
Lymph nodes & spleen, nonlymphoma
Spleen-vascular tumors
Littoral cell angioma
Author: Patricia Tsang, M.D., M.B.A.
Editorial Board Member: Debra L. Zynger, M.D.
Deputy Editor-in-Chief: Genevieve M. Crane, M.D., Ph.D.
Last author update: 2 September 2022
Last staff update: 7 November 2023
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Littoral cell angioma spleen
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnostic criteria | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Tsang P. Littoral cell angioma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/spleenlittoralcellangioma.html. Accessed April 20th, 2024.
Definition / general
- Rare, typically benign splenic vascular tumor
- Originates from littoral cells lining splenic red pulp sinuses
Essential features
- Strong association with diverse immunologic and neoplastic disorders
- Presentation varies from asymptomatic and incidental to fever, pain and cytopenias related to hypersplenism
- Dual endothelial and histiocytic differentiation of tumor cells, similar to normal splenic littoral cells
- CD34 is characteristically absent while other endothelial cell antigens are expressed
Terminology
- Littoral cell angioma of the spleen
ICD coding
- ICD-10: D73.89 - other diseases of spleen
Epidemiology
- Mostly in middle aged adults
- Median age: 50 years (range: 1 - 86 years)
- M = F (Int J Clin Exp Pathol 2015;8:8516)
Sites
- Unique to the spleen
Pathophysiology
- Immunodysregulation is postulated to explain the clinical association with various malignancies or immune / autoimmune disorders (Histopathology 2016;69:762)
Etiology
- Unknown etiology
Clinical features
- Almost always benign with exceedingly rare malignant transformation
- 50% asymptomatic (World J Gastroenterol 2015;21:6660)
- 50% present with splenomegaly, hypersplenism associated thrombocytopenia and anemia, abdominal pain, fever or weight loss (Histopathology 2016;69:762, World J Gastroenterol 2015;21:6660)
- 36% associated with immune / autoimmune / metabolic disorders, such as Crohn's disease or immune thrombocytopenic purpura (Blood 2017;129:1564)
- 40 - 60% associated with malignancies, such as colonic adenocarcinoma, pancreatic tumor, lung carcinoma, renal cell carcinoma, lymphoma, myelodysplasia, aplastic anemia or testicular seminoma (Histopathology 2016;69:762)
Diagnostic criteria
- Splenomegaly with nodules composed of benign tortuous vascular channels
- Dual endothelial and histiocytic immunophenotype lacking CD34
Laboratory
- Thrombocytopenia, anemia in subset of patients
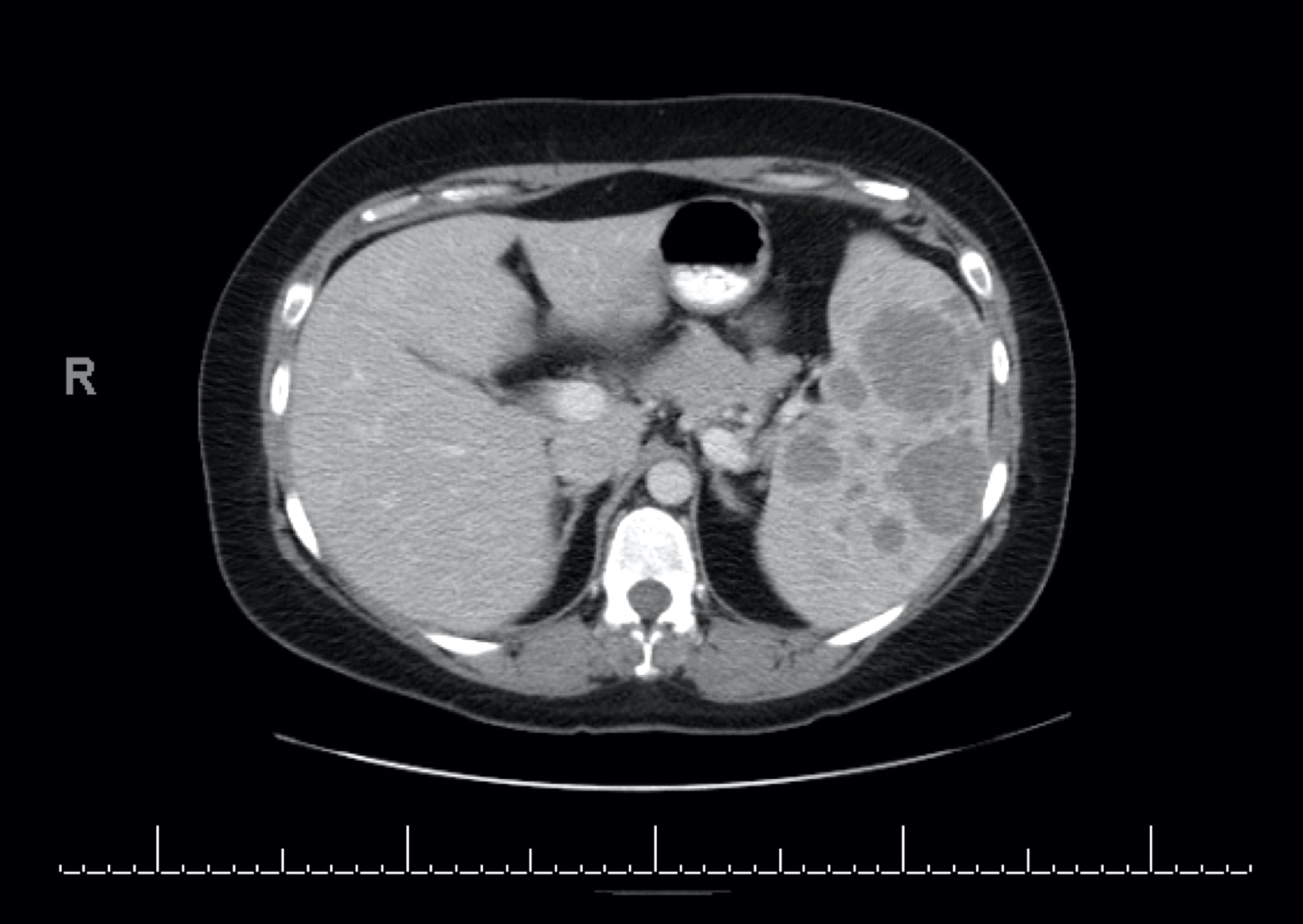
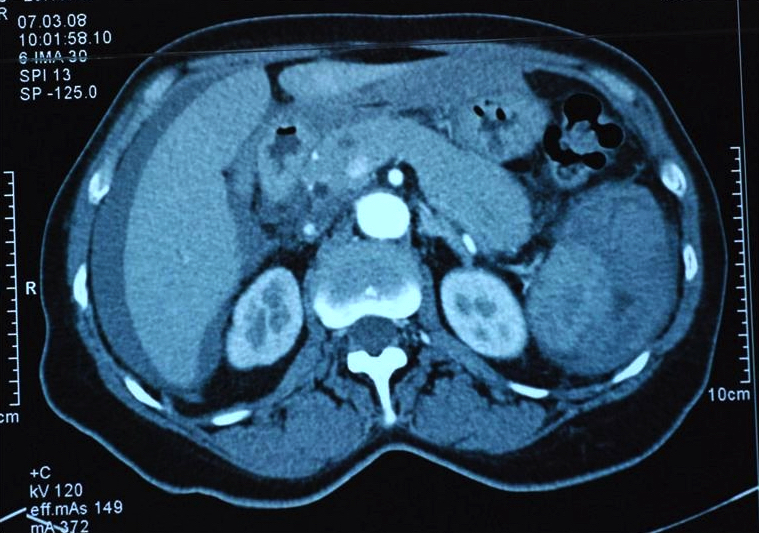
Radiology description
- Enlarged spleen
- Ultrasound varies from heterogeneous echotexture without specific nodules to hyperechogenic, hypoechogenic or isoechogenic lesions
- CT shows solitary or multiple hypoattenuating nodules (BMJ Case Rep 2015;2015:bcr2015212882)
- MRI shows hypodense lesions on T1 and T2 weighted scans due to hemosiderin (Int J Clin Exp Pathol 2015;8:8516)
Radiology images
Prognostic factors
- Typically benign with excellent prognosis postsplenectomy
- Increased risk of malignant transformation with massive splenomegaly (> 1,500 g or > 20 cm long) (Minerva Chir 2014;69:229)
- Rare reports of recurrence in accessory spleen or metastasis (Medicine (Baltimore) 2018;97:e0378)
Case reports
- 30 year old man presented with abdominal pain, fever and multiple splenic masses (Acta Chir Belg 2021;121:357)
- 38 year old man with splenic, renal and hepatic cysts (Arch Pathol Lab Med 2001;125:1505)
- 43 year old man with prior pulmonary sarcoidosis (World J Surg Oncol 2011;9:106)
- 45 year old man with obstructive jaundice (Indian J Pathol Microbiol 2012;55:109)
- 46 year old women and 52 year old man with littoral cell angioma detected during physical examination (Chin Med J (Engl) 2011;124:3423)
- 58 year old woman with large solitary littoral cell angioma (J Clin Imaging Sci 2012;2:69)
- 60 year old man with rapid increase in size of spleen (Rare Tumors 2010;2:e17)
- 61 year old woman with metastasis to the liver treated with chemotherapy (Medicine (Baltimore) 2018;97:e0378)
Treatment
- Splenectomy
- Management of any potential complications of asplenia (e.g., severe infection and thrombosis)
- Clinical evaluation for any coexisting neoplastic or immune disorders (World J Gastroenterol 2015;21:6660)
Gross description
- Solitary or multiple distinct splenic nodules (solitary to multiple ratio is ~0.3:1) (Front Oncol 2022;12:790332)
- Minute to large nodules of variable consistency
- Various colors (yellow / brown / red / black) depending on degree of necrosis, cyst formation, thrombi and fibrosis (Int J Clin Exp Pathol 2015;8:8516)
- Spongy / cystic (J Cytol 2017;34:121)
- Well demarcated but lacking a fibrous capsule
Gross images



Microscopic (histologic) description
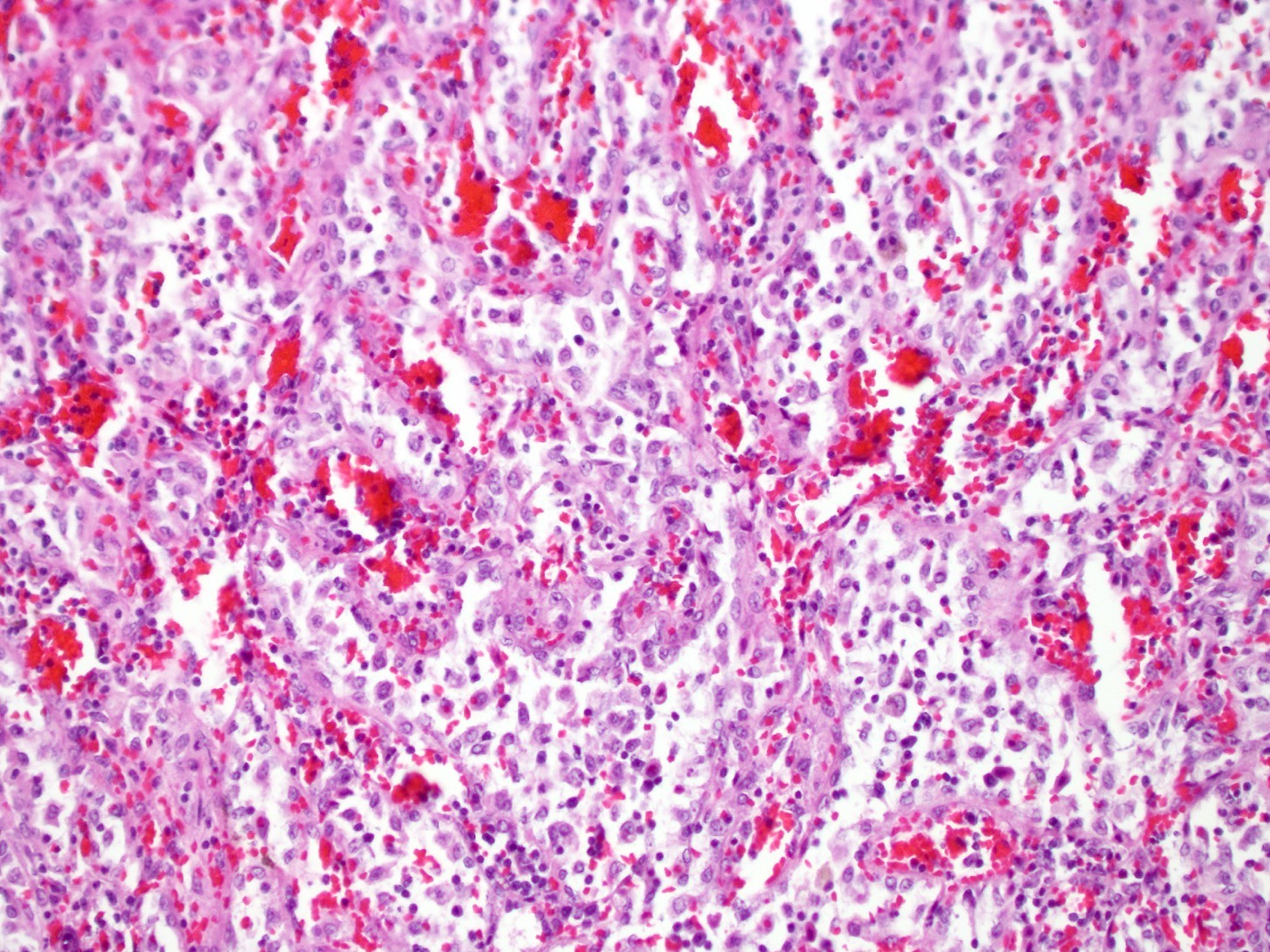
- Proliferation of anastomosing, tortuous, blood filled vascular channels (Int J Clin Exp Pathol 2015;8:8516)
- Irregular channel lumina, often with papillary projections and cystic spaces
- Lined by tall endothelial cells with variable hemophagocytosis (BMJ Case Rep 2015;2015:bcr2015212882)
- Sloughing of endothelial cells into vascular spaces
- No sclerosis or cytologic atypia
Microscopic (histologic) images
Contributed by Patricia Tsang, M.D., M.B.A.
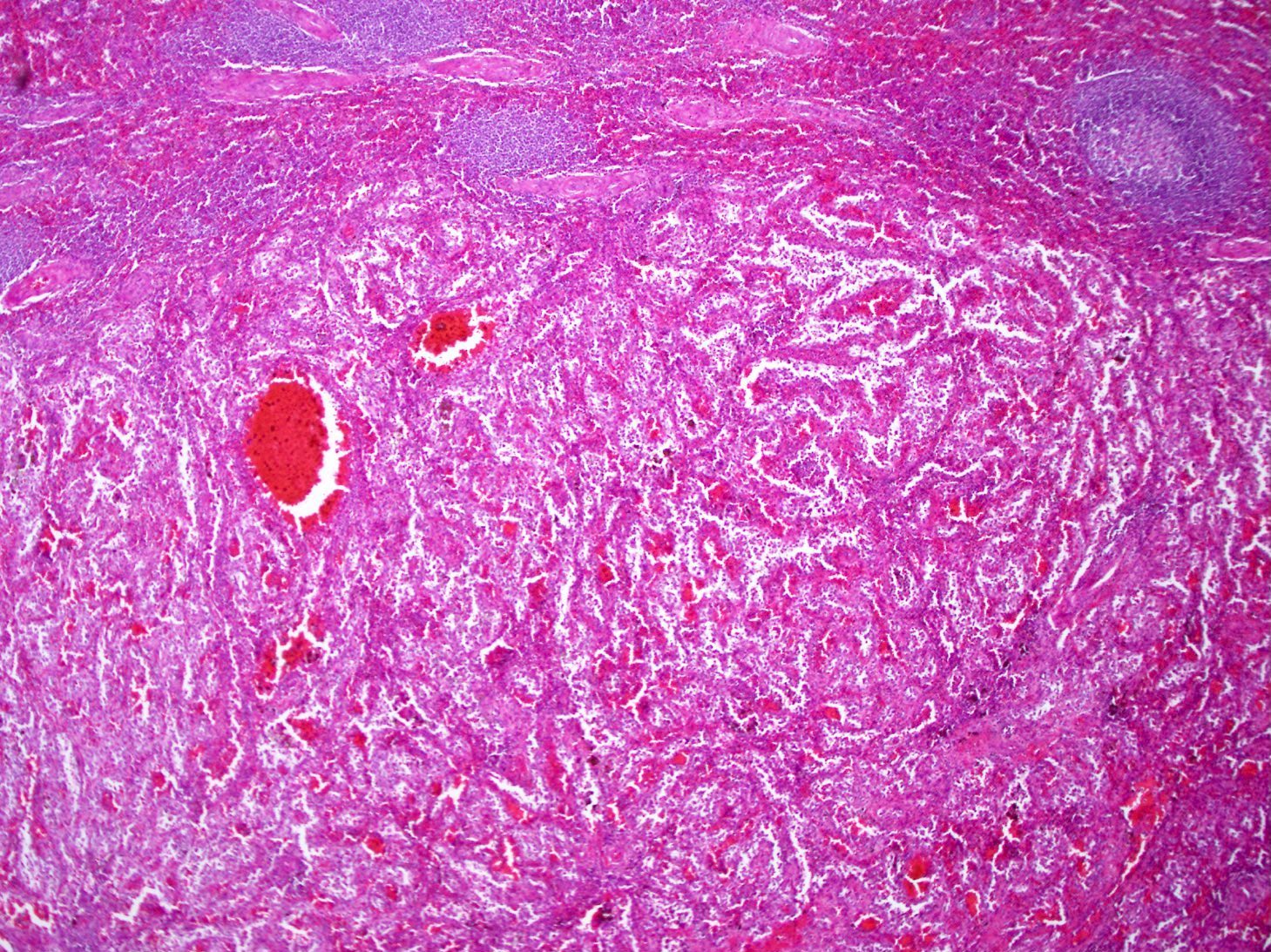
Tortuous vascular channels

Anastomosing vascular channels
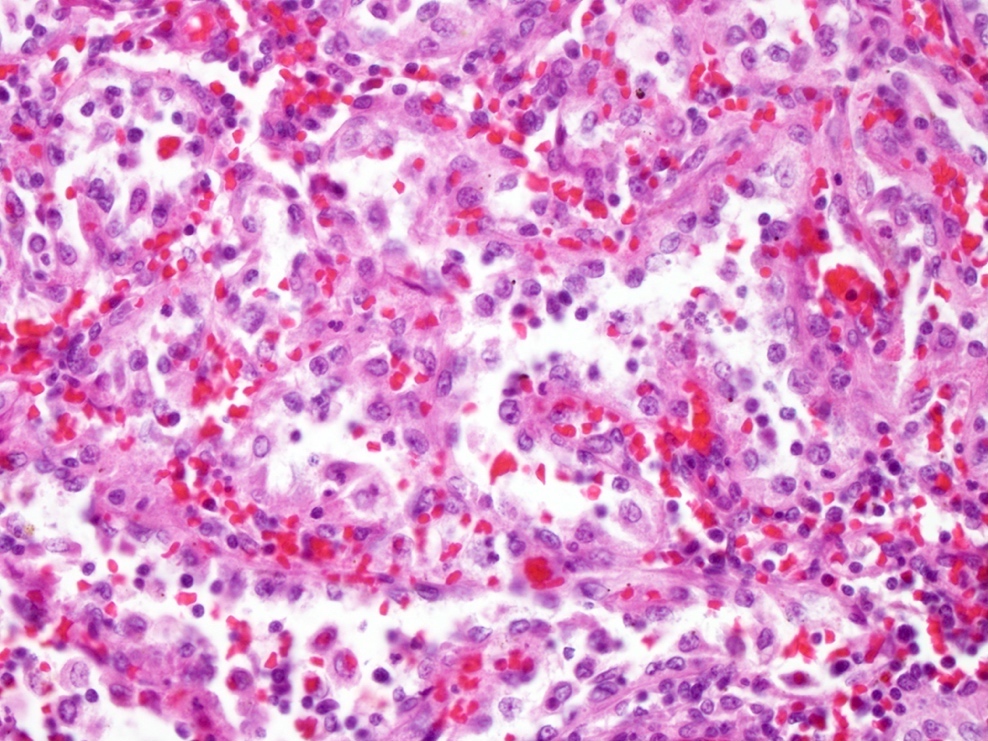
Vascular channels appear papillary
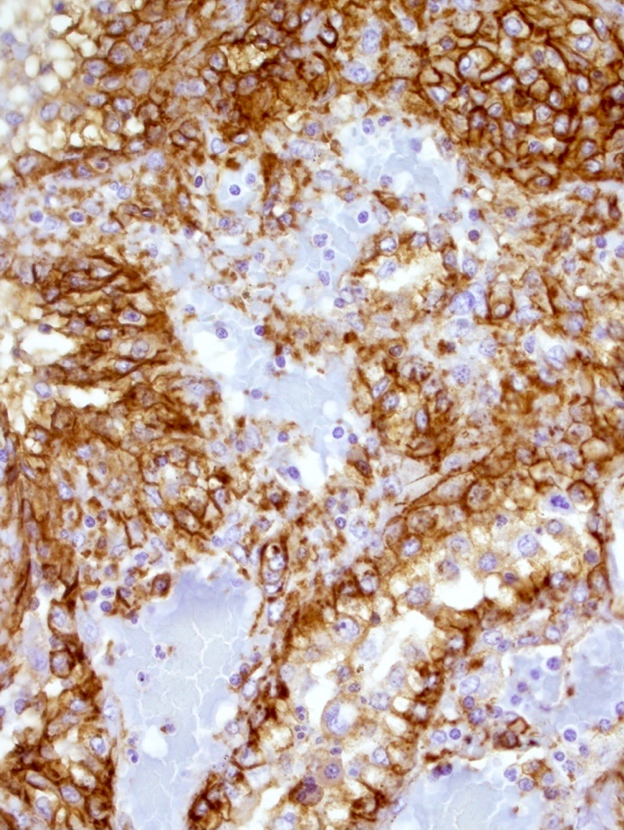
CD31
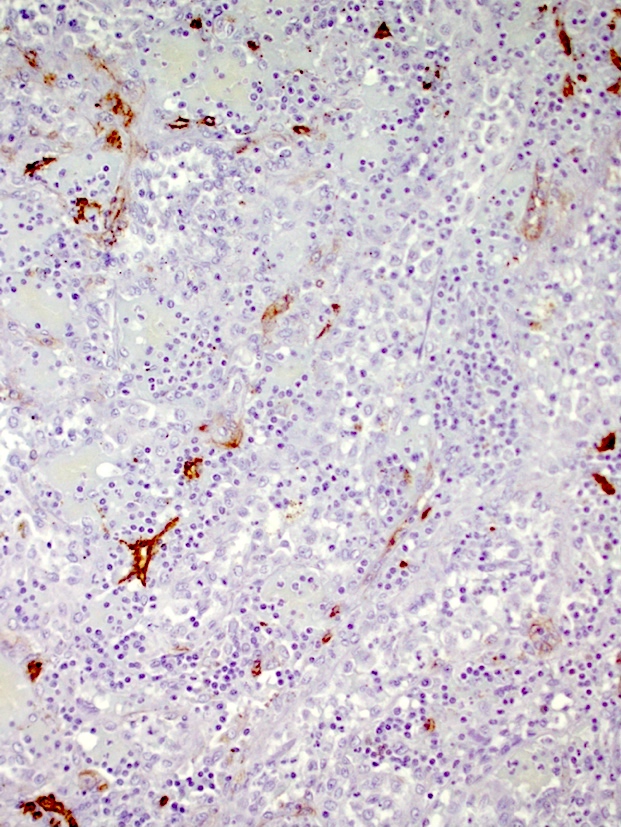
CD34
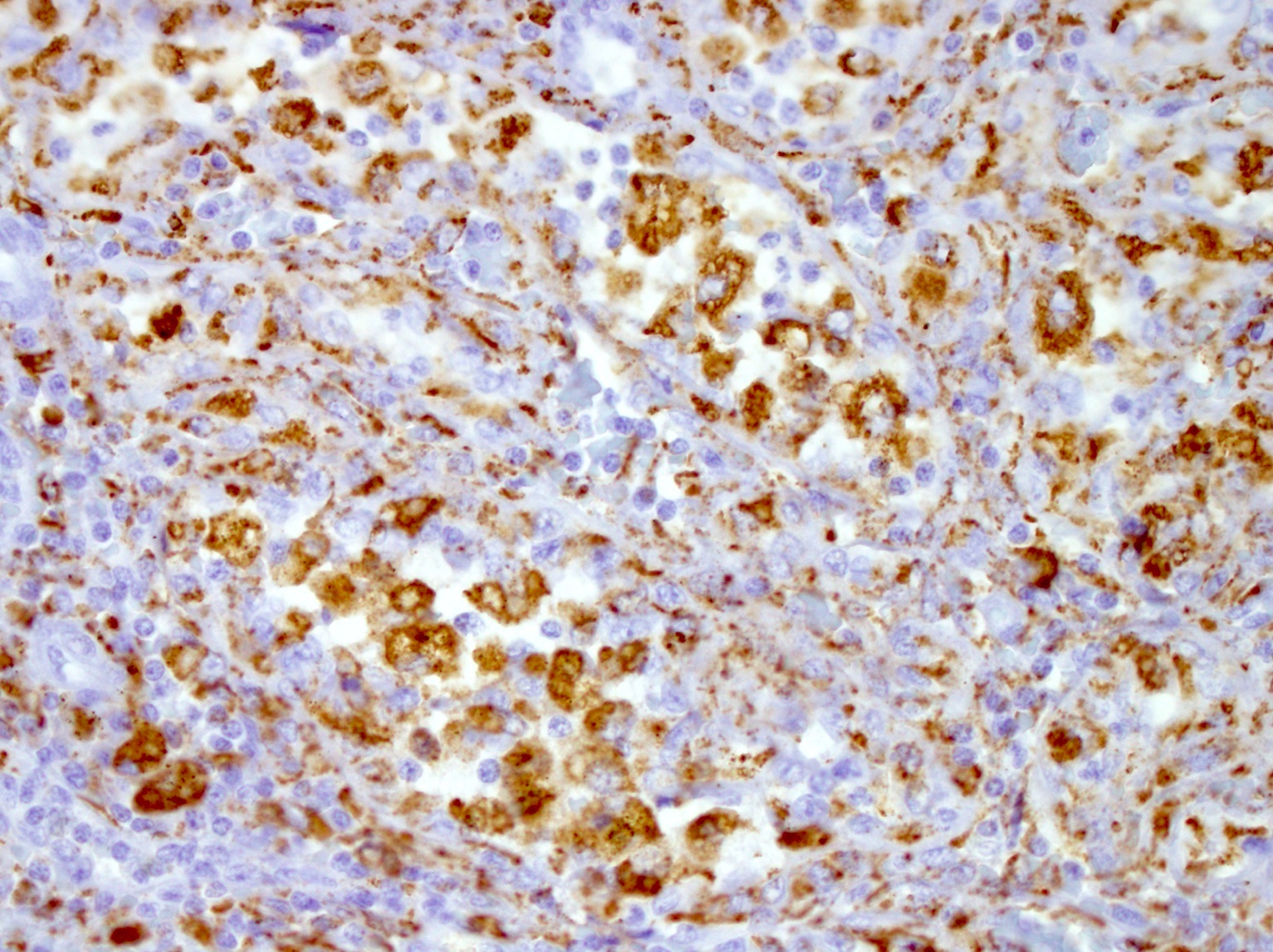
CD68
Cytology description
- 3 dimensional, bland appearing, epithelioid foamy cells with low N:C ratio (J Cytol 2017;34:121)
- May contain intracytoplasmic hemosiderin pigment
Positive stains
- Dual endothelial (factor VIII, CD31, von Willebrand factor) and histiocytic (CD4, CD68, CD163, FLI1, MAC387, HAM56, lysozyme) differentiation (Histopathology 2016;69:762)
- Langerin (CD207) (Hum Pathol 2019;83:43)
- CD21
- Vimentin
- Cyclin D1
- Low Ki67 proliferative index
- S100 (variable; 20%) (Hum Pathol 2019;83:43)
Negative stains
- CD34 (characteristically absent despite expression of other endothelial cell antigens)
- ERG and WT1 vascular endothelial cell markers (Ann Diagn Pathol 2015;19:143)
- CD45, CD8 (usually negative), CD117, HHV8, CD1a, cytokeratins
Molecular / cytogenetics description
- No specific molecular findings
Sample pathology report
- Spleen, splenectomy:
- Littoral cell angioma (see comment)
- Comment: The nodule in the splenic red pulp is composed of tortuous blood vessels lined by plump endothelial cells that form papillary projections into the lumina. No overt cytologic atypia or mitoses are seen. The white pulp is histologically unremarkable.
- Immunohistochemistry demonstrates dual endothelial and histiocytic differentiation of the vascular lining cells. The phenotypic profile is as follows: CD31+, factor VIII+, CD68+, lysozyme+, langerin+. Not expressed are CD34, CD117 and HHV8. The proliferative fraction based on Ki67 is low (about 15%).
- The overall findings are characteristic of splenic littoral cell angioma, which is benign in most cases. However, this lesion may be seen in association with a variety of neoplastic and immune / autoimmune conditions. Clinical correlation and follow up are suggested.
Differential diagnosis
- Angiosarcoma:
- Atypical sarcomatous cells with hyperchromatic nuclei
- Frequent tumor necrosis, high mitotic rate and poor demarcation
- CD34+
- Hamartoma:
- Disorganized blood vessels with entrapped adipocytes
- CD8+
- Splenic littoral cell hemangioendothelioma:
- Typically mild to moderate cytologic atypia
- May have solid areas
- Potentially malignant or metastasizing
- Kaposi sarcoma:
- Hemangioma:
- Hemangiopericytoma:
- Lymphangioma:
- Cystic, malformed lymphatic channels, often subcapsular
- Attenuated endothelial lining
- Lacks histiocytic markers and langerin
Additional references
Board review style question #1
A 55 year old man presents with abdominal pain and multiple splenic nodules. The microscopic H&E image is shown above. The proliferative fraction is 20%. Which of the following immunostains is expected to be negative?
- CD31
- CD34
- CD68
- Factor VIII
Board review style answer #1
B. CD34. The photomicrograph shows anastomosing vascular channels in the spleen with sloughing of plump endothelial cells into the lumina, morphologically consistent with littoral cell angioma. The proliferative fraction is low. CD34 is characteristically negative in littoral cell angioma, while other vascular endothelial cell associated markers (CD31 and factor VIII) are positive. The histiocytic marker CD68 is also characteristically expressed.
Comment Here
Reference: Littoral cell angioma
Comment Here
Reference: Littoral cell angioma
Board review style question #2
Which of the following statements is true about littoral cell angioma of the spleen?
- Hypersplenism related anemia or thrombocytopenia is a well recognized manifestation
- It is pathogenetically linked to human herpesvirus 8 (HHV8)
- It originates from the white pulp vascular lining cells of the spleen
- Malignant transformation is common among middle aged and elderly patients
Board review style answer #2
A. Hypersplenism related anemia or thrombocytopenia is a well recognized manifestation. Hypersplenism in patients with littoral cell angioma can cause entrapment of RBCs and platelets in the spleen, leading to anemia and thrombocytopenia.
Comment Here
Reference: Littoral cell angioma
Comment Here
Reference: Littoral cell angioma
