

Soft tissue
Vascular
Benign
Intramuscular angioma


Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed search: Intramuscular hemangioma
See also: Hemangioma
- Benign vascular neoplasm arising within skeletal muscle, accompanied by variable amount of adipose tissue
- Variable admixture of arteries, veins, lymphatics of cavernous / capillary or mixed type of vessels
- Prominent intralesional adipose tissue and infiltrative growth pattern
- Complete excision is the recommended treatment as recurrence rate is high; therefore, a comment on resection margin is essential
- Degenerated entrapped skeletal muscle fibers may mimic malignancy due to nuclear hyperchromasia
- Intramuscular hemangioma
- Intramuscular infiltrating angiolipoma (not recommended)
- ICD-O: 9132/0 - intramuscular hemangioma
- ICD-11: 2E81.0Y & XH0553 - neoplastic hemangioma of other specified site & intramuscular hemangioma
- Wide age range
- Up to 90% of cases in adolescents and young adults (Histopathology 1991;18:53)
- M = F
- Deep soft tissues of lower extremities > head and neck region > upper limbs > trunk (Stockman: Diagnostic Pathology - Vascular, 1st Edition, 2015)
- Any muscle can be involved, even myocardium (Pediatr Cardiol 2010;31:868)
- Unknown
- Likely represents true neoplasms (particularly capillary type), contrary to the previous reports suggesting these lesions are congenital vascular malformations (Goldblum: Enzinger and Weiss’s Soft Tissue Tumors, 7th Edition, 2019)
- Unknown
- Evidence to suggest an association with trauma is not significant (Goldblum: Enzinger and Weiss’s Soft Tissue Tumors, 7th Edition, 2019)
- Pain is a commonly encountered symptom, particularly in the extremities after exercise (Sports Health 2013;5:448)
- Slow growing nodular swelling in more superficial areas like head and neck, with variable skin discoloration
- Rare presentation with limited functionality, when located near large joints (Medicine (Baltimore) 2019;98:e14343)
- Requires high level of suspicion and characteristic radiological findings, especially on vascular imaging modalities (color Doppler, CT and MR angiography), along with diagnostic histopathological features
- Plain Xray:
- Not the preferred imaging modality
- May show high density shadows in soft tissues (J Int Med Res 2020;48:300060520966897)
- Helpful in visualizing phleboliths (Int J Environ Res Public Health 2021;18:9088)
- Ultrasound: variable hyperechoic or hypoechoic appearance (Rom J Morphol Embryol 2016;57:521, Ann Maxillofac Surg 2021;11:148)
- Computed tomography: shows hypervascular lesions and helps in assessing the extent within soft tissues (Clin Exp Otorhinolaryngol 2015;8:298)
- Magnetic resonance imaging:
- Most important technique
- Isointense on T1, hyperintense on T2 and contrast enhanced T1
- Intralesional fat is hyperintense on T1 (Singapore Med J 2020;61:122)
- Enhanced susceptibility weighted angiography (ESWAN):
- Newer technique
- Helps in subtyping capillary, cavernous and mixed intramuscular angiomas preoperatively, based on the variability in blood flow (Acta Radiol 2021 Dec 17 [Epub ahead of print])
- Digital subtraction angiography (DSA): helps to locate the feeding vessels (Medicine (Baltimore) 2019;98:e14678)
Images hosted on other servers:

Nonhomogeneous arm mass

Hypoechogenic right parapharyngeal mass

Medial rectus lesion

Gluteus medius lesion

Phleboliths, right foot

Multilobulated mass, right foot

Phlebolith, biceps mass

Lobulated calf mass

Fast flow phenomenon, shoulder lesion

Right buccal mass
- Benign with no risk of malignant transformation
- Incomplete excision is the most important factor in local recurrence (30 - 50%) (Clin Orthop Relat Res 2007;459:186, Sports Health 2013;5:448)
- Local recurrence is also determined by size of tumor
- Multiple recurrences can cause disfigurement (Medicine (Baltimore) 2017;96:e5939)
- 14 year old boy with right hand deformity (Medicine (Baltimore) 2017;96:e5939)
- 16 year old girl, a softball player, presented with right shoulder lump (Curr Sports Med Rep 2022;21:42)
- 18 year old woman with painful mass in left foot (Int J Surg Case Rep 2020;77:682)
- Man in early 20s with swelling at right angle of mouth (BMJ Case Rep 2016;2016:bcr2013201457)
- 60 year old woman with sudden onset posterior neck pain (Medicine (Baltimore) 2020;99:e21741)
- Complete surgical excision with clear margins is the recommended treatment
- Preoperative embolization reduces preoperative bleeding (Clin Exp Otorhinolaryngol 2015;8:298)
- Conservative management (with corticosteroids, sclerotherapy, etc.) sometimes works, depending on the individual case (Sports Health 2013;5:448)
Images hosted on other servers:

Asymmetrical right lateral neck swelling

Right masseter swelling

Abductor hallucis mass
- Size range: 1 - 29 cm; mean size: 6.5 cm
- Irregular, ill defined, soft, multilobulated mass (Int J Environ Res Public Health 2021;18:9088)
- May show solid to hemorrhagic cut surface with thrombosis of vascular channels
- Yellowish appearance, based on amount of adipose tissue present
Contributed by Nasir Ud Din, M.B.B.S.
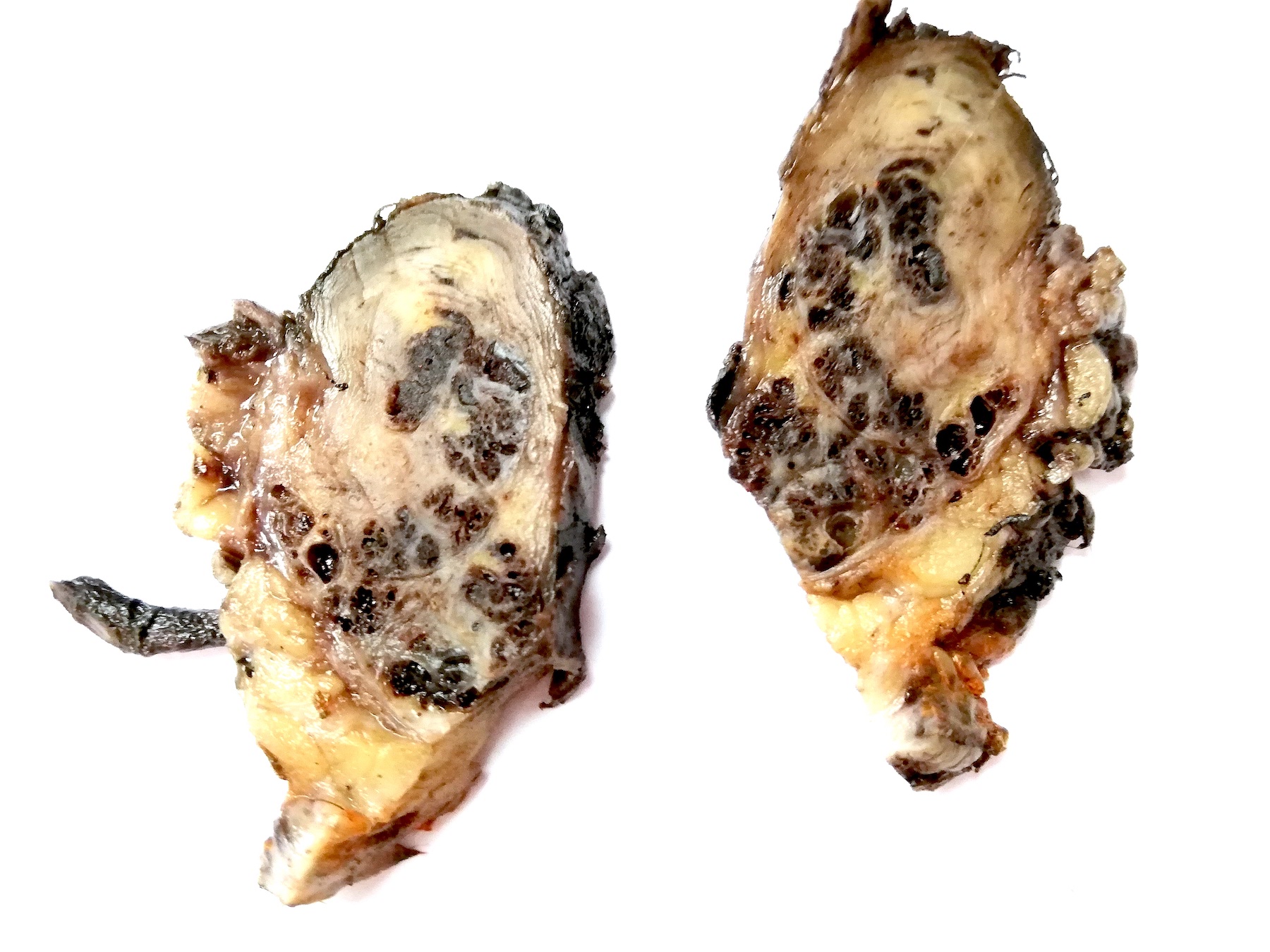
Circumscribed multilobulated lesion, elbow
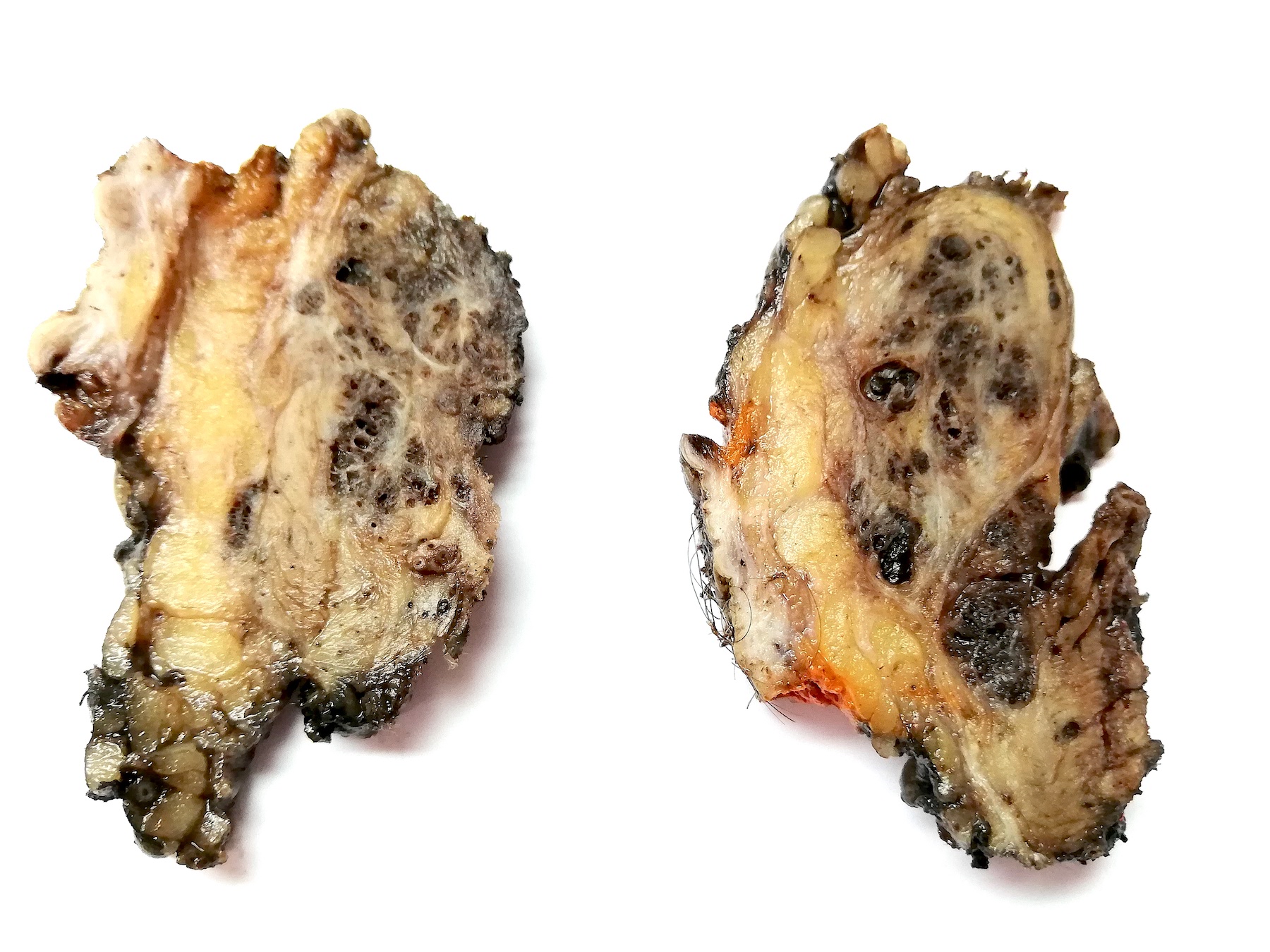
Ill defined, diffuse lesion, neck
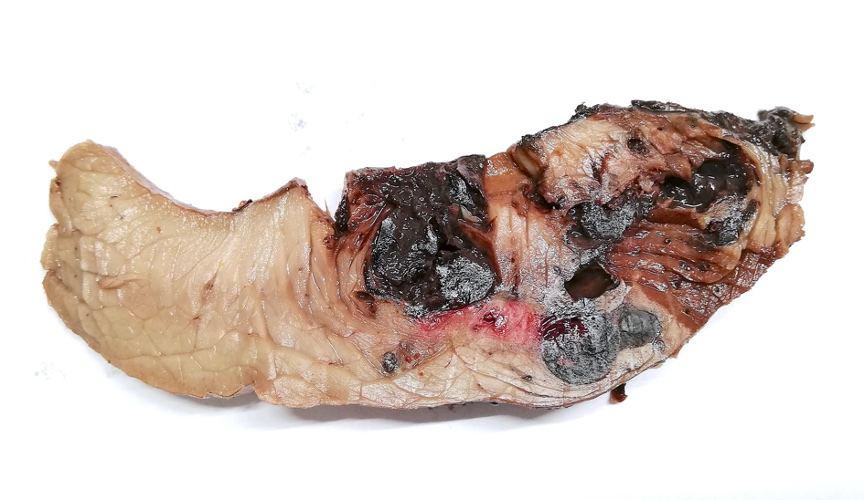
Intramuscular lobulated lesion, gastrocnemius
Images hosted on other servers:

Plantar intramuscular angioma

Gluteus lesion
- Can be diagnosed on frozen; however, bleeding remains a complication (J Oral Maxillofac Surg 1985;43:214)
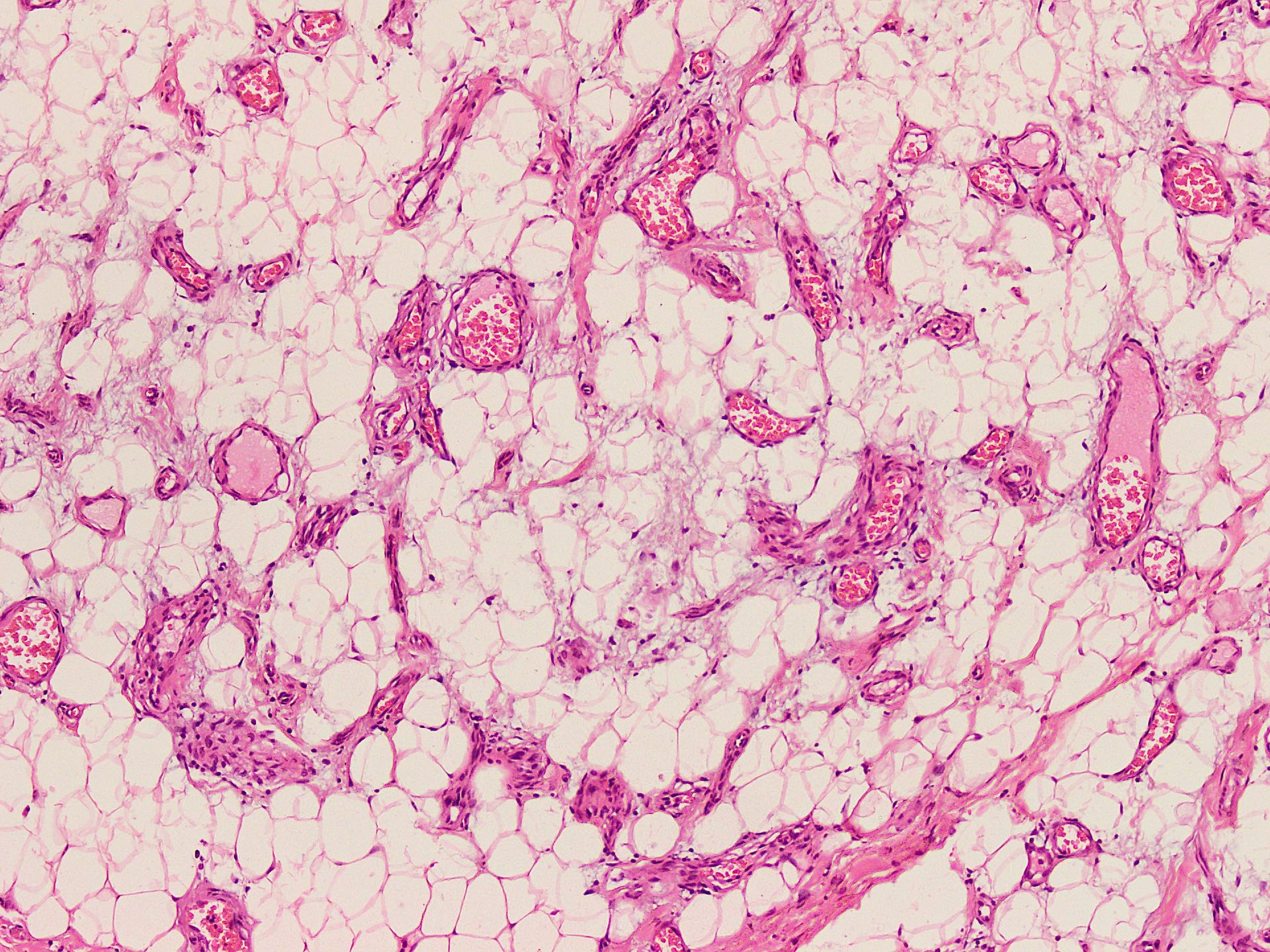
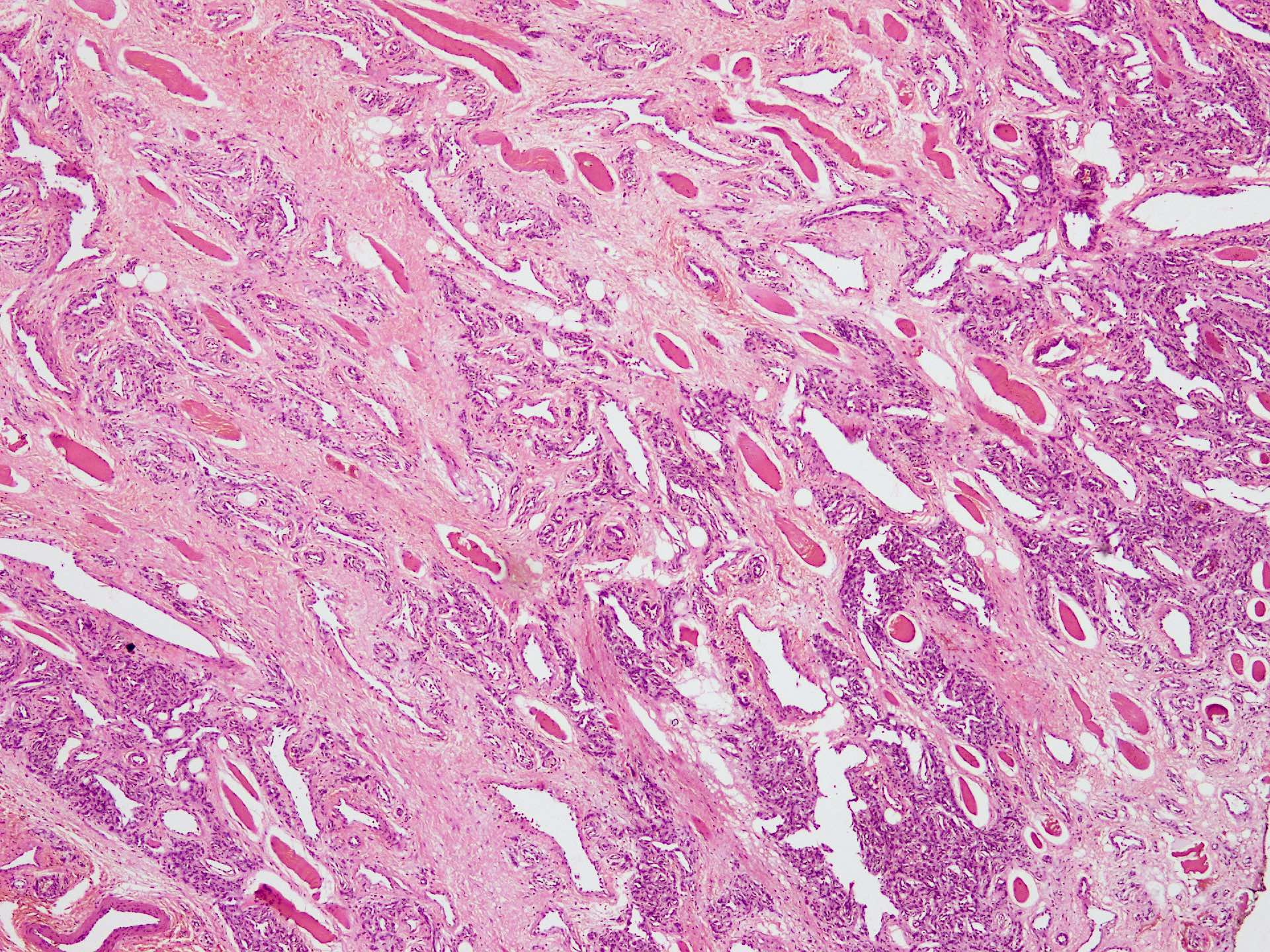
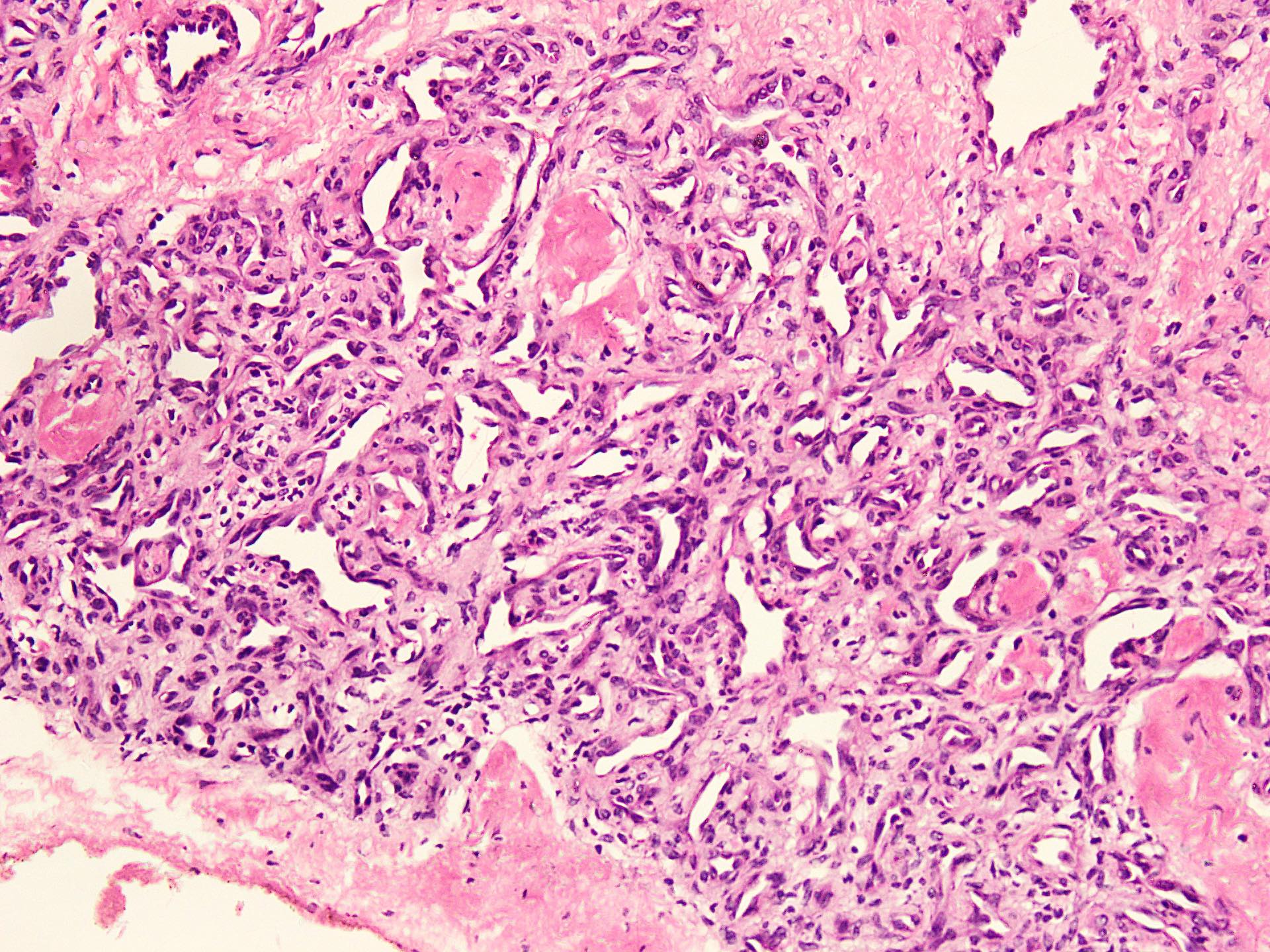
- Variable mixture of large and medium arteries and veins with small capillary sized vessels and ectatic lymphatic channels
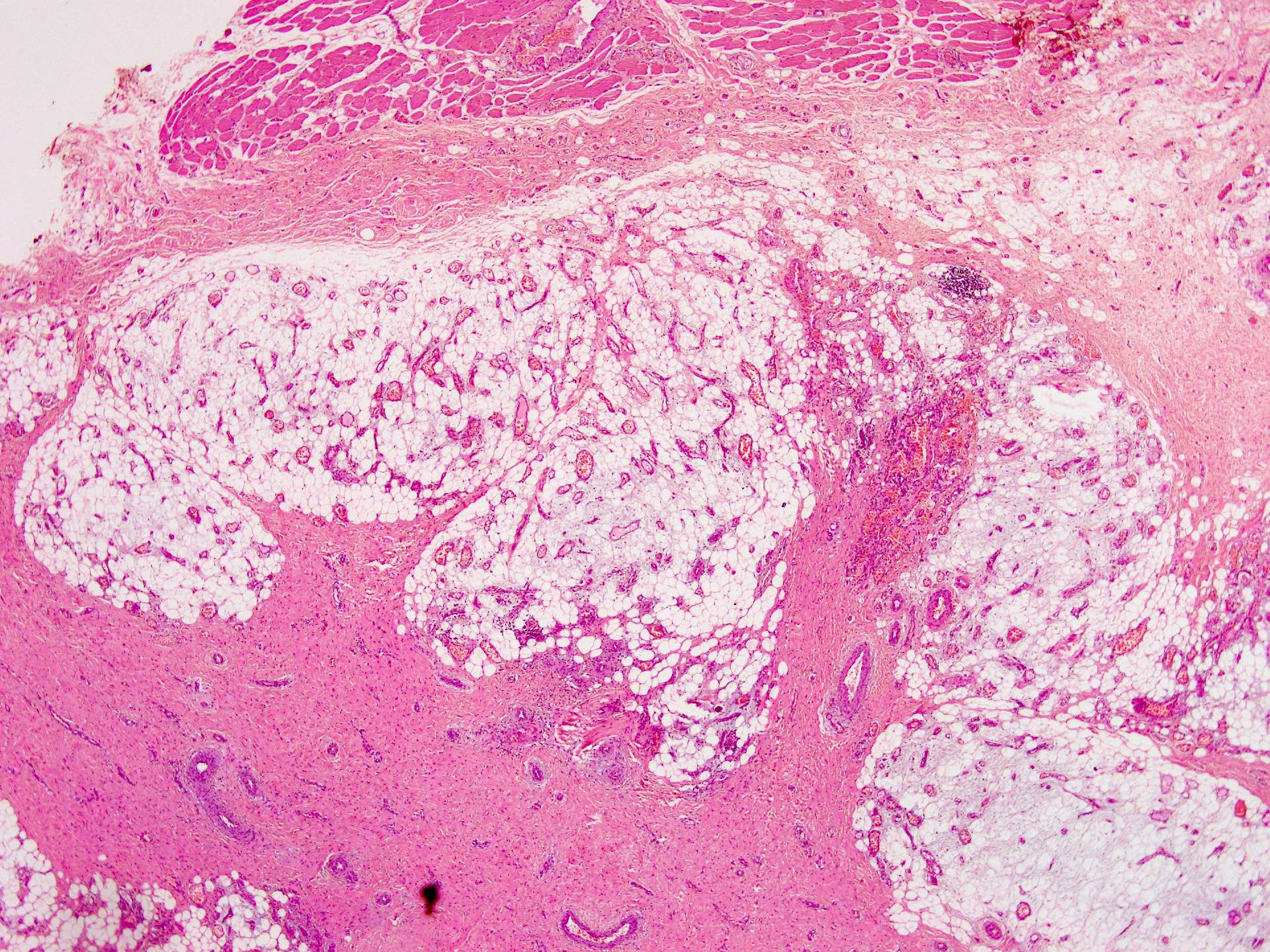
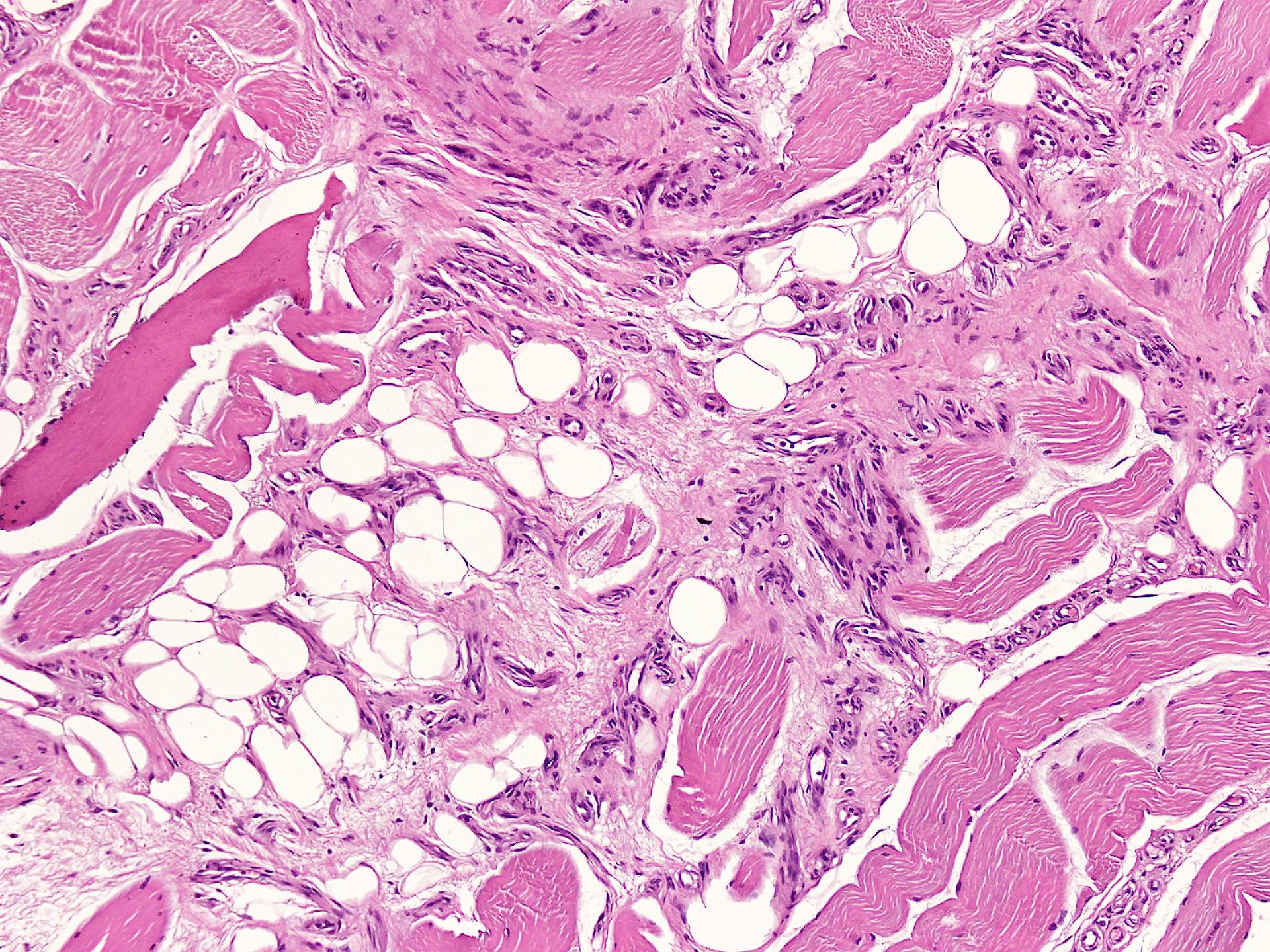
- Infiltration into skeletal muscle with ill defined edges
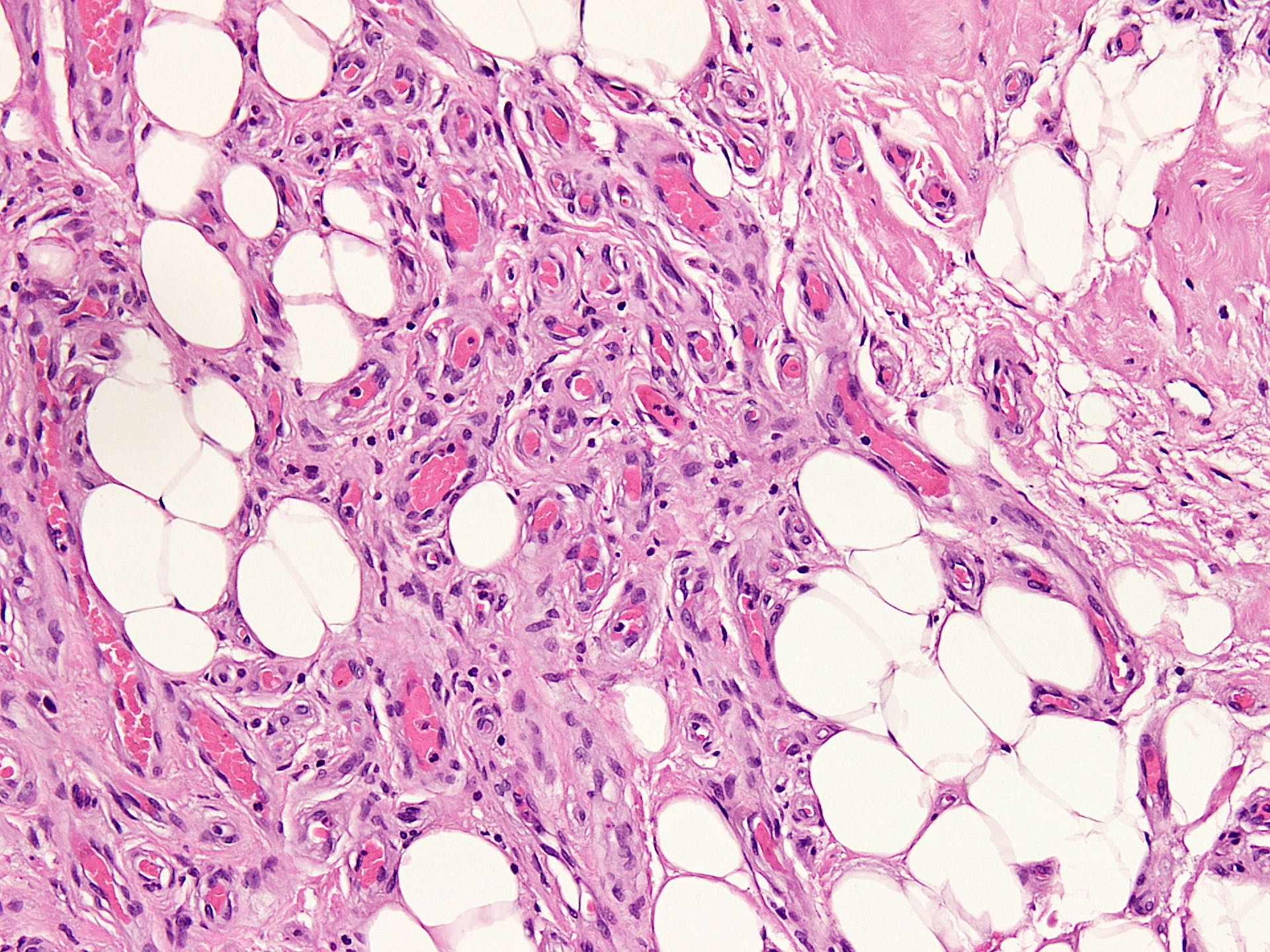
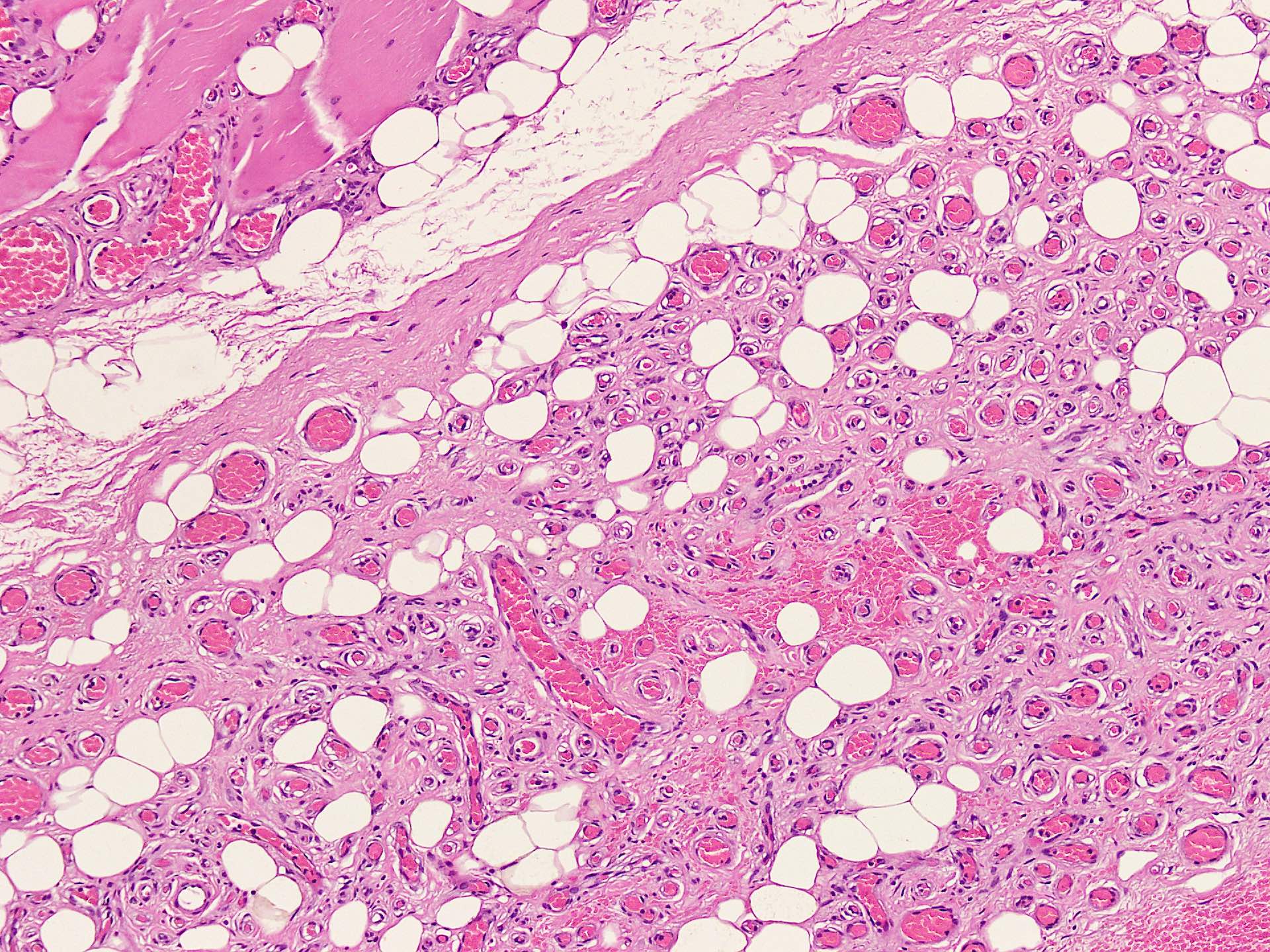
- Variable intralesional adipose tissue with some examples mimicking angiolipoma; checkerboard pattern is also seen
- Phleboliths may be seen in longstanding lesions
- Variable atrophy of native skeletal muscle with degenerative hyperchromatic appearance of sarcolemmal nuclei
- Perineural proliferation of small vessels, does not indicate aggressive behavior (Goldblum: Enzinger and Weiss’s Soft Tissue Tumors, 7th Edition, 2019)
- Preoperative embolization shows intravascular foreign material with degenerative changes in the lesion, including necrosis and inflammation (Stockman: Diagnostic Pathology - Vascular, 1st Edition, 2015)
- Rarely, intralesional bone tissue is seen
- Traditionally classified into:
- Capillary type:
- More common in head and neck region
- Small capillary sized vessels, with solid areas mimicking infantile hemangioma
- Plump endothelial cells
- Cavernous type:
- More common in trunk locations
- Proliferating small capillaries at periphery of larger vessels
- Attenuated bland endothelial cells
- Thrombosis is frequent
- Mixed type:
- Most common
- May also have lymphatic channels
- Capillary type:
Contributed by Nasir Ud Din, M.B.B.S.
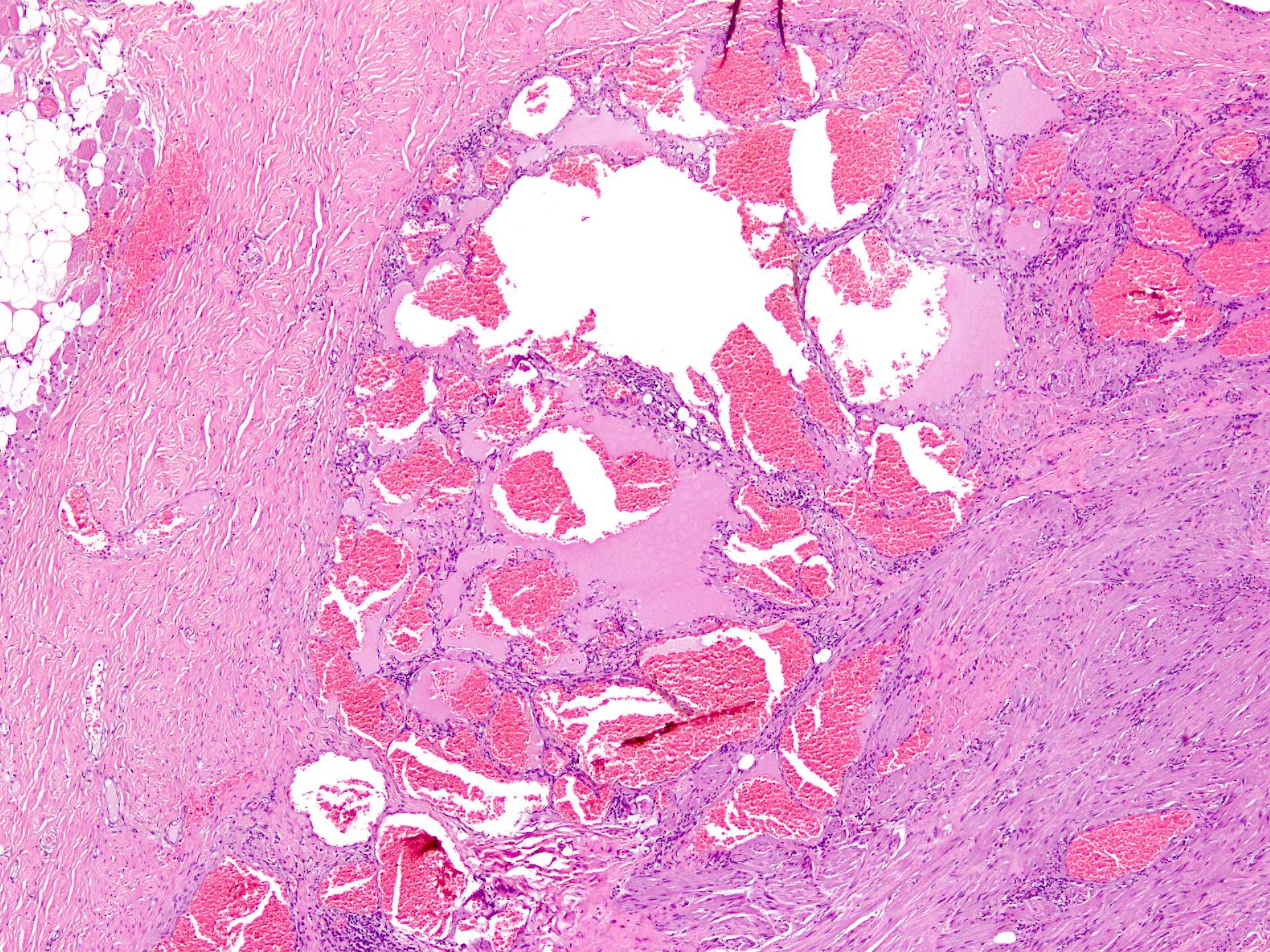
Lobulated lesion

Cavernous vessels

Variably sized vessels
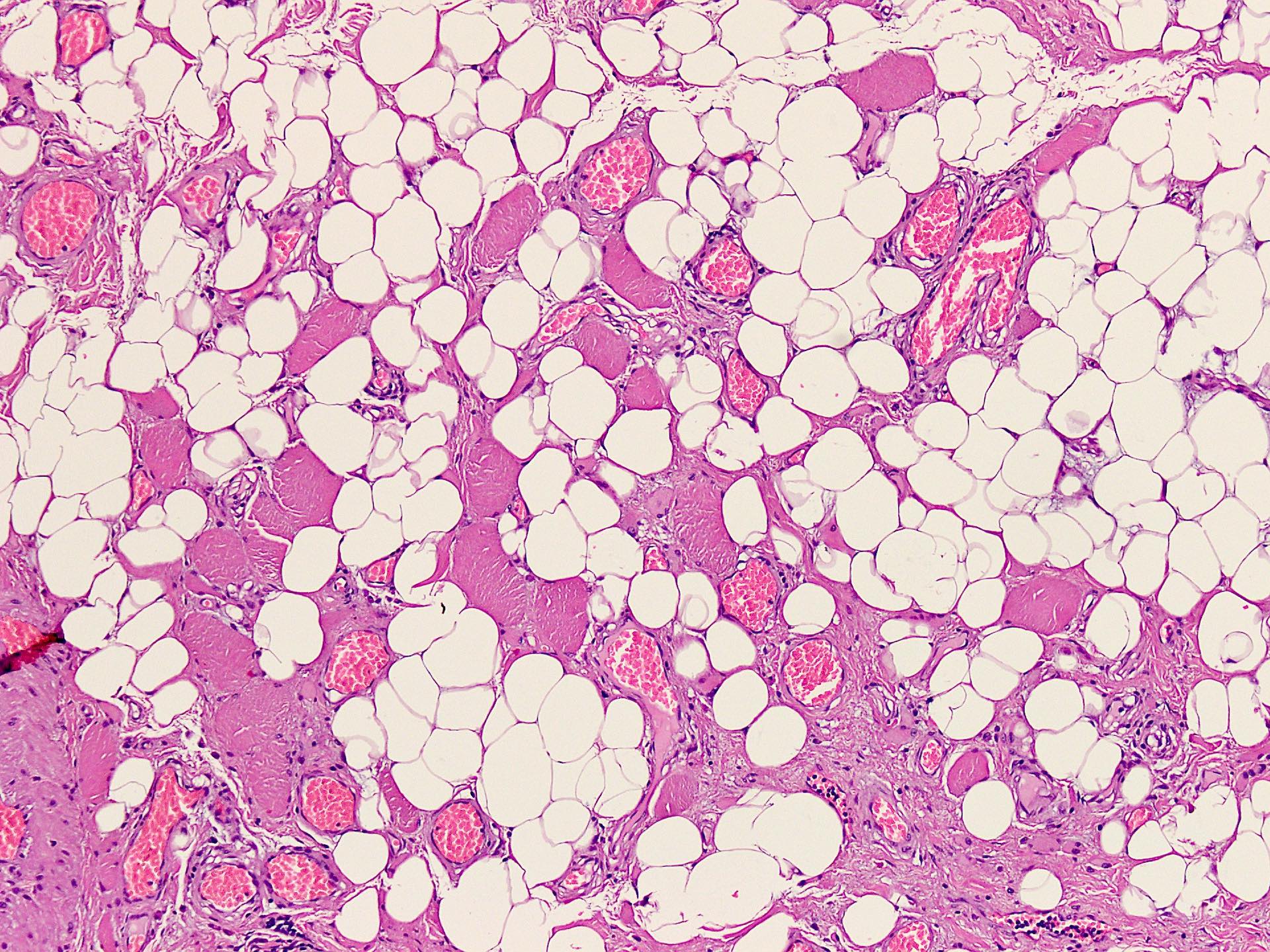
Intralesional adipose tissue
Angiolipoma-like appearance
Capillary vessels
Slit-like vessels
Infantile hemangioma-like appearance

Lobular proliferation of vessels
Inflammatory cells

Diffuse pattern
Thickened basement membrane
Hyalinization
Images hosted on other servers:

Intramuscular hemangioma
- May show hemorrhage, spindle endothelial cells and plump skeletal muscle cells (Arch Iran Med 2020;23:144)
- CD31: endothelial cells (membranous) (Rom J Morphol Embryol 2016;57:521)
- CD34: endothelial cells (membranous)
- ERG: endothelial cells (nuclear)
- SMA: pericytic smooth muscle (cytoplasmic)
- HHV8: positive in Kaposi sarcoma
- GLUT1: positive in infantile hemangioma
- Transmission electron microscopy shows composition of a mixture of cavernous and capillary channels within the muscle (Acta Ophthalmol Scand 2002;80:336)
- Not required for diagnosis
Hemangioma, capillary and cavernous: clinical features and morphology
- Right thigh, excisional biopsy:
- Benign vascular lesion infiltrating into skeletal muscle, composed of small to intermediate sized vascular channels lined by bland endothelial cells, favoring diagnosis of intramuscular angioma (see comment)
- Size: 12 x 10 x 3 cm
- Margin: painted excision margin is involved
- Comment: Although benign, these lesions have tendency to recur, if incompletely excised, in 30 - 50% of cases. Follow up with clinical findings and radiographic studies is recommended.
- Angiomatosis:
- Usually congenital
- Involves large areas of body and multiple tissue planes
- Microscopic features similar to intramuscular angioma; distinction requires clinical input
- Infantile hemangioma:
- Involves skin / soft tissue of face, head and neck of infants
- Lobular arrangement and proliferation of capillaries separated by thin fibrous tissue
- Cellularity and number of vessels decrease with time
- GLUT1 positivity by IHC
- Angiolipoma:
- Occurs in subcutaneous tissue
- Small, painful, circumscribed lesions, often multiple
- Capillary sized vascular channels only
- Vessels may show fibrin thrombi
- Angiosarcoma:
- Extremely rare in deep soft tissues
- Complex interanastomosing vascular channels with atypia
- Multiple layers of endothelial cells with nuclear pleomorphism and increased mitotic activity
- Intramuscular lipoma:
- Site predilection same as intramuscular angioma
- Infiltrative lesion with sheets of mature adipocytes and intervening skeletal muscle component
- Vascular component is sparse

A 25 year old man presented with right leg pain, particularly after exercise. Physical examination showed slightly increased bulkiness of the right leg as compared to the left. MRI showed a well defined lesion in the belly of gastrocnemius, which was isointense on T1, hyperintense on T2 and showed an intralesional fat component. A photomicrograph of the excised lesion is given. Which of the following statements regarding this lesion is true?
- Association with trauma is well established in these lesions
- Capillary proliferation within perineural sheaths is ominous
- Examples with adipose tissue represent intramuscular lipoma
- Recurrence rate is high after incomplete excision
- These tumors represent congenital malformations
Comment Here
Reference: Intramuscular angioma

A 16 year old girl presented with a slowly growing left leg mass. Gross specimen was comprised of skin covered fibroadipose and fibromuscular tissue with an ill defined, diffuse lesion within muscle. Cut surface showed small to intermediate sized blood filled vessels arranged in lobules. Microscopy revealed a proliferation of benign appearing vascular channels of variable sizes with intervening adipose tissue. No atypia, necrosis or increased mitoses were observed. A photomicrograph of the lesion is shown. What is the most likely diagnosis?
- Angioleiomyoma
- Angiolipoma
- Angiosarcoma
- Intramuscular angioma
- Intramuscular lipoma
