
Salivary glands
Inflammatory
Chronic sialadenitis / sialolithiasis
Author: Kim A. Ely, M.D.
Editorial Board Member: Lisa Rooper, M.D.
Editor-in-Chief: Debra L. Zynger, M.D.

Last author update: 4 December 2020
Last staff update: 26 May 2021
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Chronic sialadenitis / sialolithiasis pathology [TIAB]
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology images | Case reports | Treatment | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Ely KA. Chronic sialadenitis / sialolithiasis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/salivaryglandssialolithiasis.html. Accessed April 16th, 2024.
Definition / general
- Repeated episodes of pain and inflammation due to impedance of salivary flow with stasis as a result of a stone
Essential features
- Results from impedance of salivary flow with stasis as a result of obstruction from a sialolith
- Affects the submandibular gland (80%) unilaterally without a side predilection
Terminology
- Obstructive sialadenitis
Epidemiology
- Sialolithiasis is estimated to affect 1/10,000 - 1/30,000 individuals (Otolaryngol Head Neck Surg 2011;145:935)
- 30 - 60 year old adults with a higher incidence in males
Sites
- Obstructive sialadenitis due to stones mostly affects the submandibular gland (80%) unilaterally without a side predilection (Oral Surg Oral Med Oral Pathol 1972;33:2)
- Alkaline pH, increased mucinous and mineral content of its saliva (elevated calcium and phosphate concentrations) predisposes to calculi
- Wharton duct runs upward, making saliva flow against gravity and is narrow and tortuous, further contributing to salivary stasis (Mayo Clin Proc 2018;93:266)
- Approximately 15% of salivary stones occur within the parotid gland
- Sublingual and other minor salivary glands are rarely affected
Pathophysiology
- Mechanism is unclear and may be due to:
- Multiple intracellular microcalculi which accumulate during secretory inactivity and are excreted into the ducts where they act as a nidus for the eventual formation of a sialolith (Otolaryngol Clin North Am 2009;42:927)
- Bacteria or food debris enter the distal submandibular or parotid ducts and act as a nidus for the development of larger calculi (Arch Otolaryngol Head Neck Surg 2001;127:66)
Etiology
- Uncertain but possible factors for stone formation include:
- Anatomic, affecting saliva formation or flow, such as duct stenosis or inflammation
- Composition factors, such as increased calcium content or altered enzyme function (StatPearls Publishing: Sialolithiasis [Accessed 16 September 2020])
Clinical features
- Intermittent, periprandial pain and swelling of a single salivary gland
- Risk factors include reduced fluid intake, tobacco use, prolonged illness, diuretics and drugs that diminish saliva (Otolaryngol Head Neck Surg 2011;145:935)
Diagnosis
- If inconclusive clinically, sialography is the gold standard for the diagnosis
Radiology images
Images hosted on other servers:

Hypoechoic mass
Case reports
- 35 year old man with swelling below jaw (Mayo Clin Proc 2018;93:266)
- 39 year old woman with a history of migraines presented for evaluation of recurrent left sided submandibular swelling (J Oral Maxillofac Surg 2016;74:2447)
- 67 year old woman with mass of the upper lip (Oral Maxillofac Surg 2019;23:91)
Treatment
- Treatment is conservative, with excision reserved for the minority of cases
Gross images
Images hosted on other servers:

Smooth mass

Sialolith
Microscopic (histologic) description
- Varying degrees of acinar destruction, fibrosis and chronic inflammation, with lymphoid aggregates containing prominent germinal centers
- Ducts may undergo squamous and mucous metaplasia
- Lobular arrangement is maintained
- May see microliths
- Otolaryngol Clin North Am 2009;42:927
Microscopic (histologic) images
Contributed by James S. Lewis, M.D.
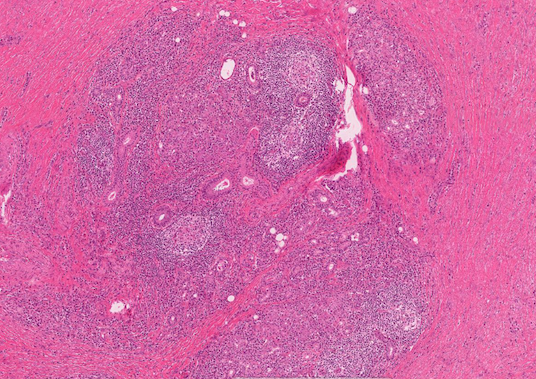
Preservation of lobular architecture
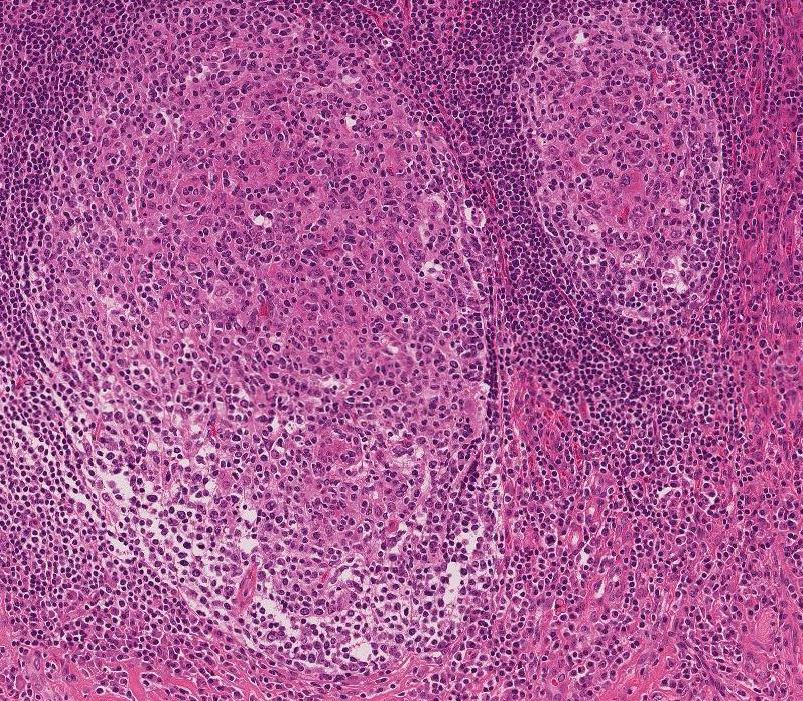
Intense chronic inflammation
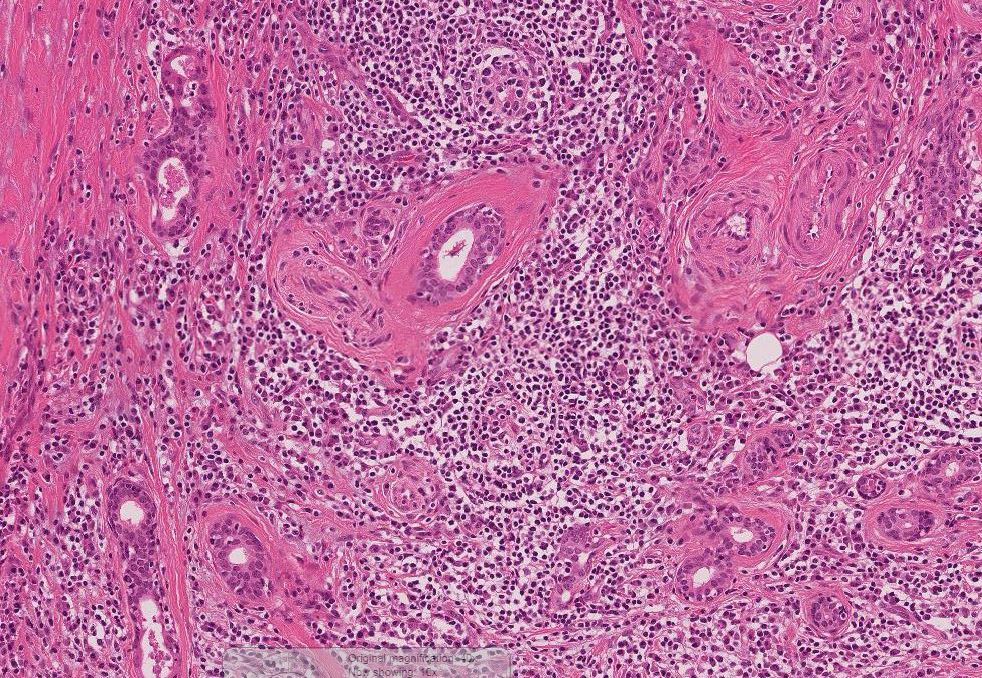
Acinar destruction
Sample pathology report
- Submandibular gland, left, excision:
- Chronic sialadenitis (see comment)
- Comment: There is a prominent periductal lymphoplasmacytic infiltrate containing lymphoid aggregates with prominent germinal centers. Some ducts appear ectatic and filled with debris suggestive of a microlith. Others are affected by squamous and mucinous metaplasia. These changes are associated with varying degrees of acinar atrophy and fibrosis.
Differential diagnosis
- Mucoepidermoid carcinoma:
- Infiltrative growth pattern
- Complex architecture
- IgG4 related sialadenitis:
- Dense chronic inflammatory infiltrate rich in plasma cells
- IgG4/IgG ratio greater than 40%
- Fibrosis which focally is storiform
- Obliterative phlebitis (Head Neck Pathol 2016;10:530)
- Dense chronic inflammatory infiltrate rich in plasma cells
- Lymphoepithelial sialadenitis (LESA):
- Affects the parotid, usually women
- Contains lymphoepithelial islands
Board review style question #1

A 55 year old man presents with a history of intermittent pain and swelling of the submandibular gland after eating. A biopsy with immunostains for IgG4 and IgG was performed and demonstrated a positive plasma cell ratio of 20%. Which of the following is the most likely diagnosis?
- Chronic sialadenitis
- IgG4 related sialadenitis
- Lymphoepithelial sialadenitis
- Mucoepidermoid carcinoma
Board review style answer #1
Board review style question #2
Why is it thought that stones most commonly arise in the submandibular gland?
- Acid pH of its saliva predisposes to the precipitation of minerals
- Caliber of Wharton duct is wide, causing stasis of secretions
- Mucinous and viscous nature of its saliva results in a more stagnant flow of secretions
- Wharton duct descends precipitously leading to pooling of saliva
Board review style answer #2
C. Mucinous and viscous nature of its saliva results in a more stagnant flow of secretions
Comment Here
Reference: Chronic sialadenitis / sialolithiasis
Comment Here
Reference: Chronic sialadenitis / sialolithiasis
