251)
- AMACR (racemase) can be focally or diffusely expressed in up to 18% of cases of adenosis (Am J Surg Pathol 2002;26:921)
- Lack of ERG expression in adenosis supports the notion that it is not a precursor lesion of adenocarcinoma (Hum Pathol 2013;44:1895)
Terminology
- Atypical adenosis, atypical small acinar hyperplasia, atypical hyperplasia (Int J Surg Pathol 2005;13:167)
ICD coding
- ICD-10: N40.2 - nodular prostate without lower urinary tract symptoms
Epidemiology
- 2 - 20% of transurethral resections of the prostate, 1% of prostate needle biopsies
Sites
- More commonly in the transition zone of the prostate (Surg Pathol Clin 2008;1:1)
Pathophysiology
- Associated with benign prostatic hyperplasia
Clinical features
- Morphologic variant of benign crowded glands, a mimicker of low grade prostatic adenocarcinoma
- Does not have clinical implications
Diagnosis
- Detected on needle biopsy or transurethral resection
Radiology description
- Multiparametric magnetic resonance imaging (mpMRI) may be difficult to interpret because it shows overlapping features with low grade prostatic adenocarcinoma (Eur Radiol 2017;27:2095)
Prognostic factors
- Not a precursor lesion of prostatic adenocarcinoma (Hum Pathol 2013;44:1895)
- Comparative genomic hybridization and multiplex PCR did not find common alterations between adenosis and accompanying cancer foci and concluded that adenosis should not be considered as an obligate premalignant lesion (Int J Oncol 2005;26:267)
- Diffuse adenosis of the peripheral zone should be considered a risk factor for prostate cancer (Am J Surg Pathol 2008;32:1360)
Case reports
- 62 year old man with urinary obstruction and elevated serum PSA (Diagn Pathol 2008;3:34)
- 73 year old man with signs of urinary obstruction and elevated PSA (Rom J Morphol Embryol 2012;53:1093)
Treatment
- Treatment not needed
Microscopic (histologic) description
- Relatively well circumscribed proliferation of small, crowded, closely spaced acini merging with surrounding benign glands
- Lobular proliferation of small disorderly glands with an expansile or minimally infiltrative growth pattern
- Budding of small glands from larger, more obvious benign glands
- Occasional single cells or poorly formed glands are common; may represent tangential section of small glands
- Resembles low grade (Gleason score 3 + 3 = 6) prostatic adenocarcinoma (Am J Surg Pathol 1995;19:737, Rom J Morphol Embryol 2012;53:1093, Arch Pathol Lab Med 2010;134:427, Am J Surg Pathol 2019;43:361, Am J Surg Pathol 2005;29:874)
- Clear cytoplasm, usually normal sized nuclei, normochromasia and common corpora amylacea
- Occasionally, prominent nucleoli (13 - 15%) and mitotic figures (3 - 11%); rarely, blue tinged luminal mucinous secretions (3%) (Am J Surg Pathol 1994;18:863, Am J Surg Pathol 1995;19:737)
- Crystalloids can be present in 24 - 40% of cases (Am J Surg Pathol 1994;18:863, Am J Surg Pathol 1995;19:737)
- HMWCK labels the basal cells focally in a patchy fashion
- 3 dimensional renderings show network of interconnecting tubules with extensive branching, lacking obvious acinar organization (Histopathology 2019;74:1036)
Microscopic (histologic) images
Contributed by Cristina Magi-Galluzzi, M.D., Ph.D.
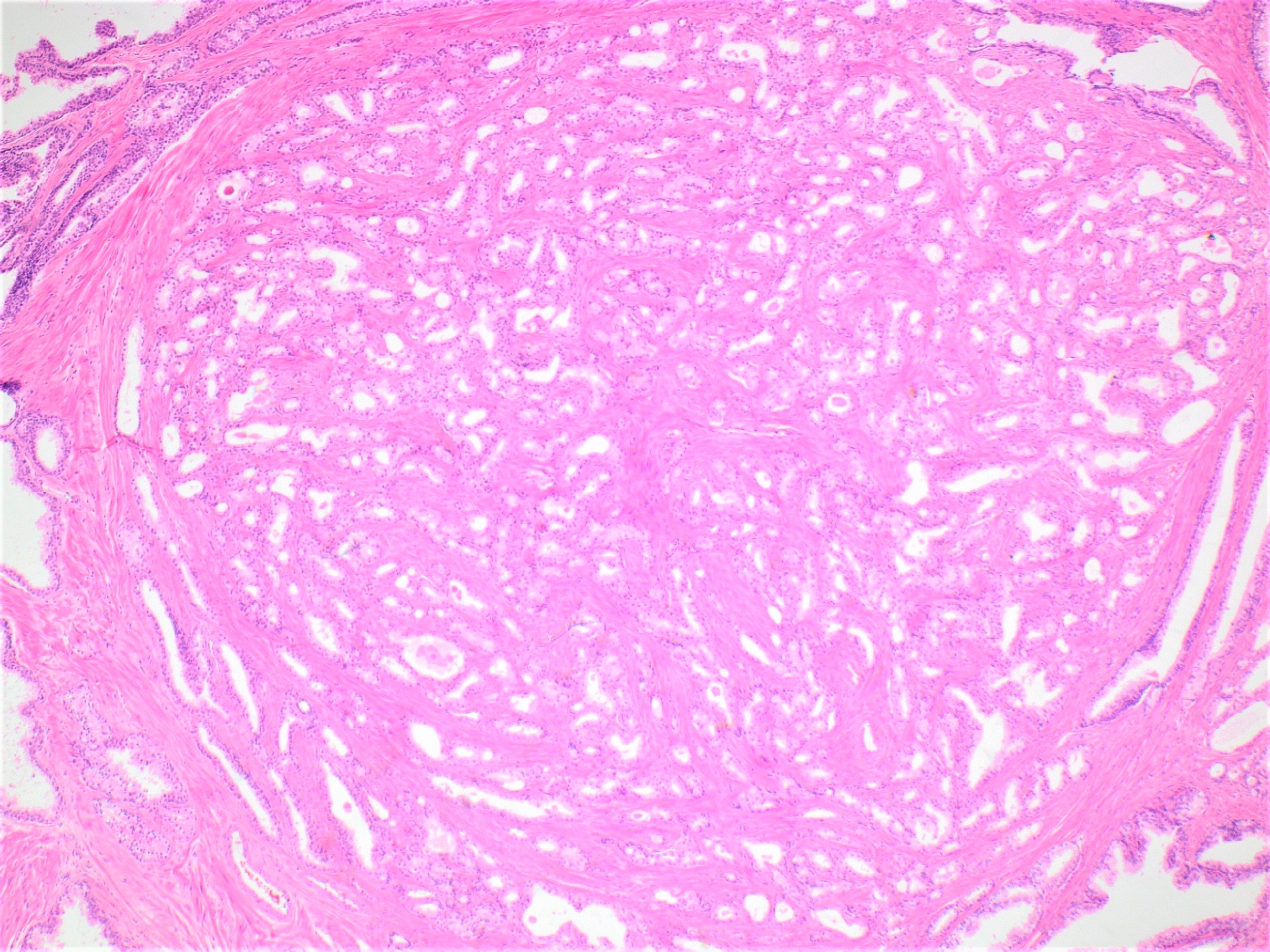
Well circumscribed nodule
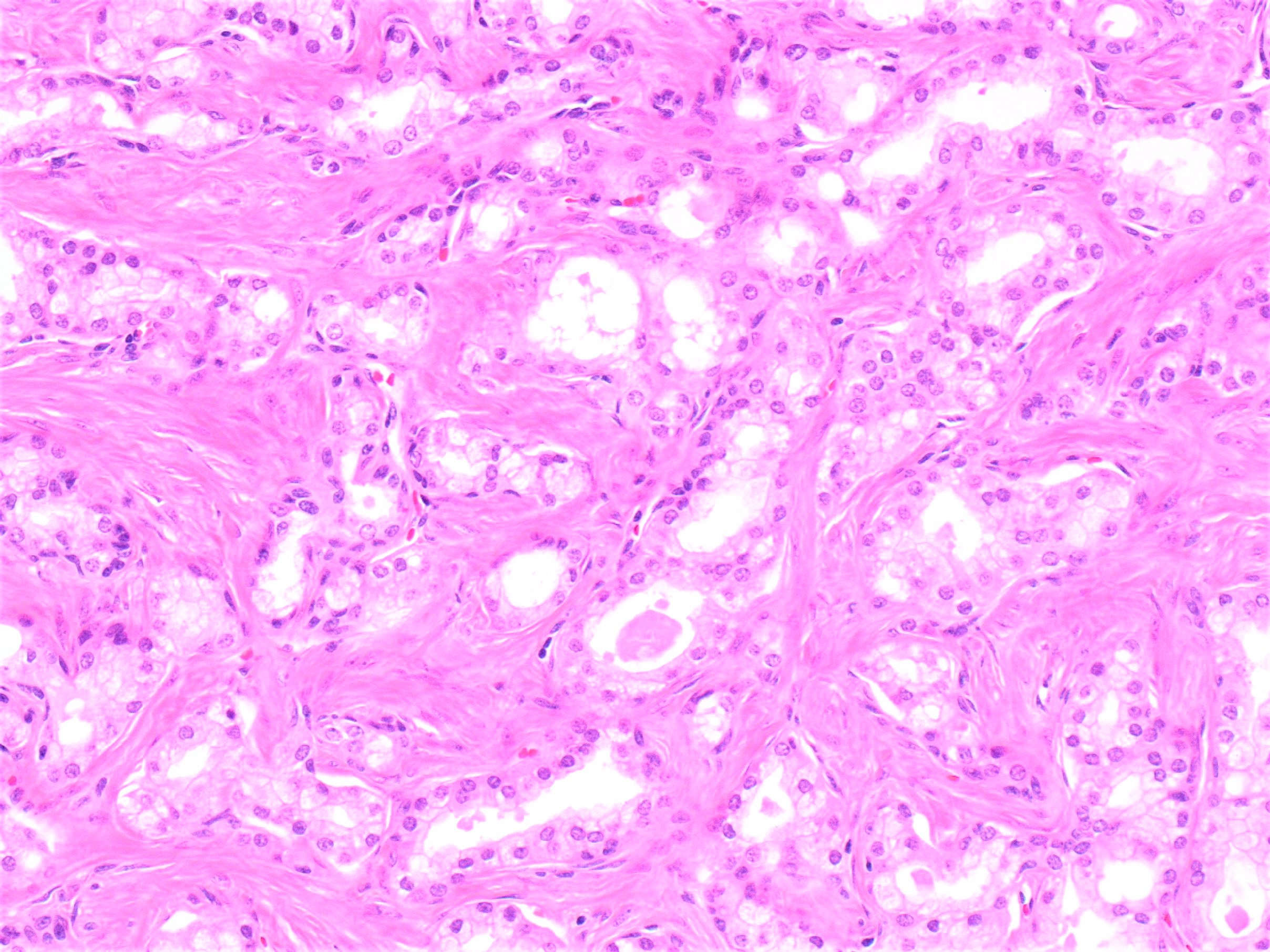
Mixed small and large acini
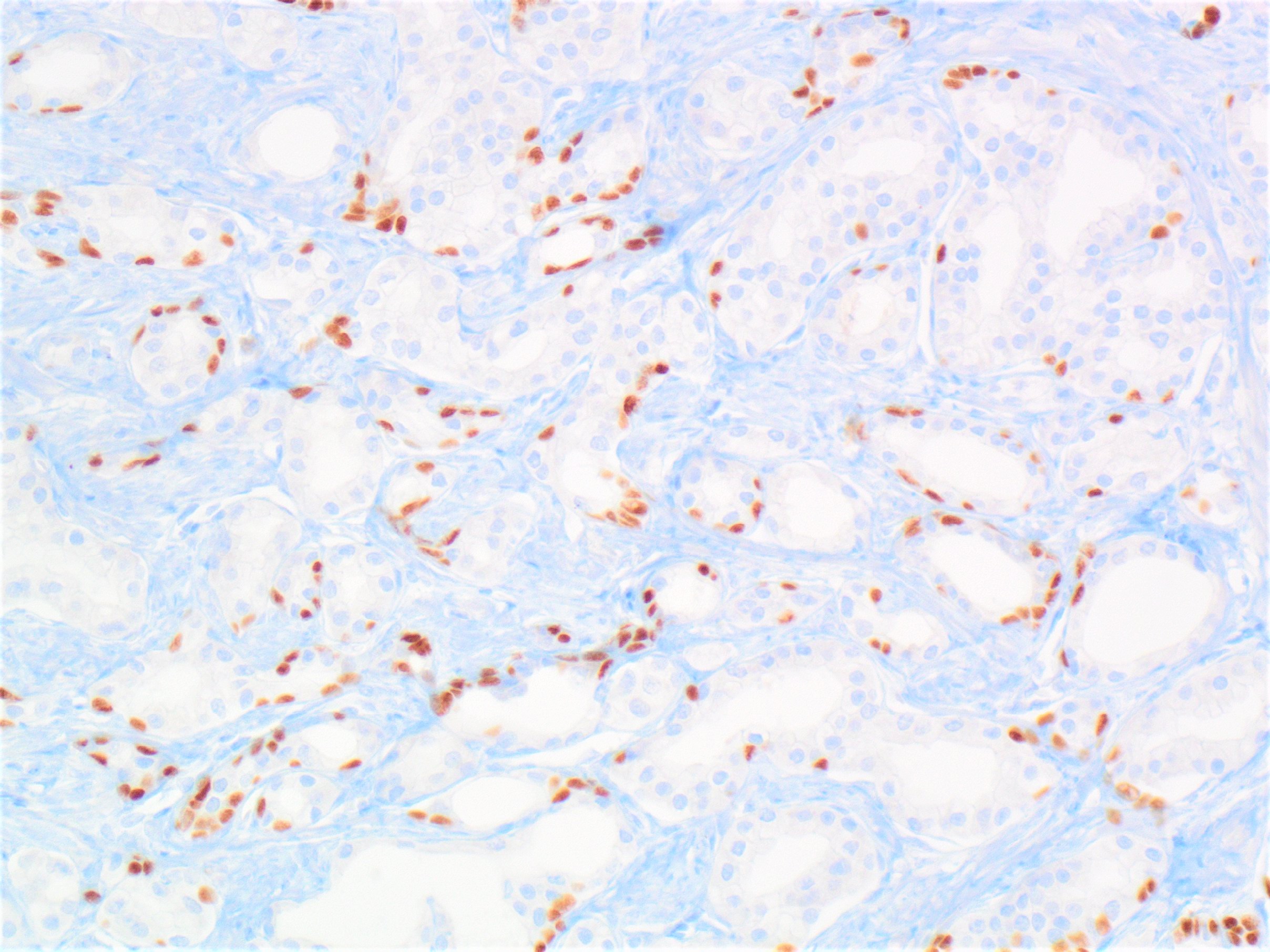
Basal cells
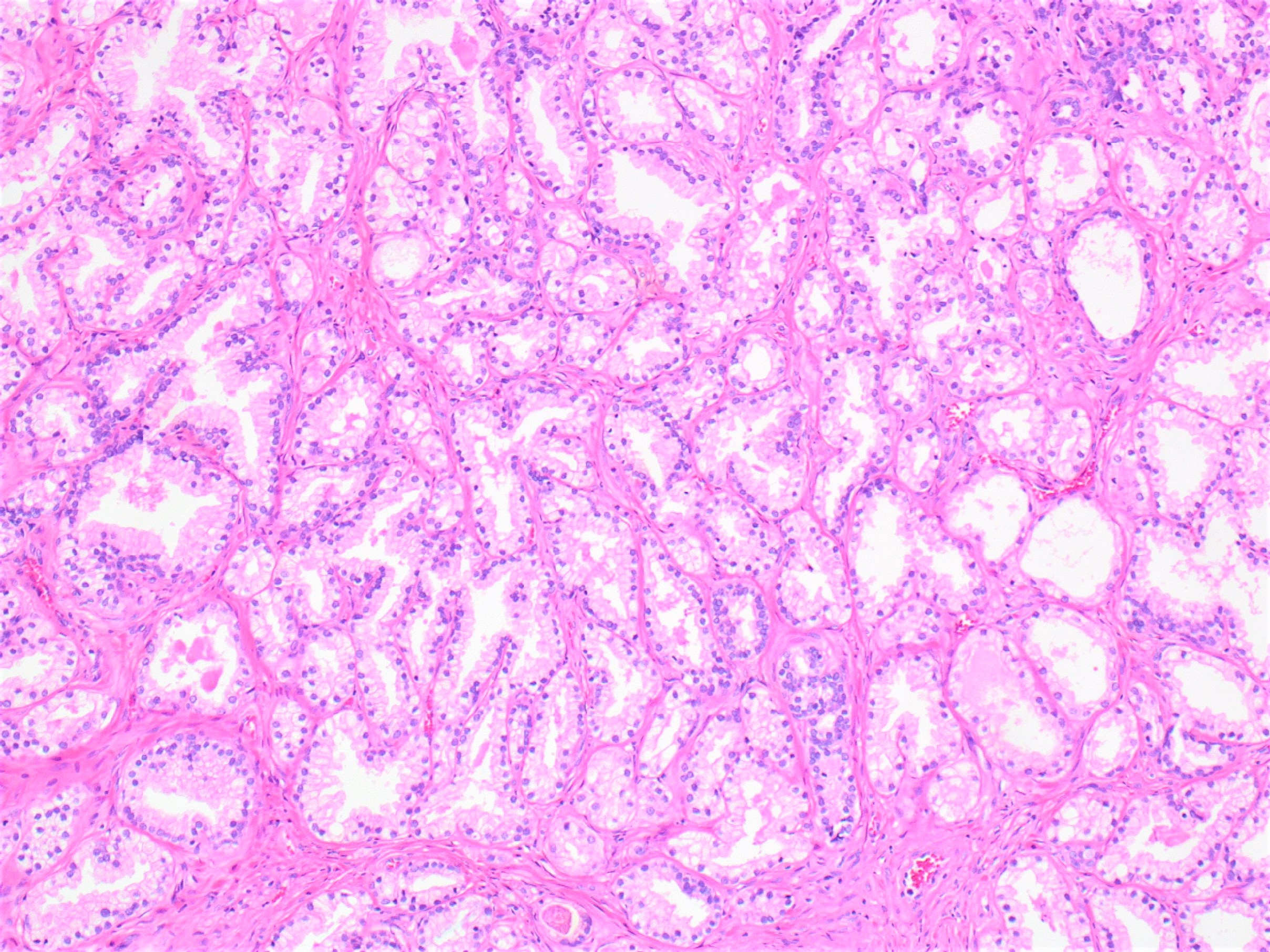
Crowded glands
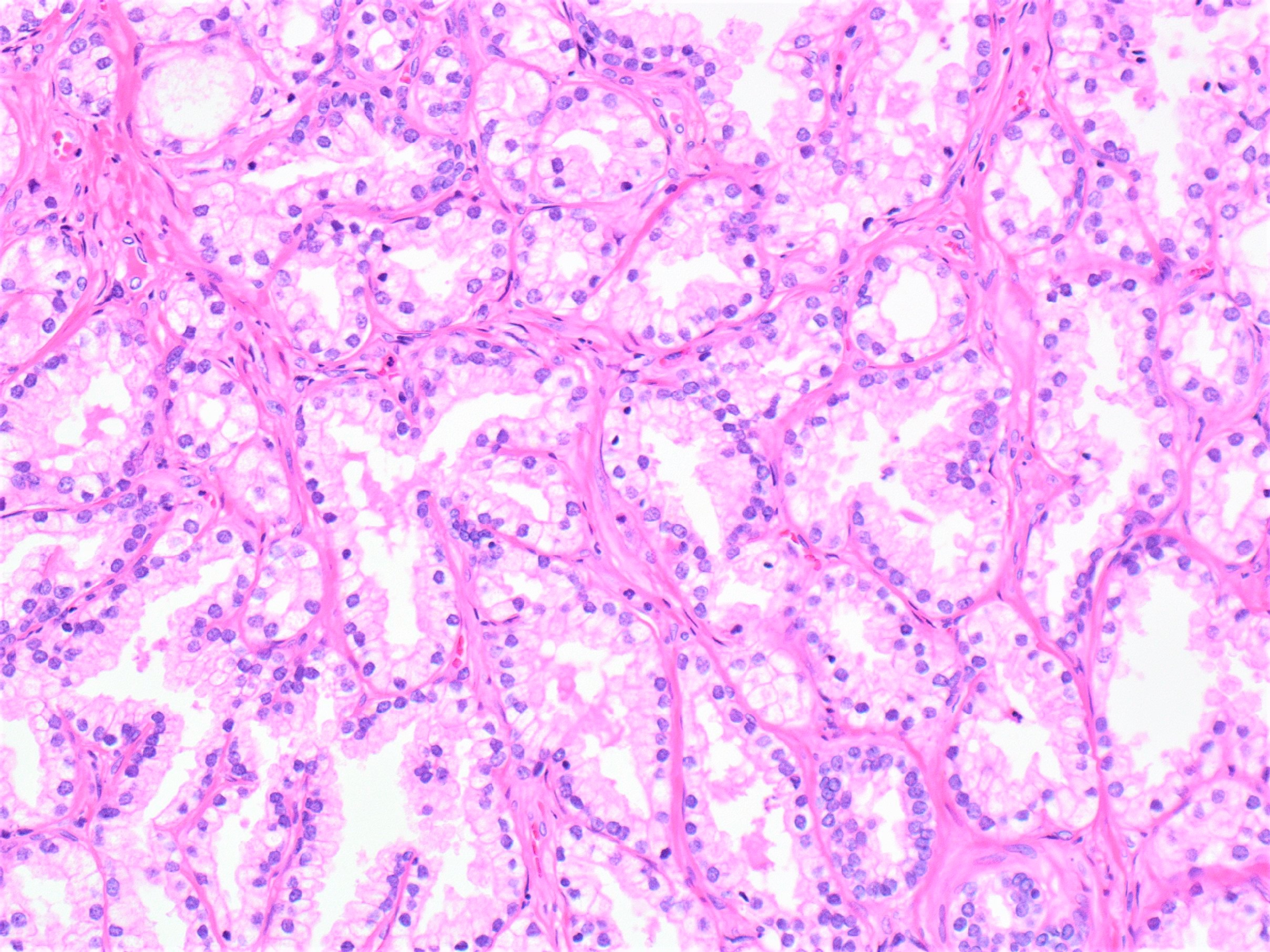
Bland nuclear features
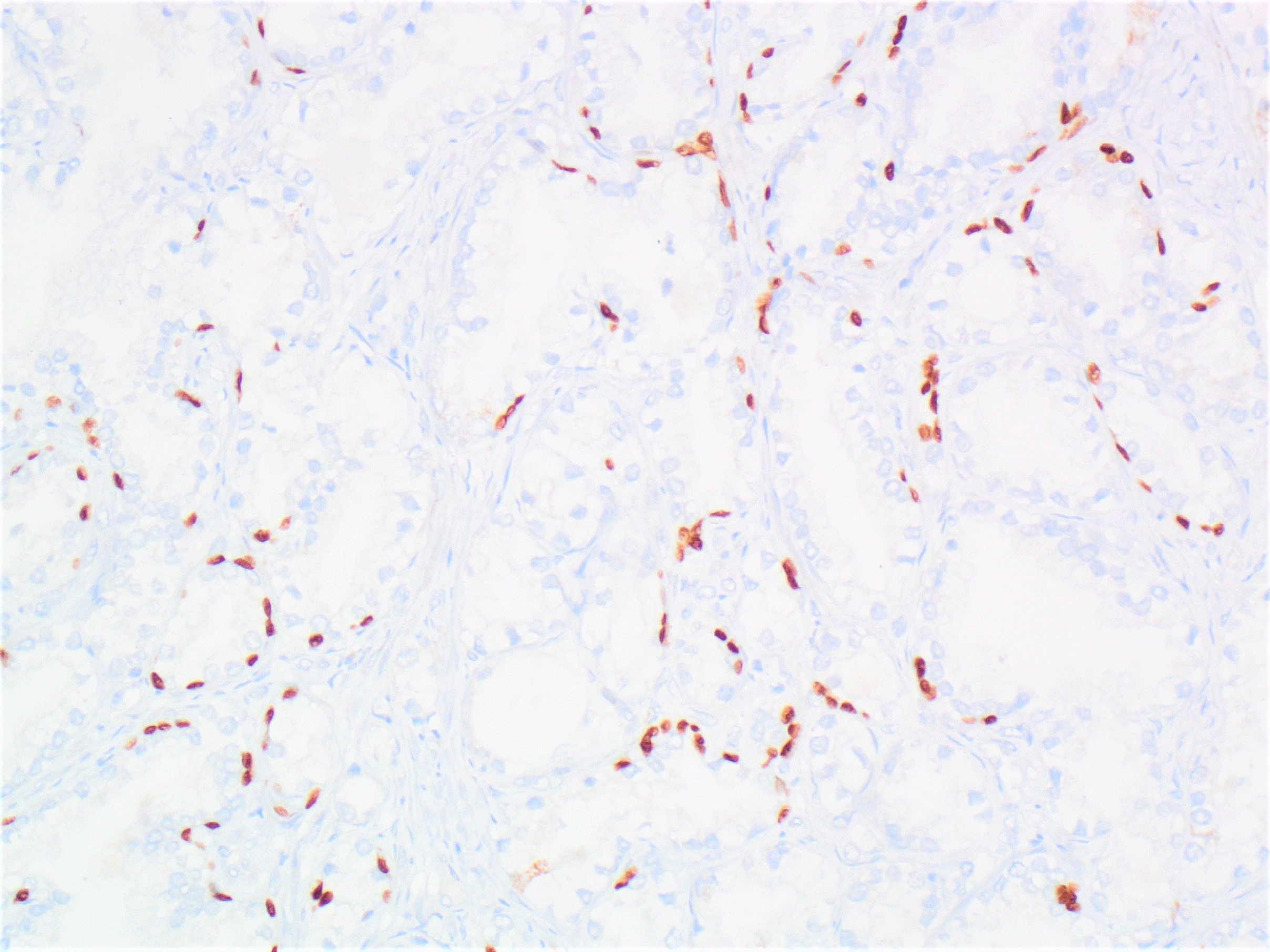
Fragmented basal cells
Positive stains
- Basal cell markers (p63, CK5/6 and HMWCK) are positive in a patchy fashion (discontinuous staining; mixture of glands with and without basal cell layer) (Pathology 2013;45:251)
Negative stains
- ERG (Hum Pathol 2013;44:1895)
- AMACR (racemase) can be focally or diffusely expressed in up to 18% of cases of adenosis (Am J Surg Pathol 2002;26:921)
Molecular / cytogenetics description
- 12% allelic imbalance, with loss within chromosome 8p11-12 (Am J Pathol 1999;155:967)
Sample pathology report
- It is not recommended to report adenosis
- Prostate, needle biopsy or transurethral resection:
- Benign prostatic tissue
Differential diagnosis
- Low grade (Gleason score 3 + 3 = 6, grade group 1) prostatic adenocarcinoma:
- Cytologic atypia, including prominent nucleoli and lack of basal cells
- Partial atrophy:
- Glands are partially atrophic with undulating luminal surface with papillary infolding; cytologic features are benign
Board review style question #1

Which of the following statements is true about the lesion depicted above?
- Atypical small acinar proliferation, favor benign
- Atypical small acinar proliferation, suspicious for malignancy
- Benign small acinar proliferation
- Prostatic carcinoma, Gleason score 3 + 3 = 6
Board review style answer #1
C. Benign small acinar proliferation. This is an example of adenosis (atypical adenomatous hyperplasia) with small acini lacking cytologic atypia and retaining basal cells.
Comment Here
Reference: Adenosis / atypical adenomatous hyperplasia
Comment Here
Reference: Adenosis / atypical adenomatous hyperplasia
Board review style question #2
Which of the following statements is true about adenosis?
- A fragmented and discontinuous basal cell layer is present
- AMACR is always negative
- It is a precursor lesion of prostatic adenocarcinoma
- More commonly in the peripheral zone
Board review style answer #2
A. A fragmented and discontinuous basal cell layer is present. Adenosis more commonly involves the transition zone; AMACR can be focally or diffusely expressed in up to 18% of cases of adenosis. Adenosis is not a precursor lesion of prostatic adenocarcinoma.
Comment Here
Reference: Adenosis / atypical adenomatous hyperplasia
Comment Here
Reference: Adenosis / atypical adenomatous hyperplasia
