

Soft tissue
Fibroblastic / myofibroblastic
Superficial acral fibromyxoma
Authors: Saira Fatima, M.B.B.S., Nasir Ud Din, M.B.B.S.
Editorial Board Member: Jose G. Mantilla, M.D.
Deputy Editor-in-Chief: Borislav A. Alexiev, M.D.


Last author update: 11 March 2024
Last staff update: 11 March 2024
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Superficial acral fibromyxoma
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Electron microscopy description | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Fatima S, Ud Din N. Superficial acral fibromyxoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/softtissuesuperficialacral.html. Accessed April 18th, 2024.
Definition / general
- Benign neoplasm of fibroblastic origin, with tendency for affecting periungual regions of the digits on acral sites
- Lesions are prone to local recurrence
Essential features
- Acral region especially around the digits are favored sites
- Lobulated dermal and subcutaneous spindle cell lesion with myxoid and collagenous stroma
- Stroma and prominent vessels
- RB1 gene deletions are observed
- Surgical excision with adequate margins is treatment of choice
Terminology
- Acceptable: digital fibromyxoma, superficial acral fibromyxoma
- Not recommended: cellular digital fibroma
ICD coding
Epidemiology
- Occurs in mid adult life, with a wide age range of 4 - 86 years (Hum Pathol 2001;32:704)
- Especially males, M:F = 1.3:1 (Am J Surg Pathol 2012;36:789)
Sites
- Most commonly periungual or subungual region of fingers and toes (Hum Pathol 2001;32:704)
- Great toe is the most frequent one among digits (Cutis 2015;95:E15)
- Regions under the matrix are unusual (Ann Dermatol Venereol 2014;141:94)
- Hands and feet (other than digits such as wrists and heels) can be affected (J Cutan Pathol 2008;35:1020)
- Ankles and leg are rarely involved (Am J Surg Pathol 2012;36:789)
Pathophysiology
- RB1 gene deletions at chromosome 13q14.2 (Diagnostics (Basel) 2021;11:430)
- Variable co-loss of the corresponding 13q12 signal (monosomy at the 13q region) (Hum Pathol 2017;60:192)
Etiology
- Unknown
Clinical features
- Slow growing, single and often painful tumors
- Nail erosion was reported (Arch Orthop Trauma Surg 2008;128:271)
- Ulceration may also occur (An Bras Dermatol 2014;89:147)
- Preceding trauma has been noticed in few of the cases (Arch Pathol Lab Med 2011;135:1064)
- Pseudoclubbing, onychogryphosis (ram horn nail) or triangular macrolunula were presenting features of rare lesions under the matrix (Ann Dermatol Venereol 2014;141:94)
- Erosive or lytic lesion of underlying bone may be seen on imaging (Am J Surg Pathol 2012;36:789)
Diagnosis
- Acral soft tissue lesion affecting digits with or without cortical erosion
- Typical location around digits should raise clinical suspicion
- Radiological features are not characteristic
- Histological examination of the lesion is diagnostic
- Reference: J Cutan Pathol 2008;35:1020
Radiology description
- Plain radiograph (Skeletal Radiol 2008;37:499)
- Well circumscribed soft tissue mass with secondary saucer-like erosion of bone cortex
- Calcification is absent
- There may be sclerosis and buttressed margin of cortex in longstanding cases
- Magnetic resonance imaging (MRI): soft tissue lesion, T2 hyperintense with focal thinning of the cortex (Skeletal Radiol 2008;37:499)
Radiology images
Contributed by Nasir Ud Din, M.B.B.S.

AP Xray of distal phalanx
Images hosted on other servers:

Plain Xray

MRI

Computed tomography (CT) and MRI
Prognostic factors
- Local recurrences developed in 3 of 14 patients (22%) in a study (J Cutan Pathol 2008;35:1020)
- In a study of 18 patients (mean follow up interval of 10.1 years), there was 1 recurrence after local excision and 2 cases persisted / progressed after partial excision (Hum Pathol 2001;32:704)
- Local recurrence was seen in 24% of cases in another study (all near the nail unit of the fingers or toes) after a mean interval of 27 months (Am J Surg Pathol 2012;36:789)
- 1 tumor recurred twice
- Margins on initial biopsy or subsequent excision had been involved
- No other clinical or pathologic features were predictive of recurrence / persistence
- Metastasis has not been reported
Case reports
- 18 year old woman with painless subungual nodule of great toe (Indian Dermatol Online J 2017;8:45)
- 28 year old woman with a painless, slow growing mass on right distal aspect of the phalanx (JAAD Case Rep 2023;33:109)
- 54 year old man with 2 lobed mass lesion in the fifth finger (Int J Surg Case Rep 2020;77:531)
- 64 year old man presented to the emergency room for an ingrown toenail associated lesion (J Surg Case Rep 2023;2023:rjad027)
- 70 year old woman with ulcerated firm nodule on sole of foot (BMJ Case Rep 2022;15:e247565)
Treatment
- Surgical excision with adequate margin is recommended
- Locally recurrent lesions can undergo re-excision
Clinical images
Contributed by Jose G. Mantilla, M.D.

Well circumscribed periungual mass
Images hosted on other servers:

Retronychia of toe

Subungual round tumor, green nail plate

Subungual round pinkish tumor

Subungual tumor distorting nail plate

Dermoscopy
Gross description
- Dome shaped, polypoidal, verrucous, nodular, flesh colored (Skin Appendage Disord 2021;7:468)
Gross images
Images hosted on other servers:

Nodules with firm consistency

Soft lobulated lesion

Nodular pink mass
Microscopic (histologic) description
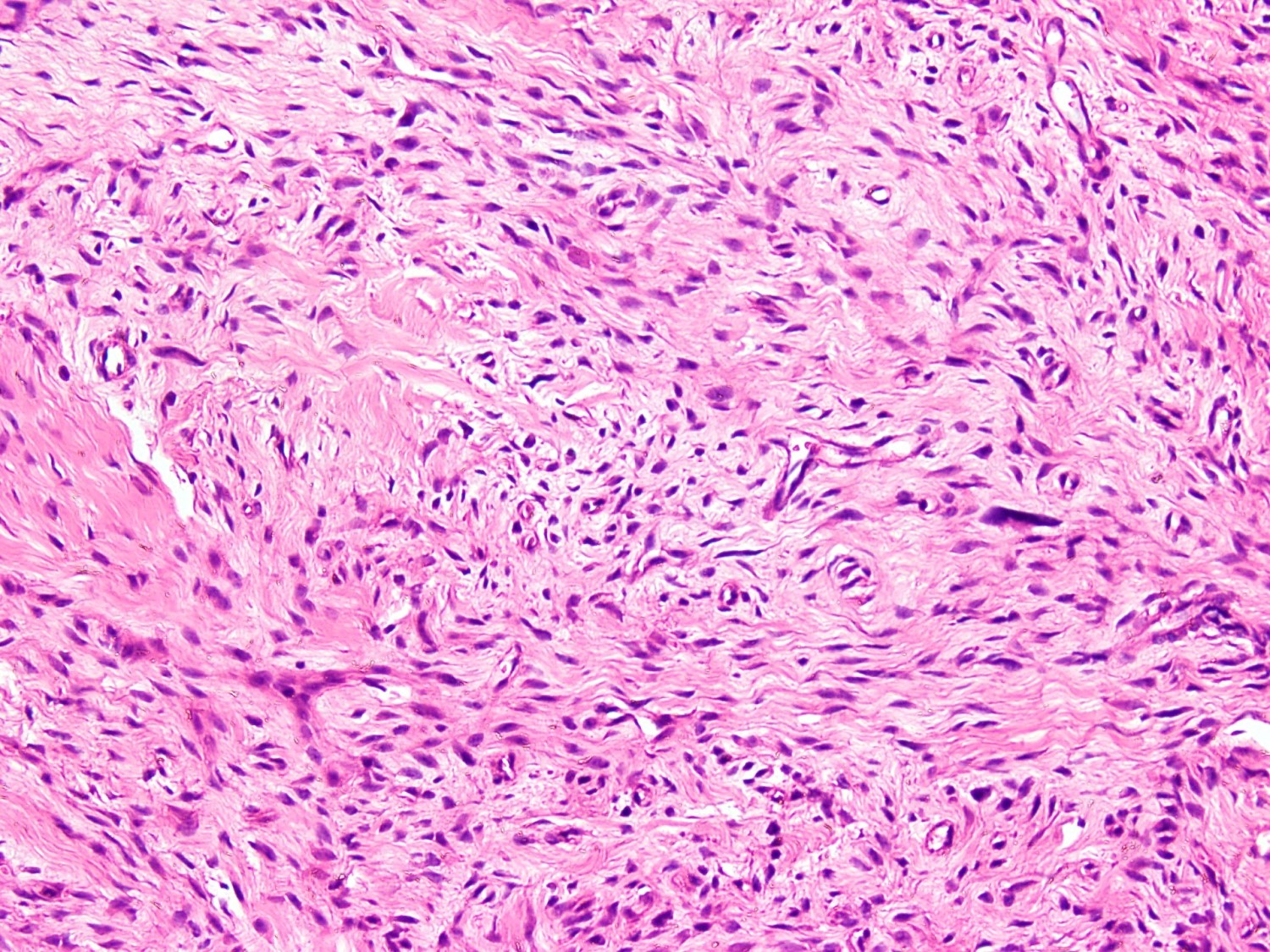
- Poorly circumscribed lesion in dermis composed of spindle to stellate shaped fibroblastic cells arranged in a loose storiform / fascicular pattern with alternating myxoid and collagenous stroma (Am J Surg Pathol 2012;36:789)
- Microvasculature is prominent (Hum Pathol 2001;32:704)
- Multinucleated stromal cells may be present and mast cells are frequent (Hum Pathol 2001;32:704)
- Bland nuclei lacking significant mitoses or necrosis; occasionally degenerative atypia may be encountered
- Infiltration in adipose tissue can occur
- Cellular variants are also encountered
- Cartilaginous and osseous metaplasia may be observed
Microscopic (histologic) images
Contributed by Nasir Ud Din, M.B.B.S.
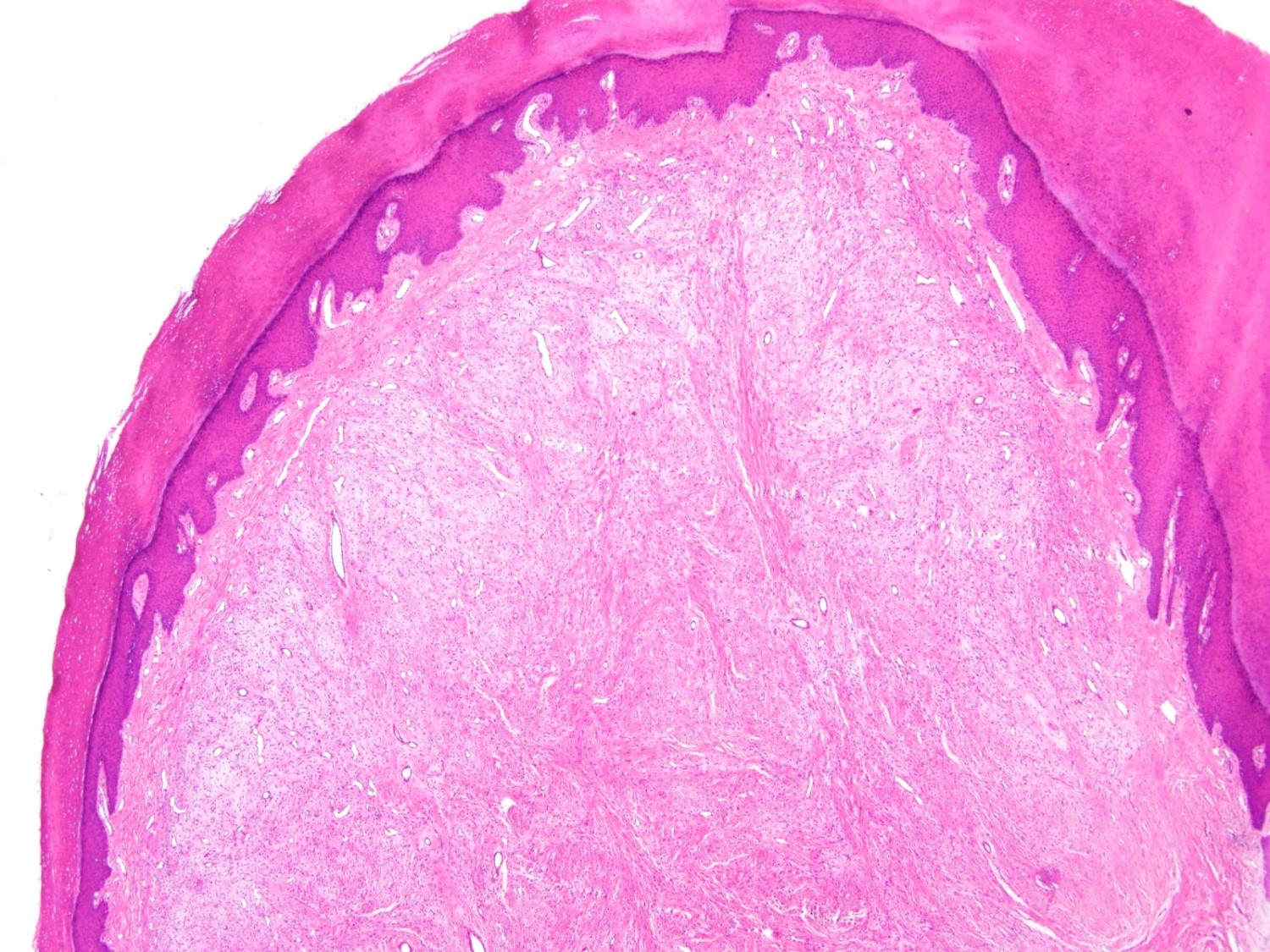
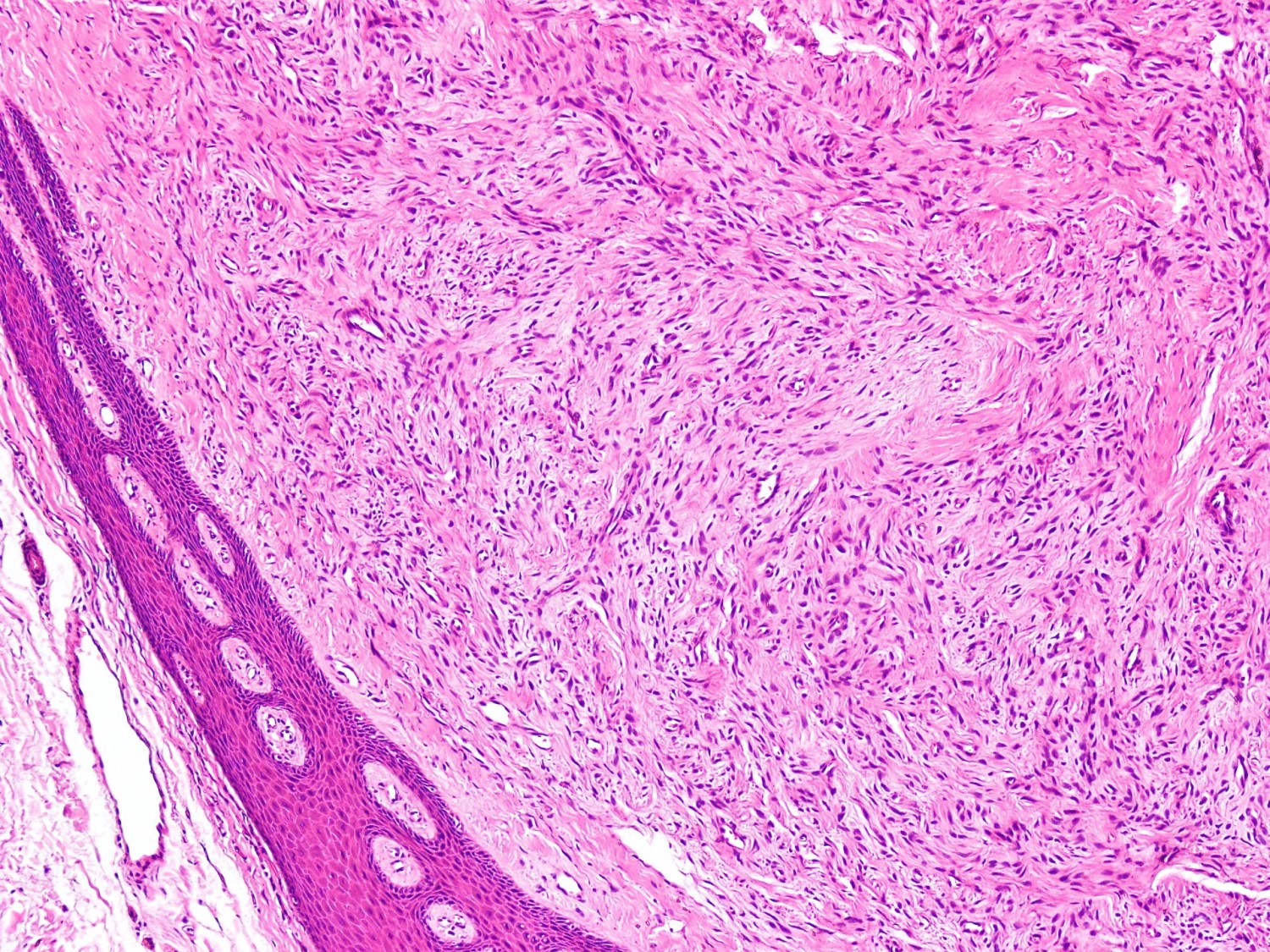
Polypoid acral skin lesion
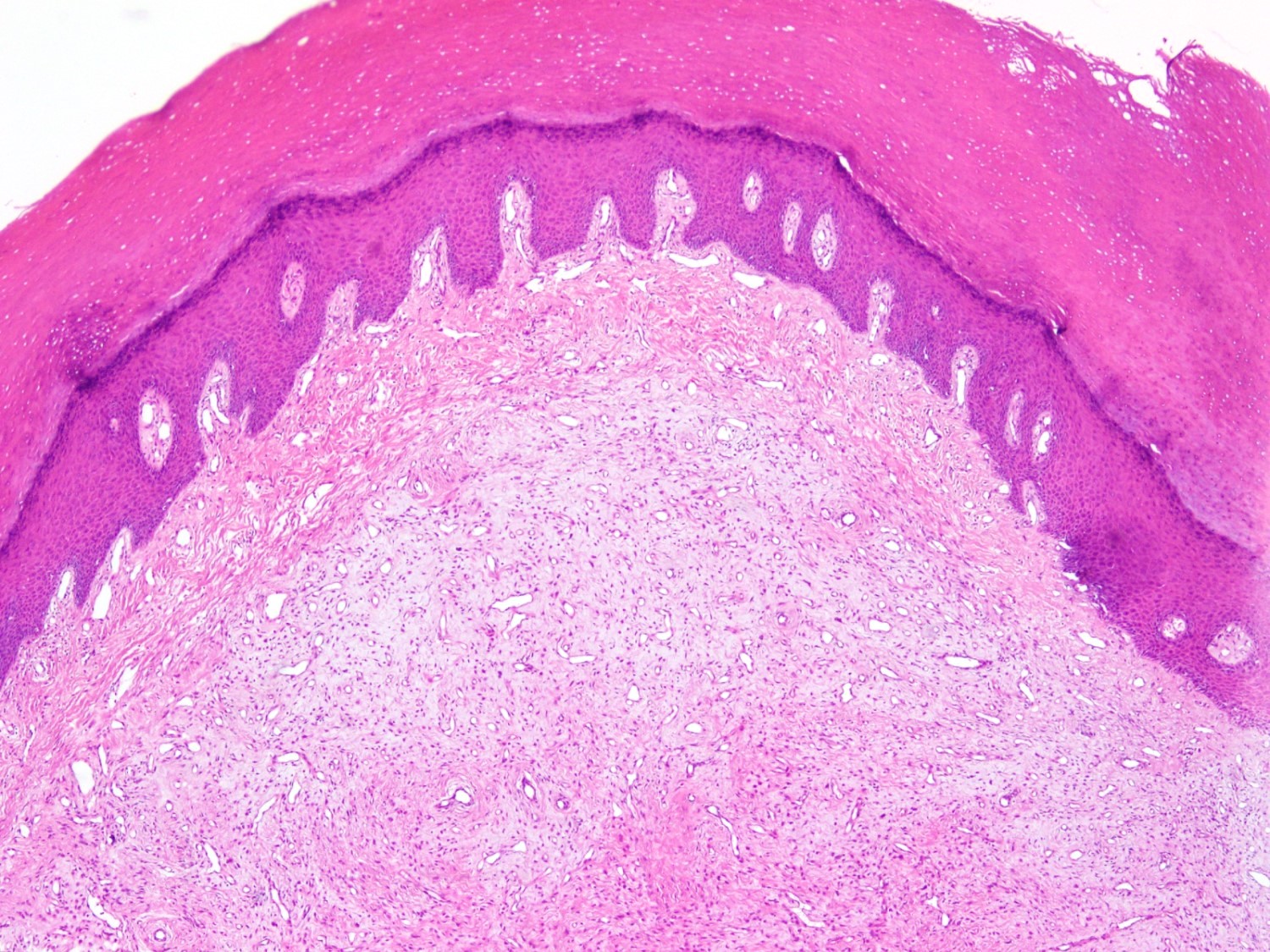
Acral skin lesion
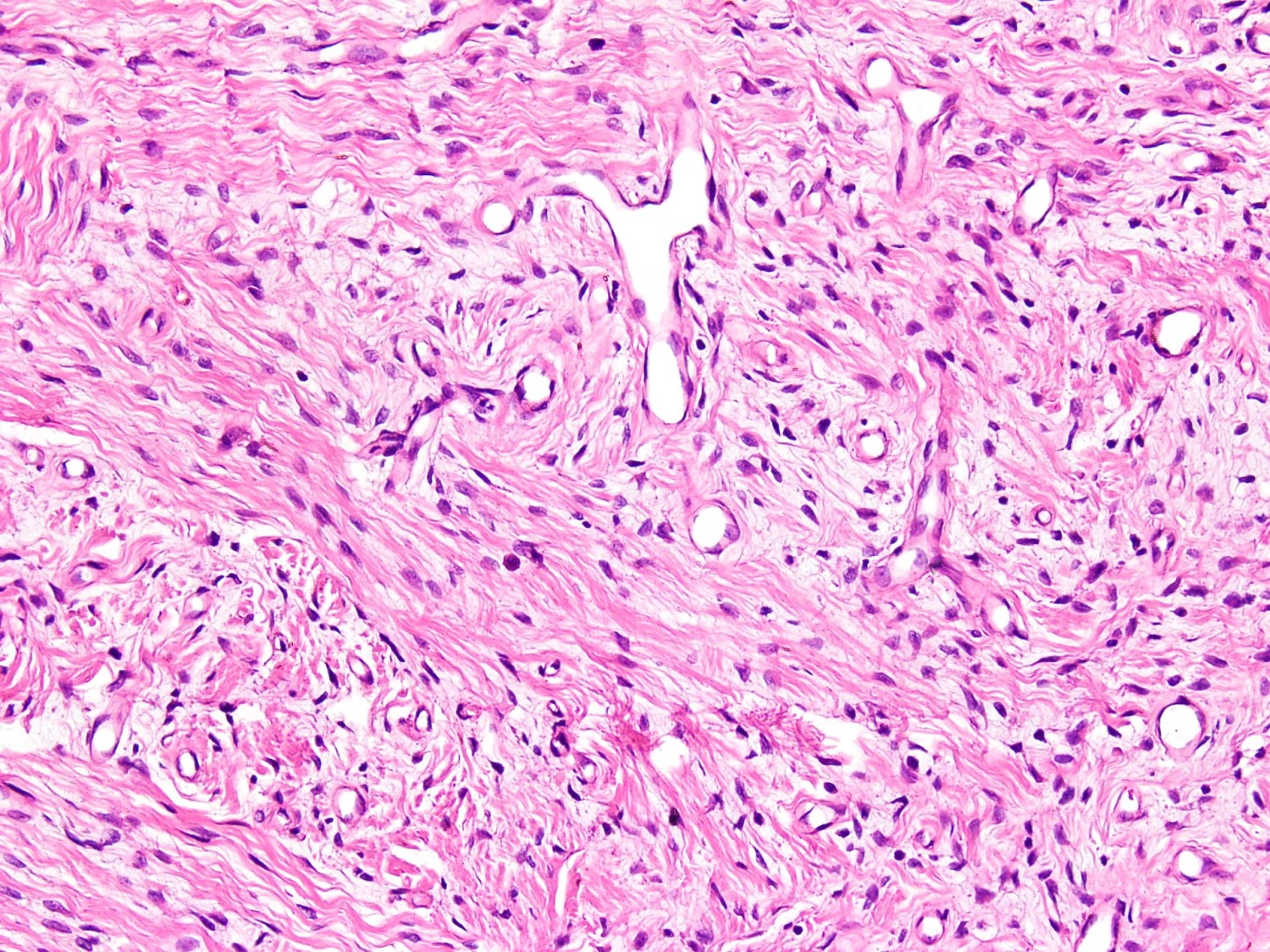
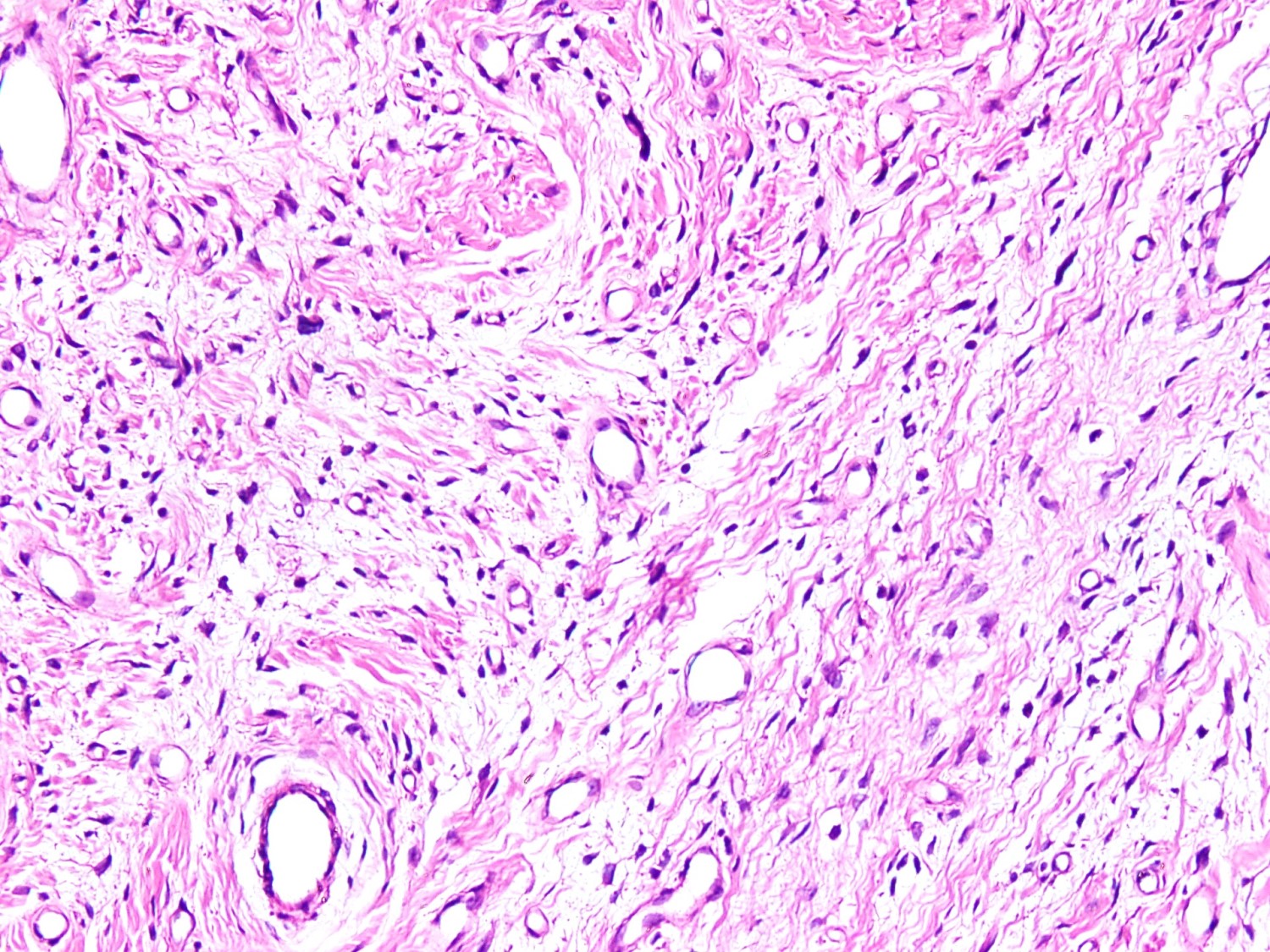
Spindle cell lesion
Giant cells
Storiform pattern
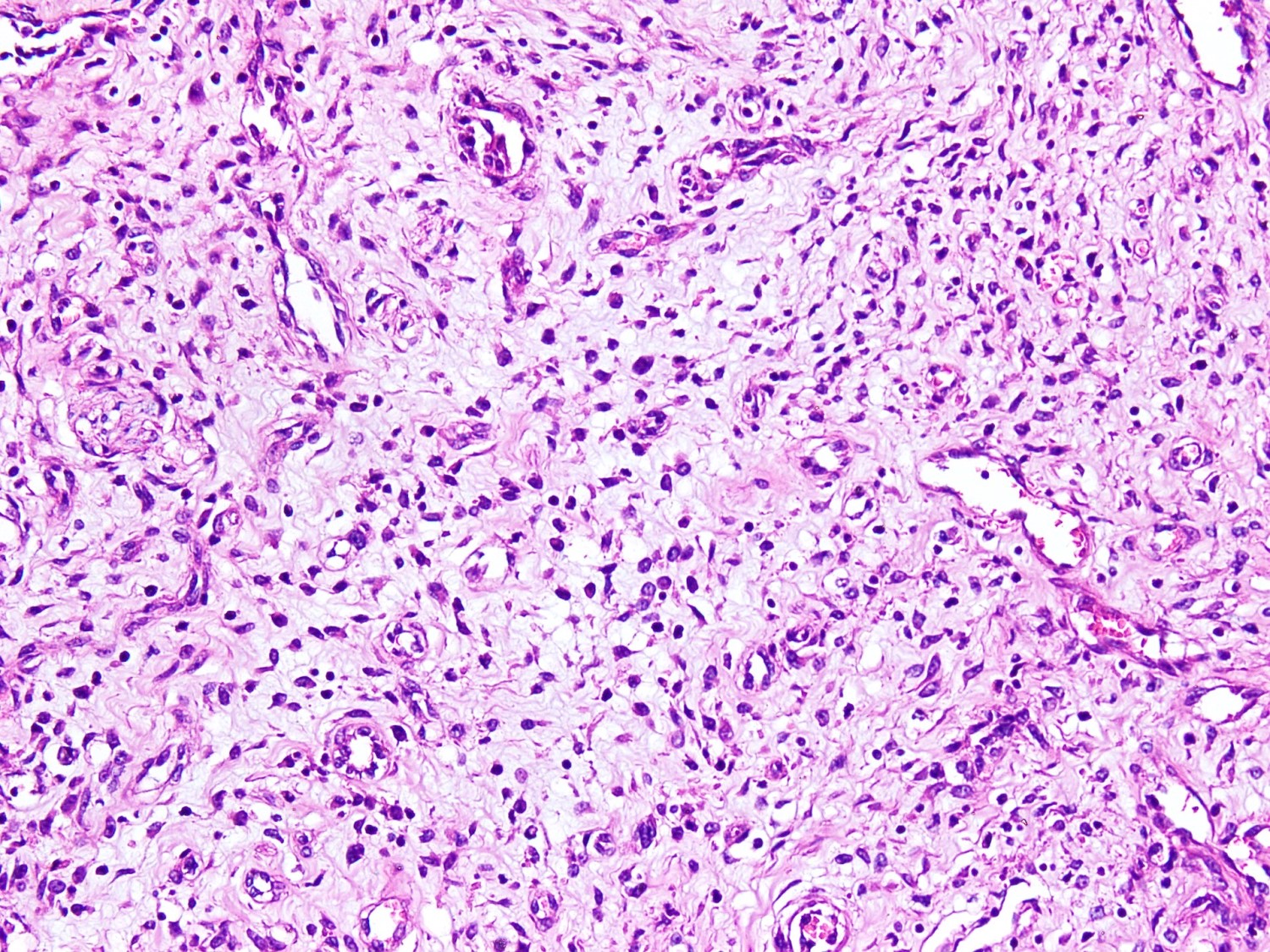
Cellular region
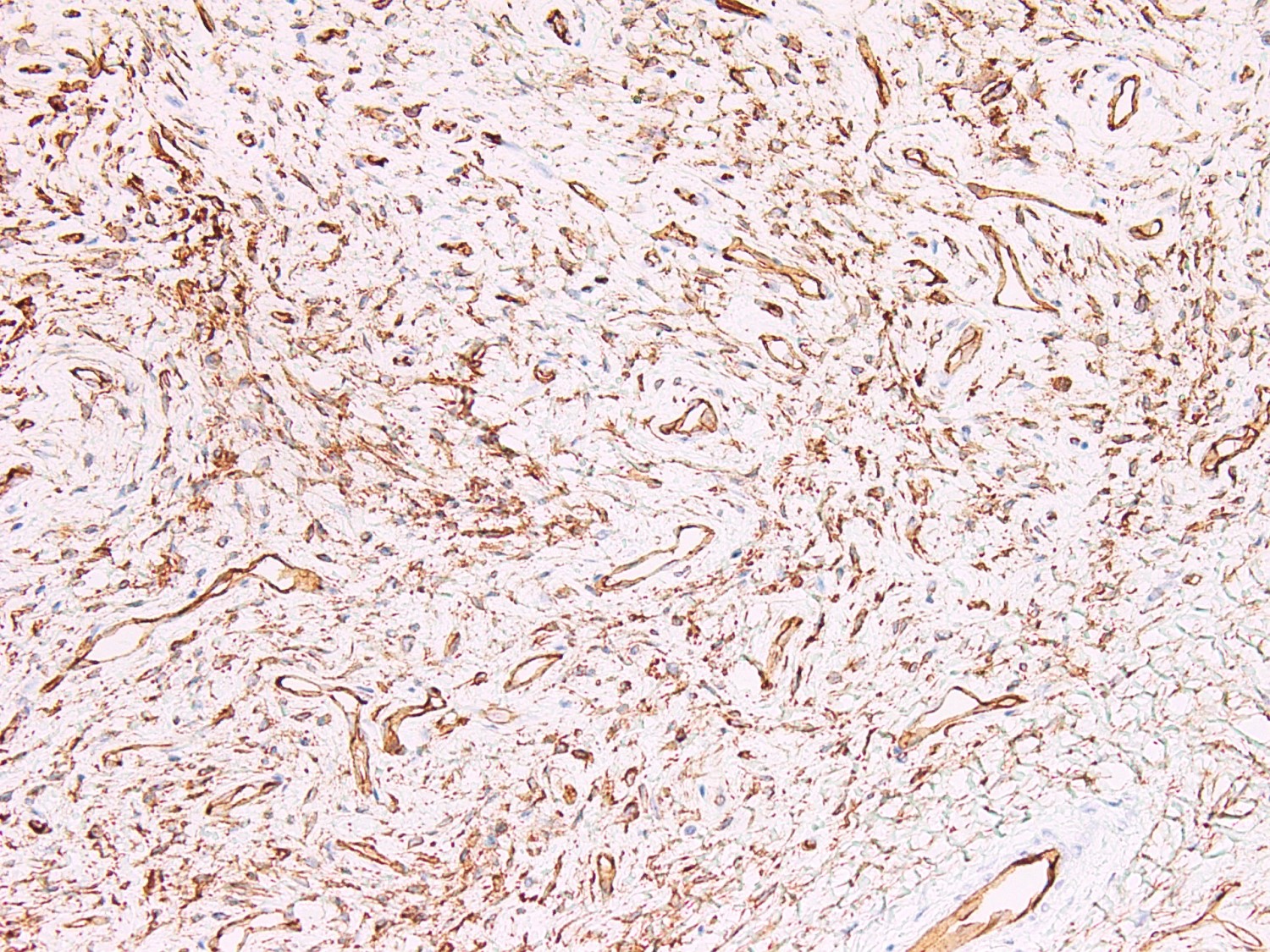
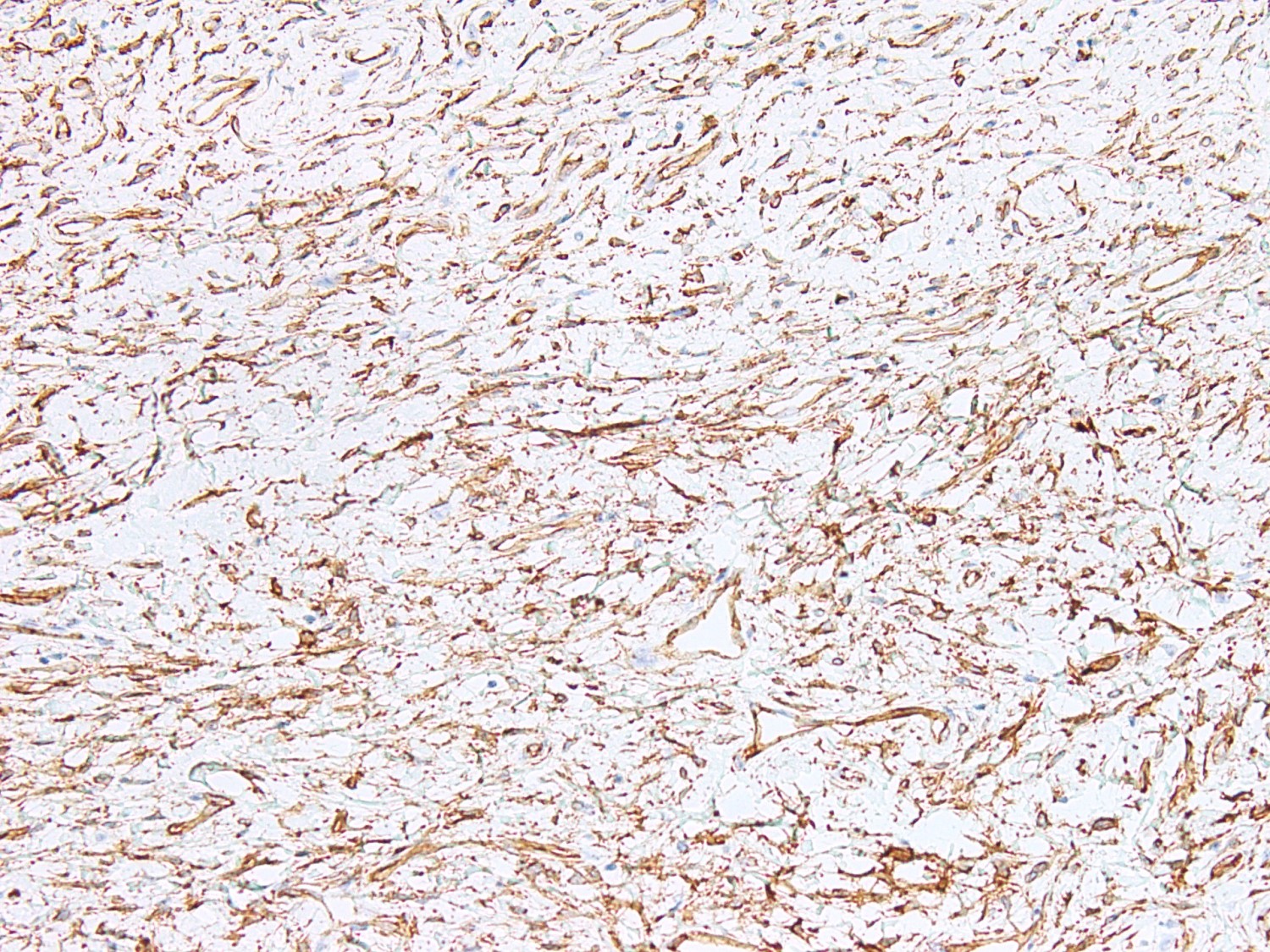
CD34 stain
Cytology description
- Oval to spindle cells with bland nuclear chromatin with background mucoid / myxoid material
- Groups and cohesive clusters of spindle cells with scattered thin walled capillaries (J Cytol 2015;32:39)
Cytology images
Images hosted on other servers:

Myxoid matrix with bland spindle cells
Positive stains
- CD34: diffuse and strong
- CD99: diffuse and strong (Rev Bras Ortop (Sao Paulo) 2019;54:491)
- EMA: focally positive
- Smooth muscle actin: focally positive
- CD10: less frequently (Ultrastruct Pathol 2009;33:293)
Negative stains
Electron microscopy description
- Fibroblastic origin
- Cytoplasmic intermediate filaments and large amount of rough endoplasmic reticulum cisternae (Ultrastruct Pathol 2009;33:293)
Molecular / cytogenetics description
- Deletion of the RB1 gene is detected but not required to establish the diagnosis
Videos
Superficial acral fibromyxoma
Sample pathology report
- Left big toe, excision biopsy:
- Acral fibromyxoma (see comment)
- Comment: There is a well circumscribed dermal based spindle cell neoplasm comprised of collagenous and myxoid areas. The stellate cells are bland, lacking atypia. Mitoses are rare. There is prominent thin vasculature. Scattered mast cells are noticed. Immunohistochemical stains for CD34 and CD99 are positive in spindle cells; features are consistent with superficial acral fibromyxoma, a benign fibroblastic tumor. The tumor is completely excised. Local recurrence is uncommon following complete excision.
Differential diagnosis
- Onychomatricoma:
- Rarely affects nail matrix
- Spindle shaped stromal cells with epithelial component
- CD34 is positive
- Myxoid neurofibroma:
- Superficial angiomyxoma:
- Acral fibrokeratoma:
- Polypoid dome shaped
- Dense collagenous stroma, mature spindle cells and small vessels
- Vertical orientation of collagen fibers
- Dermatofibrosarcoma protuberans (DFSP):
- Affecting trunk and extremities
- Myxoid DFSP is rare in digits
- Storiform pattern and deep infiltration in the subcutaneous fat
- CD34 is positive
- Fibroma of tendon sheath:
- Giant cell tumor of tendon sheath:
- Glomus tumor:
Additional references
Board review style question #1
A 30 year old woman presented with a slow growing painless subungual mass. Plain Xray revealed uninvolved bone. Magnetic resonance imaging (MRI) confirmed a soft tissue confined lesion without bone erosion. Excision specimen revealed histological features as shown in the given image. Which positive IHC stain helps confirm the diagnosis?
- CD34
- Desmin
- MUC4
- S100
- SMA
Board review style answer #1
A. CD34. In superficial acral fibromyxoma (SAF), only CD34 will be diffuse and strongly positive.
Answer E is incorrect because SMA is only focally positive and is not diagnostic, as it can be positive in many other spindle cell lesions. Answer D is incorrect because S100 is negative in SAF and will exclude nerve sheath tumor. Answer B is incorrect because desmin negativity excludes rhabdoid differentiation. Answer C is incorrect because MUC4 will be negative in SAF, which is a positive marker in low grade fibromyxoid sarcoma.
Comment Here
Reference: Superficial acral fibromyxoma
Comment Here
Reference: Superficial acral fibromyxoma
Board review style question #2
A 30 year old woman presented with a slow growing painless subungual mass. Plain Xray revealed erosion of underlying bone. Magnetic resonance imaging (MRI) confirmed a soft tissue lesion and bone erosion. Excision specimen revealed histological features as shown in the given H&E image. The provided IHC stain is CD34. What is the treatment of choice?
- Local excision
- Moh's microsurgery
- Neoadjuvant chemotherapy
- Radiation
- Wide excision
Board review style answer #2
A. Local excision. The current diagnosis of superficial acral fibromyxoma warrants only local excision with adequate margins. Answer B is incorrect because Moh's microsurgery is a procedure done for skin cancers, including basal cell carcinoma, squamous cell carcinoma and melanoma at critical sites like eyes, ear, nose and lips where excision margins are sent for frozen section to secure clear margins with minimal tissue defect. Answers C, D and E are incorrect because a benign diagnosis does not merit chemotherapy, radiation or wide excision.
Comment Here
Reference: Superficial acral fibromyxoma
Comment Here
Reference: Superficial acral fibromyxoma
