

Skin nontumor
Infestations
Myiasis
Last author update: 1 December 2016
Last staff update: 7 March 2024
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Botfly[TI]
See also: Myiasis


Table of Contents
Definition / general | Terminology | Epidemiology | Sites | Etiology | Diagrams / tables | Clinical features | Diagnosis | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Videos | Differential diagnosis | Additional referencesCite this page: Nagarajan P, Suo L. Myiasis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skinnontumorbotfly.html. Accessed April 19th, 2024.
Definition / general
- Infestation by larvae of the human botfly (Dermatobia hominis) and tumbu fly (Cordylobia anthropophaga) are common causes of myiasis
- Skin lesions are due to growth and burrowing of the larva, which feed on the host tissues, liquid body substance or ingested food
- Other cutaneous locations such as eye, mucosa, breast and gastrointestinal tract can be affected (West Afr J Med 2013;32:149)
Terminology
- Human botfly, Dermatobia hominis, myiasis
Epidemiology
- Tropical and subtropical areas with warm and humid climate, such as the Americas, Central and South Africa are most common (CDC: Parasites - Myiasis [Accessed 10 October 2018])
- Rarely seen in the continental United States; most commonly seen in travelers
Sites
- Any body site can be affected, especially wounded or exposed skin (Infect Genet Evol 2014;23:209)
- Other cutaneous and mucosal locations such as eyes and gastrointestinal tract can also be affected (West Afr J Med 2013;32:149)
- When mucosal sites such as nasal sinuses are affected, the sequelae are grave (J Clin Neurosci 2013;20:1178, BMJ Case Rep 2010 Dec 29;2010)
Etiology
Life cycle:
- In endemic areas, D. hominis flies typically lay their eggs on mosquitoes, which in turn deposit them on warmblooded mammals such as humans
- In wound myiasis, an open wound or orifice attracts flies to deposit their eggs
- The eggs hatch in the skin, stimulated by the heat from the host
- The larvae mature through 3 stages during which they develop posterior spines, which makes them difficult to dislodge
- 5 - 10 weeks after deposition, the mature third stage larvae drop from the host and complete the pupal stage in soil
- Adult botfly emerges from soil after 4 - 11 weeks
Diagrams / tables
Images hosted on other servers:

Life cycle of D. hominis
Clinical features
- May clinically resemble insect bites, allergic reactions, herpes virus or molluscum contagiosum
- Furuncular myiasis: a pruritic papule that develops within 24 hours of penetration, enlarging to 1 - 3 cm in diameter
- These lesions can be painful or tender and may become crusted and purulent
- In wound myiasis, the larvae are deposited in a suppurating wound or on decomposing flesh
- Creeping (or migratory) cutaneous myiasis resembles cutaneous larva migrans, but the larvae migrate more slowly, persist for longer (often months) and are larger than helminth larvae
- In most cases, myiasis is self limited with minimal morbidity
- Secondary infection by bacteria may be a complication
Diagnosis
- Thorough physical examination and documentation of relevant exposure history, including travel to warm humid climates
- Surgical extraction and histologic examination can confirm the presence of larvae
- Supportive travel history
Case reports
- 10 year old Indian boy with redness of both eyes (Ocul Immunol Inflamm 2011;19:444)
- 29 year old man with an unusual cause of an abscess (BMJ Case Rep 2014 Oct 21;2014)
- 50 year old male traveler to Belize (CJEM 2007;9:380)
- 61 year old woman traveler to Belize with pruritic lesions on back, thigh and supraclavicular area (Arch Pathol Lab Med 2001;125:453)
- Patient returning from Bolivia with nonhealing furuncle containing botfly (Pritt: Creepy Dreadful Wonderful Parasites Blog - Case of the Week 505 [Accessed 9 October 2018])
Treatment
- The major reasons for treatment are reduction of pain, cosmesis, psychological relief and to prevent secondary infections
- Surgical extraction of larvae is the key treatment
- Systemic medication: broad spectrum antibiotics, oral steroid and ivermectin may also be used (Ocul Immunol Inflamm 2011;19:444)
Clinical images
Images hosted on other servers:

Close up, adult and larvae of D. hominis
Gross description
- Helpful features for identification (Pritt: Creepy Dreadful Wonderful Parasites Blog - Answer to Case 505 [Accessed 9 October 2018]):
- Overall robust and somewhat pear shaped body with a narrow posterior
- Large spines on all but the terminal 3 body segments
- Posterior spiracle with 3 slightly curved slits and a weak peritreme
Gross images
Contributed by Bobbi Pritt, M.D.


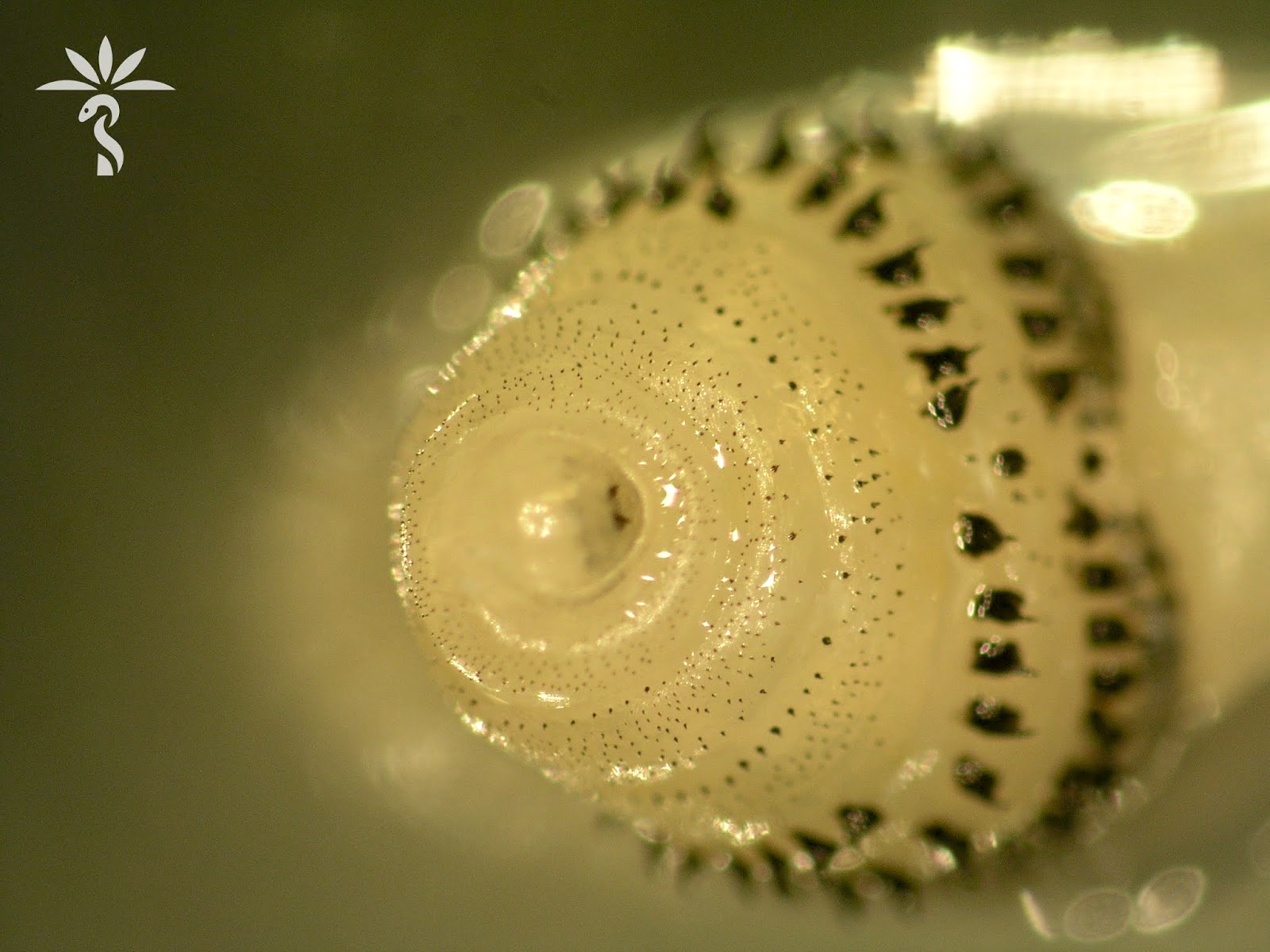
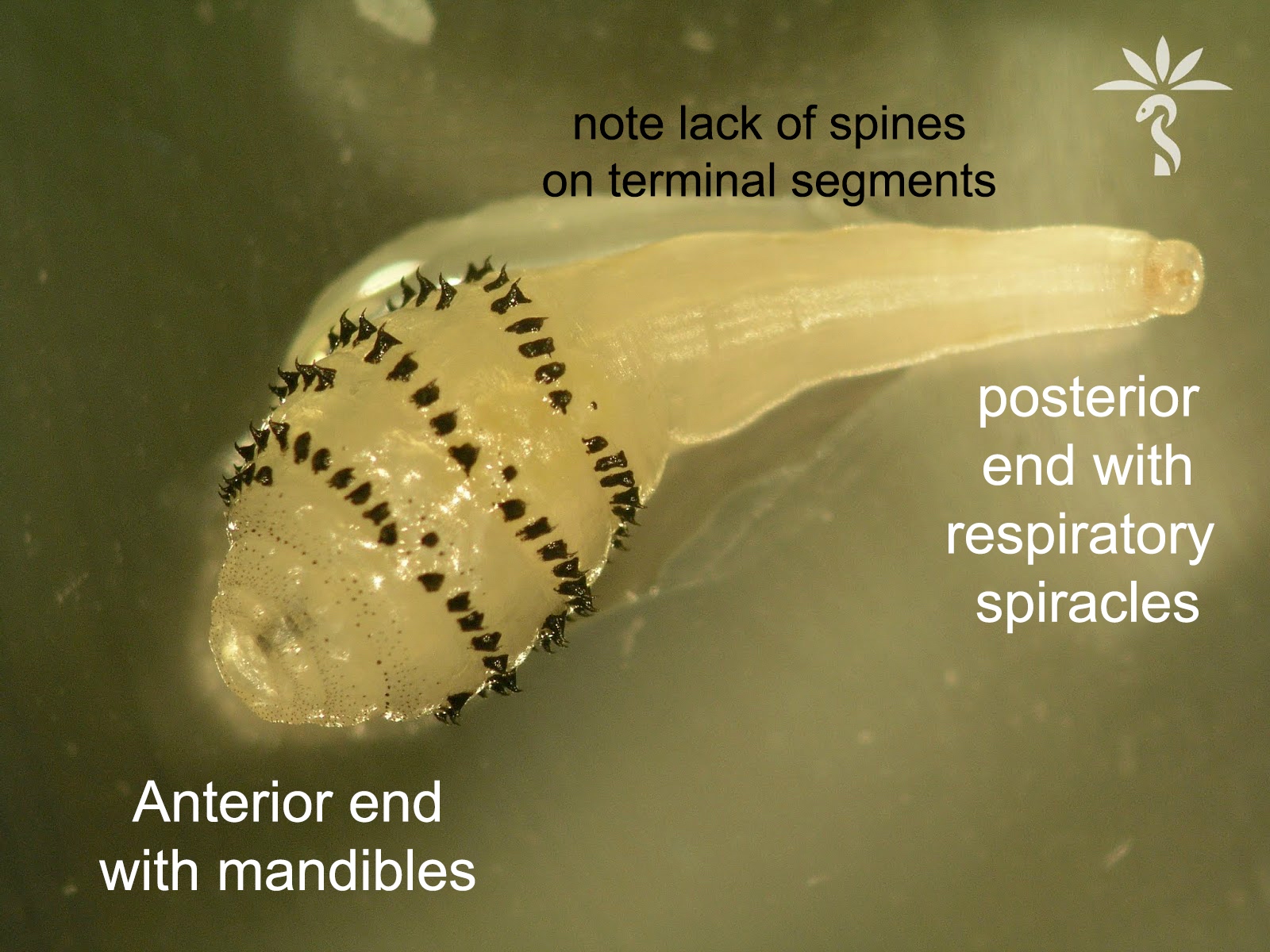
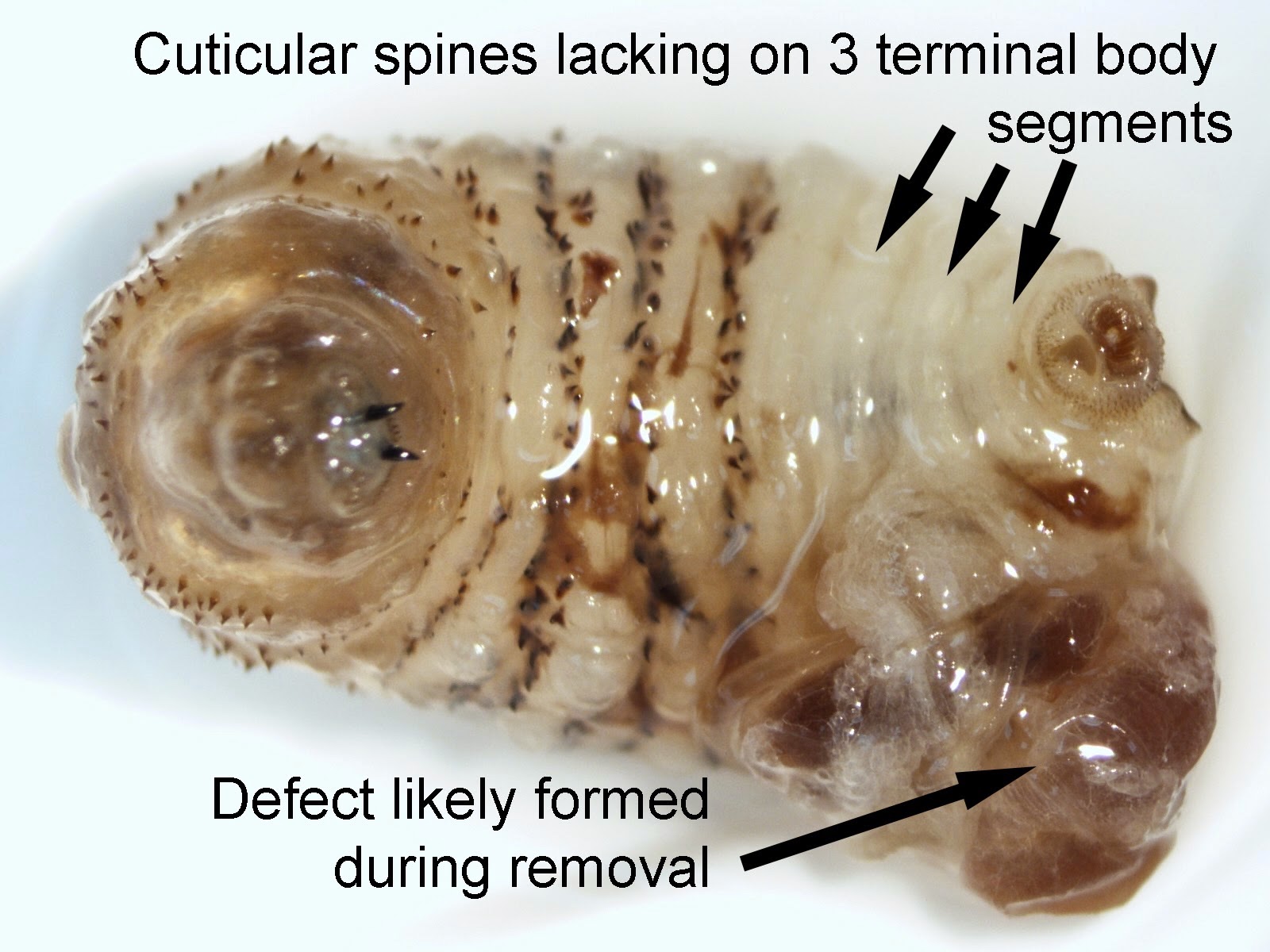
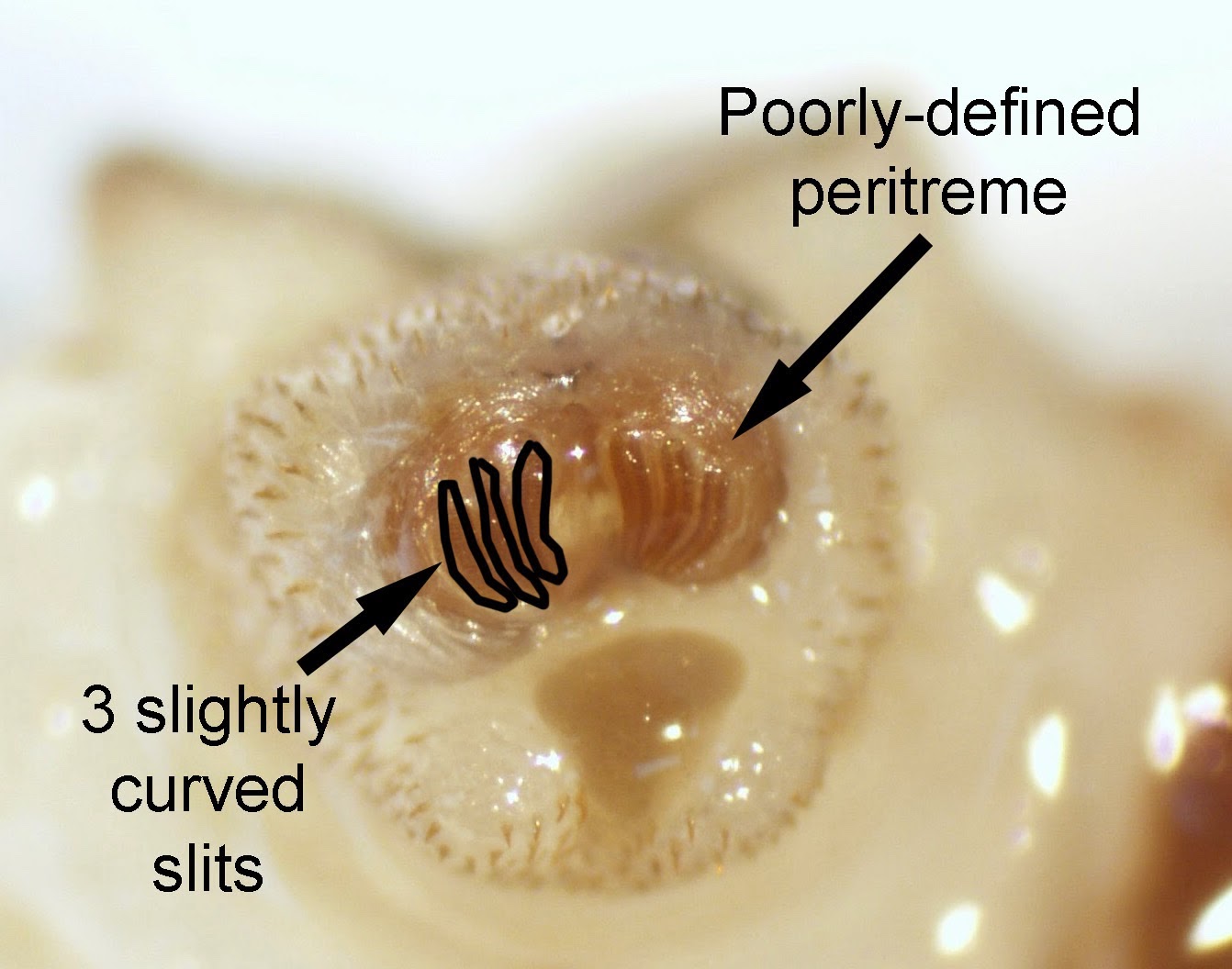
Dermatobia hominis, the human botfly
Microscopic (histologic) description
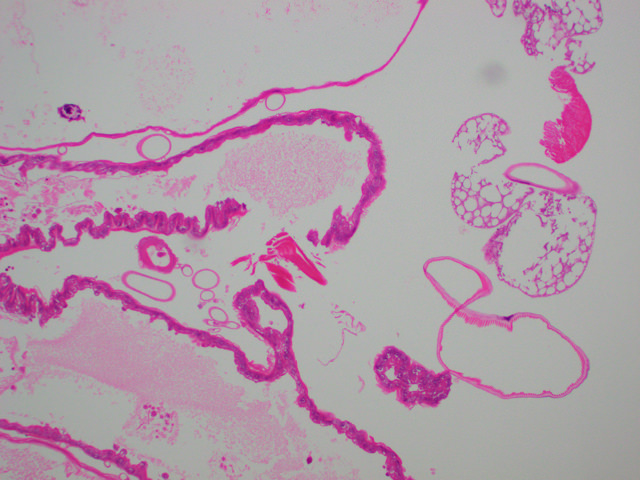
- Histologically, a mixed acute and chronic inflammatory infiltrate composed of varying proportions of neutrophils (early), lymphocytes, plasma cells and histiocytes (late), admixed with eosinophils (J Am Acad Dermatol 2004;50:S26)
- Histologically, larvae are characterized by an undulating chitinous exoskeleton and pigmented spines (setae) protruding from exoskeleton
Microscopic (histologic) images
Contributed by Priya Nagarajan, M.D., Ph.D.



2x magnification
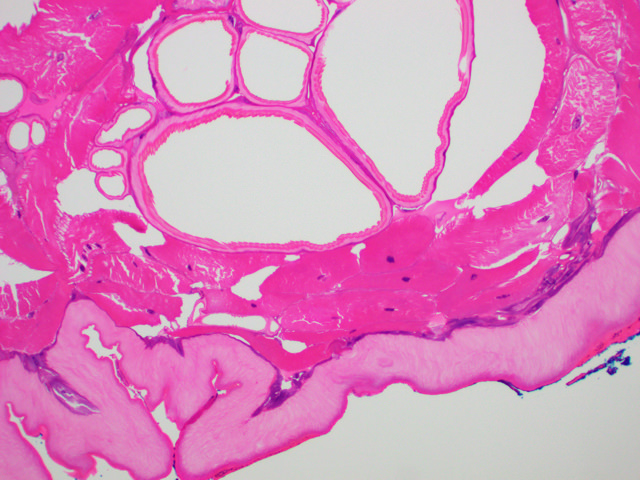
10x magnification
Videos
Differential diagnosis
- Furuncular cutaneous myiasis should be differentiated from:
- Ruptured epidermoid cyst
- Abscess
- Furunculosis
- Foreign body reaction
- Exaggerated arthropod bite reaction
- Lymphadenopathy
- Tungiasis
- Onchocerciasis
- Tick infestation (tick head burrows; lack pigmented setae)
- Creeping cutaneous myiasis should be differentiated from:
- Scabies (scabies or burrows may be seen in biopsies)
- Larva migrans
- Cellulitis (no parasite seen)
