

Soft tissue
Fibroblastic / myofibroblastic
Elastofibroma


Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Elastofibroma
- Benign, ill defined proliferation of fibroelastic tissue with excessive abnormal degenerated elastic fibers
- Mostly asymptomatic mass at infrascapular region, incidentally found on radiological examination for other causes
- Well circumscribed lesion, comprised of mature fat, fibrous tissue and characteristic abnormal eosinophilic looking elastic fibers
- Surgical excision is curative, required mostly in symptomatic cases, with very rare local recurrence
- Acceptable: elastofibroma dorsi
- ICD-O: 8820/0 - elastofibroma
- ICD-11: FB51.Y & XH3BQ8 - other specified fibroblastic disorders & elastofibroma
- Exact prevalence is unknown as most are detected incidentally
- Arises almost exclusively in the elderly, with peak incidence between the seventh and eighth decades of life
- F > M (Ann R Coll Surg Engl 2020;102:84)
- Mostly arises in the deep soft tissue between the lower scapula and the thoracic wall
- Other (rare) sites include
- Thigh (Cureus 2023;15:e42174)
- Pancreas (Case Rep Gastrointest Med 2016;2016:2697187)
- Arm / hand (Am J Case Rep 2022;23:e937787)
- Umbilicus (Ann R Coll Surg Engl 2020;102:84)
- Greater omentum (Rom J Morphol Embryol 2020;61:841)
- Aortic valve (Ann R Coll Surg Engl 2020;102:84)
- Gluteal region (BMC Musculoskelet Disord 2020;21:16)
- Face (J Dent (Shiraz) 2015;16:73)
- Neck (West Indian Med J 2014;63:189)
- Elastotic degeneration of collagen or abnormal elastotic fibrogenesis may underlie the pathogenesis of elastofibroma and active neovascularization or endothelial mesenchymal transition plays a potential pathogenetic role (Eur J Histochem 2015;59:2459)
- Most recently, chromosomal abnormalities have been described in a few cases, including those for chromosome 1, suggesting a neoplastic nature for this tumor (Cancer Genet Cytogenet 2001;126:68)
- Traditionally, it was thought to be associated with microtrauma, being reported more commonly in laborers
- Case reports show positive relationship with a patient's dominant hand side (Turk Gogus Kalp Damar Cerrahisi Derg 2022;30:250)
- Unknown at this time
Images hosted on other servers:

Proposed pathogenesis
- Lesion usually presents as a slow growing, asymptomatic mass or rarely causes stiffness, pain, scapular snapping and impingement
- Radiology is characteristic, particularly if the tumor arises at the typical subscapular location
- Most asymptomatic cases do not require a biopsy unless there is a need to rule out malignancy
- Symptomatic ones are excised and histopathology confirms the diagnosis suggested on imaging
- Reference: Saudi Med J 2022;43:156
- Ultrasound: complex hypoechoic lesion
- CT scan: attenuation appears similar to skeletal muscle
- MRI: heterogeneous masses with internal fatty areas
- Diffusion MRI (Sisli Etfal Hastan Tip Bul 2020;54:103)
- Newly proposed technique
- Lesions appear heterogeneous with hyperintensity on T2 weighted images
- More sensitive than conventional MRI in differentiating malignant lesions
- PET CT: moderate increased uptake, symmetrical in bilateral lesions (Indian J Nucl Med 2019;34:258)
Images hosted on other servers:

Coronal CT

Axial CT

MRI of subscapular mass

CT of subscapular and gluteal masses

CT scan

Ultrasonographic appearance


MRI findings


PET CT findings

MRI with diffusion sequences
- Benign lesion cured by simple excision
- Local recurrence is extremely rare with only occasional case reports (J Orthop 2014;12:S133)
- 48 year old woman with incidental bilateral subcapsular masses (Indian J Nucl Med 2019;34:258)
- 55 year old woman with painful thigh mass (Cureus 2023;15:e42174)
- 66 year old woman with mass arising at subcapsular port site after lung cancer surgery (Surg Case Rep 2017;3:121)
- Most asymptomatic cases do not require any treatment
- Complete excision is curative
Images hosted on other servers:

Bilateral subscapular masses

Bilateral painful masses

Left parotid region mass

Intraoperative view of subscapular mass

Surgical excision of the elastofibroma dorsi

Typical location (arrow)
- May or may not be well circumscribed lesion, without a definite capsule
- Cut surface is firm to rubbery and shows fibrous and fatty areas
Contributed by Nasir Ud Din, M.B.B.S
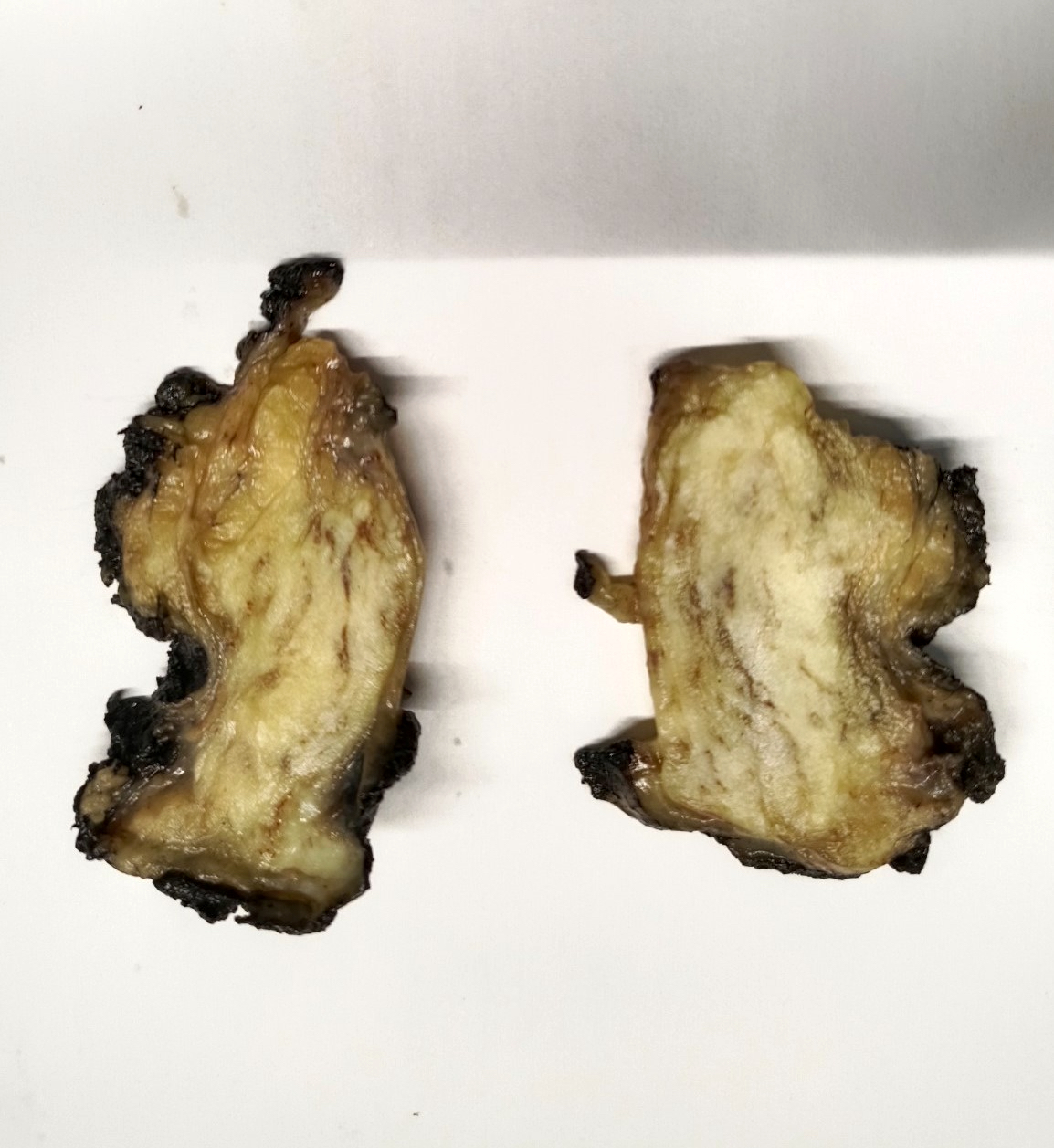
Fibrous and fatty areas
Images hosted on other servers:

Excised masses


Poorly circumscribed lesion

Bilateral excised masses

Whole and cut up specimen

Pancreatic lesion
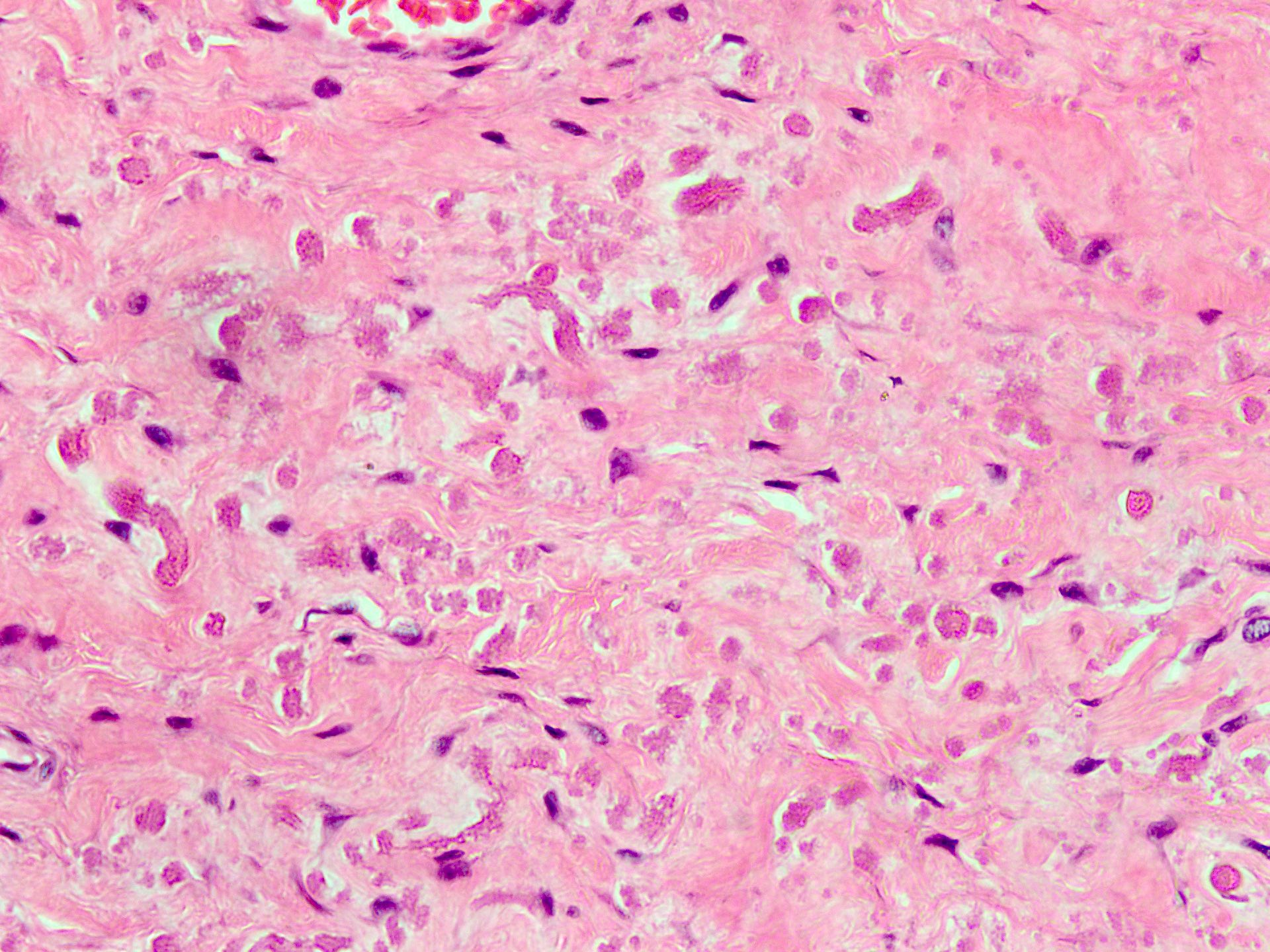
- Essential diagnostic criteria: bland appearing fibrofatty tumor with abnormal elastic fibers
- Infiltrative, ill defined, unencapsulated hypocellular lesion, which may entrap skeletal muscle fibers at the periphery or invade periosteum
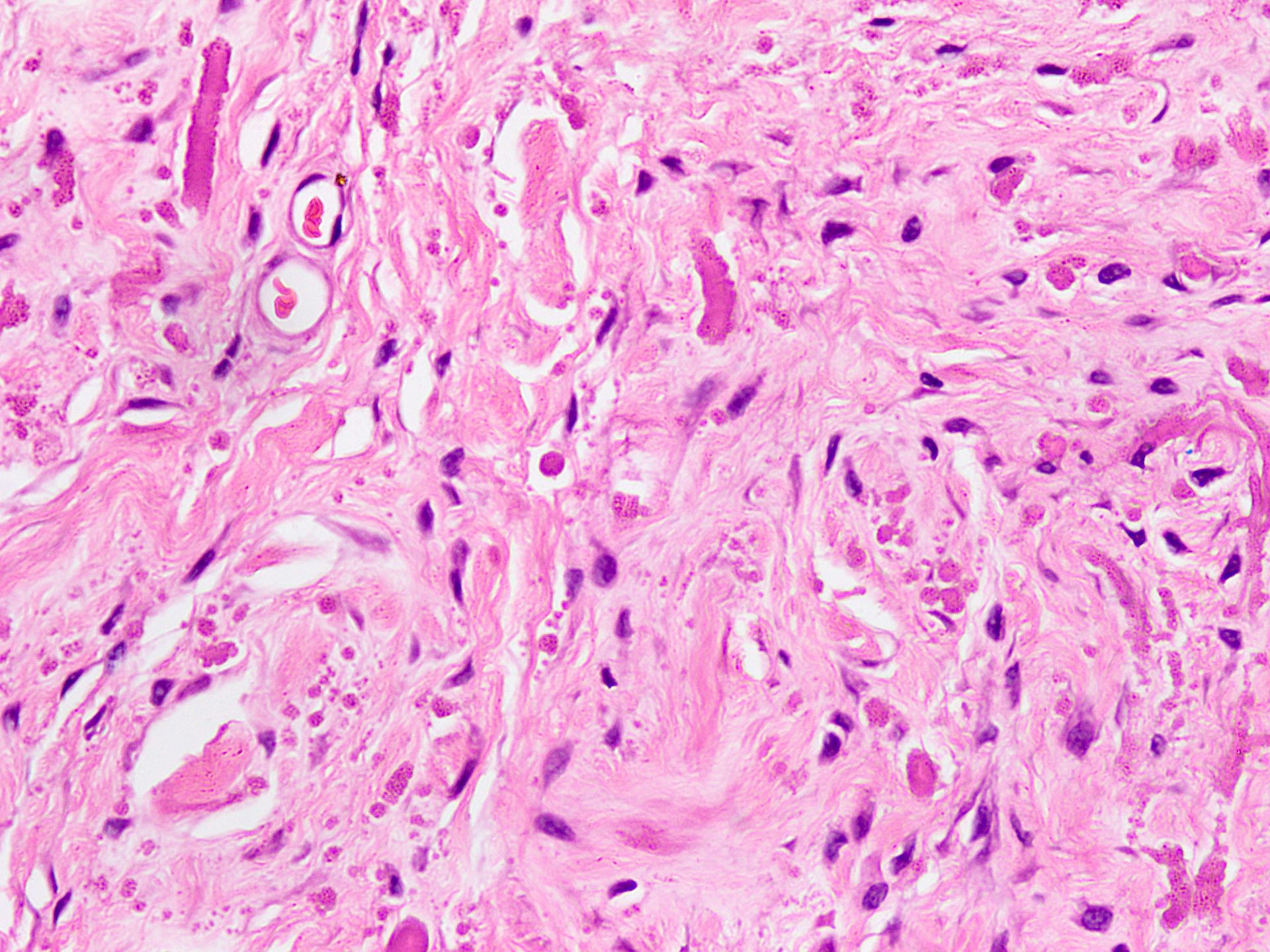
- Collagenized stroma with variable hypocellular myxoid to edematous areas
- Admixed mature adipocytes present
- Scattered abnormal elastic fibers appear as densely eosinophilic, round to irregular, variably sized globules, elongated structures with irregular fuzzy outlines or beaded cords
- Scattered spindle to stellate, bland looking fibroblasts are seen
- Lacks significant nuclear atypia or foci of necrosis
- Reference: Anticancer Res 2021;41:2211
Contributed by Nasir Ud Din, M.B.B.S.
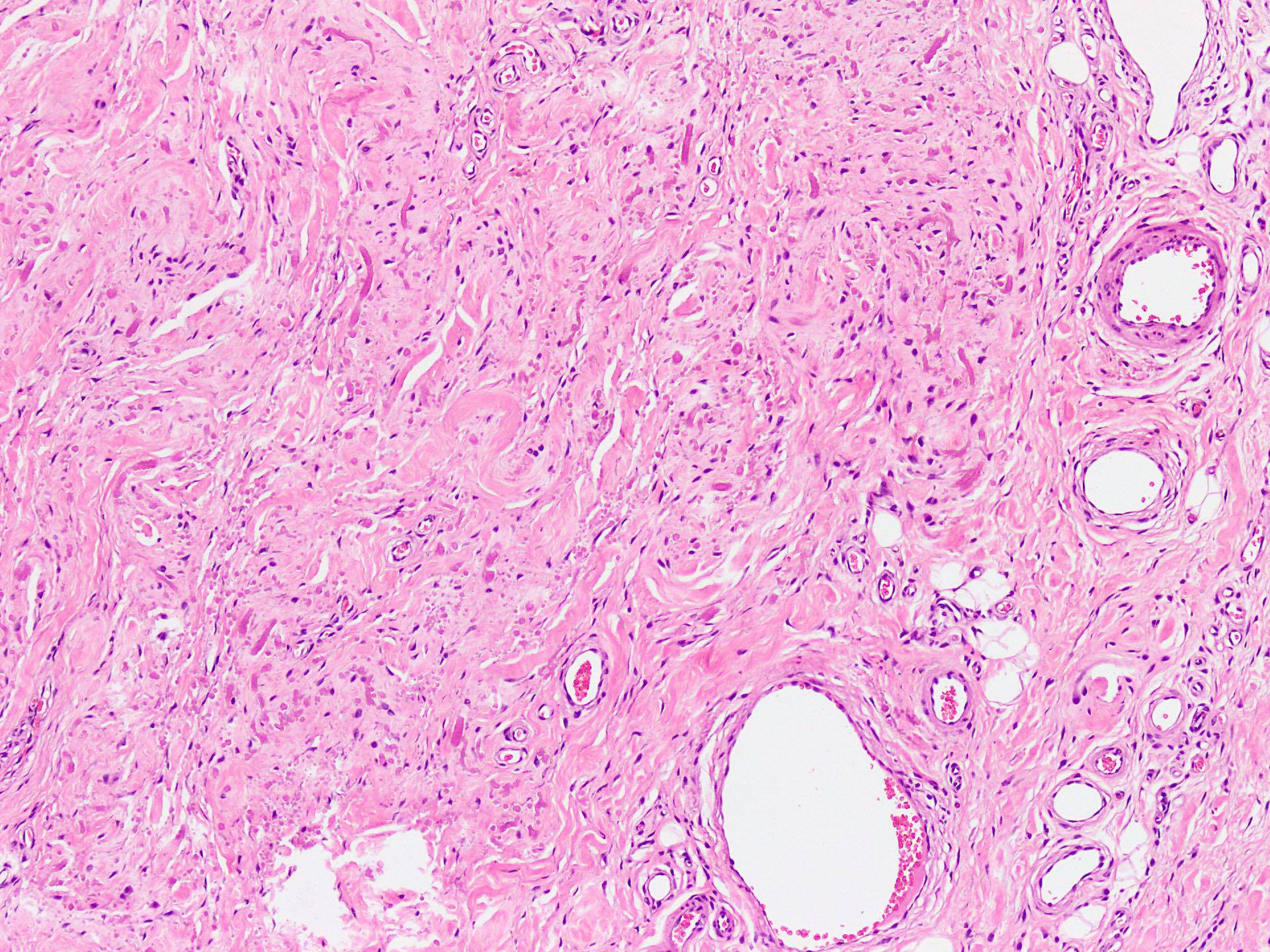
Stroma with fat and elastic fibers
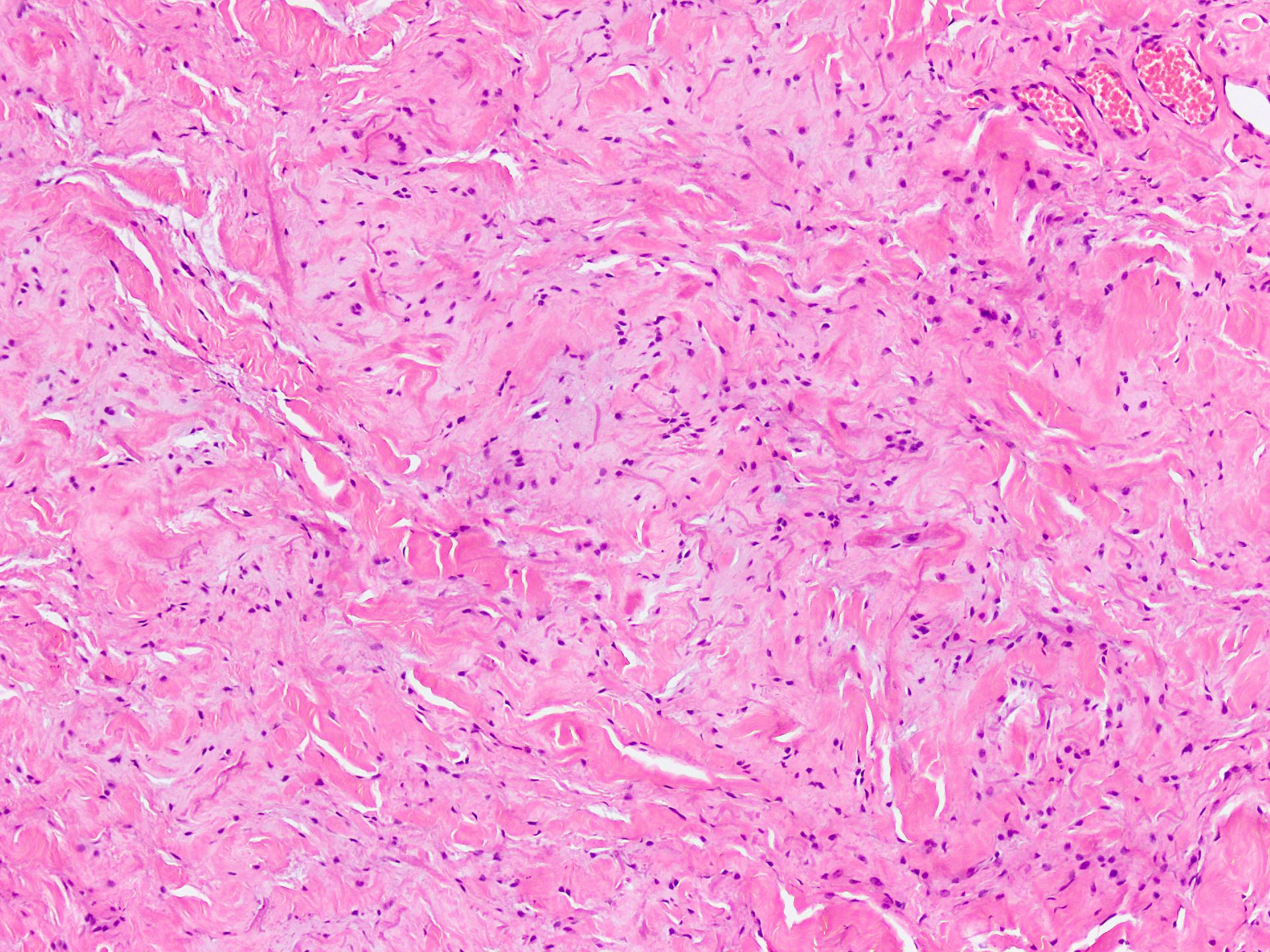
Bland looking fibroblasts
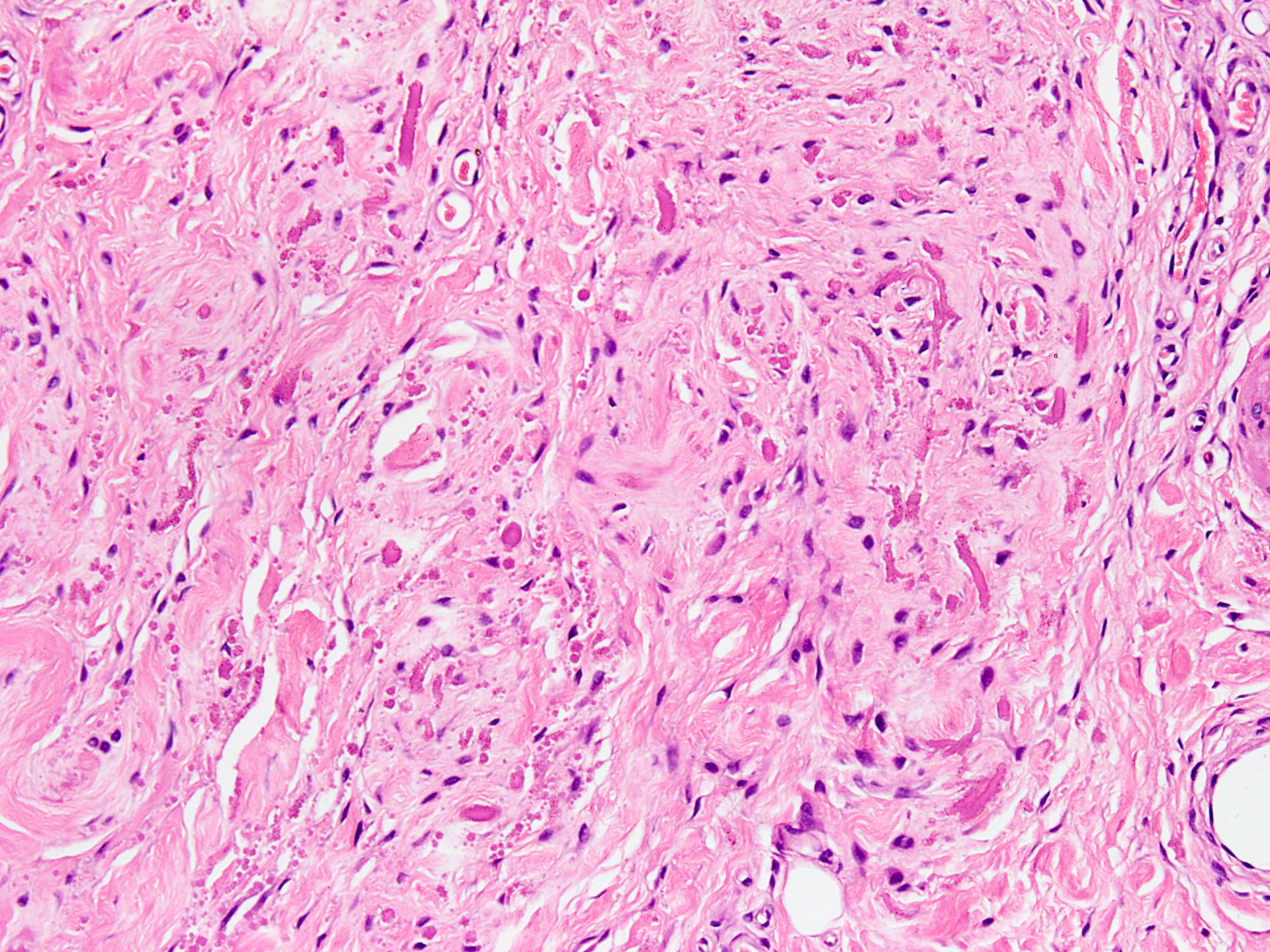
Eosinophilic elastic fibers
Globular appearance of elastic fibers
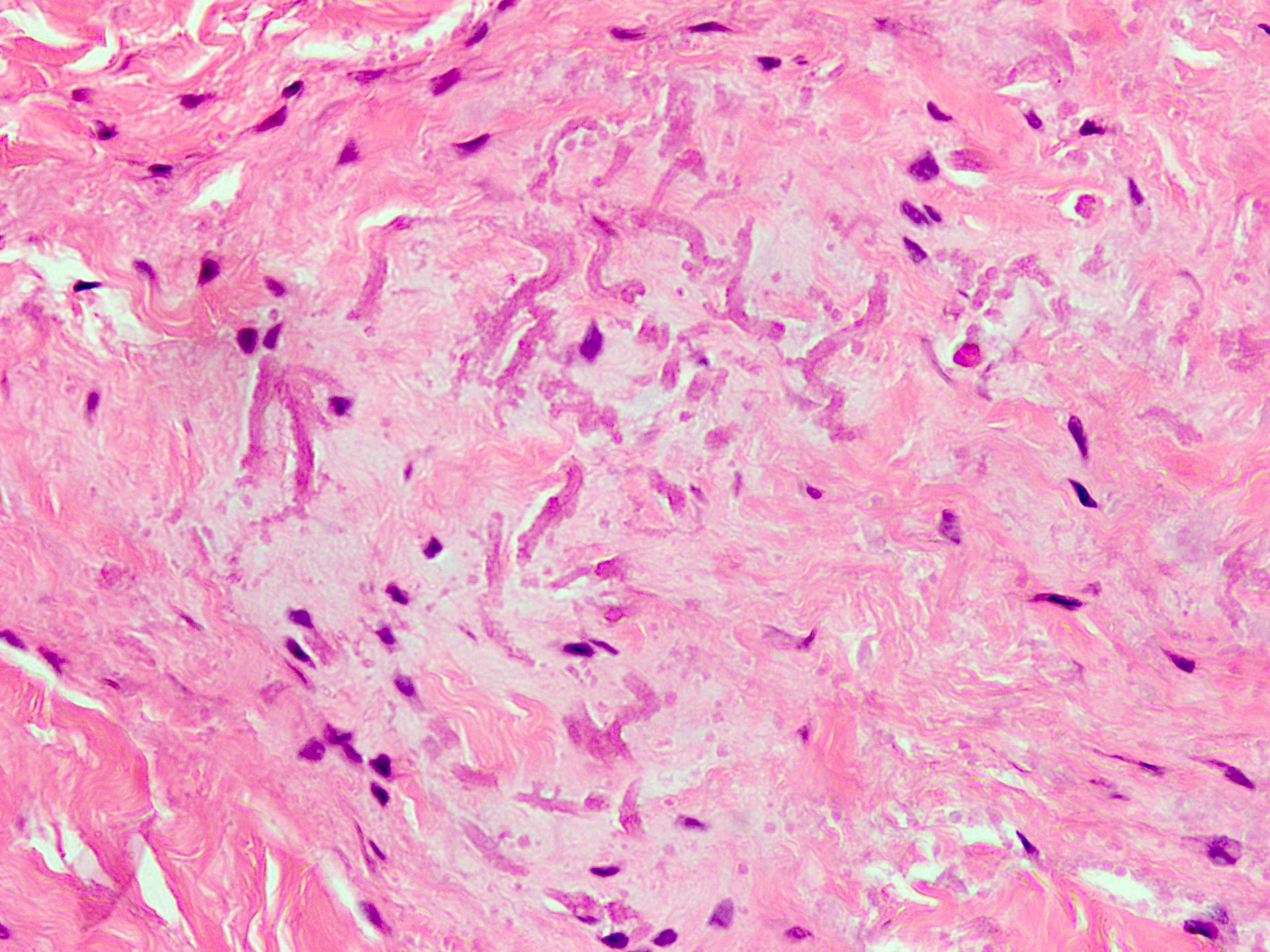
Clustering of elastic fibers
Abnormal elastic fibers
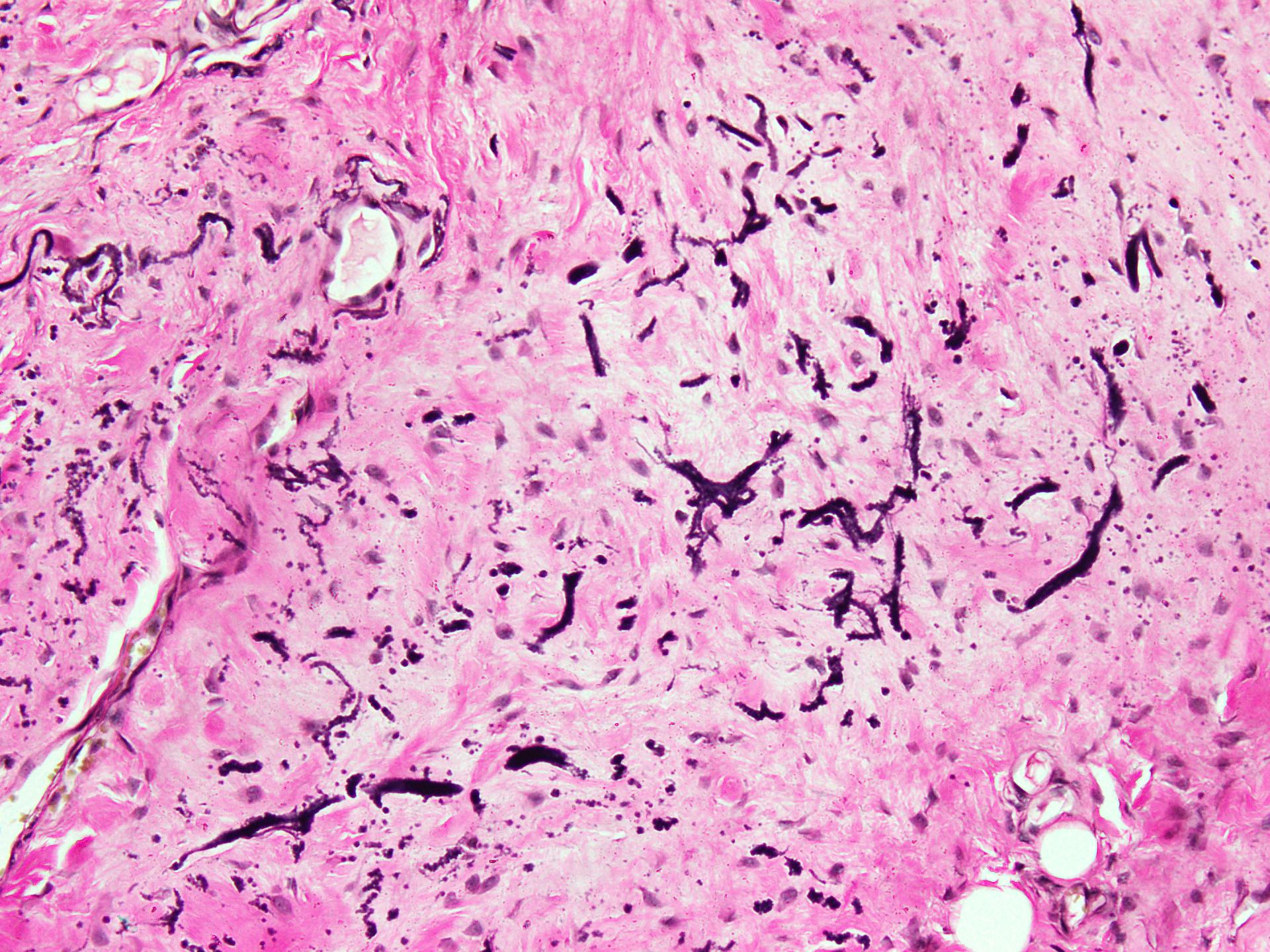
Elastic stain
Images hosted on other servers:

Elastofibroma whole slide image (WSI)

Infrascapular lesion

Chest wall lesion
- Cytological smears show degenerated abnormal elastic fibers in the form of globules, braids and elongated fibers
- Altered elastic fibers have green-yellow autofluorescence with ultraviolet light (Diagn Cytopathol 2002;26:310)
- Elastic (Verhoeff van Gieson): intense black staining of abnormal elastic fibers (J Dent (Shiraz) 2015;16:73)
- Alcian blue: stains mucopolysaccharide component of stromal connective tissue (Eur J Histochem 2015;59:2459)
- CD34: membranous positivity in a patchy manner seen in the fibroblasts (Cureus 2023;15:e42174)
- Periostin: cytoplasmic staining of cells around lesional blood vessels (Cureus 2023;15:e42174)
- Tenascin C: cytoplasmic staining of stromal cells; not specific as most human connective tissue cells also stain with this marker (Cureus 2023;15:e42174)
- Abnormal elastic fibers appear as electron dense masses of 3 - 5 micron diameter, removed by elastase digestion
- Some areas may show homogeneous, extremely dense core surrounded by dense, irregular fibers of diameter 350 A to 400 A with an indistinct outline (J Clin Pathol 1968;21:463)
Images hosted on other servers:


Electron dense fibers


Electron dense fibers
- Pathognomonic cytogenetic abnormalities have not been described to date
- Recent studies have described DNA copy number changes in a few cases, particularly involving chromosome 1 and X chromosome (Cancer Genet Cytogenet 2001;126:68)
Elastofibroma pathology
Elastofibroma radiology
- Right subscapular mass, excision:
- Benign soft tissue lesion, consistent with elastofibroma (see comment)
- Comment: An ill defined, hypocellular lesion showing spindle cells and collagenized stroma in the background, with entrapment of fat and skeletal muscle at the periphery. Scattered abnormal elastic fibers appear as densely eosinophilic, round to irregular, variably sized globules to beaded structures. These tumors follow a benign course with complete excision being curative. Recurrence is extremely rare.
- Desmoid fibromatosis:
- More cellular as compared with elastofibroma
- Prominent collagenous background
- Nuclear beta catenin positivity in most cases
- Fibrolipoma:
- Mixture of fibrous connective tissue and adipocytes
- Arises at anatomic sites other than those characteristic for elastofibroma
- Lacks abnormal elastic fibers
- Gardner / nuchal type fibroma:
- Densely collagenous lesions with cracking artifact
- Adipocytic component is minimal to absent
- Abnormal elastic fibers are not seen
- Differs in anatomic distribution
- Atypical lipomatous tumor / well differentiated liposarcoma:
- Characteristically shows atypical stromal cells or lipoblasts
- Adipocytes show variation in size as well as atypia
- Lacks abnormal elastic fibers
- Chest wall elastofibroma protruding into thoracic cavity may mimic liposarcoma on imaging (Acta Radiol Open 2022;11:20584601221080514)
- Elastofibromatosis / elastofibromatous change:
A 60 year old man undergoes MRI for staging of biopsy proven lung cancer. Imaging shows bilateral subscapular masses with attenuation similar to adjacent skeletal muscle. Surgical excision is performed and light microscopic appearance is shown in the photomicrograph. What is the most likely diagnosis in this case?
- Elastofibroma
- Metastatic carcinoma
- Neurofibroma
- Nodular fasciitis
- Spindle cell lipoma
Comment Here
Reference: Elastofibroma
A 60 year old man undergoes MRI for staging of biopsy proven lung cancer. Imaging shows bilateral subscapular masses with attenuation similar to adjacent skeletal muscle. Surgical excision is performed and light microscopic appearance is shown in the photomicrograph. Which of the following special stains will help the most in reaching the correct diagnosis?
- Alcian blue
- Elastic stain
- Reticulin stain
- Schiff
- Trichrome
Comment Here
Reference: Elastofibroma
