
Prostate gland & seminal vesicles
Seminal vesicles
Amyloid
Author: Andres Matoso, M.D.

Last author update: 1 January 2017
Last staff update: 1 December 2023
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: prostatic amyloid
Table of Contents
Definition / general | Essential features | Epidemiology | Sites | Etiology | Pathophysiology | Clinical features | Diagnosis | Radiology description | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Electron microscopy description | Differential diagnosisCite this page: Matoso A. Amyloid. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/prostateamyloid.html. Accessed April 16th, 2024.
Definition / general
- Primary amyloidosis of the prostate is a rare disease
- Involves seminal vesicles in about 10% of radical prostatectomies, usually represents a localized form
- Amyloidosis develops subepithelially spreading to include the wall of seminal vesicles and ejaculatory ducts; appears to be related to advanced age (Ann Diagn Pathol 2008;12:235)
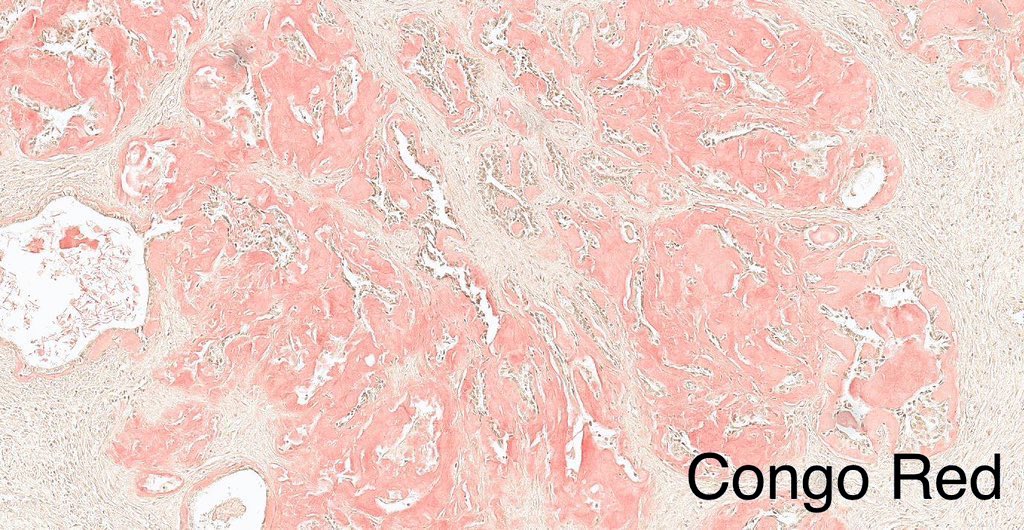
- Note: corpora amylacea may stain positive with Congo red
Essential features
- Pale amorphous hyaline, eosinophilic substance that accumulates and can pressure the adjacent epithelium
- Often displays processing cracks
- More common in seminal vesicles and vas deferens
- Subepithelial and vascular deposits
Epidemiology
- Occurs in 2-10% of radical prostatectomies (Turk Patoloji Derg 2012;28:44)
- Incidence increases with age, reaching 21% in men age 75 years and older (Histopathology 1993;22:173, Am J Pathol 1983;110:64)
- Vascular amyloid deposits are present in 2% - 10% of prostates with nodular hyperplasia or adenocarcinoma
- Higher incidence of amyloid deposits in patients with myeloma, primary amyloidosis of kidney or chronic diseases
- Amyloidosis of the seminal vesicles involves 10% of radical prostatectomy specimens
Sites
- More common in seminal vesicles and vas deferens
- Deposits are more commonly subepithelial and vascular
Etiology
- Although immunohistochemistry often detects lactoferrin (Ann Pathol 2004;24:236), amyloid apparently derives from semenogelin I, the major secretory product of the seminal vesicles (J Lab Clin Med 2005;145:187)
- Semenogelin I and II are mainly responsible for immediate gel formation of freshly ejaculated semen, and are degraded by the proteolytic action of prostate specific antigen/PSA (J Androl 1996;17:17)
Pathophysiology
- Abnormal folding of proteins that deposit as fibrils in the extracellular tissue and may accumulate preventing normal function
- Amyloidosis includes multiple biochemically distinct proteins but with similar morphologic appearance
- Different forms of amyloidosis include:
- Primary systemic amyloidosis (no evidence of preceding or coexisting disease, paraproteinemia or plasma cell neoplasia)
- Amyloidosis associated with multiple myeloma
- Secondary to coexisting previous chronic inflammatory or infectious conditions, hemodialysis
- Localized form
Clinical features
- Most commonly asymptomatic
- Can simulate prostate or bladder cancer invasion of seminal vesicles on MRI
Diagnosis
- Histology: amorphous pale eosinophilic material often with cracks from processing
- Histochemical stain with Congo red shows green birefringence on polarized microscopy
Radiology description
- Can simulate prostate or bladder cancer invasion of seminal vesicles on MRI
Case reports
- 55 year old man (Int Urol Nephrol 2005;37:495)
- 59 and 60 year old men with localized amyloidosis of seminal vesicle and vas deferens: report of two cases (J Korean Med Sci 2003;18:447)
- 66 year old man with prostatectomy for adenocarcinoma (Case of Week #85)
- 2 cases diagnosed at biopsy (Int J Urol 2004;11:925)
- Amyloidosis of the seminal vesicle; a case report and review of the literature (Scand J Urol Nephrol 2003;37:519)
Treatment
- Based on the underlying condition
Gross description
- Usually not seen grossly
- When involvement is massive, the organ can be enlarged and firm and cut section could show a waxy appearance
Microscopic (histologic) description
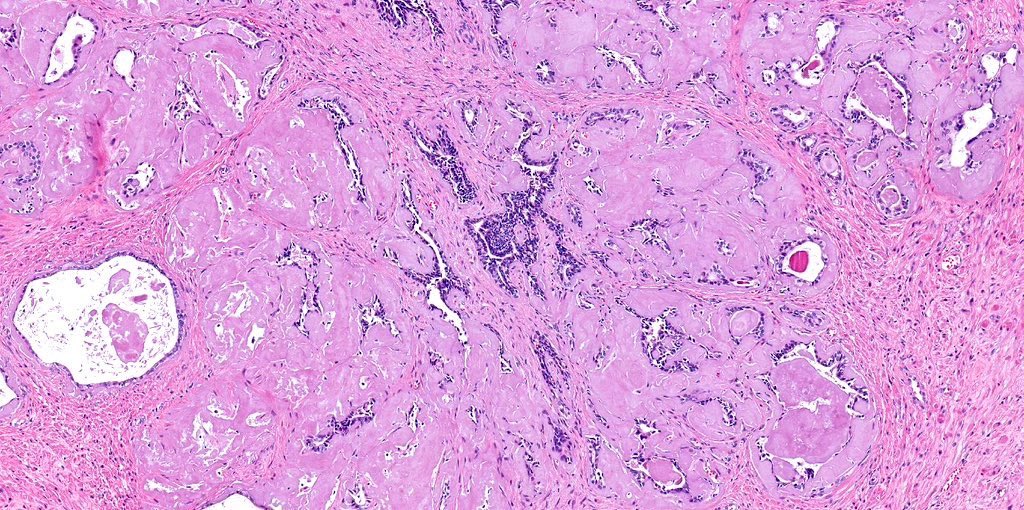
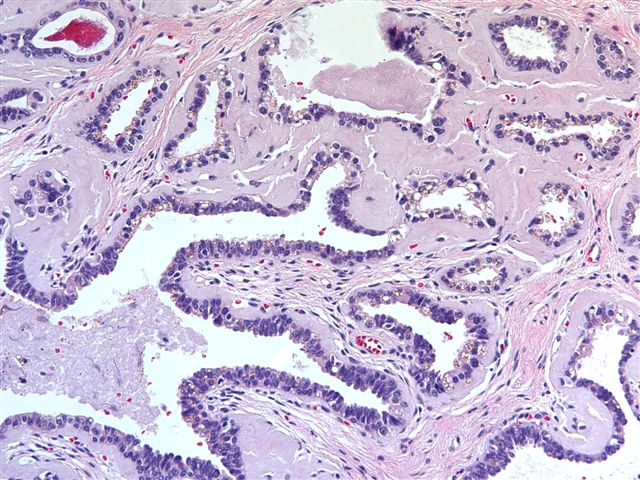
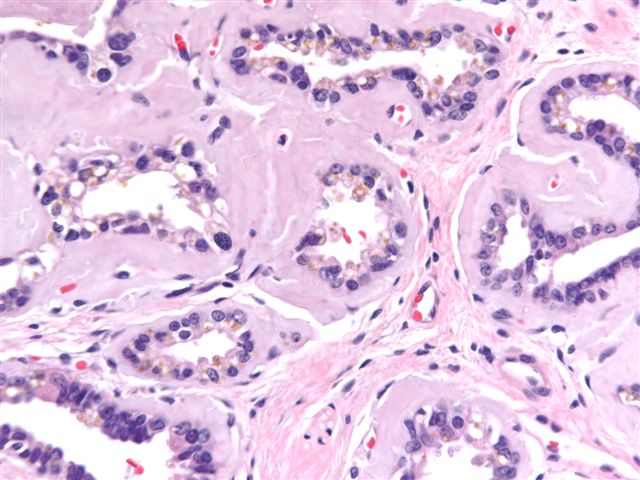
- Pale amorphous hyaline, eosinophilic substance that accumulates and can pressure the adjacent epithelium
- Often displays processing cracks
- Subepithelial location
- Can compress the adjacent epithelium
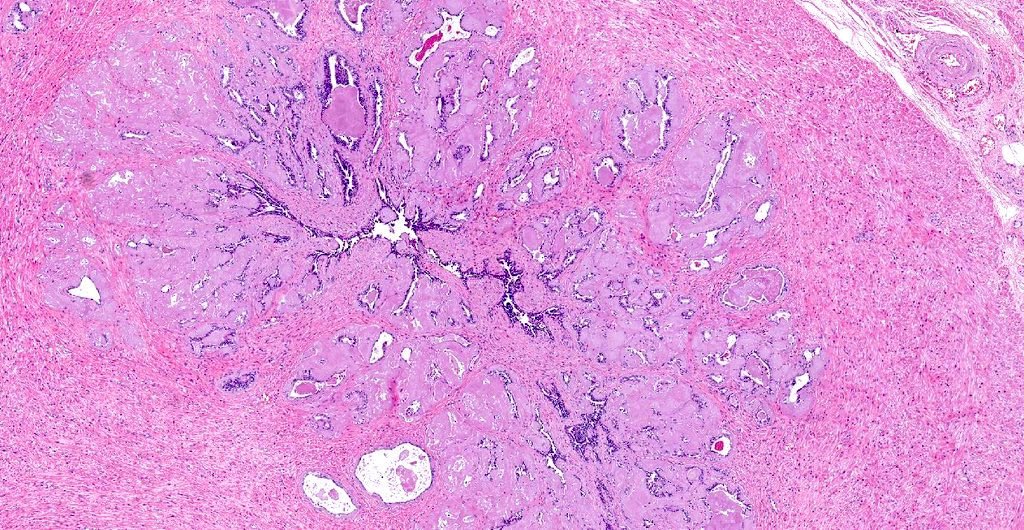
Microscopic (histologic) images
Contributed by Andres Matoso, M.D., @katcollmd on Twitter and Case #85
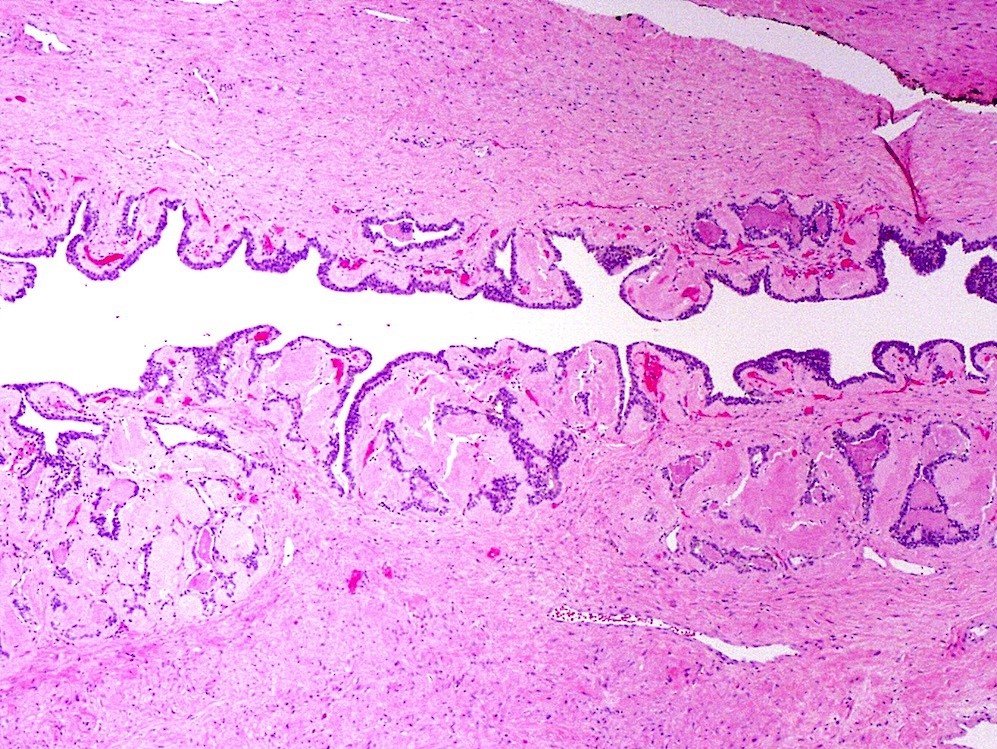
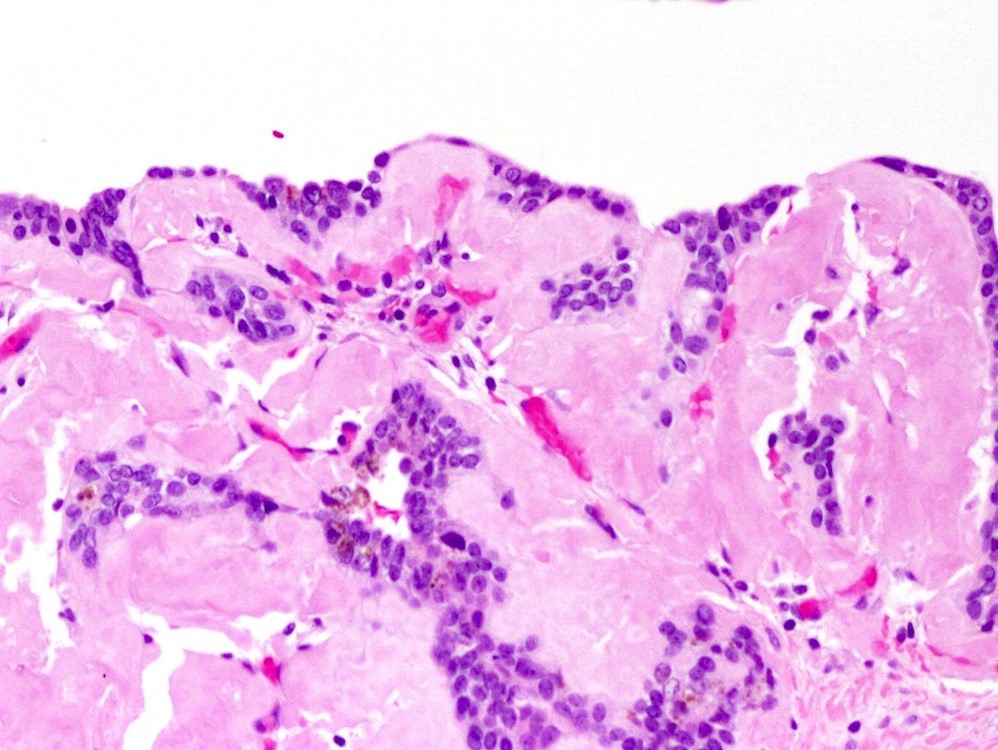
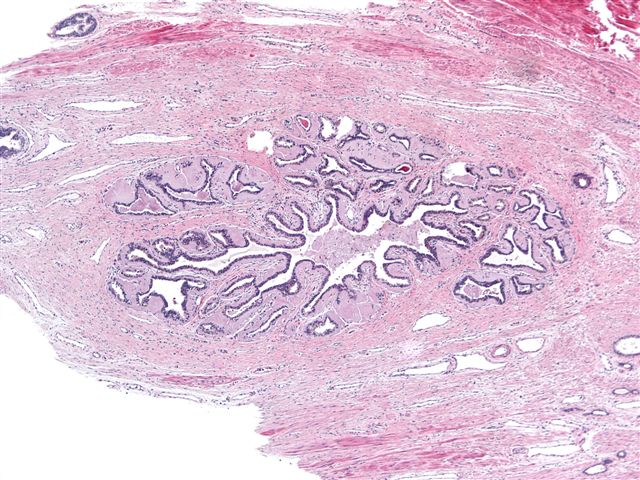
Various images

Amyloid
Amyloid
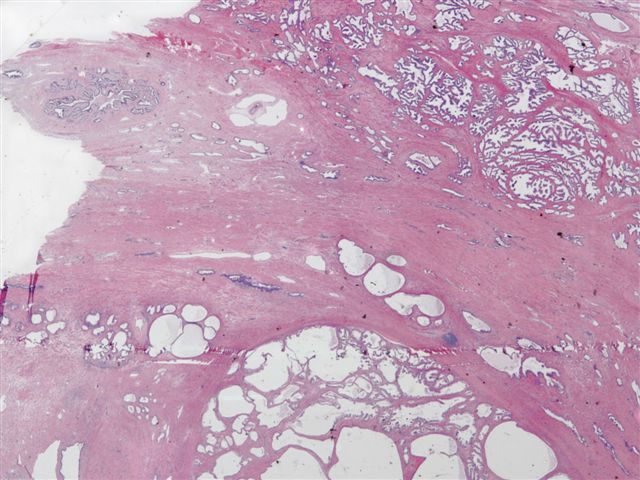
66 year old man with radical prostatectomy for adenocarcinoma
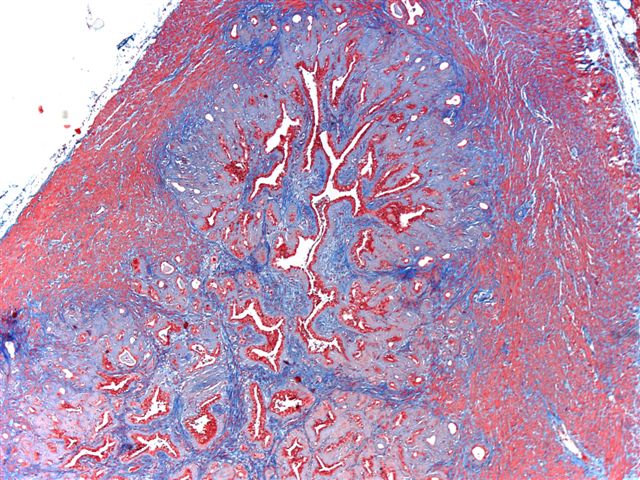
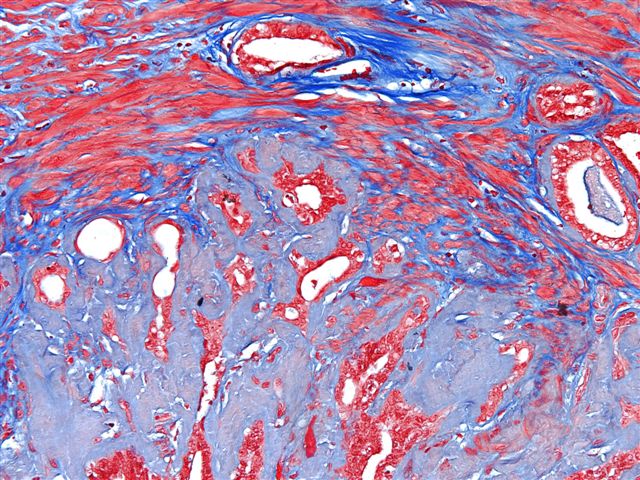
Trichrome stain
Positive stains
Electron microscopy description
- Electron microscopy shows nonbranching amyloid fibrils that measure 7.5 to 10 nm (Mod Pathol 1989;2:671)
Differential diagnosis
- It is important to exclude an underlying etiology including plasma cell neoplasia or an inflammatory condition
