

Soft tissue
Smooth muscle
Leiomyosarcoma
Inflammatory leiomyosarcoma
Editorial Board Member: Nasir Ud Din, M.B.B.S.
Deputy Editor-in-Chief: Borislav A. Alexiev, M.D.


Last author update: 21 March 2024
Last staff update: 21 March 2024
Copyright: 2019-2024, PathologyOutlines.com, Inc.
PubMed Search: Inflammatory leiomyosarcoma
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Montoya-Cerillo DM, Velez-Torres JM. Inflammatory leiomyosarcoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/softtissueinflammatoryleiomyosarcoma.html. Accessed April 24th, 2024.
Definition / general
- Inflammatory leiomyosarcoma (ILMS) is a malignant neoplasm showing smooth muscle differentiation, a prominent inflammatory infiltrate and near haploidization
Essential features
- Fascicular proliferation of variably atypical eosinophilic spindle cells, which show mitotic activity (most often lymphoid or histiocytic / xanthomatous) but the composition is variable
- Calcospherites (psammomatous calcifications) are an uncommon and striking feature
- Virtually all cases show immunopositivity for some combination of SMA, desmin, MyoD1, myogenin and h-caldesmon (Genes Chromosomes Cancer 2022;61:653)
- Near haploid karyotype (Genes Chromosomes Cancer 2022;61:653)
- Most cases follow an indolent clinical course with low metastatic potential; rarely may progress to rhabdomyosarcoma (Mod Pathol 2023;36:100131, Genes Chromosomes Cancer 2022;61:653)
Terminology
- Related terminology: these tumors have significant pathologic and genetic overlap with the recently described inflammatory rhabdomyoblastic tumor (IRT) and low grade inflammatory myogenic tumor (LGIMT), suggesting that ILMS and IRT / LGIMT may belong to 1 entity (Mod Pathol 2021;34:758, Virchows Arch 2020;477:219).
ICD coding
- ICD-O: 8890/3 - leiomyosarcoma, NOS
- ICD-10: C49.9 - malignant neoplasm of other connective and soft tissue, unspecified
- ICD-11: 2B58 & XH7ED4 - leiomyosarcoma, primary site & leiomyosarcoma, NOS
Epidemiology
- Young to middle aged adults (30 - 40 years)
- Male predilection (Mod Pathol 2021;34:758)
Sites
- Deep soft tissue of the extremities and trunk
- Neck, abdominal cavity and retroperitoneum are less frequent locations
Pathophysiology
- Near haploidization and NF1 mutations are the 2 most common defining genetic abnormalities
- May progress to high grade rhabdomyosarcoma in a small subset (Mod Pathol 2021;34:1035)
Etiology
- Unknown at this time
Clinical features
- Commonly presents as an enlarging soft tissue mass with indolent behavior
- In 2 reported cases, the tumor was associated with paraneoplastic inflammatory syndrome (Int J Surg Pathol 2005;13:185)
- When rhabdomyosarcomatous transformation occurs, pulmonary metastases are frequently present at the time of diagnosis (Mod Pathol 2023;36:100131)
Diagnosis
- Clinical presentation: enlarging soft tissue mass
- Imaging: computed tomography (CT), magnetic resonance imaging (MRI)
Radiology description
- Predominantly solid, deep seated soft tissue mass
- Well circumscribed
- Homogeneously enhancing
- T1 and T2 hyperintense
- Reference: Int J Surg Case Rep 2021:82:105907
Radiology images
Contributed by Diego M. Montoya-Cerrillo, M.D.
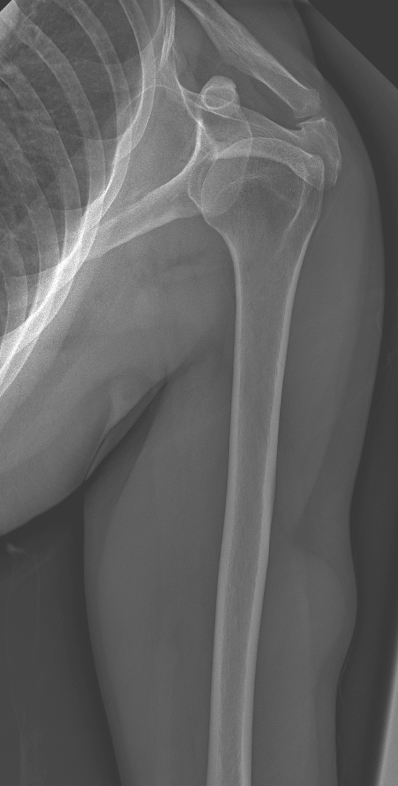
Xray

Ultrasound
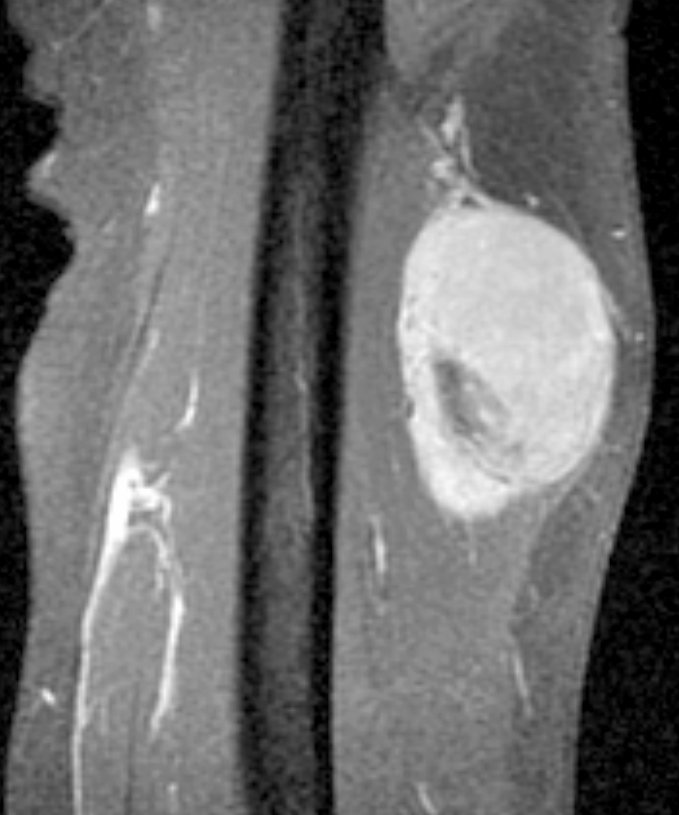

Well circumscribed soft tissue mass
Prognostic factors
- When completely excised, it rarely recurs (Virchows Arch 2020;477:219)
Case reports
- 23 year old woman with Lynch syndrome and a thigh mass (Genes Chromosomes Cancer 2022;61:653)
- 58 year old man with thigh mass for more than 20 years (Medicine (Baltimore) 2021;100:e26105)
- 68 year old woman with a periscapular mass (Diagn Cytopathol 2023;51:E109)
Treatment
- Wide local excision with negative surgical margins
- Radiation and chemotherapy are reserved to cases where rhabdomyosarcoma is present
Gross description
- Well demarcated, oval - round
- Median size: ~4 cm (range: 2 - 12 cm)
- Reference: Mod Pathol 2023;36:100131
Gross images
Contributed by Andrew E. Rosenberg, M.D.

Upper arm tumor
Microscopic (histologic) description
- Well circumscribed tumor surrounded by a fibrous pseudocapsule
- Calcifications (calcospherites), lymphoid aggregates, hyalinized blood vessels and hemosiderin deposits are commonly present
- Spindle and epithelioid tumor cells arranged in sheets and fascicles with eosinophilic cytoplasm, vesicular nuclei and conspicuous nucleoli
- Prominent inflammatory infiltrate of foamy histiocytes and variable lymphocytes, plasma cells or Touton type giant cells
- Degree of nuclear atypia and pleomorphism varies, as does mitotic count, depending on the histologic grade (Mod Pathol 2021;34:758)
Microscopic (histologic) images
Contributed by Diego M. Montoya-Cerrillo, M.D. and Elizabeth A. Montgomery, M.D.
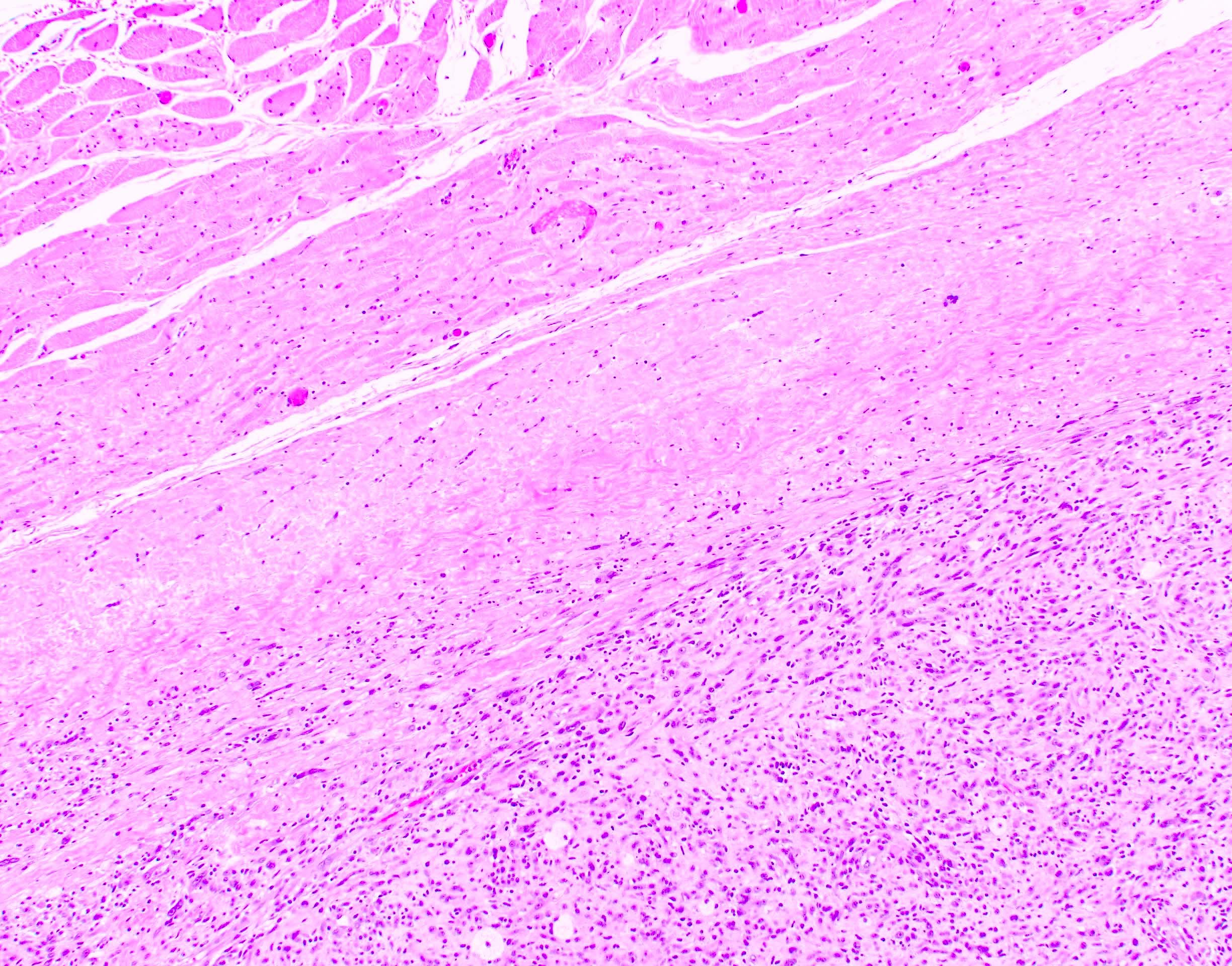
Fibrous pseudocapsule
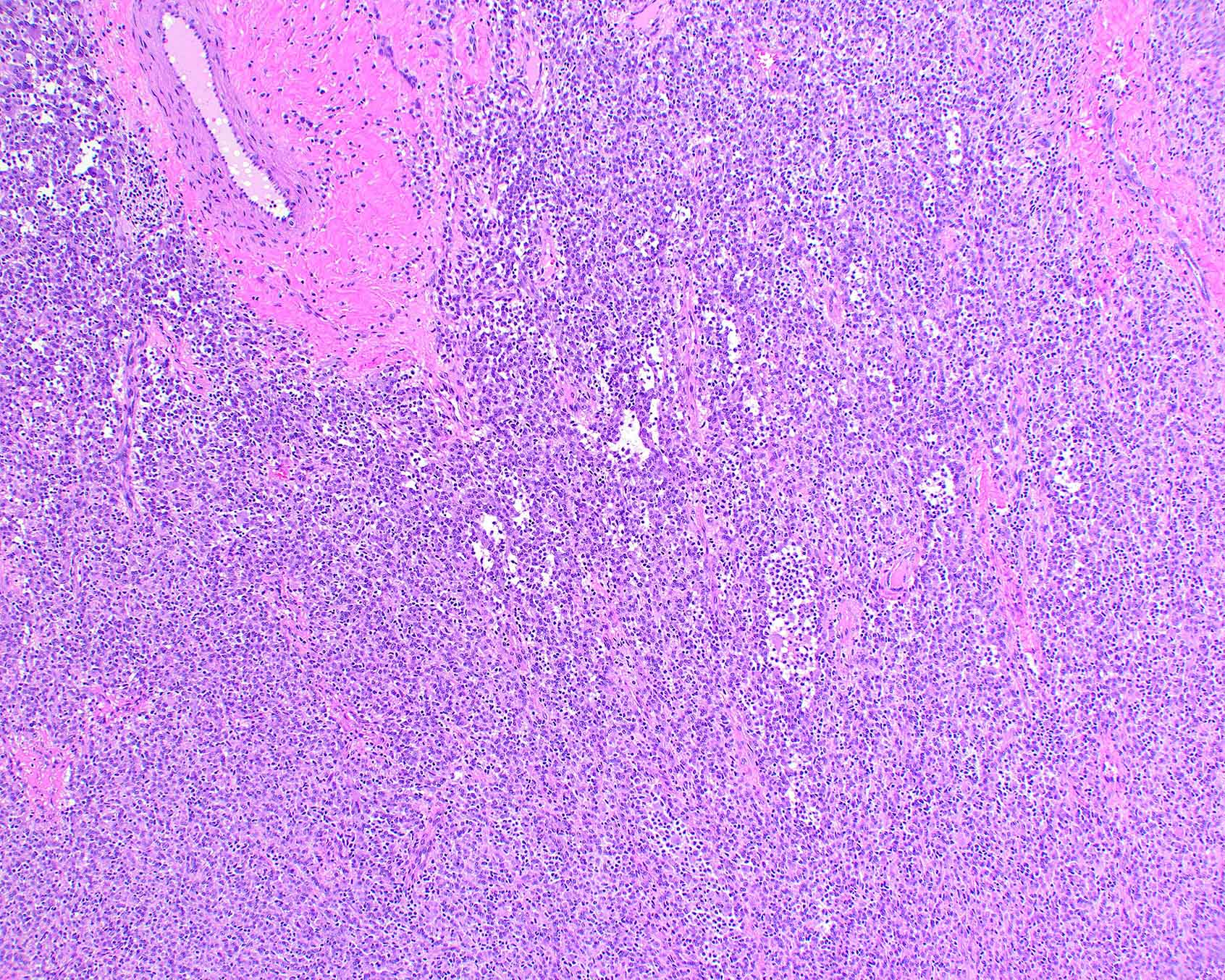
Prominent inflammation and thickened blood vessels
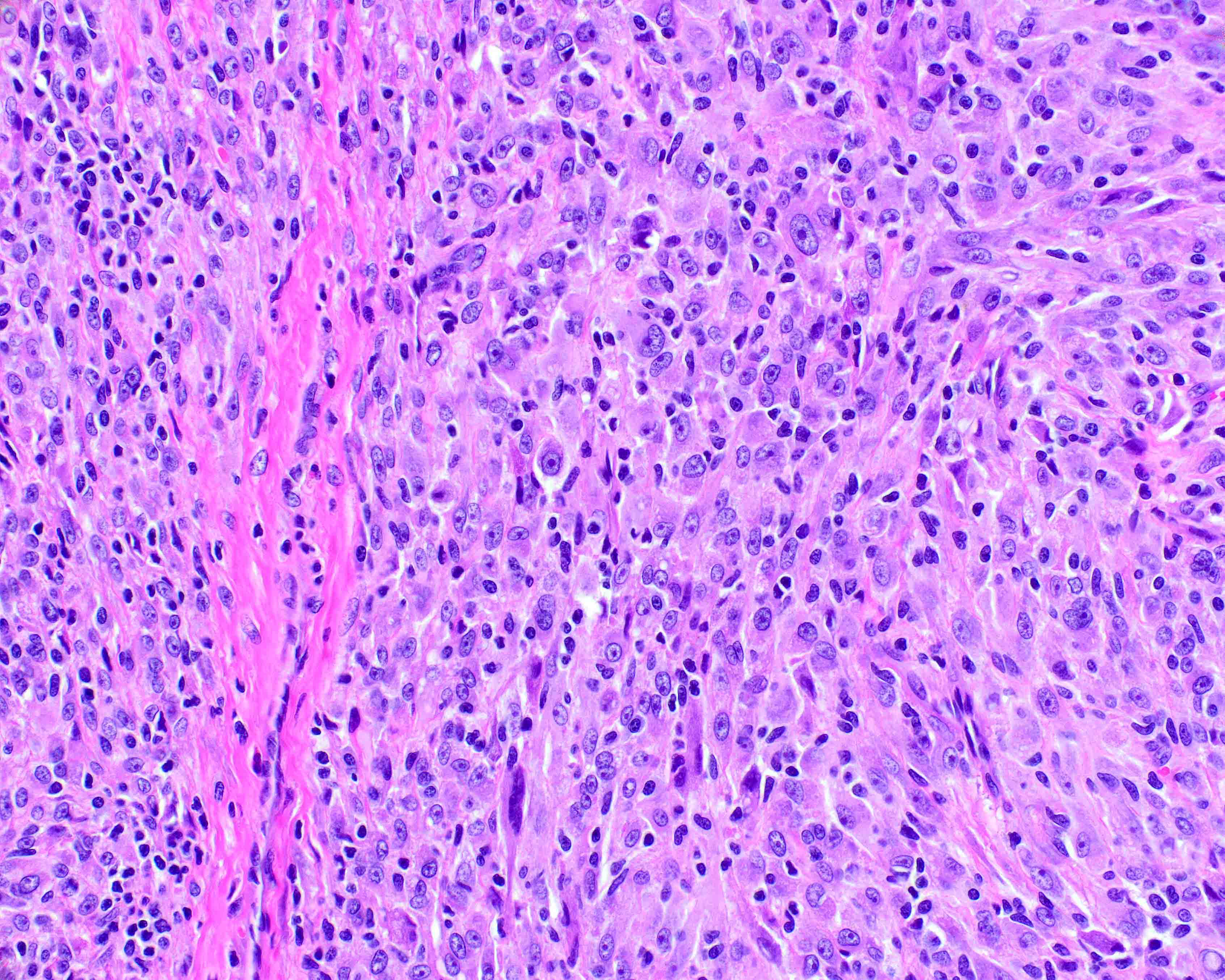
Prominent nucleoli

Pleomorphic cells

Foamy macrophages

Desmin
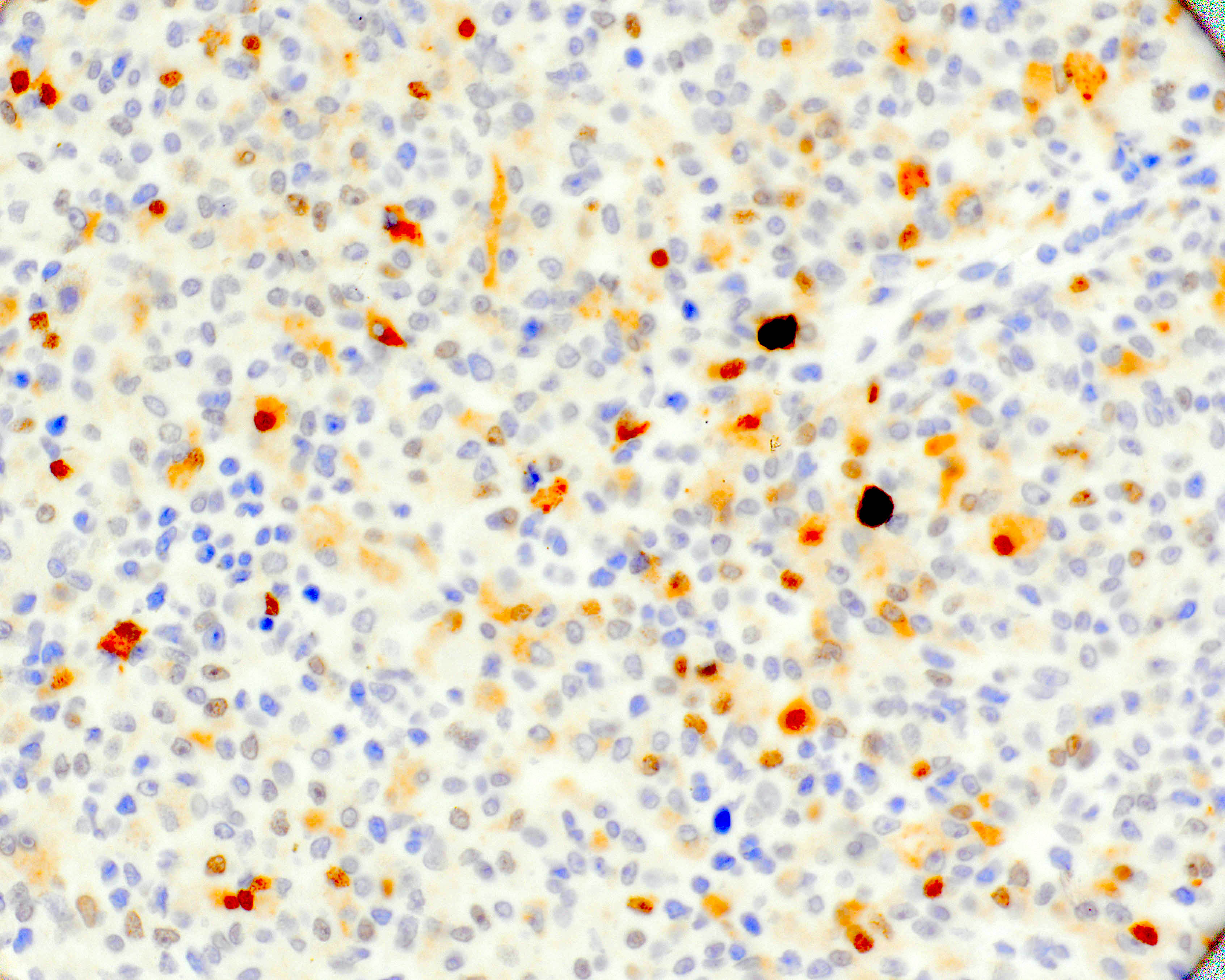
MyoD1
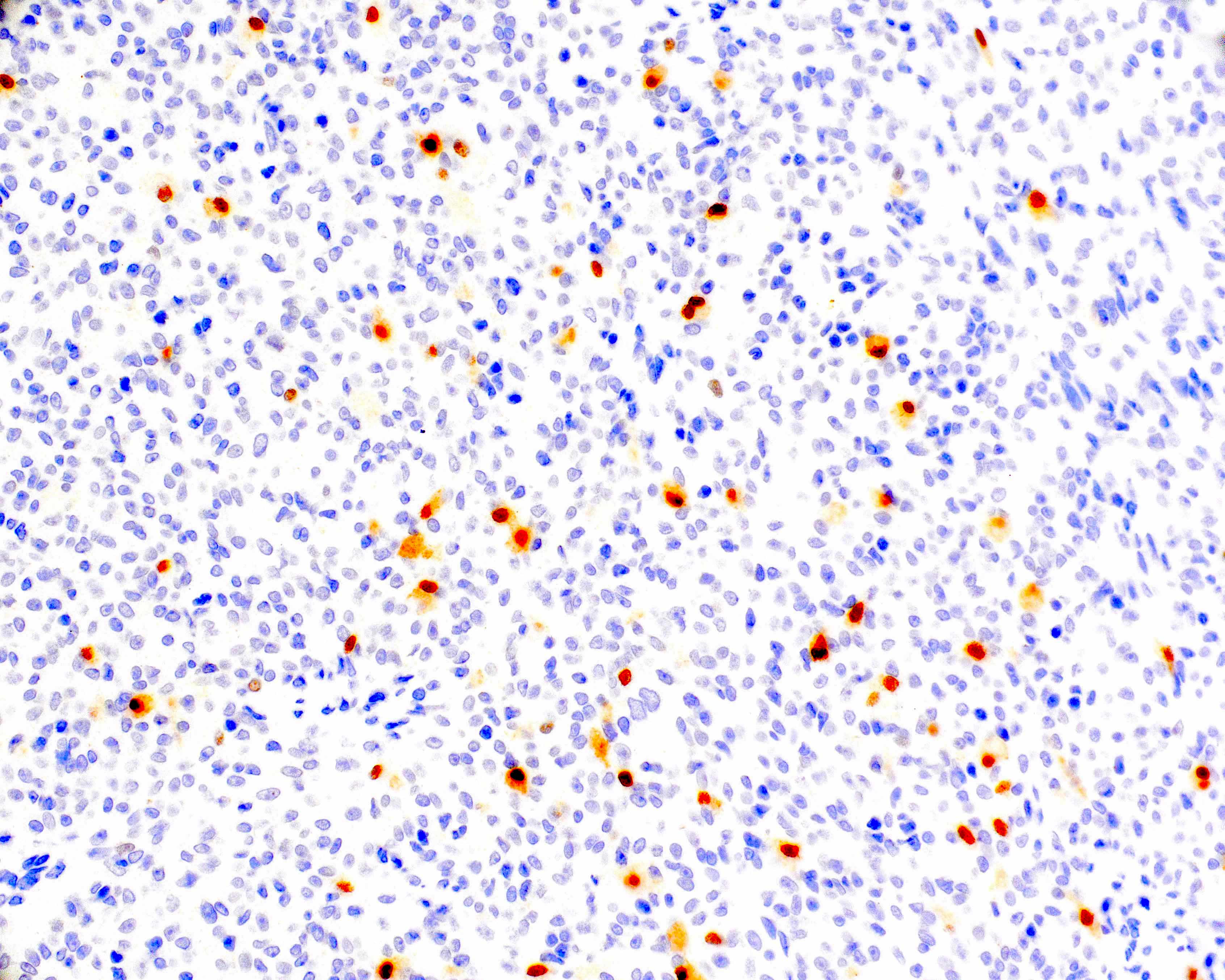
Myogenin
Positive stains
- Virtually all cases show immunopositivity for some combination of SMA, desmin, MyoD1 and myogenin (Genes Chromosomes Cancer 2022;61:653)
- CD163 and CD168 (highlights intratumoral histiocytes)
- Very low proliferation index by Ki67 (< 5%) in the majority of cases
- Reference: Mod Pathol 2021;34:758
Negative stains
Electron microscopy description
- Lack of filament arrangement pattern characteristic of smooth muscle cells with varying amounts of stromal collagen fibers (Int J Surg Pathol 2005;13:185)
Molecular / cytogenetics description
- Near haploidization with loss of almost all chromosomes and retention of heterodisomy of chromosomes 5, 22, 18, 20 or 21 is the distinct genomic pattern (Mod Pathol 2021;34:758, Mod Pathol 2021;34:1434)
- Next generation sequencing identified sequence variants in NF1, TP53, SMARCA4, KRAS and MSH6 (Genes Chromosomes Cancer 2022;61:653)
- In one case, an MSH6 germline splice site variant was identified by next generation sequencing and it was consistent with Lynch syndrome (Genes Chromosomes Cancer 2022;61:653)
Molecular / cytogenetics description
Images hosted on other servers:

Loss of heterozygosity
Sample pathology report
- Soft tissue tumor, left thigh, biopsy / resection:
- Inflammatory leiomyosarcoma (see comment and synoptic report)
- Comment: There is moderate cytological atypia, limited mitotic activity (x mitoses per 10 HPF) and no foci of necrosis. Immunohistochemistry shows that the tumor cells are positive for desmin, MyoD1 and focally positive for myogenin and SMA. CD68 / CD163 highlights intratumoral histiocytes. The proliferation index by Ki67 is x%. All surgical margins are negative for tumor. No areas concerning for rhabdomyosarcoma are present. No vascular invasion is present.
- Overall, these pathologic findings are consistent with inflammatory leiomyosarcoma. These tumors have significant pathologic and genetic overlap with the recently described inflammatory rhabdomyoblastic tumor (IRT) and low grade inflammatory myogenic tumor (LGIMT), suggesting that ILMS and IRT / LGIMT may belong to 1 entity (Mod Pathol 2021;34:758, Virchows Arch 2020;477:219)
Differential diagnosis
- Spindle cell / sclerosing rhabdomyosarcoma (Arch Pathol Lab Med 2022;146:953):
- Displays aggressive behavior
- Typically lacks the inflammatory component and if present is not prominent
- Harbors MYOD1 mutations or rearrangements of VGLL2::NCOA2, TFCP2 and VGLL3
- Angiomatoid fibrous histiocytoma (Am J Surg Pathol 2019;43:1156):
- Inflammatory myofibroblastic tumor (Am J Surg Pathol 2015;39:957):
Additional references
Board review style question #1

A 35 year old man presented with a slowly growing mass in the right thigh. Magnetic resonance imaging showed a 6 cm well circumscribed tumor in the deep planes. A biopsy was performed. The tumor cells are diffusely positive for desmin and MyoD1. What is the diagnosis?
- Inflammatory leiomyosarcoma
- Inflammatory myofibroblastic tumor
- Pleomorphic rhabdomyosarcoma
- Sclerosing rhabdomyosarcoma
Board review style answer #1
A. Inflammatory leiomyosarcoma. The histology shows spindle and epithelioid cells with eosinophilic cytoplasm, moderate pleomorphism but no mitotic activity and prominent nucleoli admixed with inflammatory cells characteristic of inflammatory leiomyosarcoma / inflammatory rhabdomyoblastic tumor. Answer D is incorrect because the cells in sclerosing rhabdomyosarcoma are small, round to spindle and embedded in a prominent hyalinized stroma. Answer C is incorrect because pleomorphic rhabdomyosarcoma is a high grade tumor with marked pleomorphism and increased mitotic activity. Answer B is incorrect because inflammatory myofibroblastic tumor does not show expression of skeletal muscle markers and is ALK positive instead.
Comment Here
Reference: Inflammatory leiomyosarcoma
Comment Here
Reference: Inflammatory leiomyosarcoma
Board review style question #2
Which of the following genetic alterations is most commonly seen in inflammatory leiomyosarcoma?
- 1q21 amplification
- Mutation of MYOD1
- Near haploidization
- VGLL2 rearrangements
Board review style answer #2
C. Near haploidization. Near haploidization with preservation of biparental disomy of chromosomes 5 and 22 is the most common genetic finding in inflammatory leiomyosarcoma / inflammatory rhabdomyoblastic tumor. Genome doubling leading to hyperdiploidy and mutations of NF1 are other recurrent genetic alterations. Answers B and D are incorrect because mutations of MYOD1 and rearrangements of VGLL2 are commonly seen in sclerosing / spindle cell rhabdomyosarcoma. Answer A is incorrect because amplification of 1q21 is one of the most frequent cytogenetic aberrations in multiple myeloma.
Comment Here
Reference: Inflammatory leiomyosarcoma
Comment Here
Reference: Inflammatory leiomyosarcoma
