

Soft tissue
Fibroblastic / myofibroblastic
Fibromatosis
Fibromatosis-palmar / plantar
Editorial Board Member: Jose G. Mantilla, M.D.
Deputy Editor-in-Chief: Borislav A. Alexiev, M.D.

Last author update: 28 November 2023
Last staff update: 28 November 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Palmar fibromatosis / plantar fibromatosis
See Review Article: J Pathol Transl Med 2021;55:265
See Also: Peyronie disease
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Frozen section description | Frozen section images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Cytology images | Positive stains | Negative stains | Electron microscopy description | Electron microscopy images | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2 | Board review style question #3 | Board review style answer #3Cite this page: Stewart BD, Nascimento AF. Fibromatosis-palmar / plantar. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/softtissuefibromatosissuperficial.html. Accessed April 25th, 2024.
Definition / general
- Palmar and plantar fibromatosis are benign nodular fibroblastic / myofibroblastic proliferations typically arising in the volar aspect of the hands and fingers or involving plantar aponeuroses, respectively
- Both processes are histologically similar, composed of a bland cellular proliferation of spindle cells with a bluish appearance and with a variable amount of background collagen, depending on the age of the lesion (J Pathol Transl Med 2021;55:265)
Essential features
- Bland, variably cellular proliferation of spindled fibroblasts / myofibroblasts
- Collagenous stroma
- Involvement of aponeurosis and variably subcutis and dermis
- A subset shows nuclear beta catenin expression, despite the absence of CTNNB1 or APC gene mutations (Histopathology 2007;51:509, Mod Pathol 2001;14:695)
Terminology
- Palmar fibromatosis: Dupuytren disease or contracture
- Plantar fibromatosis: Ledderhose disease, morbus Ledderhose
ICD coding
Epidemiology
- Palmar fibromatosis
- Most common type of superficial fibromatosis (1 - 2% of population)
- Prevalence increases with age (~20% of population at age 65)
- M:F = 3 - 4:1
- 50% bilateral
- Most common in northern Europeans
- Rare in Black population
- Most common type of superficial fibromatosis (1 - 2% of population)
- Plantar fibromatosis
- Prevalence not currently understood (Foot Ankle Spec 2018;11:168)
- Middle aged patients
- Several reports of patients < 16 years old to as young as 9 months (J Pediatr Orthop 1997;17:16)
- NIH list of rare diseases (< 200,000 people)
- ~25% bilateral
- M > F (Orthop Res Rev 2018;11:1)
- 2 genetic variants found in genome wide association study suggest a possible genetic predisposition
- 1 indel (chr5:118704153:D) and 1 SNP (rs62051384) (Int J Sports Med 2018;39:314)
Sites
- Palmar fibromatosis
- Metacarpophalangeal joint, the proximal interphalangeal joint or both joints (Hand (N Y) 2011;6:149)
- Plantar fibromatosis
- Most often the medial and central bands of plantar aponeurosis
Pathophysiology
- Palmar fibromatosis
- Proliferation of fibroblasts, their differentiation into myofibroblasts and the production of extracellular matrix
- Proposed roles of fibroblast growth factor (FGF), wingless / integrated (WNT) and transforming growth factor beta (TGFβ) in disease progression (Exp Cell Res 2010;316:2390, Med Hypotheses 2012;78:385, Cell Physiol Biochem 2012;30:927, N Engl J Med 2011;365:307, Ann Plast Surg 2019;83:594)
- Plantar fibromatosis
- Proliferative phase: increased fibroblastic activity and cellular proliferation
- Active phase: nodule formation occurs
- Residual phase: collagen deposition, scar formation and tissue contracture
Etiology
- Palmar fibromatosis
- Unknown (WHO 5th edition)
- May be caused by fibrogenic cytokines (J Hand Surg Br 2005;30:557)
- Associations with diabetes, smoking and repetitive vibrational trauma reported but not validated (WHO 5th edition)
- Plantar fibromatosis
- Unknown (WHO 5th edition) (Foot Ankle Spec 2018;11:168)
- Associations with long term phenobarbital usage for epilepsy, frozen shoulder, smoking, alcohol addiction, diabetes and repeated trauma have not been validated (WHO 5th edition) (Epilepsia 2008;49:1965, Foot Ankle Spec 2018;11:168)
Clinical features
- Palmar fibromatosis
- Often presents with subcutaneous nodules on distal palmar crease
- Puckers overlying skin as it ages
- Causes flexion contracture, most commonly of digits 4 and 5, due to cord-like expansion of digital aponeurotic slips
- Does not involve deep structures (i.e., tendons or skeletal muscle)
- 10% also have plantar disease; 1 - 4% have penile fibromatosis
- Plantar fibromatosis
- 0.5 - 3.0 cm in diameter subcutaneous nodule(s), slow growing and located in the medial or central plantar aponeurosis
- Initially painless but later associated with pain after standing or walking, typically on the medial aspect of the sole (arch)
- Associated with concomitant palmar and penile fibromatoses and keloids
- Usually not associated with contractures (Foot Ankle Int 2018;39:751)
Diagnosis
- Usually clinical; however, occasionally may be a histologic confirmation
Radiology description
- Palmar fibromatosis
- Ultrasound
- Nodules superficial to flexor tendons in superficial fascia
- Early lesions: hypoechoic with hypervascularity
- Chronic lesions: hyperechoic without vascularity (J Ultrason 2012;12:381)
- Magnetic resonance imaging (MRI)
- Subcutaneous nodules
- Typically uniformly low signal intensity on both T1 and T2 (AJR Am J Roentgenol 1993;160:813)
- Ultrasound
- Plantar fibromatosis
- Radiographs usually normal
- Ultrasound
- Better than MRI (Semin Musculoskelet Radiol 2010;14:334)
- Lesion(s) embedded on the plantar fascia
- Less reflective to the much brighter plantar fascia surrounding it with sharp juxtaposition (Semin Musculoskelet Radiol 2010;14:334)
- Hypo to mixed echogenicity
- Discrete, fusiform, multinodular thickening of plantar fascia (AJR Am J Roentgenol 2002;179:1167)
- Comb sign in 51% of cases (J Ultrasound Med 2018;37:2725)
- Alternating linear bands of hypoechogenicity and isoechogenicity relative to the plantar fascia
- MRI
- Nodules appear as focal, oval shaped areas of disorganization embedded in plantar fascia (Semin Musculoskelet Radiol 2010;14:334)
- T1: iso to low signal (compared to muscle)
- T2: low to intermediate signal (AJR Am J Roentgenol 2002;179:1167, Radiographics 2000;20:333)
Radiology images
Contributed by Mark R. Wick, M.D.
Plantar fibromatosis
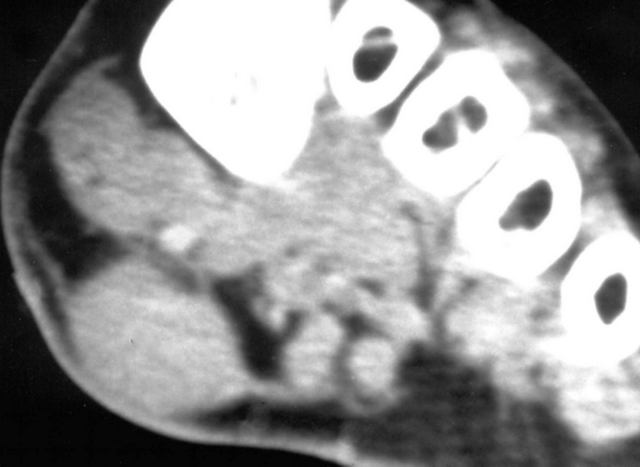
CT of heel
Images hosted on other servers:
Palmar fibromatosis


Ultrasound
MRI
Palmar and plantar fibromatosis

Axial T1 weighted MRI
Prognostic factors
- Palmar fibromatosis
- Worse in White men with a strong family history, bilateral involvement, severe disease and ectopic manifestations (BMJ 2006;332:397)
- Plantar fibromatosis
- Worse with bilateral involvement, multiple nodules and a positive family history (Foot (Edinb) 2017;31:31)
Case reports
- Palmar fibromatosis
- 59 year old woman with bilateral Dupuytren contractures of the thumb interphalangeal joints (J Plast Reconstr Aesthet Surg 2012;65:1738)
- 65 year old man with hand flexion contracture (BMJ 2014;349:g6137)
- 82 year old man with heterotopic ossification in Dupuytren disease (J Bone Joint Surg Br 2011;93:1676)
- Plantar fibromatosis
- 28 year old Brazilian woman with 6 year history of painless bilateral plantar nodules (J Clin Aesthet Dermatol 2010;3:45)
- 30 year old man presented with painful bilateral plantar nodules (Surg J (N Y) 2016;2:e102)
- 51 year old woman with giant bilateral plantar fibromatosis (Int J Dermatol 2018;57:365)
- 54 year old man with nodular swelling of the right plantar arch (Diagn Interv Imaging 2014;95:893)
- 64 year old woman with osseous metaplasia in a case of plantar fibromatosis (J Foot Ankle Surg 2004;43:430)
Treatment
- Palmar fibromatosis
- Observation, excision or incision of contracture band
- Often recurs
- Surgical treatment is necessary if the contracture results in functional disability and the total flexion deformity is > 30° (Plast Reconstr Surg 2017;139:240e)
- Collagenase (clostridial collagenase histolyticum) (Plast Reconstr Surg 2017;139:240e, Ir J Med Sci 2020;189:529, Foot Ankle Spec 2018;11:168)
- Plantar fibromatosis
- Conservative measures should be used prior to recommending surgery (Orthop Res Rev 2018;11:1)
- Observation, surgery if symptomatic; complete fasciectomy has fewer recurrences (0 - 50%) than local excision (57 - 100%) and wide excision (8 - 80%) (Plast Reconstr Surg 2008;122:486, Foot Ankle Spec 2018;11:168, Orthop Res Rev 2018;11:1)
- Wide excision: 2 - 3 cm margin
- Several nonoperative treatments with variable scientific support (Orthop Res Rev 2018;11:1)
- Steroid injections
- Verapamil
- Radiation therapy
- Extracorporeal shock wave therapy
- Tamoxifen
- Collagenase
Clinical images
Contributed by Brian D. Stewart, M.D.
Palmar fibromatosis
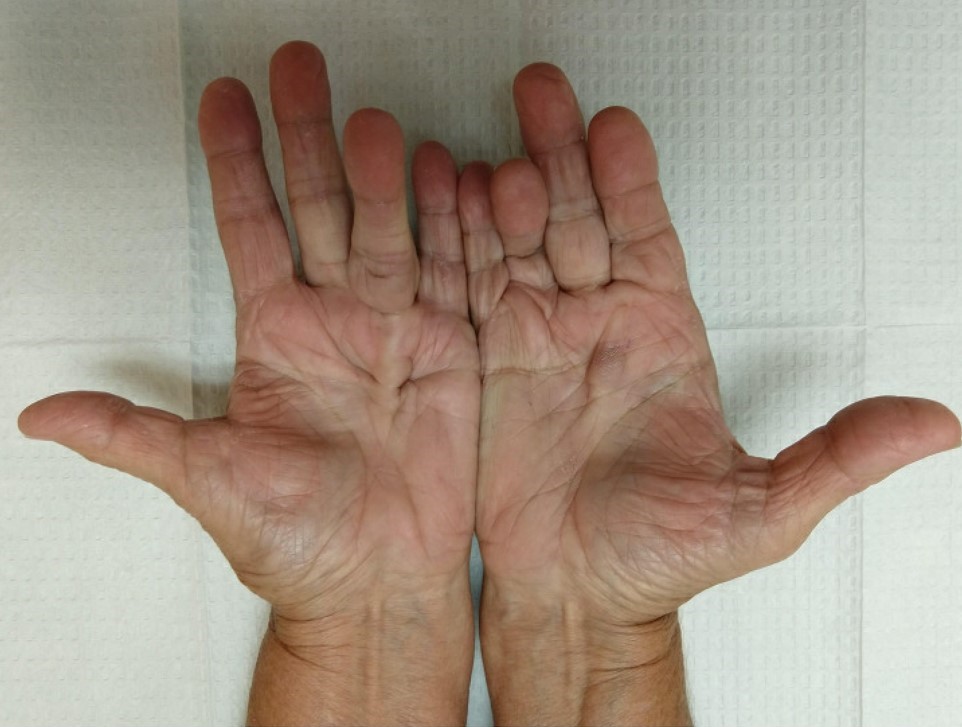

Nodules and contractures

Excision of contraction band

Postoperative improvement
Gross description
- Palmar fibromatosis
- Small nodules or nodular masses associated with aponeurosis and subcutaneous fat with gray-yellow-white cut surface (color depends on collagen content)
- Plantar fibromatosis
- 2 - 3 cm nodules associated with aponeurosis and subcutis with gray-yellow-white cut surface (color depends on collagen content)
- Reference: Weiss: Enzinger and Weiss's Soft Tissue Tumors, 7th Edition, 2019
Gross images
Contributed by Brian D. Stewart, M.D.
Palmar fibromatosis

Excised contraction band
Frozen section description
- Same as Microscopic (histologic) description but immaturity of the fibroblasts is less evident (blue staining is less intense)
Frozen section images
Contributed by Brian D. Stewart, M.D.
Plantar fibromatosis
Spindle cell proliferation
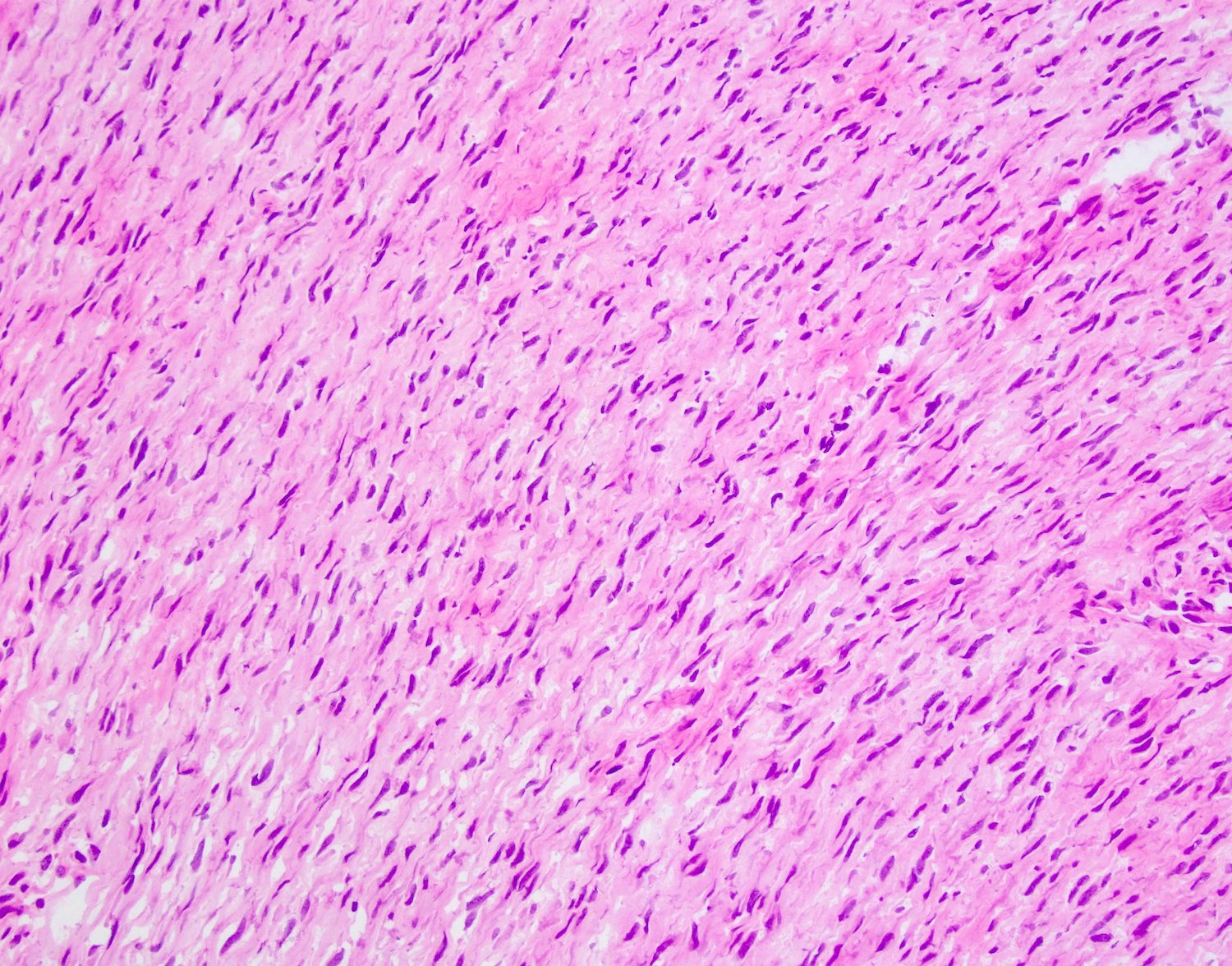
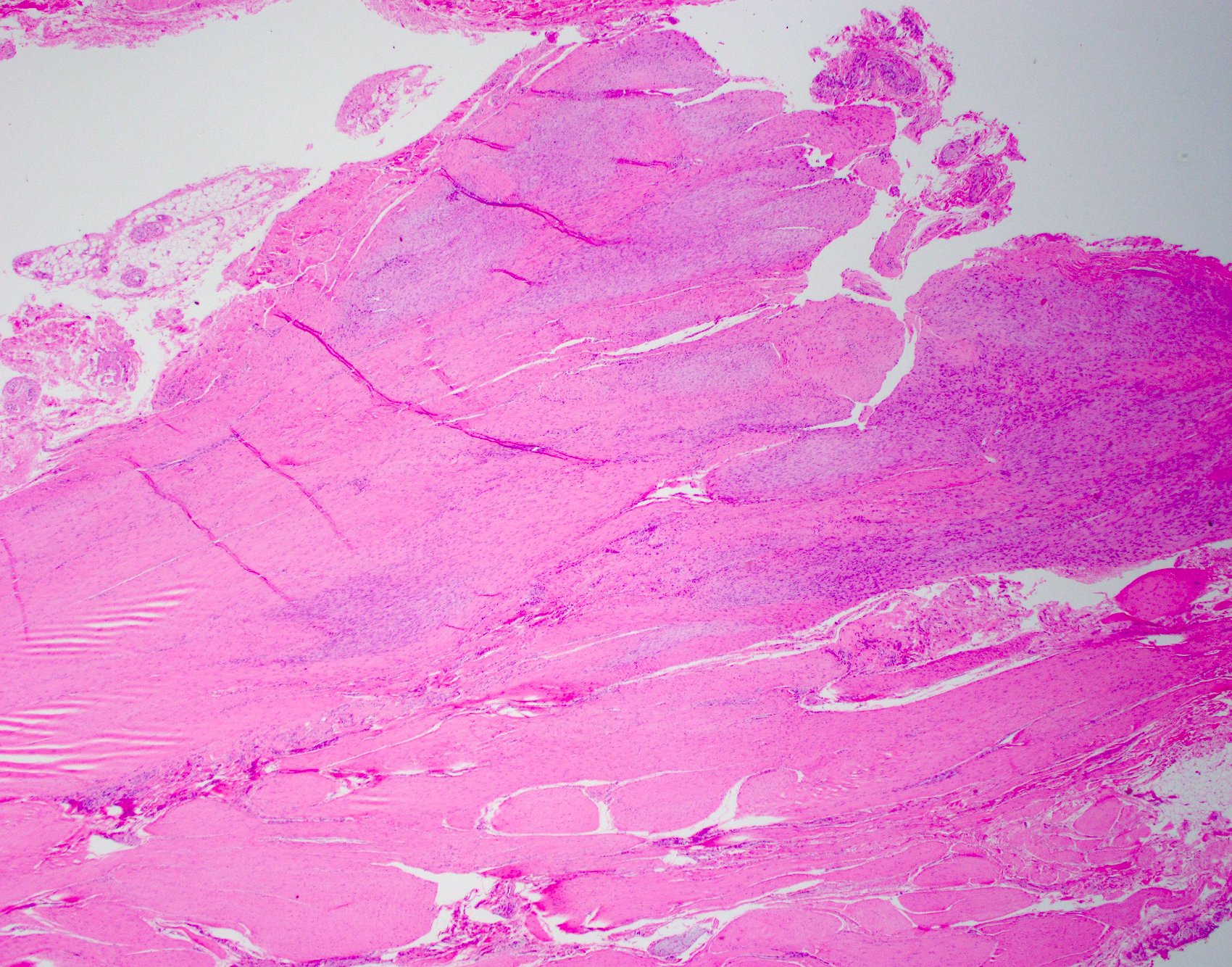
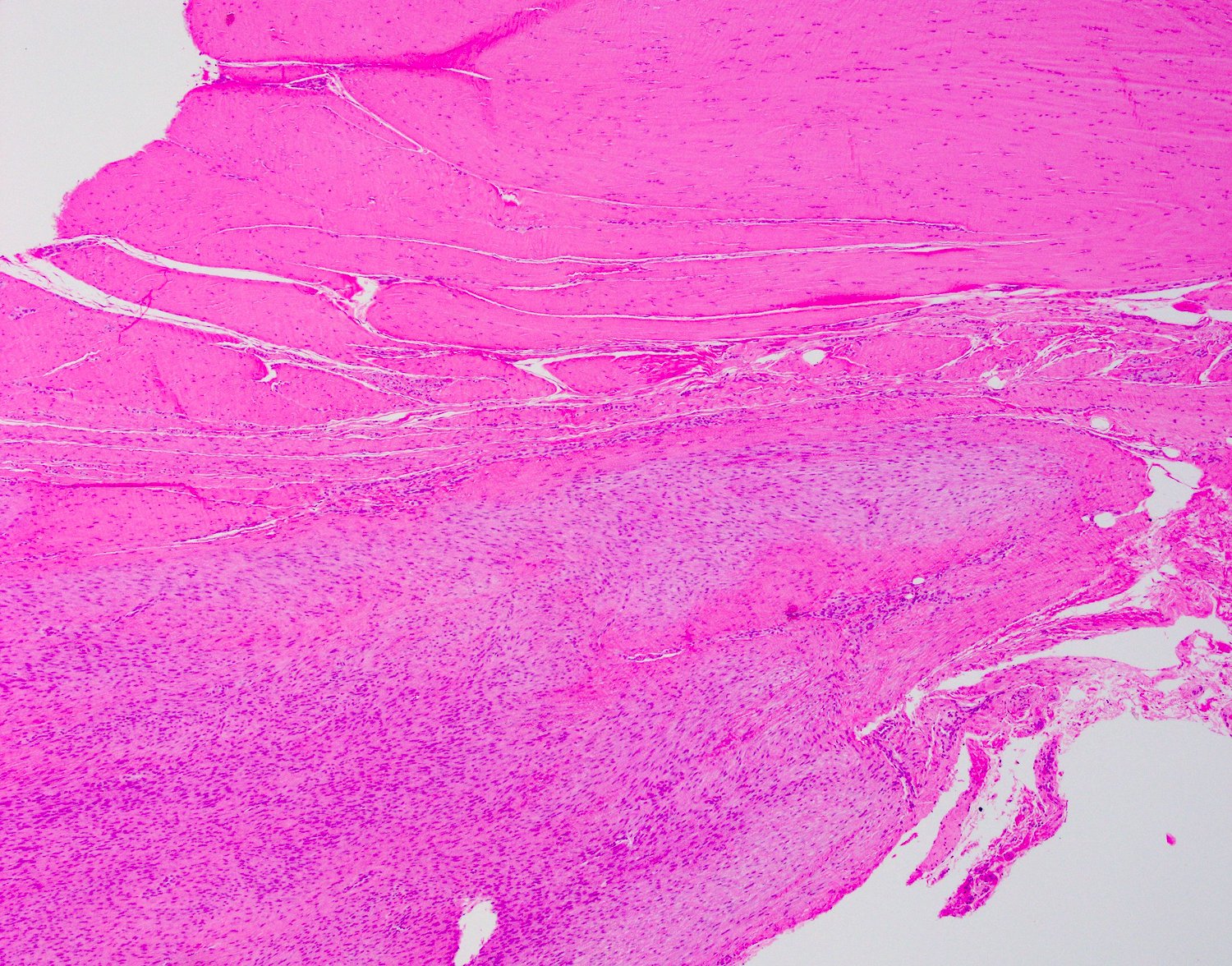
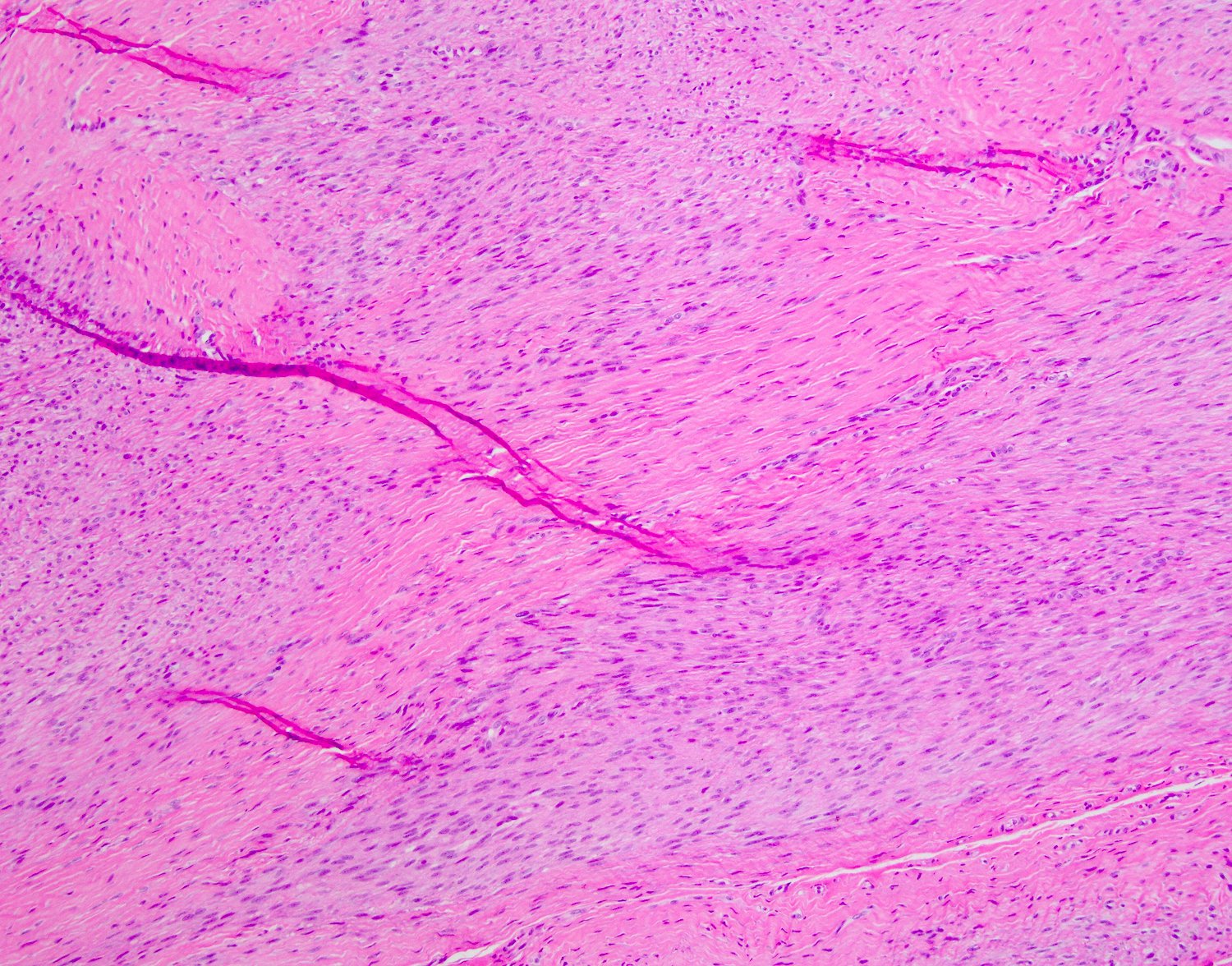
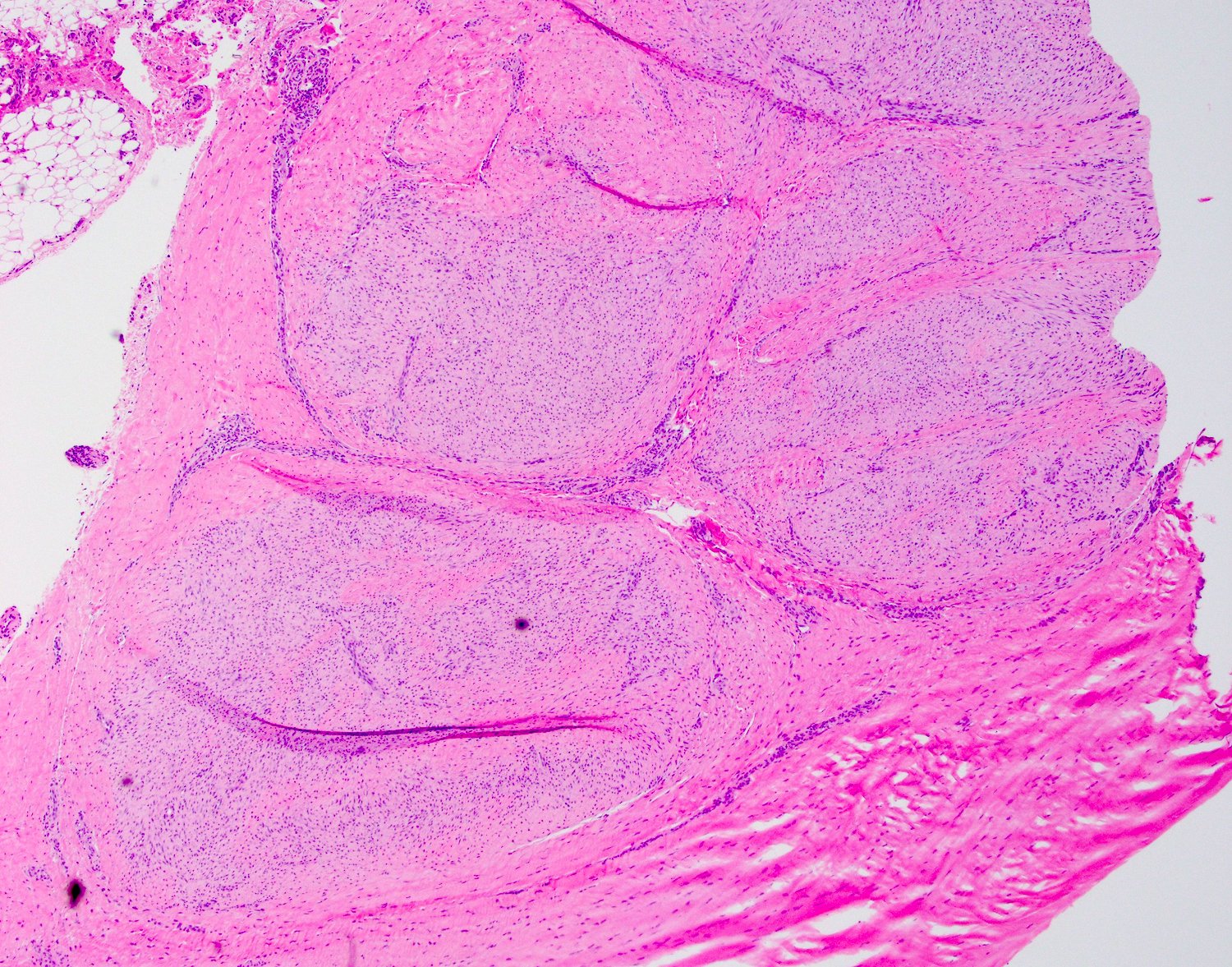
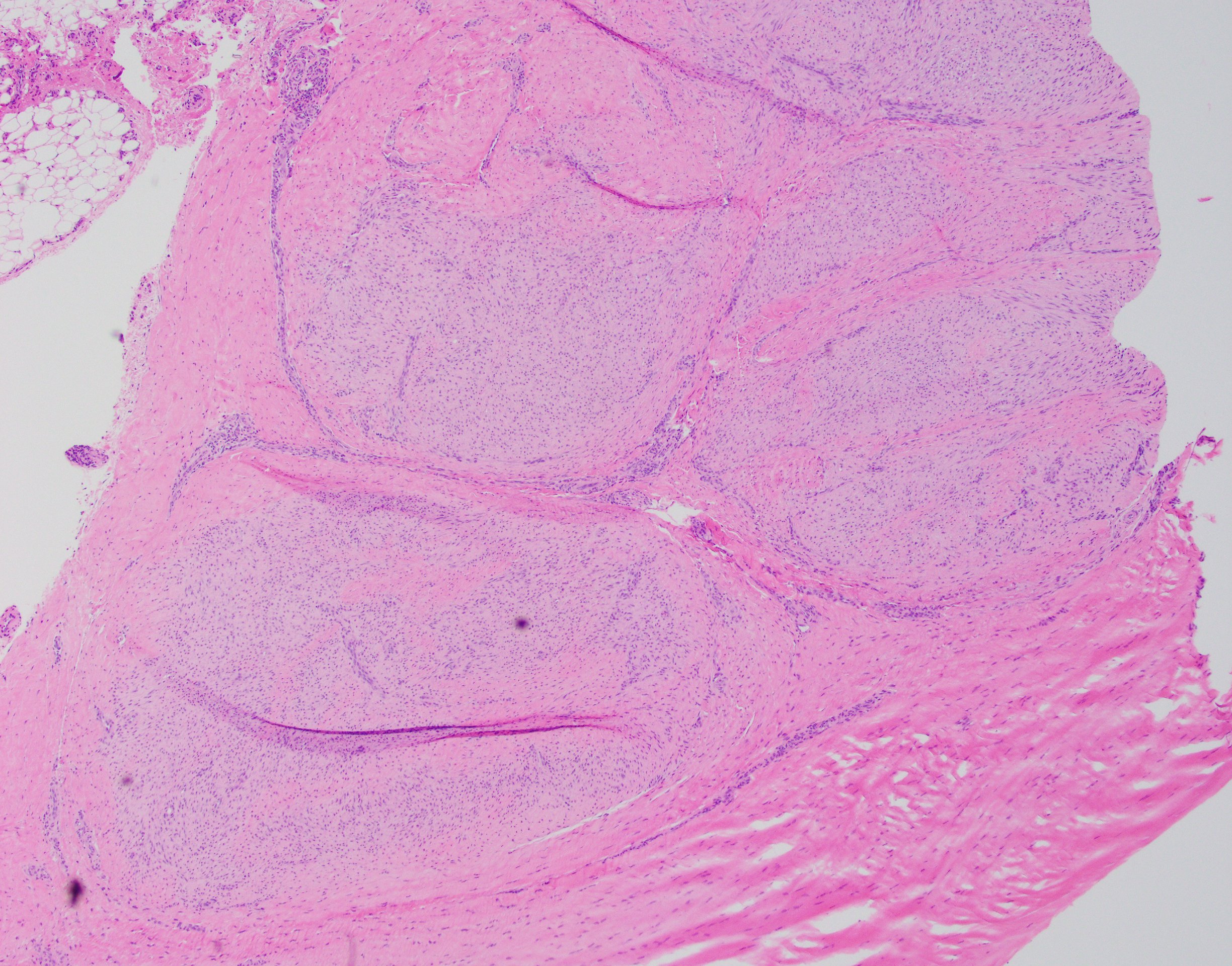
Microscopic (histologic) description
- Both processes are histologically similar
- Typically, tumors involve a thickened palmar / plantar aponeurosis and form single or multiple discontinuous, moderately cellular spindle cell nodules in a collagenous stroma (Am J Surg Pathol 2005;29:1095)
- Morphologically, there are 3 phases of growth (proliferative, involutional and late stage)
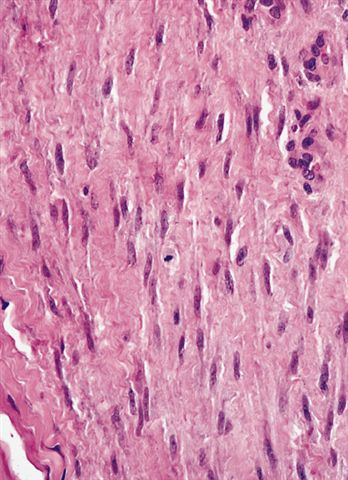
- Proliferative phase
- Cellular, parallel fascicles of bland, plump, relatively uniform spindled fibroblasts with tapering nuclei, vesicular chromatic and small or inconspicuous nucleoli, with minimal stromal collagen
- Some plantar lesions are hypercellular and can mimic spindle cell sarcomas but they lack atypia
- Scattered chronic inflammation and occasional typical mitotic figures, especially in early lesions
- Mitotic activity may be prominent in pediatric patients
- Occasional, particular plantar lesions show interspersed multinucleated cells (Am J Surg Pathol 2002;26:244)
- Late stage
- Increase collagenous matrix and decreased cellularity
- Proliferative phase
- Reference: WHO 5th edition
Microscopic (histologic) images
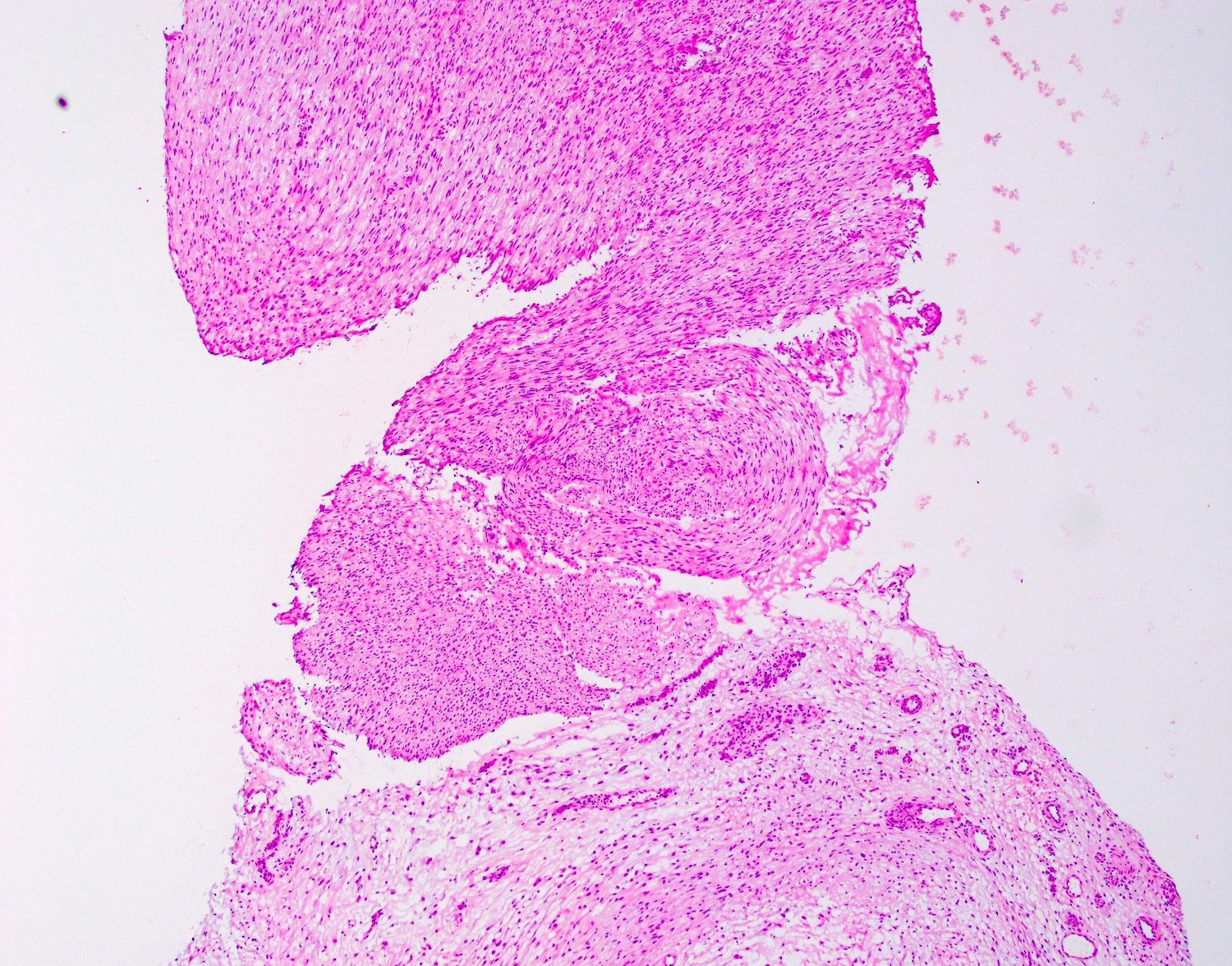
Contributed by Brian D. Stewart, M.D. and AFIP
Palmar fibromatosis
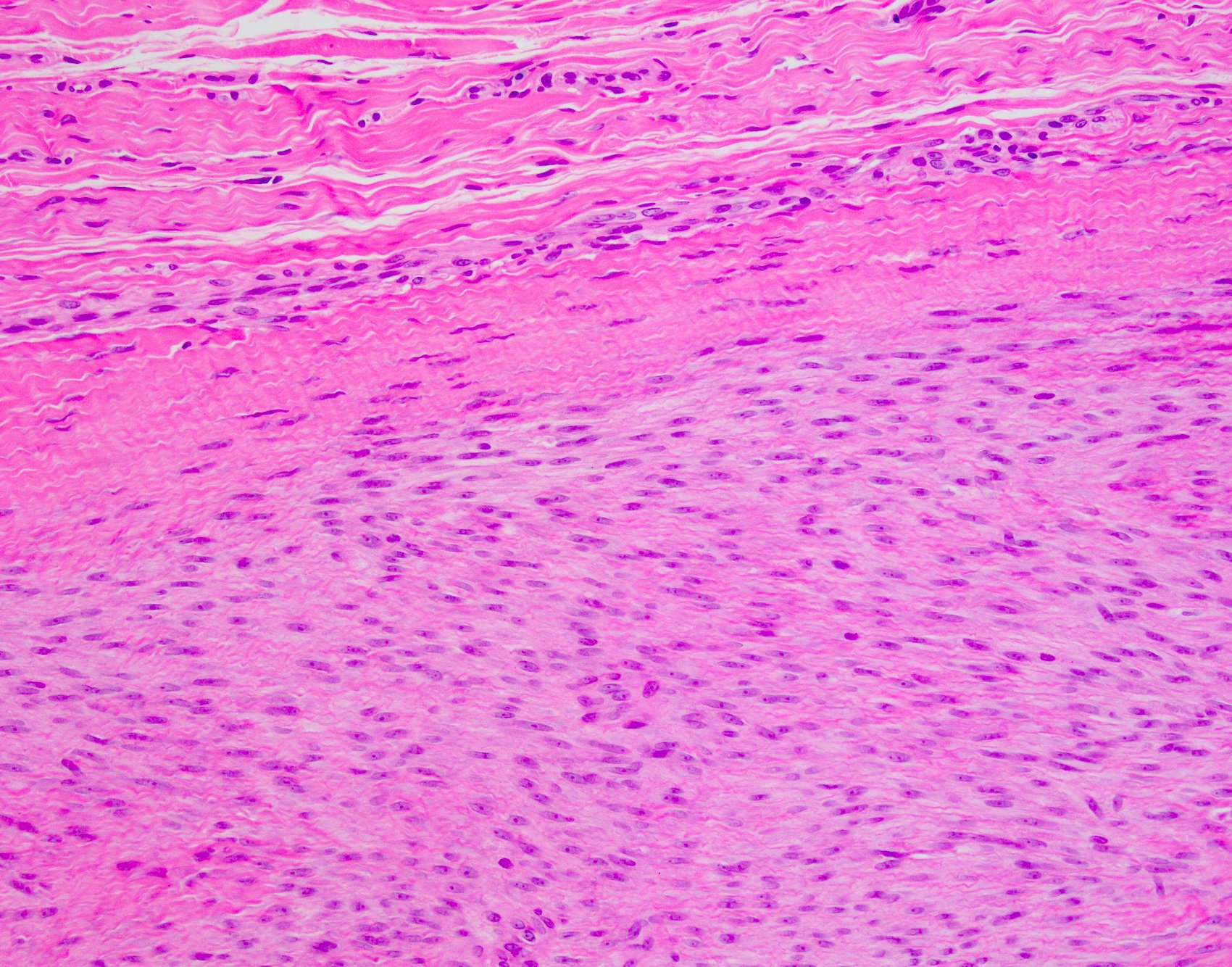
Fibroblastic proliferation
Fibroblastic nodules
Fibroblastic nodule
Tendinous infiltration
Infiltrates an aponeurosis
Mitotic figures
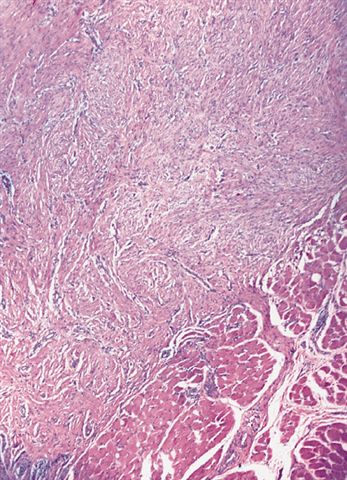
Plantar fibromatosis
Nodular proliferation
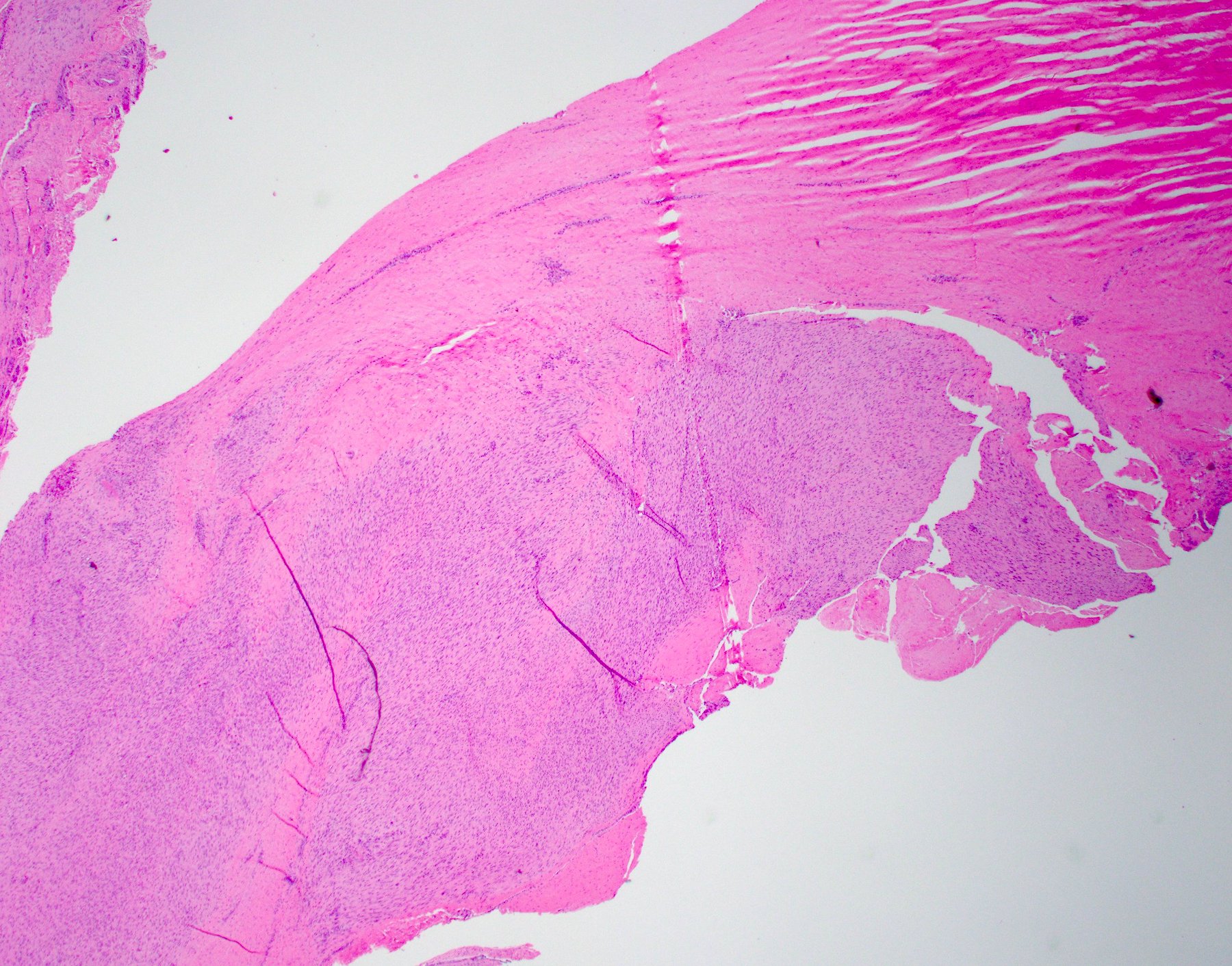
Plantar aponeurotic infiltration
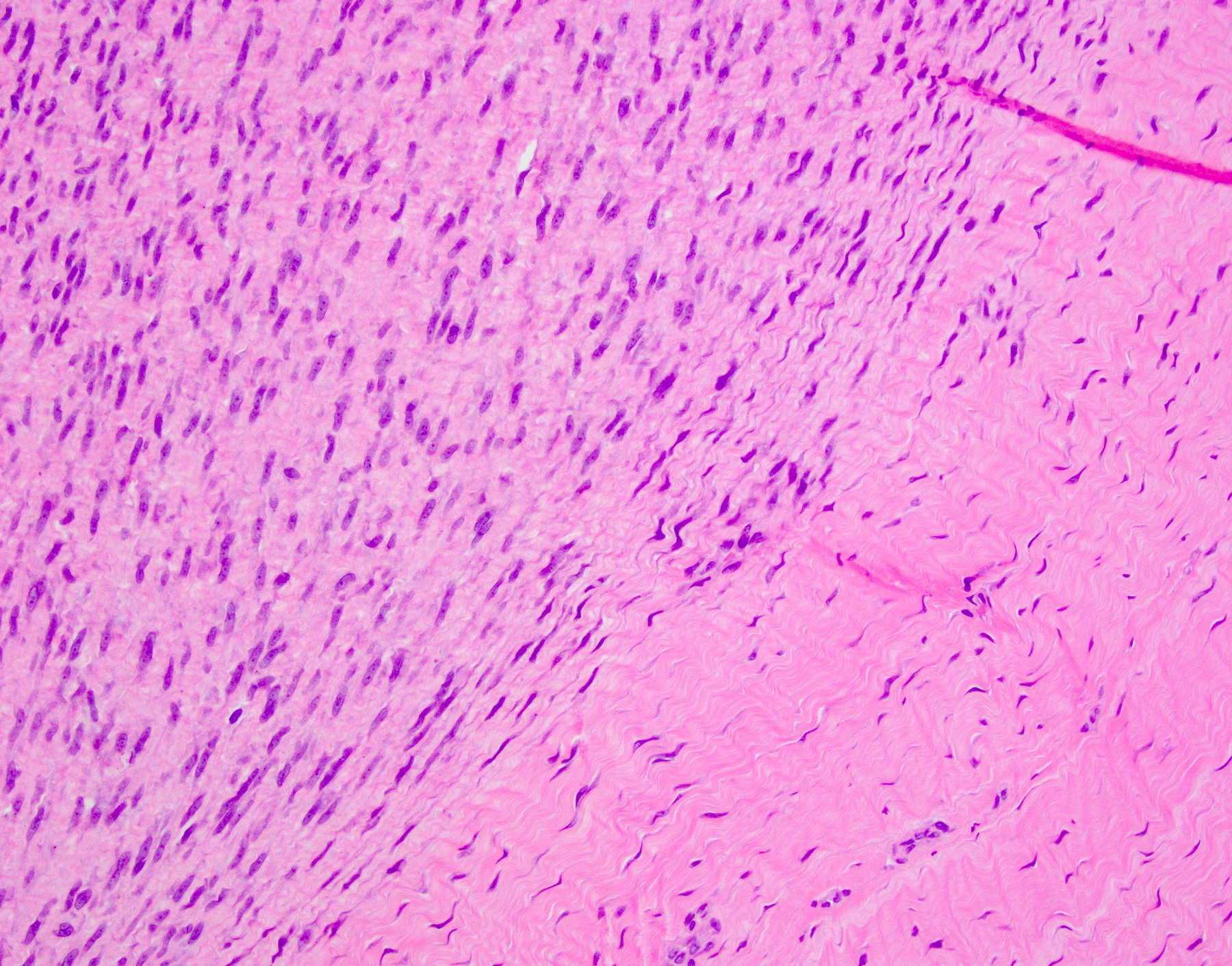
Demarcation from plantar fascia
Virtual slides
Images hosted on other servers:

Male with 6 month history of palm nodule
Cytology description
- Usually limited to touch preps during rare frozen sections (Acta Cytol 1993;37:323)
- Low cellularity, clusters of bland spindle cells with oval to elongated nuclei, no atypical features, rare or absent mitotic activity
Cytology images
Contributed by Brian D. Stewart, M.D.
Plantar fibromatosis
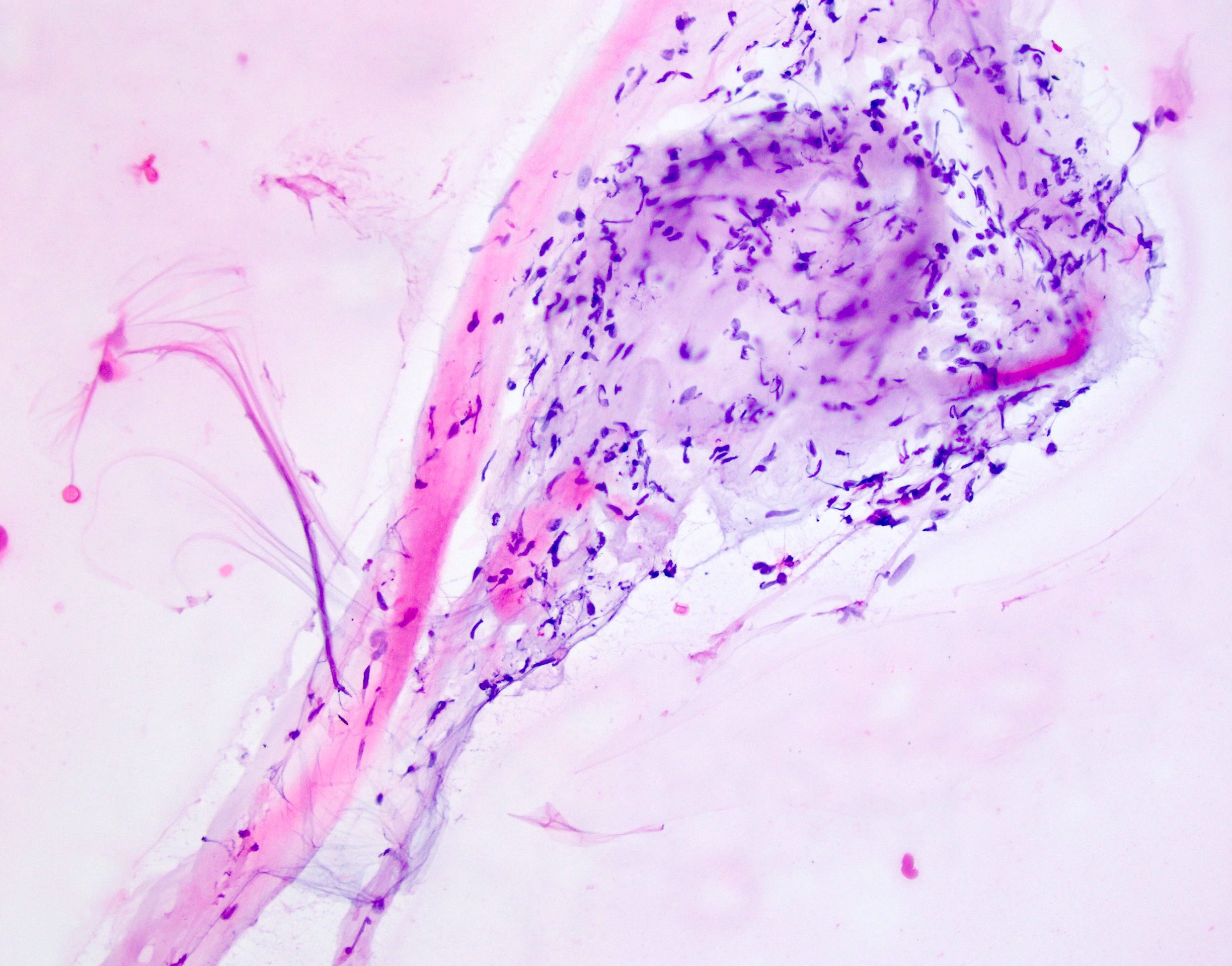
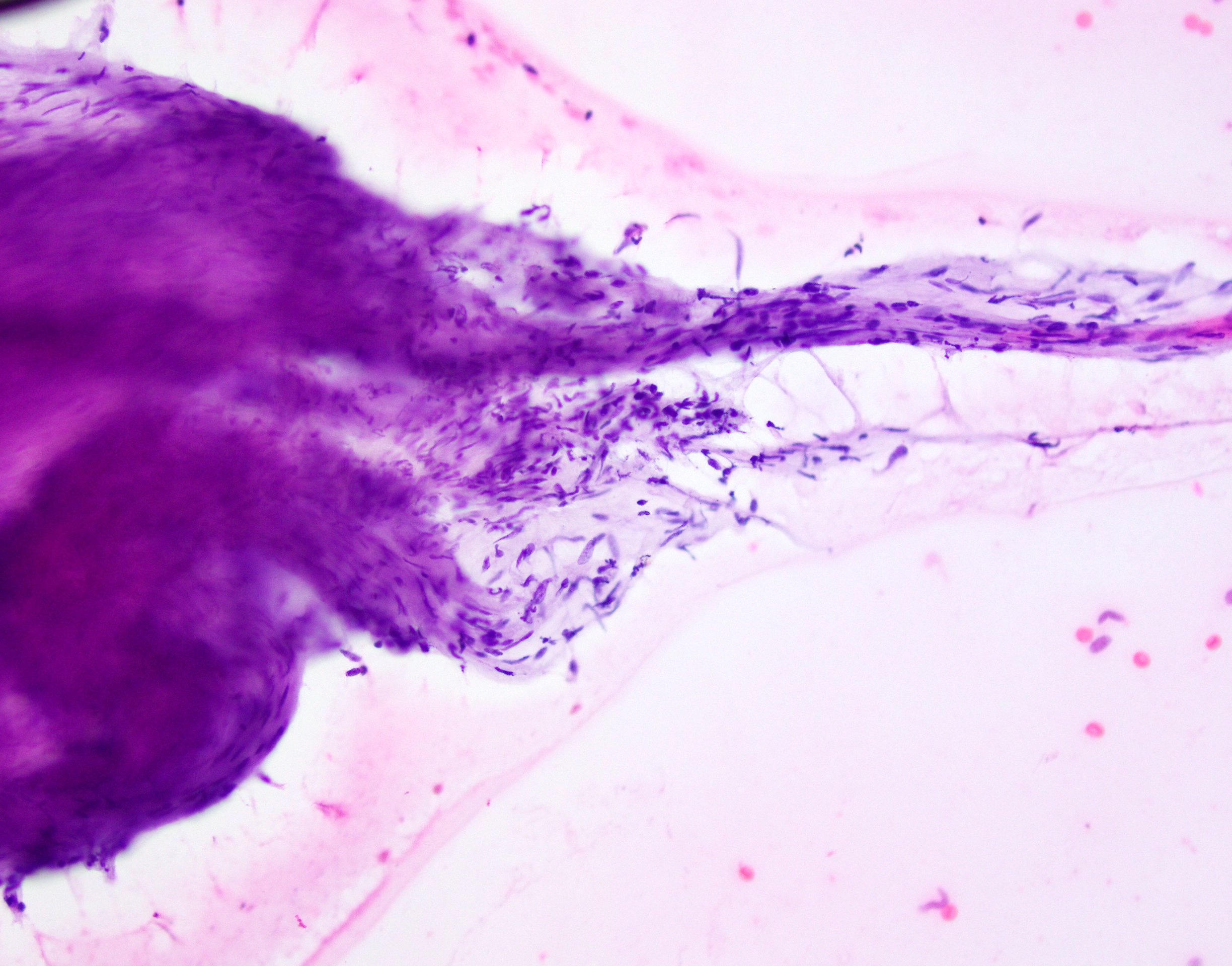
Touch prep
Positive stains
- Palmar fibromatosis
- Usually not necessary to perform due to characteristic histology
- Vimentin, variable actin - muscle specific and smooth muscle actin, less frequently desmin
- Aberrant nuclear expression of beta catenin common (Mod Pathol 2001;14:695, Histopathology 2007;51:509)
- Plantar fibromatosis
- Vimentin, variable actin - muscle specific and smooth muscle actin, less frequently desmin
Negative stains
- Palmar fibromatosis
- Plantar fibromatosis
- Reference: Weiss: Enzinger and Weiss's Soft Tissue Tumors, 7th Edition, 2019
Electron microscopy description
- Fibroblasts and myofibroblasts
Electron microscopy images
Images hosted on other servers:

Fibroblast
Molecular / cytogenetics description
- The tumor lacks the CTNNB1 and APC mutations characteristic of desmoid fibromatosis (Histopathology 2007;51:509, Mod Pathol 2001;14:695)
- Palmar fibromatosis
- Near diploid, often +7 or +8, no gene amplifications or deletions (Cancer Genet Cytogenet 2008;183:6)
- Loss of Y chromosome (Mod Pathol 2000;13:1080)
- Usually considered reactive, not neoplastic (J Transl Med 2006;4:21)
- Aberrations in Wnt signaling pathway but no somatic mutations of beta catenin genes, unlike desmoid fibromatosis (N Engl J Med 2011;365:307, Plast Reconstr Surg 2012;129:921, Joint Bone Spine 2012;79:7, Mod Pathol 2001;14:695)
- Plantar fibromatosis
- Near diploid, often +7 or +8; no somatic mutations of beta catenin genes, unlike desmoid fibromatosis (Mod Pathol 2001;14:695)
- Trisomy 8 and 14 (Cancer Genet Cytogenet 1999;108:176)
- Reciprocal t(2;7)(p13;p13) (Cancer Genet Cytogenet 2005;158:67)
Videos
Plantar fibromatosis
Sample pathology report
- Soft tissue, hand nodule, excision:
- Palmar fibromatosis (Dupuytren contracture) (see comment)
- Comment: Sections show a variably cellular proliferation of spindled fibroblasts and myofibroblasts without atypia set within a collagenous stroma, morphologically consistent with palmar fibromatosis (Dupuytren contracture).
- Soft tissue, foot nodule, excision:
- Plantar fibromatosis (see comment)
- Comment: Sections show a variably cellular proliferation of spindled fibroblasts and myofibroblasts without atypia set within a collagenous stroma, morphologically consistent with plantar fibromatosis.
Differential diagnosis
- Palmar fibromatosis
- Spindle cell sarcomas (i.e., synovial sarcoma, malignant peripheral nerve sheath tumor, etc.)
- Desmoid type fibromatosis:
- Rare in hand
- Dominant mass infiltrates skeletal muscle
- Epithelioid sarcoma:
- Epithelioid sarcoma commonly presents in the hand but cells will show a distinctive epithelioid appearance with abundant eosinophilic cytoplasm (J Pathol Transl Med 2021;55:265)
- Central necrosis or hyalinization is often seen
- Epithelioid sarcoma is characteristically reactive for cytokeratins and CD34 and shows a loss of nuclear staining for SMARCB1 (INI1)
- Plantar fibromatosis
- Clinical differential without nodules: calcaneal stress fracture, tarsal tunnel syndrome, plantar fasciitis (Orthop Res Rev 2018;11:1)
- Clinical differential with nodules: melanoma, synovial sarcoma, Kaposi sarcoma
- Calcifying aponeurotic fibroma:
- Plump or epithelioid fibroblasts palisading around cartilage and spotty calcification
- Desmoid type fibromatosis:
- Rare in feet
- Infiltrates skeletal muscle
- > 3 cm
- Often beta catenin+
- Spindle cell sarcomas (i.e., synovial sarcoma, malignant peripheral nerve sheath tumor, etc.):
- Monophasic synovial sarcoma:
- Uniformly hypercellular
- Often staghorn vascular pattern or ropy collagen
- Patchy keratin or EMA
- Rearrangement of SS18
- Malignant peripheral nerve sheath tumor:
- Monophasic synovial sarcoma:
Additional references
- WHO Classification of Tumours Editorial Board: Soft Tissue and Bone Tumours, 5th Edition, 2020, eMedicine: Dupuytren Contracture [Accessed 14 August 2023], Wikipedia: Dupuytren's Contracture [Accessed 14 August 2023], J Am Acad Orthop Surg 2011;19:746, Wikipedia: Plantar Fibromatosis [Accessed 14 August 2023], eMedicine: Plantar Fibromatosis [Accessed 14 August 2023]
Board review style question #1
Which of the following is true about the disease pictured in this photomicrograph of a painful nodule on the sole of the foot?
- Associated with similar processes in other body sites
- Beta catenin will show diffuse nuclear reactivity, confirming the diagnosis
- Most common in adolescents
- Most common in the central and lateral portions of the foot
- t(x;18) is pathognomonic
Board review style answer #1
A. Associated with similar processes in other body sites. Plantar fibromatosis is associated with similar processes in other body sites. Answer B is incorrect because beta catenin usually shows nuclear reactivity in palmar fibromatosis but not in plantar fibromatosis. Answers C and D are incorrect because plantar fibromatosis is most common in the medial and central bands of the plantar aponeurosis and in middle aged patients. Answer E is incorrect because synovial sarcoma has a pathognomonic t(x;18).
Comment Here
Reference: Palmar / plantar fibromatosis
Comment Here
Reference: Palmar / plantar fibromatosis
Board review style question #2
Which statement about plantar fibromatosis is correct?
- Associated with diabetes
- Bilateral in 5% of cases
- Often cured without recurrence after excision
- Synonymous with plantar fasciitis
- Usually rapidly growing
Board review style answer #2
A. Associated with diabetes. Plantar fibromatosis has been shown to have an association with diabetes. Answer B is incorrect because plantar fibromatosis is bilateral in about 25% of cases. Answer C is incorrect because recurrence is common after excision. Answer D is incorrect as plantar fasciitis is inflammation of the ligament itself and does not form nodules; it is part of the differential diagnosis of plantar fibromatosis. Answer E is incorrect because plantar fibromatosis is usually slow growing.
Comment Here
Reference: Palmar / plantar fibromatosis
Comment Here
Reference: Palmar / plantar fibromatosis
Board review style question #3
Which of the following stains may be positive in palmar or plantar fibromatosis although not specific?
- CD34
- CD56
- DOG1
- Keratin
- Smooth muscle actin
Board review style answer #3
E. Smooth muscle actin is the correct answer as it is reactive in many spindle cell proliferations and is not specific. Answers A - D are incorrect as all of these markers are negative in palmar and plantar fibromatosis.
Comment Here
Reference: Palmar / plantar fibromatosis
Comment Here
Reference: Palmar / plantar fibromatosis
