

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Michal M. EWSR1::SMAD3 positive fibroblastic tumor. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/softtissueesft.html. Accessed April 19th, 2024.
Definition / general
- Recently characterized, locally aggressive fibroblastic mesenchymal tumor with only 15 cases reported so far (Am J Surg Pathol 2018;42:522, Am J Surg Pathol 2018;42:1325, J Cutan Pathol 2021;48:255, Exp Mol Pathol 2019;110:104291, Int J Surg Pathol 2021;29:179)
- Has a characteristic morphology (hypercellular spindled cell merging with hyalinized areas), immunoprofile (strong ERG expression only) and molecular background (defining EWSR1::SMAD3 gene fusion)
Essential features
- Extremely rare, fusion defined, locally aggressive soft tissue tumor
- So far described only on the extremities, with a strong predilection for acral parts
- Wide age range (1 - 68 years); M:F = 1:4
- 2 main components: hypercellular spindled fibroblasts merging with acellular hyalinized areas
- All cases show diffuse strong nuclear expression of ERG, which seems to be very specific in the pertinent differential diagnosis
Terminology
- EWSR1::SMAD3 positive fibroblastic tumor
ICD coding
- No official coding established
Epidemiology
- Extremely rare tumor
- Wide age range (1 - 68 years)
- M:F = 1:4
Sites
- Extremities, particularly acral parts
Pathophysiology
- Gene fusion driven
Etiology
- Unknown
Clinical features
- Small, painless, infiltratively growing tumor located in the dermis / subcutis
- Frequently recurs due to infiltrative growth (4 of 6 cases with follow up recurred)
- May recur many years after initial excision (Am J Surg Pathol 2018;42:1325)
- Malignant variant not described
Diagnosis
- Clinical and morphological features: hypercellular tumor, usually located on the distal extremities, composed of monomorphic bland spindled fibroblasts with minimal mitotic activity merging with acellular hyalinized areas
- Diffuse strong nuclear expression of ERG
- Confirmation of EWSR1 rearrangements in challenging cases
Radiology description
- Ultrasound: subcutaneous hypoechoic nodule (Exp Mol Pathol 2019;110:104291)
- MRI: well demarcated, small nodules with a low signal on T1 weighted image and a high signal on T2 weighted image (Exp Mol Pathol 2019;110:104291)
Prognostic factors
- Negative margin status seems to affect the likelihood of recurrence
Case reports
- 24 year old man presented with a recurrent tumor in the dorsum of his right foot (Exp Mol Pathol 2019;110:104291)
- 27 year old man with multiple peritoneal masses with extension into the retroperitoneum (Case of the Month #516)
- 28 year old woman with EWSR1::SMAD3 positive fibroblastic tumor (Int J Surg Pathol 2021;29:179)
Treatment
- Complete excision seems to be curative
Gross description
- Tumors are small with firm consistency and grayish color (Exp Mol Pathol 2019;110:104291)
Microscopic (histologic) description
- Usually located in the subcutis but dermal examples directly abutting the epidermis have been described (J Cutan Pathol 2021;48:255)
- Nodular or less frequently vaguely lobulated / plexiform growth pattern
- Usually infiltrative growth, sometimes leading to engulfment of the surrounding subcutaneous adipose tissue
- 2 main components: hypercellular spindled fibroblasts gradually merging with acellular hyalinized areas
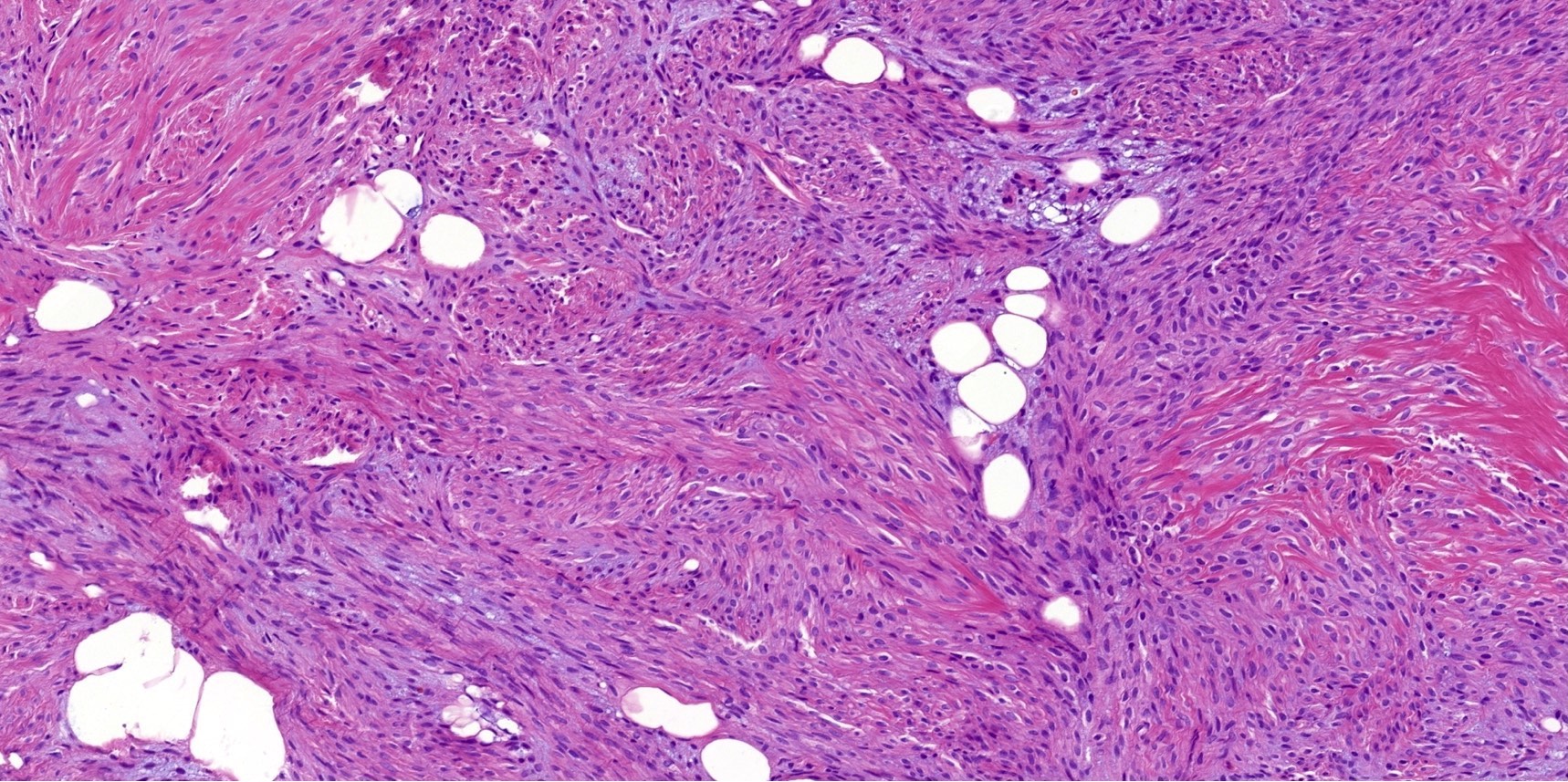
- Spindled cells form hypercellular, well organized fascicles that frequently intersect with each other
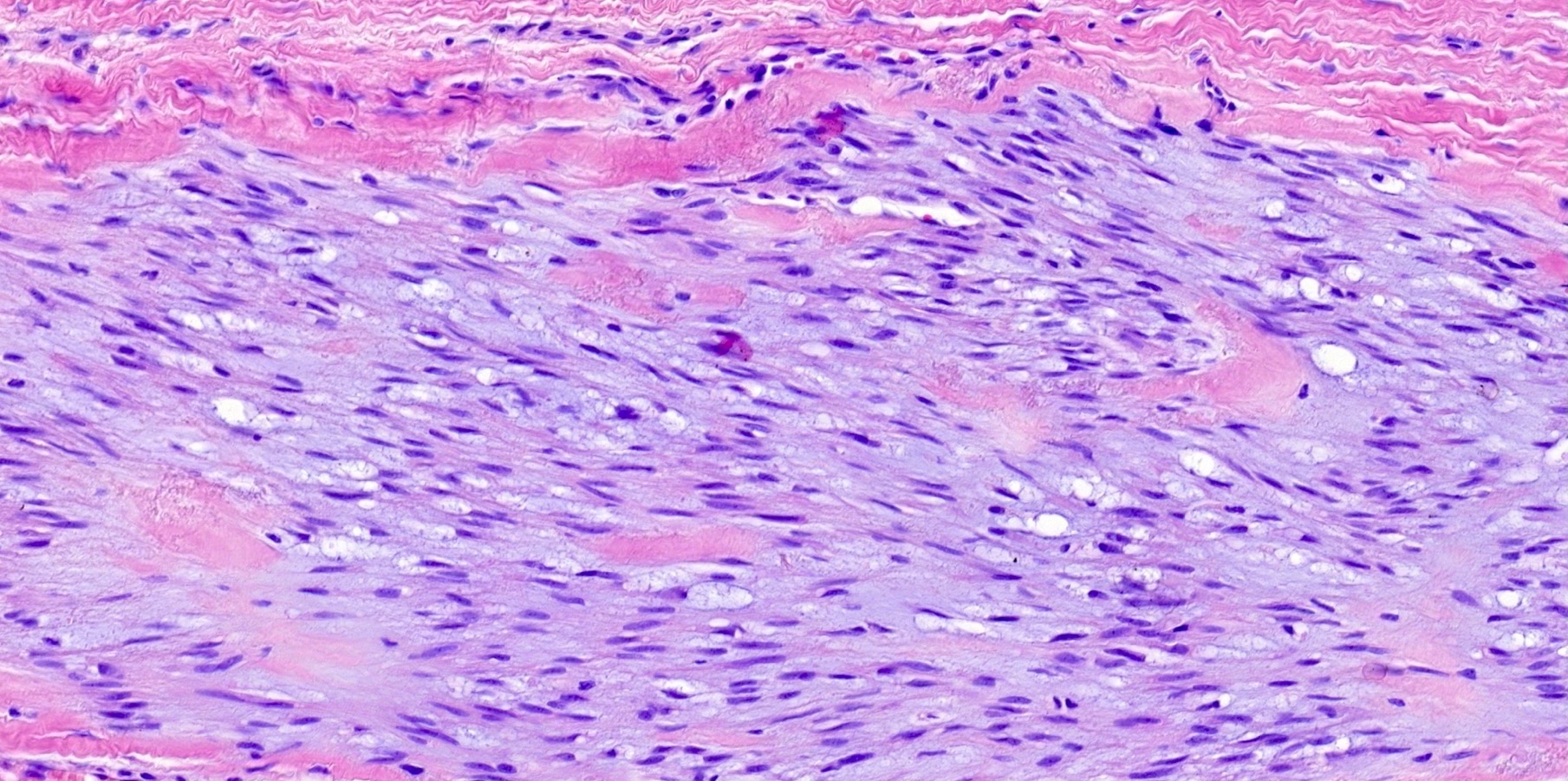
- Spindled cells have relatively uniform, elongated, focally wavy nuclei that are round when observed on a cross section
- Moderate amount of eosinophilic cytoplasm
- Lack of pleomorphism, atypia or mitoses
- Some cases show distinct zonation pattern with a hyalinized center and cellular areas at the periphery; others do not
- Only 1 case showed focal stippled calcifications in the hyalinized area
Microscopic (histologic) images
Contributed by Michael Michal, M.D., Ph.D.
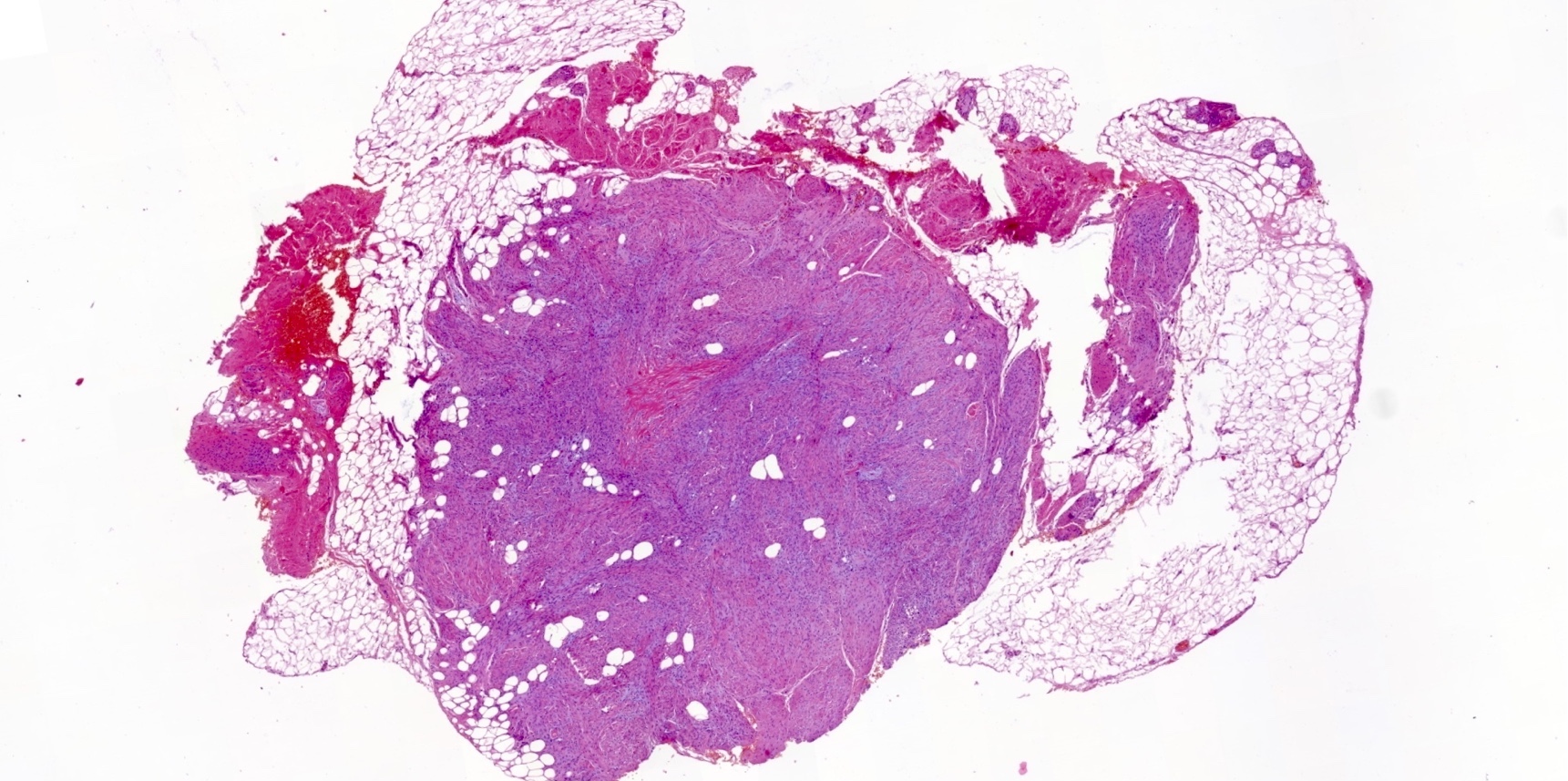
Nodular growth in most cases
Engulfment of surrounding adipose
No pleomorphism, atypia or mitoses
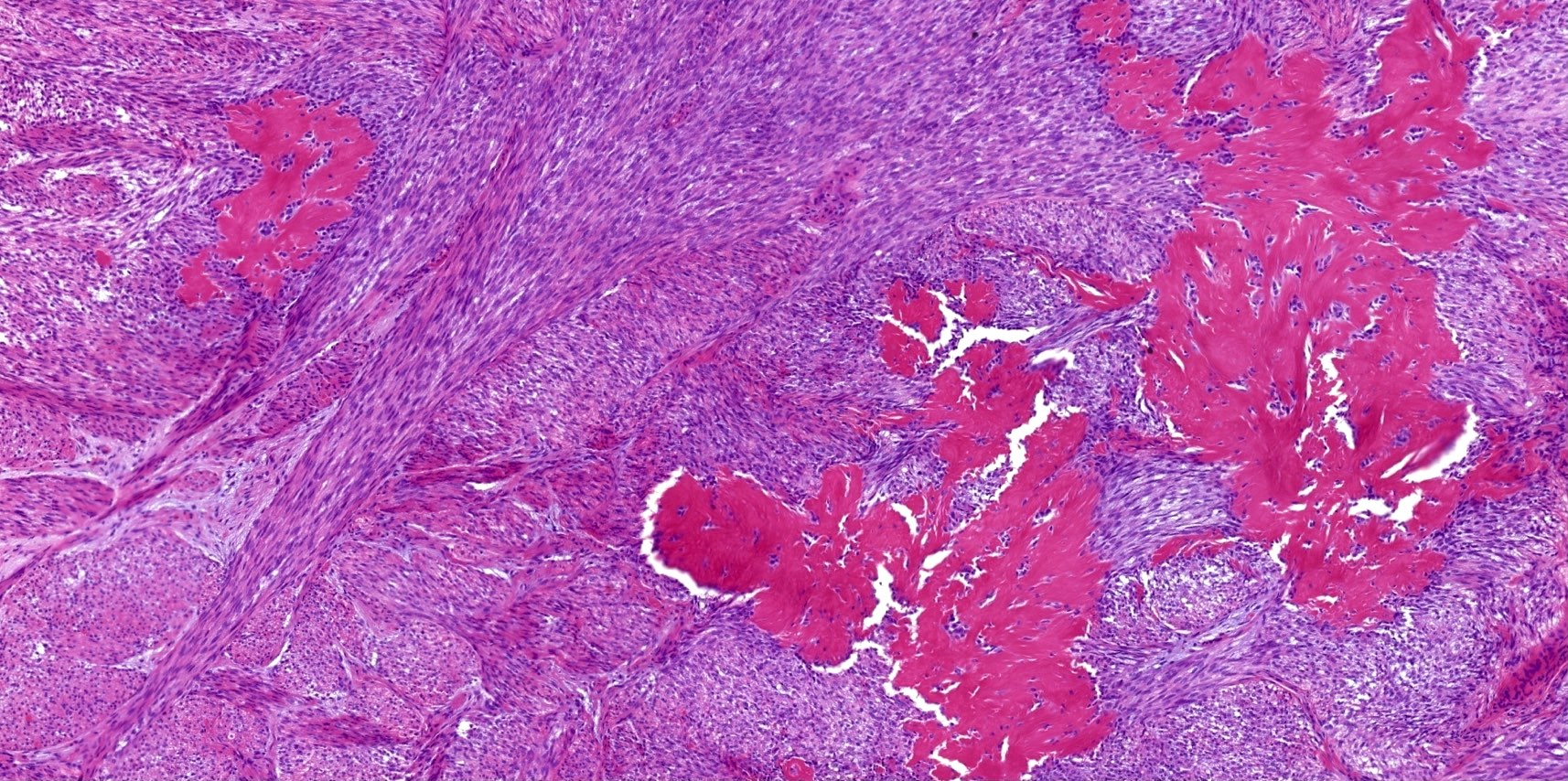
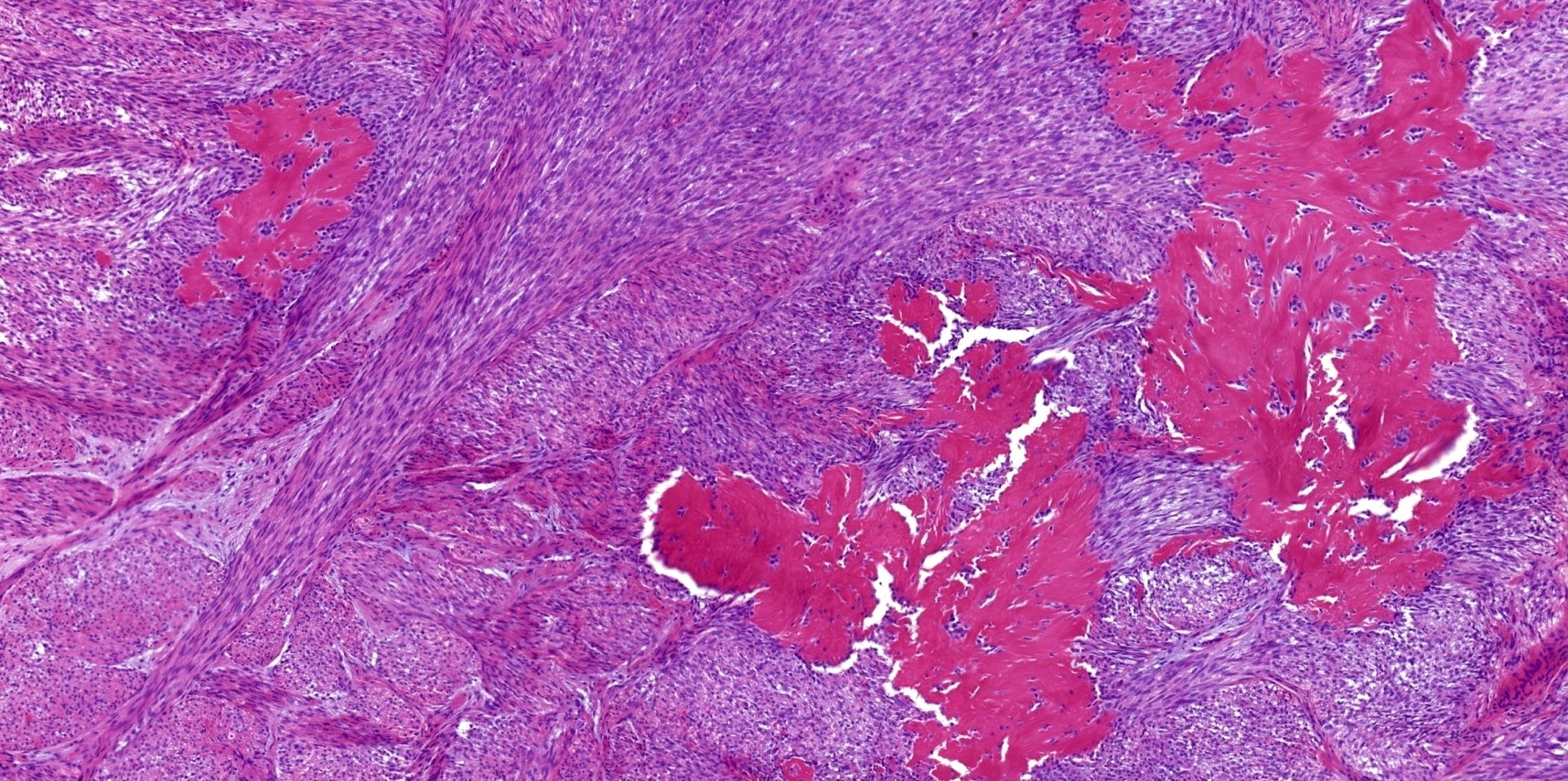
Merging of spindled and hyalinized areas
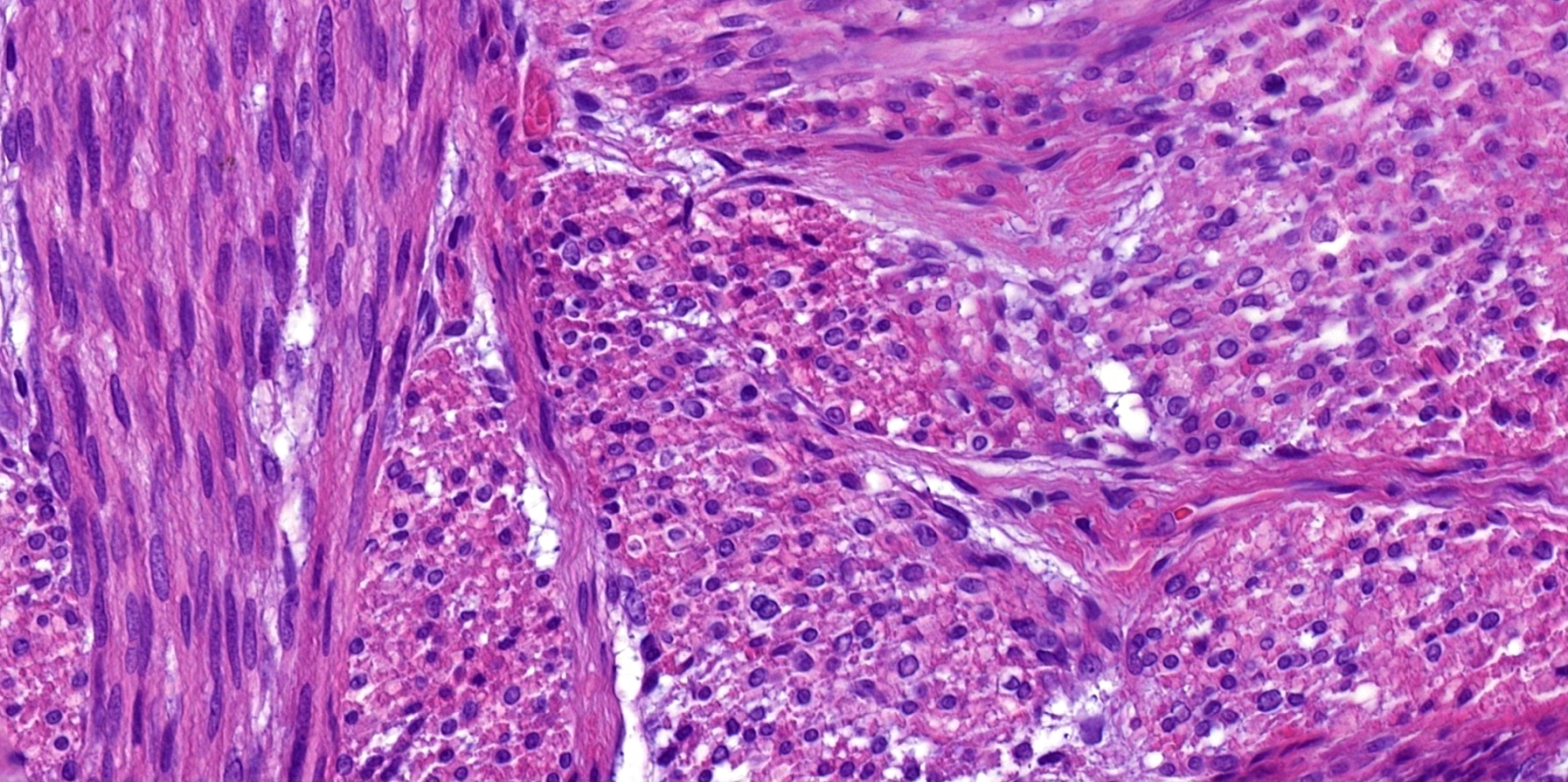
Elongated nuclei, round on cross section
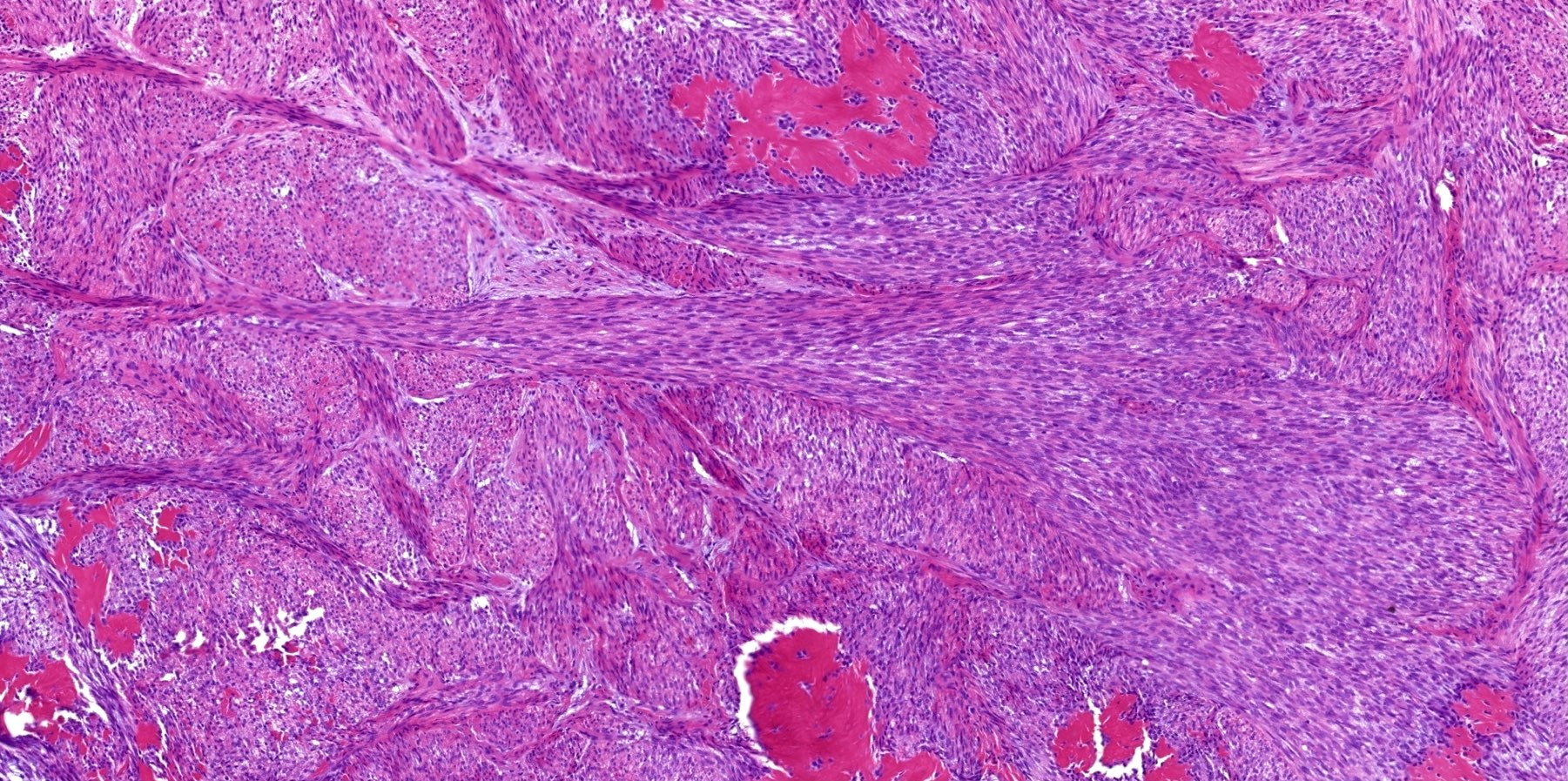
Intersecting hypercellular fascicles
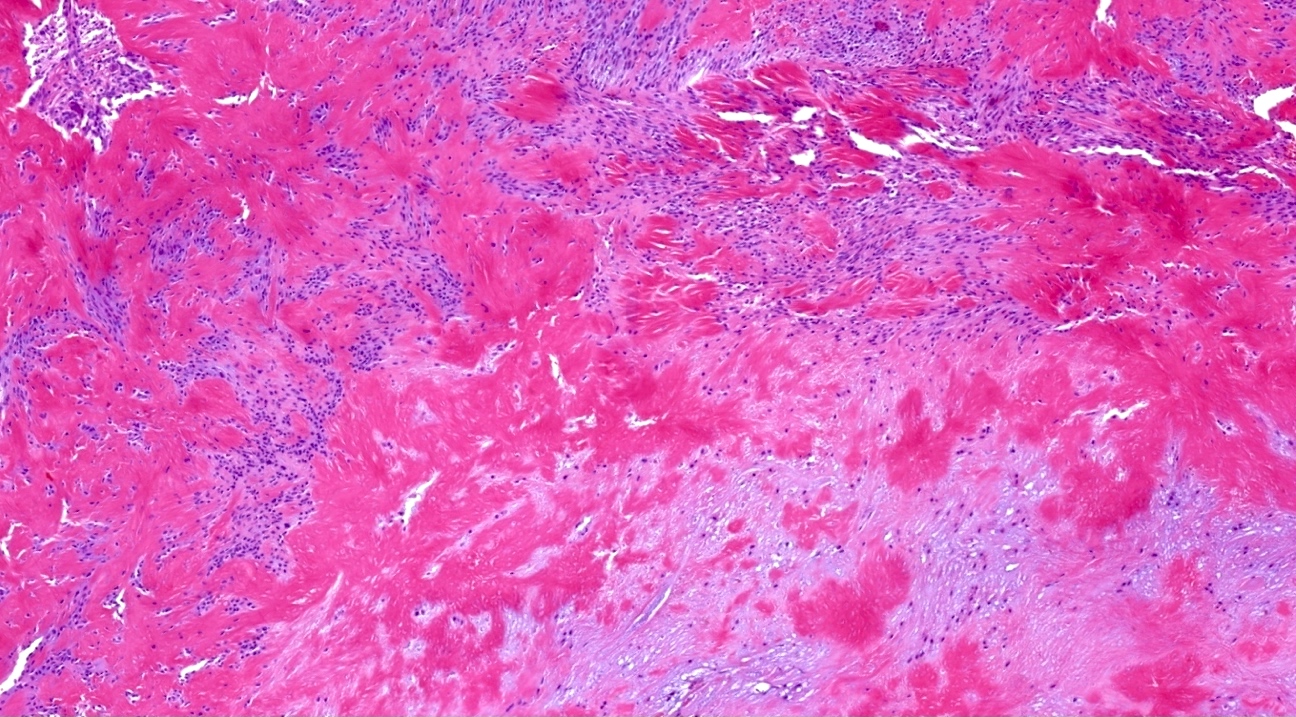
Hyalinized areas
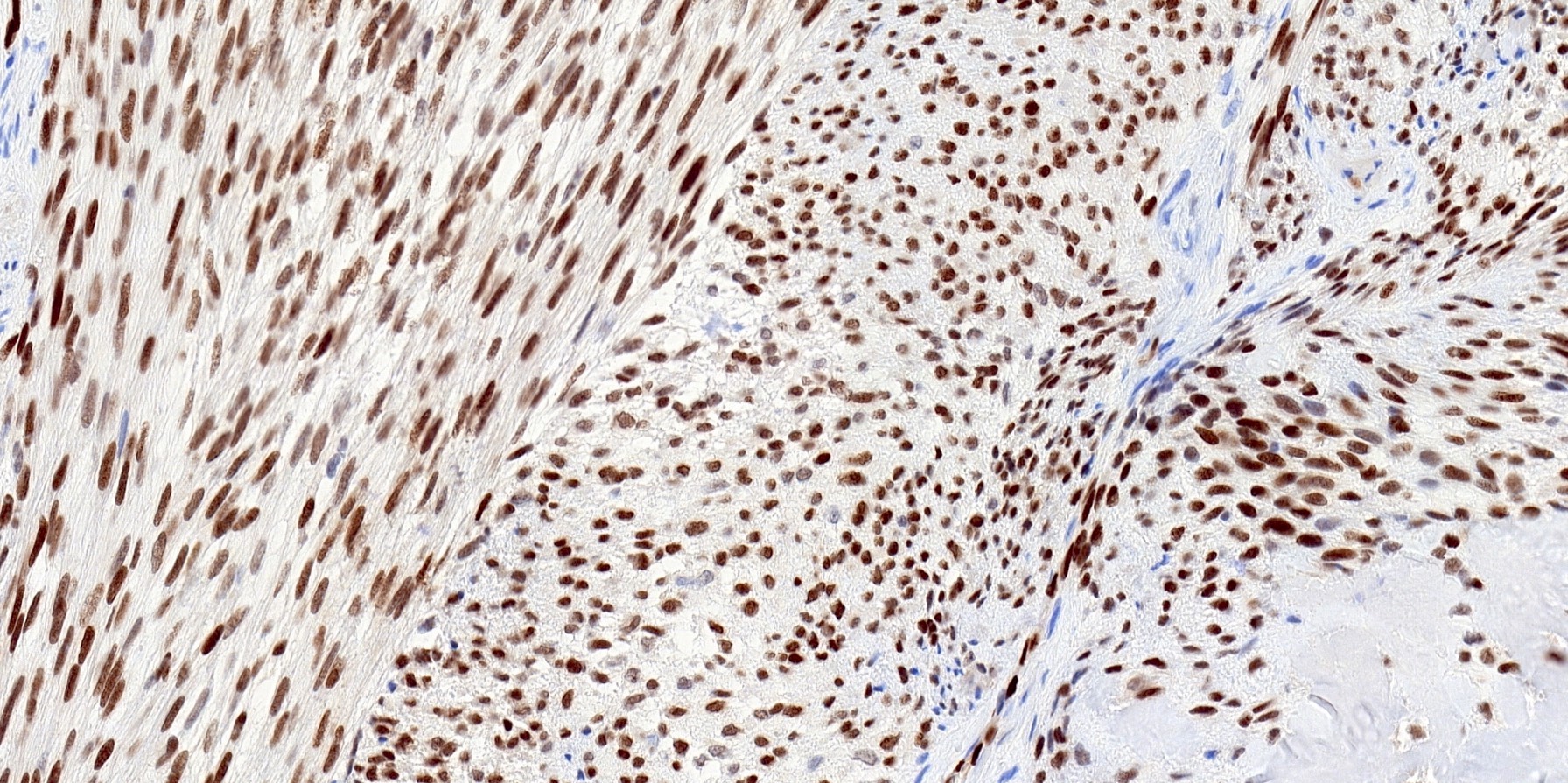
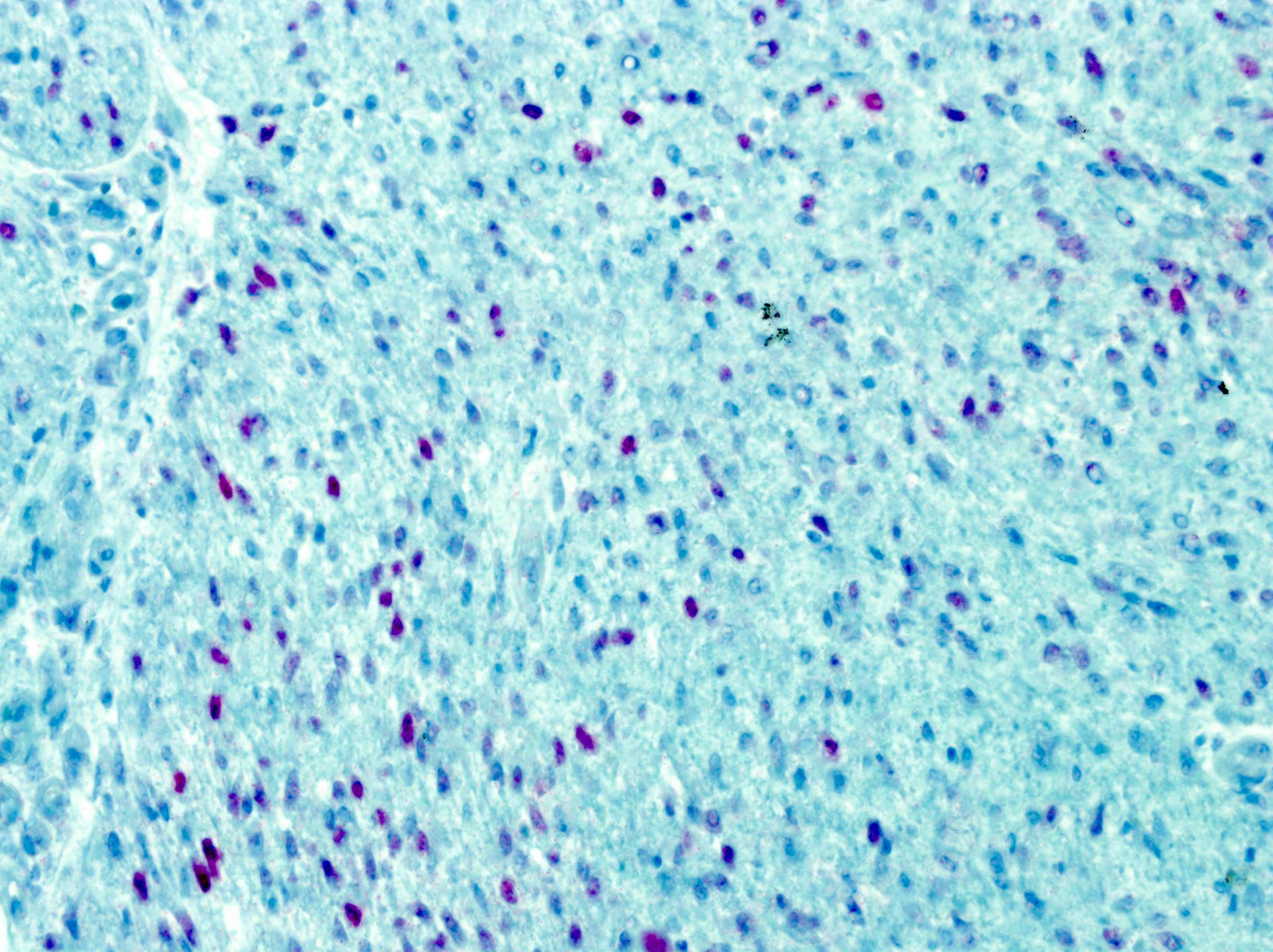
Diffuse ERG
Focal SATB2
Cytology description
- Unknown
Positive stains
- ERG
- All cases show diffuse strong nuclear expression
- This type of ERG expression seems to be very specific in the pertinent differential diagnosis, with the only exception of cellular fibrous histiocytomas, which exhibit a similar staining pattern in most cases (Am J Surg Pathol 2018;42:1325, J Cutan Pathol 2021;48:1003, Am J Clin Pathol 2015;144:A309)
- SATB2
- Focal weak to moderate nuclear staining in no more than 50% of cases
Negative stains
- Factor XIIIa, MSA, desmin, caldesmon, S100, SOX10, CD34
- HMB45, MUC4, pan-TRK, synaptophysin, chromogranin, CD17 and DOG1 tested in only 1 case
- Individual cases weakly expressed SMA, keratins and EMA
- References: Am J Surg Pathol 2018;42:1325, Am J Surg Pathol 2018;42:522, J Cutan Pathol 2021;48:255
Electron microscopy description
- Unknown
Molecular / cytogenetics description
- Defined by recurrent EWSR1::SMAD3 gene fusion
- Exon 7 of EWSR1 (22q12.2) fused to exons 5 or 6 of SMAD3 (15q22.33) (Am J Surg Pathol 2018;42:522, J Cutan Pathol 2021;48:255)
- By unsupervised hierarchical clustering of the whole transcriptome RNAseq data of > 100 various soft tissue tumors, 1 case clustered closely to other pediatric fibroblastic lesions, such as calcifying aponeurotic fibroma, lipofibromatosis and lipofibromatosis-like neural tumor (Am J Surg Pathol 2018;42:522)
Sample pathology report
- Left foot, excision:
- EWSR1::SMAD3 rearranged fibroblastic tumor (see comment)
- Comment: There is a hypercellular proliferation of spindled cells with a large hyalinized area in the center of the lesion. Immunohistochemically the tumor cells have strong nuclear expression of ERG and are negative for SMA, desmin, CD34, S100, OSCAR and EMA. This constellation of morphological and immunohistochemical features strongly supports the diagnosis of EWSR1::SMAD3 rearranged fibroblastic tumor. It is a recently characterized, locally aggressive mesenchymal neoplasm prone to recur unless completely excised. Metastatic spread has not been reported.
Differential diagnosis
- No entity in the pertinent differential diagnosis shows strong and diffuse ERG expression (Am J Surg Pathol 2018;42:1325)
- Cellular fibrous histiocytoma:
- Contains slightly shorter fascicles composed of usually less uniform spindled cells
- Exhibits more prominent storiform pattern and many cases show a characteristic collagen entrapment at the periphery, which is not typically seen in EWSR1::SMAD3 positive fibroblastic tumor
- Most cases express factor XIIIa
- Rearrangements of EWSR1 gene are absent
- Myofibroma:
- Shows plumper spindled cells
- Hemangiopericytoma-like vessels with a pericytic arrangement of the surrounding cells
- Mostly positive with SMA
- Does not have strong and diffuse ERG expression
- Most cases show PDGFRB gene mutation (Am J Surg Pathol 2017;41:195)
- Lipofibromatosis:
- Lacks the prominent hyalinized areas
- Has more abundant fat component that is present throughout the tumor and not only at the periphery
- Tumor cells are oval rather than spindled
- No prominent intersecting of tumor fascicles
- Does not have strong and diffuse ERG expression
- Molecular background characterized by various gene fusions (Mod Pathol 2019;32:423)
- Calcifying aponeurotic fibroma:
- Contains calcifications / chondroid foci rather than hyalinized areas
- Variable and overall lower cellularity
- More haphazard arrangement of the tumor fascicles
- Focal weak ERG expression (Am J Surg Pathol 2018;42:1325)
- Defined by FN1-EGF gene fusion (J Pathol 2016;238:502)
- Lipofibromatosis-like neural tumor:
- Lacks prominent hyalinized areas
- More atypical and hyperchromatic cells
- No prominent intersection of tumor fascicles
- Usually positive for S100 and CD34
- Does not have strong and diffuse ERG expression
- Most cases have NTRK1 gene fusions (those also express NTRK1 by immunohistochemistry), subset shows ALK or ROS1 rearrangement
- Fibromatosis:
- Monophasic synovial sarcoma:
- Much higher mitotic and proliferative indices
- Usually has vaguely epithelioid areas which can be confirmed by immunohistochemistry
- Hemangiopericytomatous vasculature
- Prominent mast cell infiltrate
- Stains with EMA, keratins, TLE1
- Does not have strong and diffuse ERG expression
- Characterized by SYT-SSX gene fusion
- Cutaneous forms of myoepithelioma:
- Significantly different morphologically and immunohistochemically
- Does not have strong and diffuse ERG expression
- May potentially enter the differential due to the EWSR1 gene break as detected by FISH
Board review style question #1
Which of the following is true about EWSR1::SMAD3 rearranged fibroblastic tumor?
- ~50% of cases metastasize
- All cases show diffuse and strong nuclear staining with ERG antibody
- It typically occurs in the head and neck area
- Tumor consists of neoplastic adipose tissue and epithelioid cells
- Tumor has a prominent hemangiopericytoma-like vasculature and chondroid areas
Board review style answer #1
B. All cases show diffuse and strong nuclear staining with ERG antibody
Comment Here
Reference: EWSR1::SMAD3 positive fibroblastic tumor
Comment Here
Reference: EWSR1::SMAD3 positive fibroblastic tumor
Board review style question #2
A 1 year old infant presented with a tumor on her palm. It is negative with the standard soft tissue immunohistochemical panel consisting of SMA, desmin, CD34, S100, OSCAR and EMA. It was additionally negative for NTRK1 immunohistochemistry. Which of the following is most likely the correct diagnosis?
- EWSR1::SMAD3 rearranged fibroblastic tumor
- Fibromatosis
- Lipofibromatosis-like neural tumor
- Monophasic synovial sarcoma
- Myofibroma
Board review style answer #2
A. EWSR1::SMAD3 rearranged fibroblastic tumor
Comment Here
Reference: EWSR1::SMAD3 positive fibroblastic tumor
Comment Here
Reference: EWSR1::SMAD3 positive fibroblastic tumor
