

Thyroid & parathyroid
Benign thyroid neoplasms
Follicular adenoma

Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed search: Thyroid follicular adenoma

- Benign, encapsulated tumor that exhibits thyroid follicular cell differentiation
- Lacks capsular and vascular invasion
- Absent nuclear features of papillary thyroid carcinoma
- Benign thyroid tumor, lacking infiltrative properties and usually exhibiting follicular architecture
- Needs to be differentiated from adenomatoid thyroid nodule and other follicular patterned thyroid neoplasms
- ICD-O: 8330/0 - follicular adenoma
- Incidence: 3 - 5%
- Adults, wide age range; usually in fifth to sixth decades (Clin Endocrinol (Oxf) 2018;88:936)
- Female preponderance
- Either thyroid lobe, isthmus, ectopic thyroid tissue
- Usually sporadic
- Radiation exposure (Cancer 2003;97:2397)
- Iodine deficiency (Cancer 1987;60:3096)
- Familial tumor syndromes
- PTEN (phosphatase and tensin homolog deleted on chromosome ten): younger age of presentation; multiple and bilateral (Ann Diagn Pathol 1999;3:331)
- Carney complex (Diagn Histopathol 2017;23:366)
- MEN1 syndrome (Wermer syndrome)
- McCune-Albright syndrome
- Familial multinodular goiter (FMNG) syndrome
Images hosted on other servers:

Diagnostic capsular invasions

Incomplete / questionable capsular invasions
- Painless solitary thyroid nodule
- May be detected incidentally (during palpation or neck ultrasound)
- Rarely compression symptoms, if large
- Hyperthyroidism in case of hyperfunctioning adenomas (Plummer adenoma)
- Reference: Surg Clin North Am 2014;94:499
- Diagnostic workup is similar to any thyroid nodule
- Ultrasound with fine needle aspiration cytology (FNAC)
- Thyroid function test; usually euthyroid
- Can be hyperthyroid in case of hyperfunctioning adenoma
- Sonography: solid / solid cystic nodule, smooth and well defined margins, homogeneous or heterogeneous echotexture, isoechoic or hypoechoic, occasionally peripheral hypoechoic halo (Asian J Surg 2020;43:339, J Ultrasound Med 2014;33:221, AJR Am J Roentgenol 2010;194:44)
- Doppler ultrasound: absent or low blood flow
- Radionuclide scan: cold nodule; hot nodule if hyperfunctioning
Images hosted on other servers:


Ultrasound

Ultrasound


Color Doppler sonogram



Color Doppler sonogram
- Benign tumor
- 3 year old girl with adenochondroma of the thyroid gland (Ear Nose Throat J 2021;100:412S)
- 12 year old boy with follicular adenoma harboring BRAF K601E mutation (Int J Surg Pathol 2017;25:348)
- 29 year old woman with clear cell follicular adenoma of ectopic thyroid (Endocr Pathol 1998;9:339)
- 39 year old woman with follicular adenoma having intracytoplasmic lumina (Cytopathology 2016;27:495)
- 45 year old woman with follicular adenoma with papillary architecture (Cytopathology 2015;26:256)
- 48 year old woman with renal cell carcinoma metastatic to follicular adenoma of thyroid gland (Acta Cytol 2004;48:64)
- 58 year old woman with Plummer adenoma following percutaneous thyroid ethanol injection in thyroid gland (Case Rep Endocrinol 2017;2017:1026139)
- 59 year old woman with metastasis of colonic adenocarcinoma to thyroid follicular adenoma (Pathol Int 2005;55:574)
- 61 year old man with clear cell follicular adenoma of thyroid (Exp Clin Endocrinol Diabetes 2010;118:19)
- 61 year old man with follicular adenoma showing spindle cell metaplasia (Am J Surg Pathol 2019;24:84)
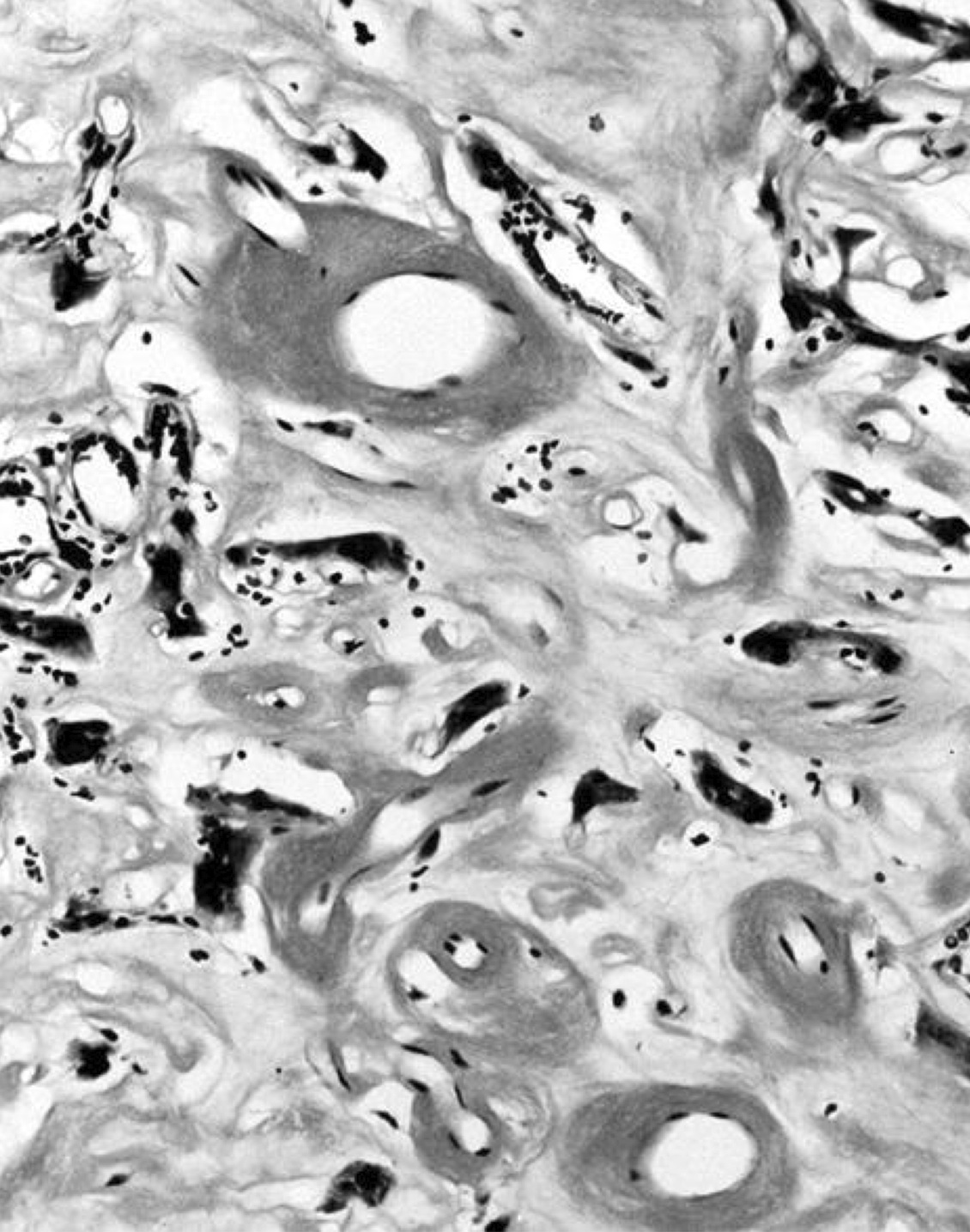
- 63 year old woman with follicular adenoma showing osseous metaplasia (Int J Surg Case Rep 2017;37:83)
- 72 year old man with follicular adenoma showing chondroid metaplasia (Histopathology 1991;18:278)
- 75 year old woman with follicular adenoma showing cellular atypia and mimicking anaplastic thyroid carcinoma on cytology (Diagn Cytopathol 2017;45:928)
- Lobectomy
- Hyperfunctioning follicular adenomas: lobectomy preferred over radioiodine (Oncologist 2011;16:585)
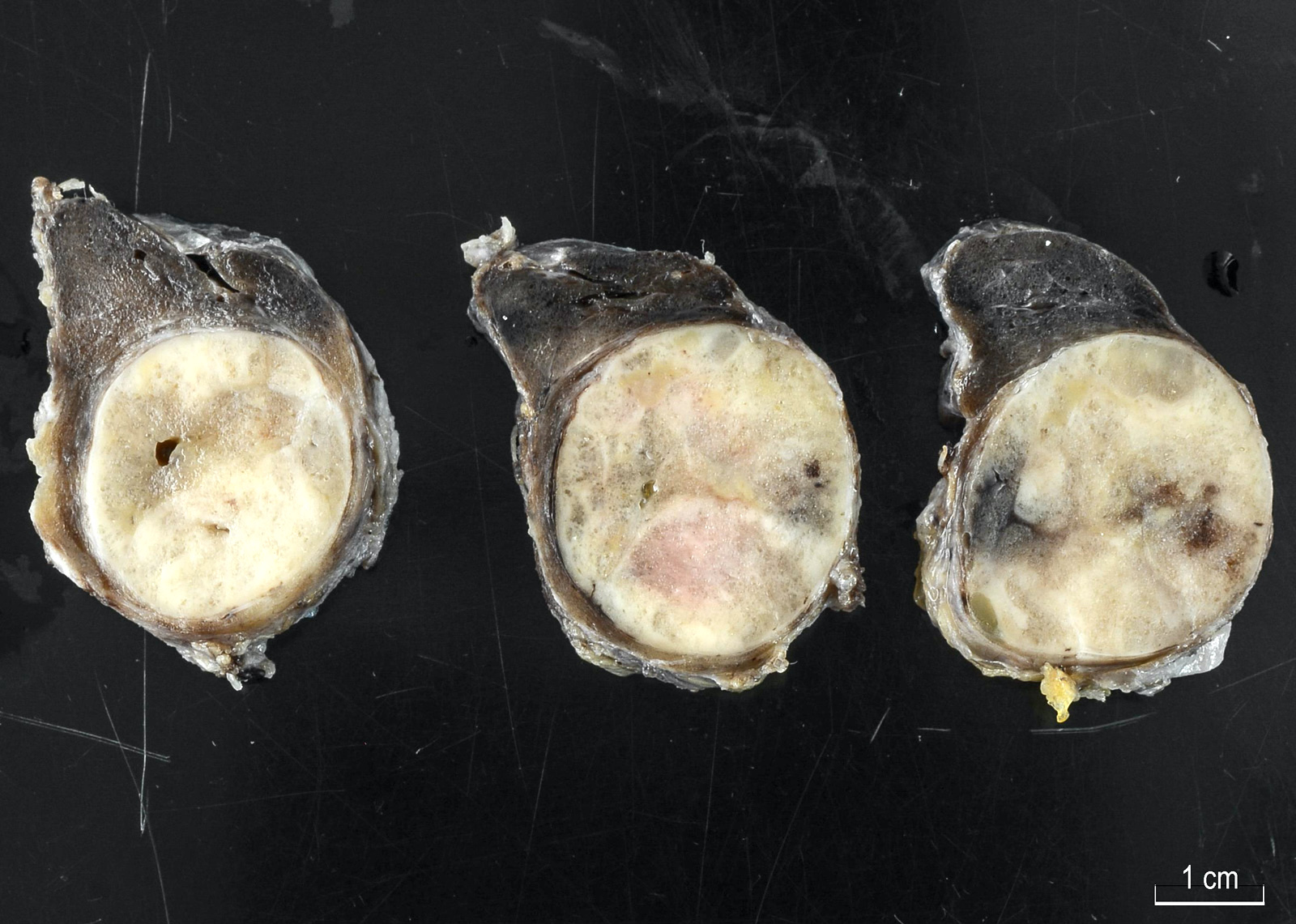
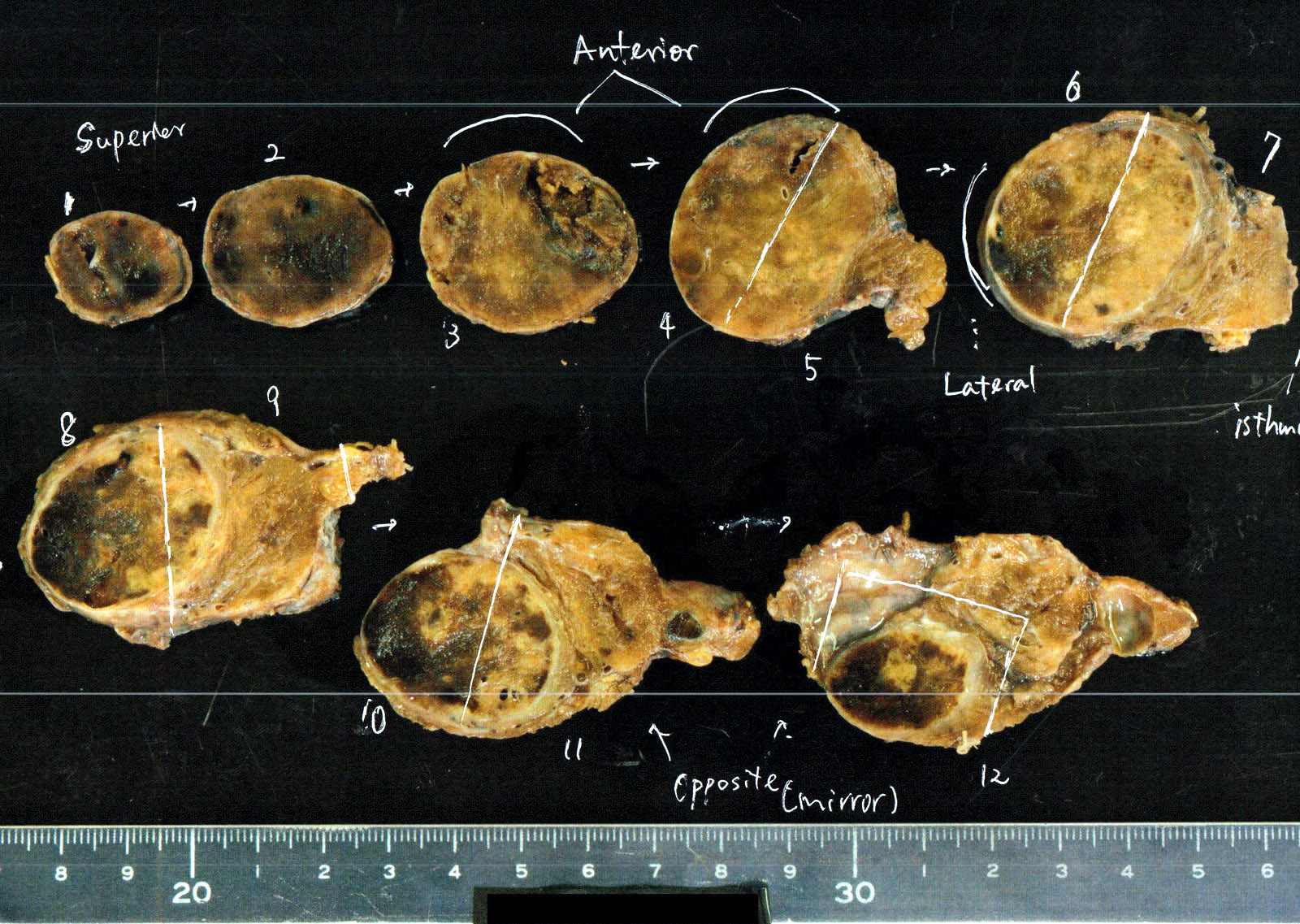
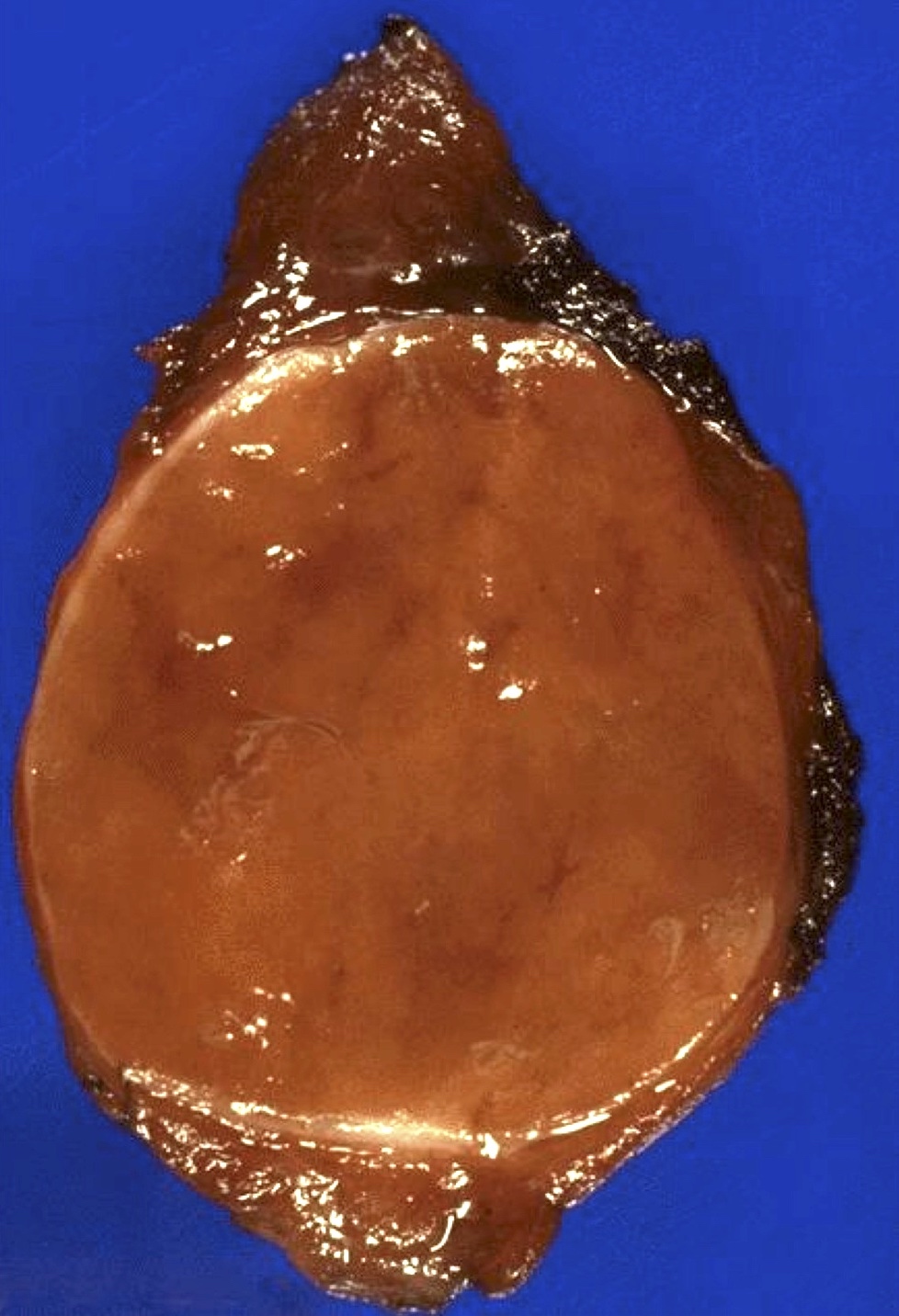
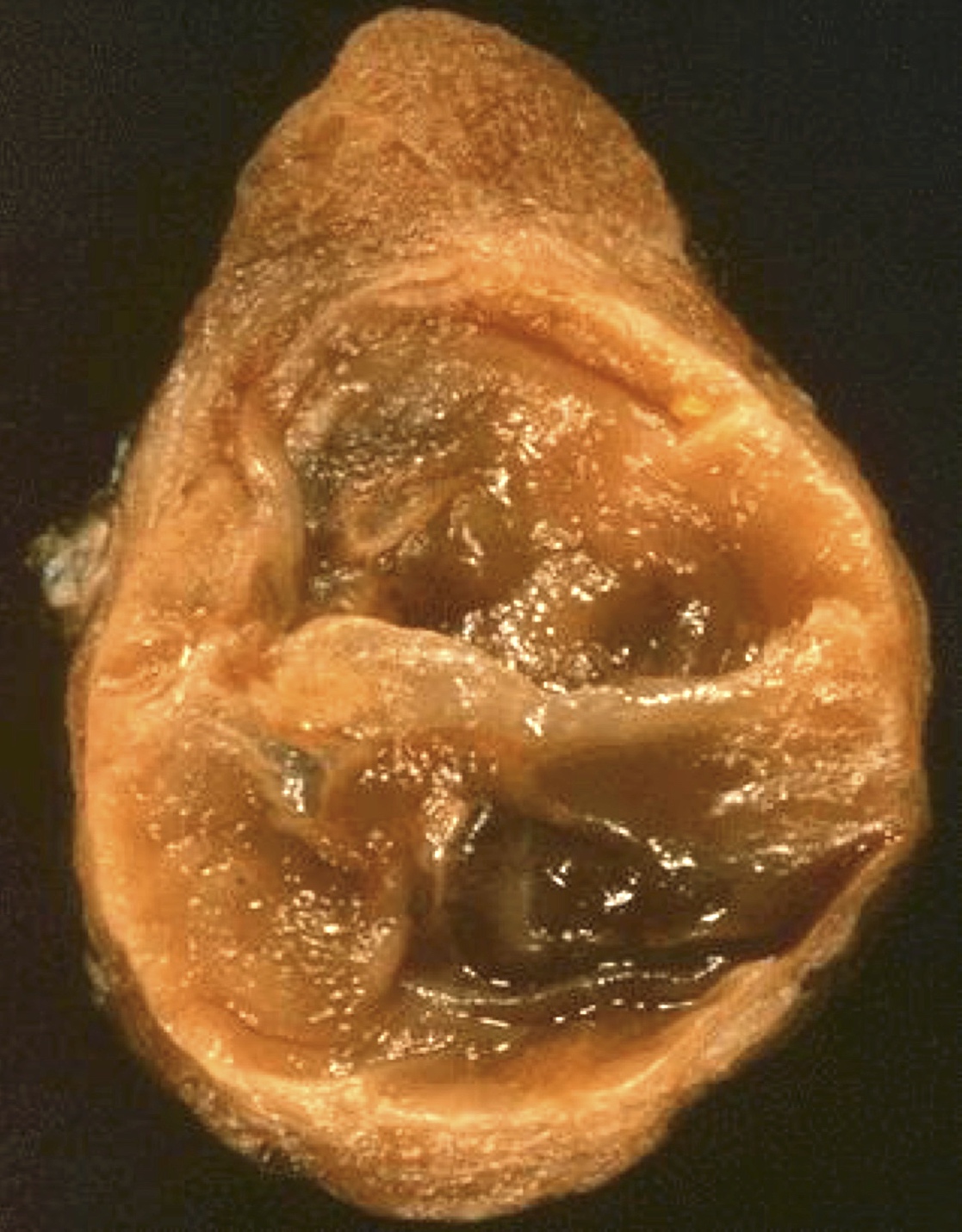
- Solitary, encapsulated nodule; multiple if familial
- Variable size (1 - 10 cm)
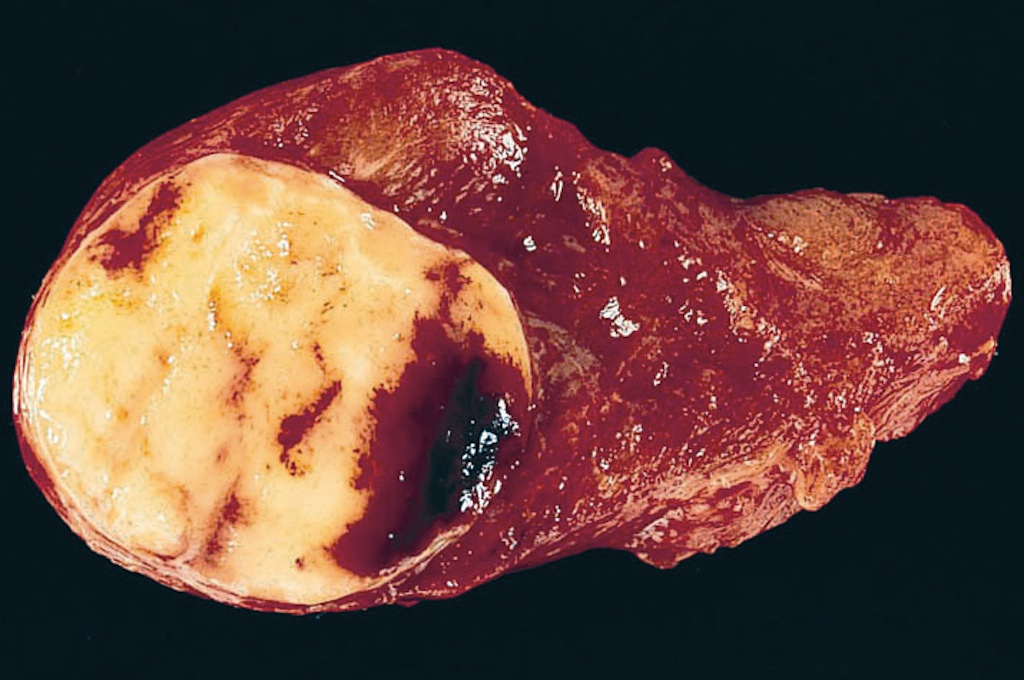
- Solid, gray-white, tan to light brown
- Secondary changes: hemorrhage, cystic change, fibrosis, calcification, infarction; may develop post-fine needle aspiration cytology
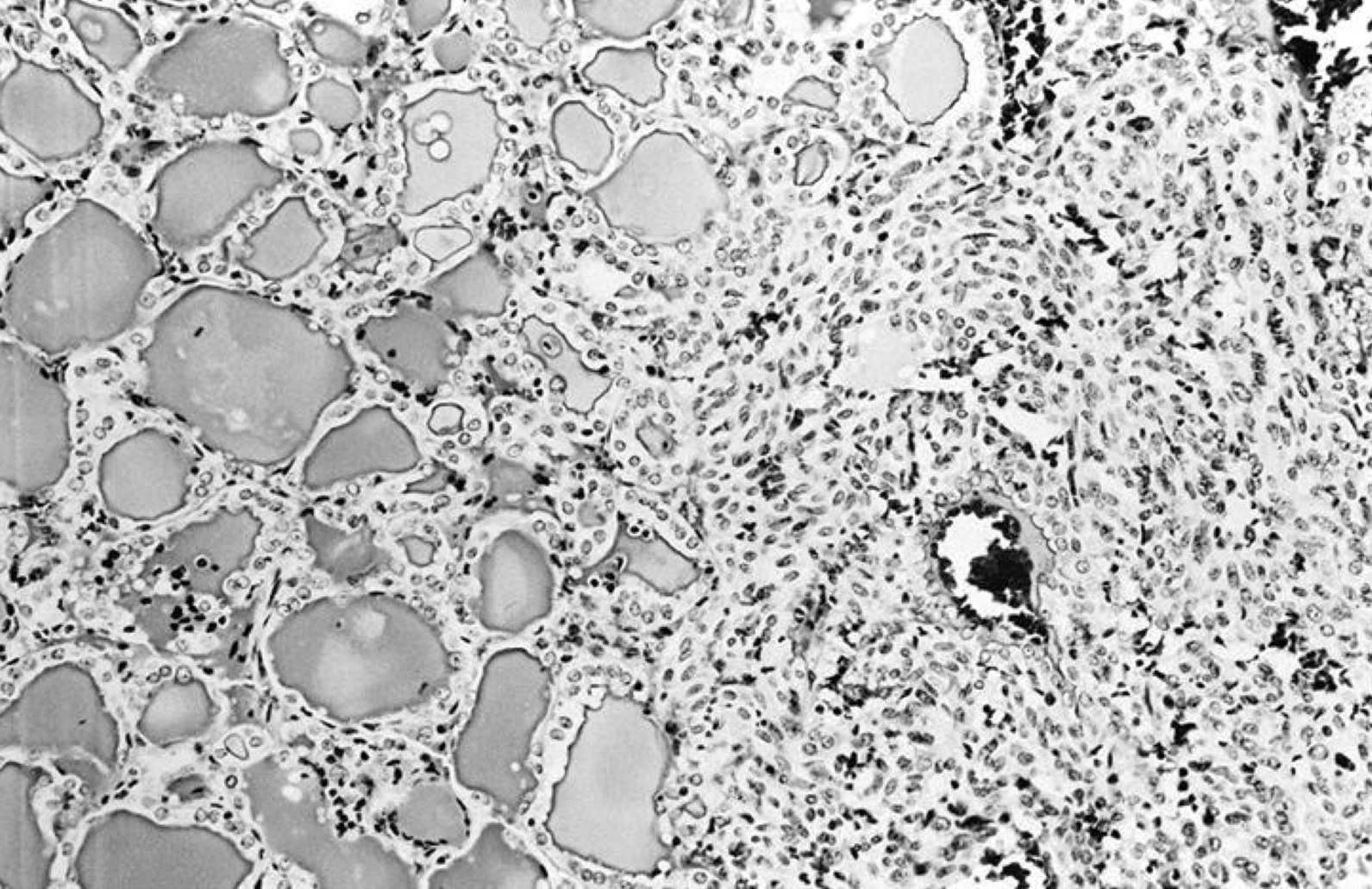
- Rarely black; especially seen with minocycline therapy
Contributed by Andrey Bychkov, M.D., Ph.D., Mark R. Wick, M.D. and AFIP
Encapsulated thyroid nodule
Circumscribed thyroid nodule
Encapsulated, homogeneous tan cut surface

Bisected adenoma has fresh hemorrhage
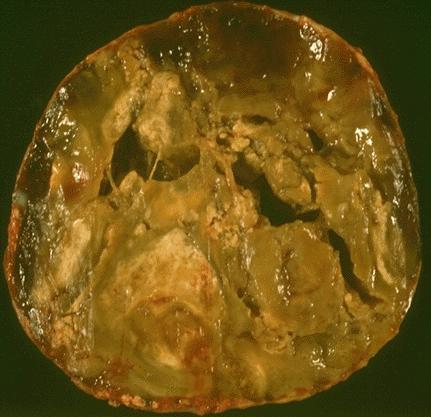
Marked necrosis, hemorrhage and cystic change
Marked cystic degeneration
Images hosted on other servers:


Well circumscribed tumor

Well encapsulated

Central scar

Cystic and partially necrotic tumor
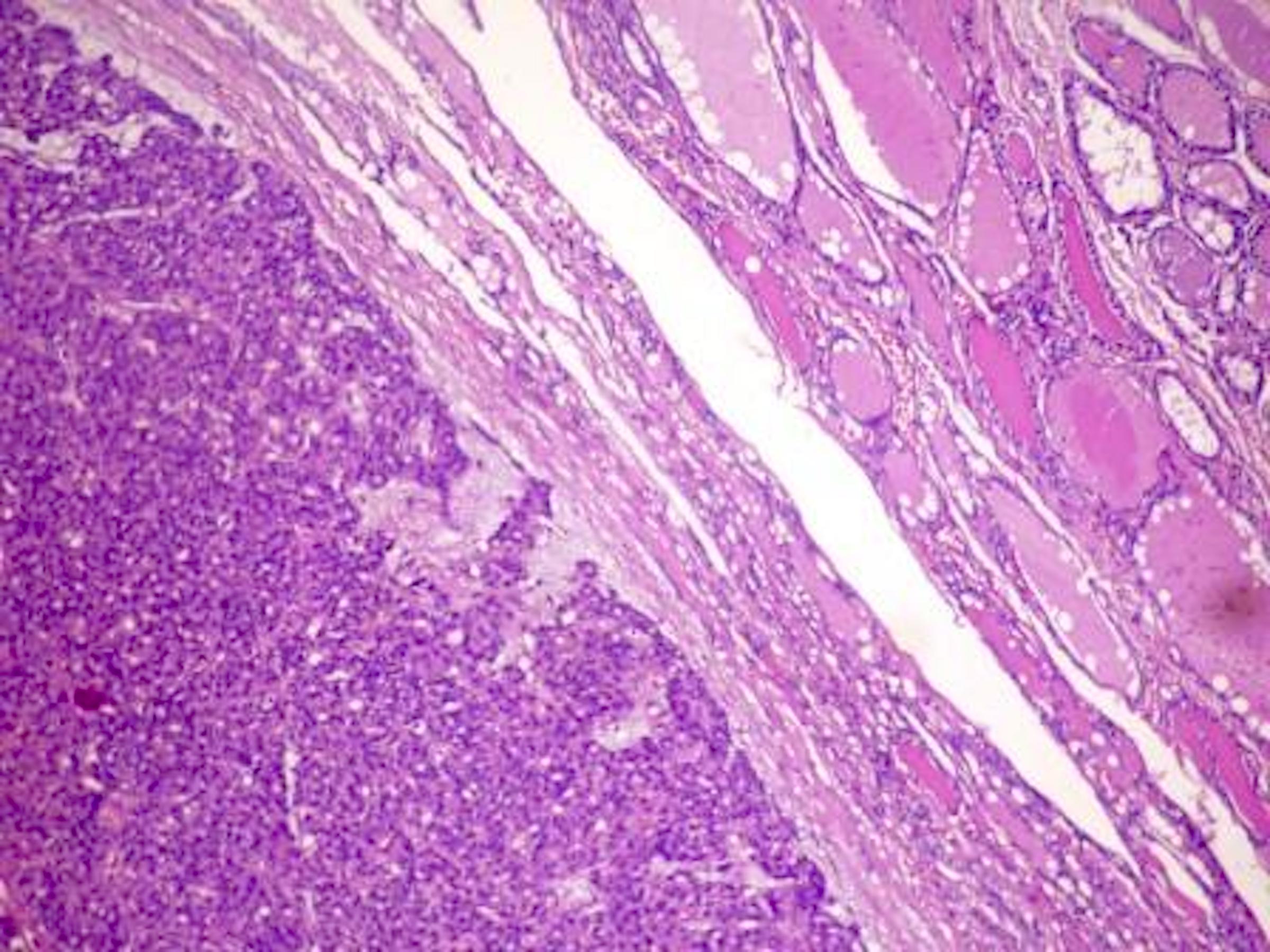
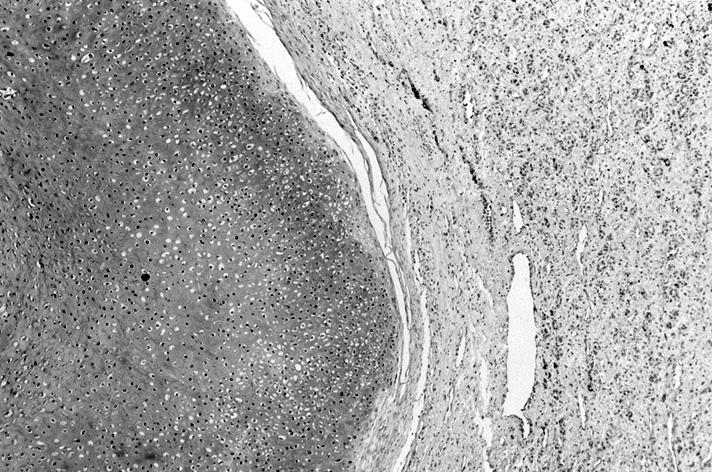
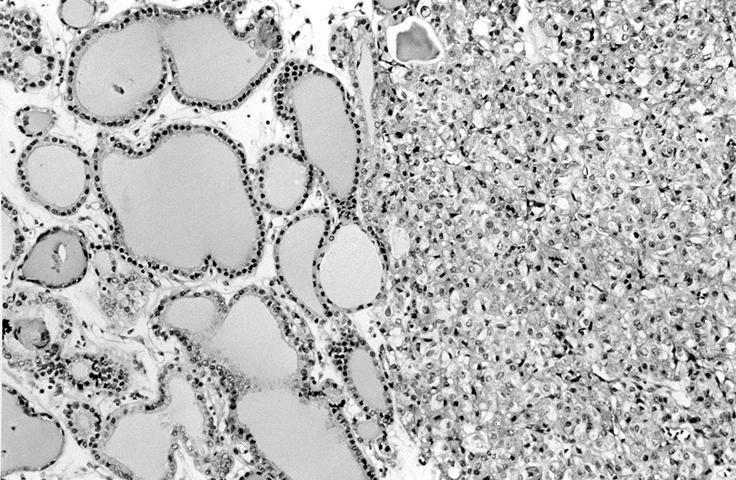
- Architecturally and cytologically different from surrounding gland
- Compression signs in surrounding thyroid tissue
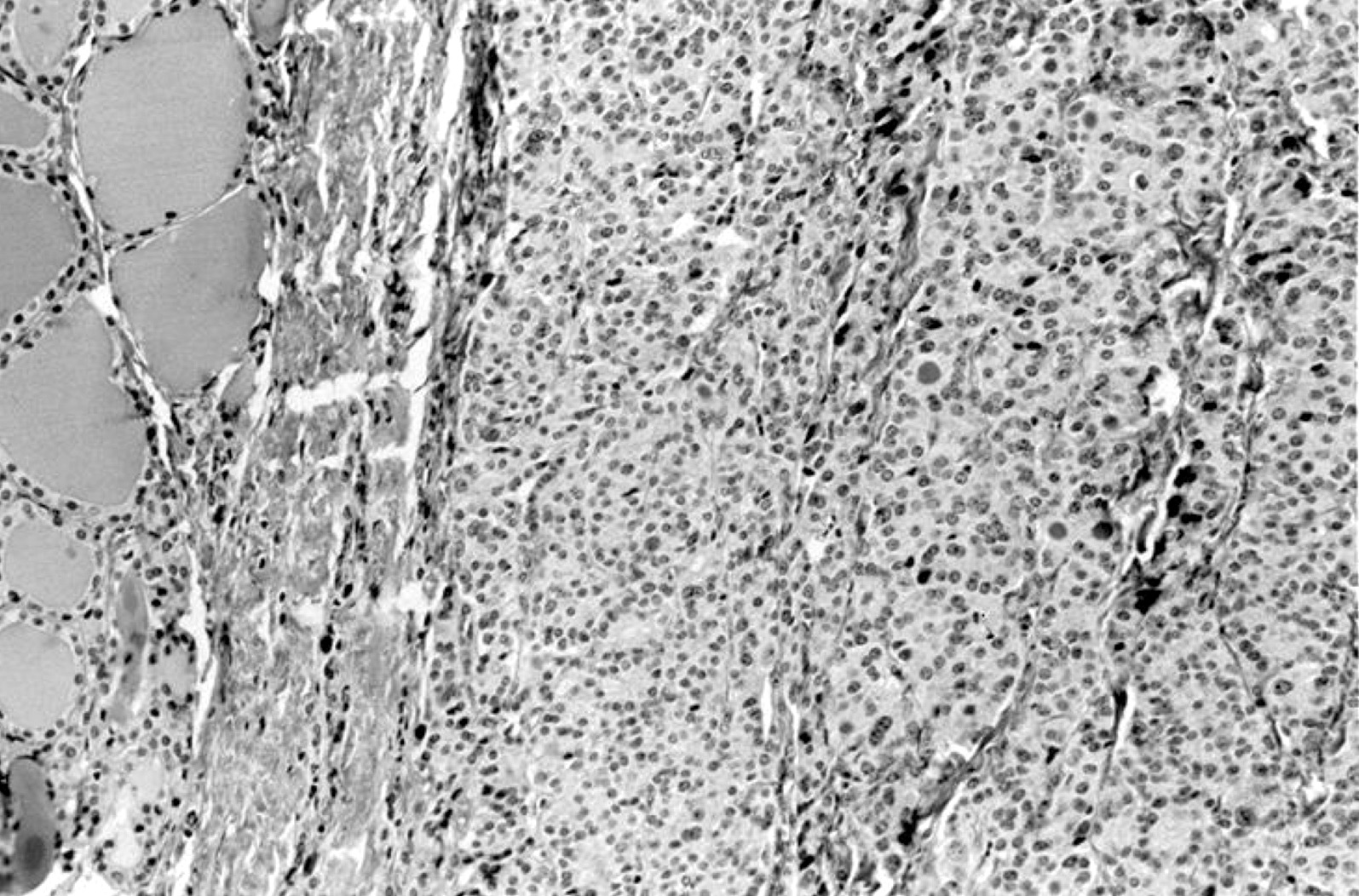
- Encapsulated; thin or moderately thick capsule
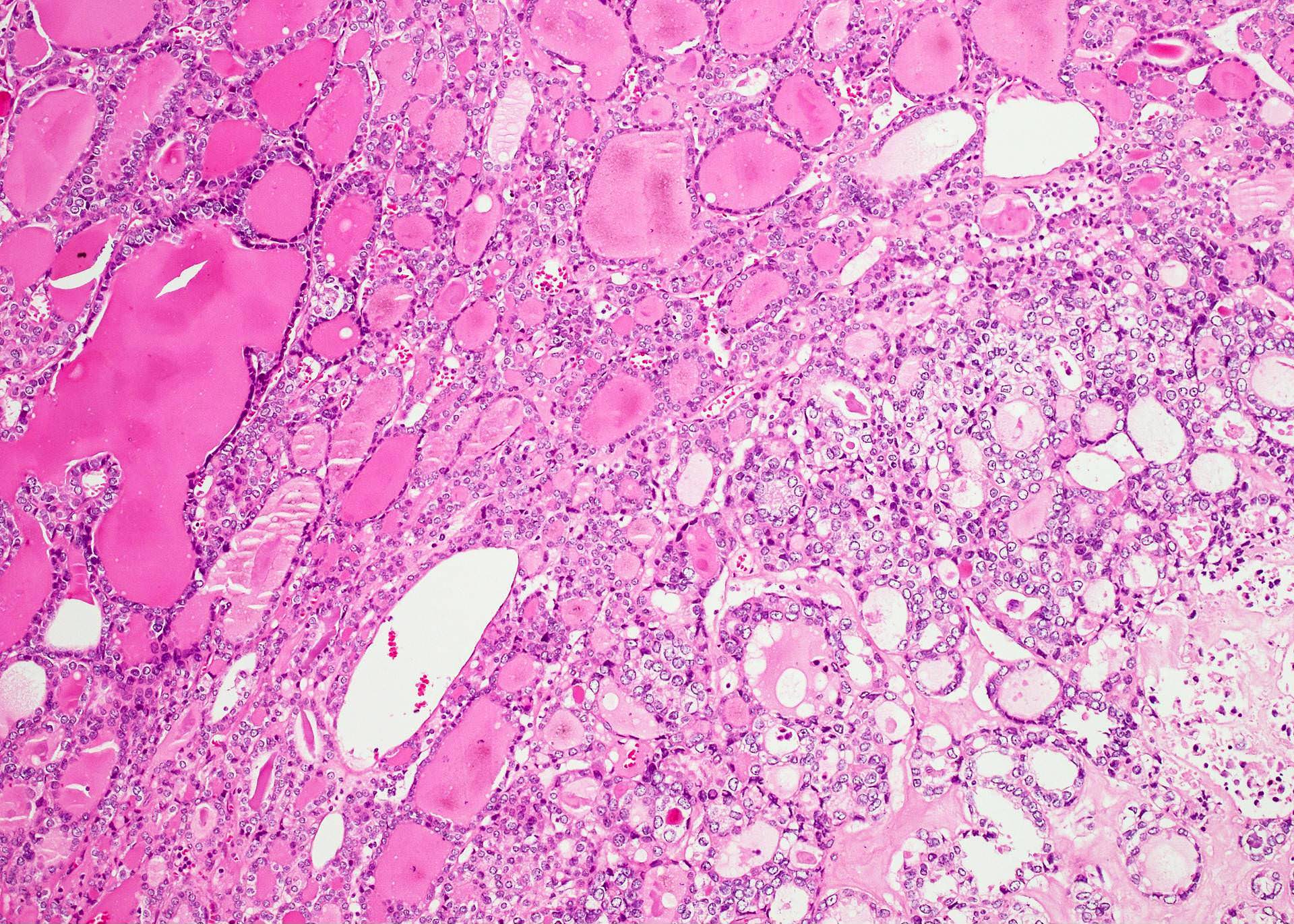
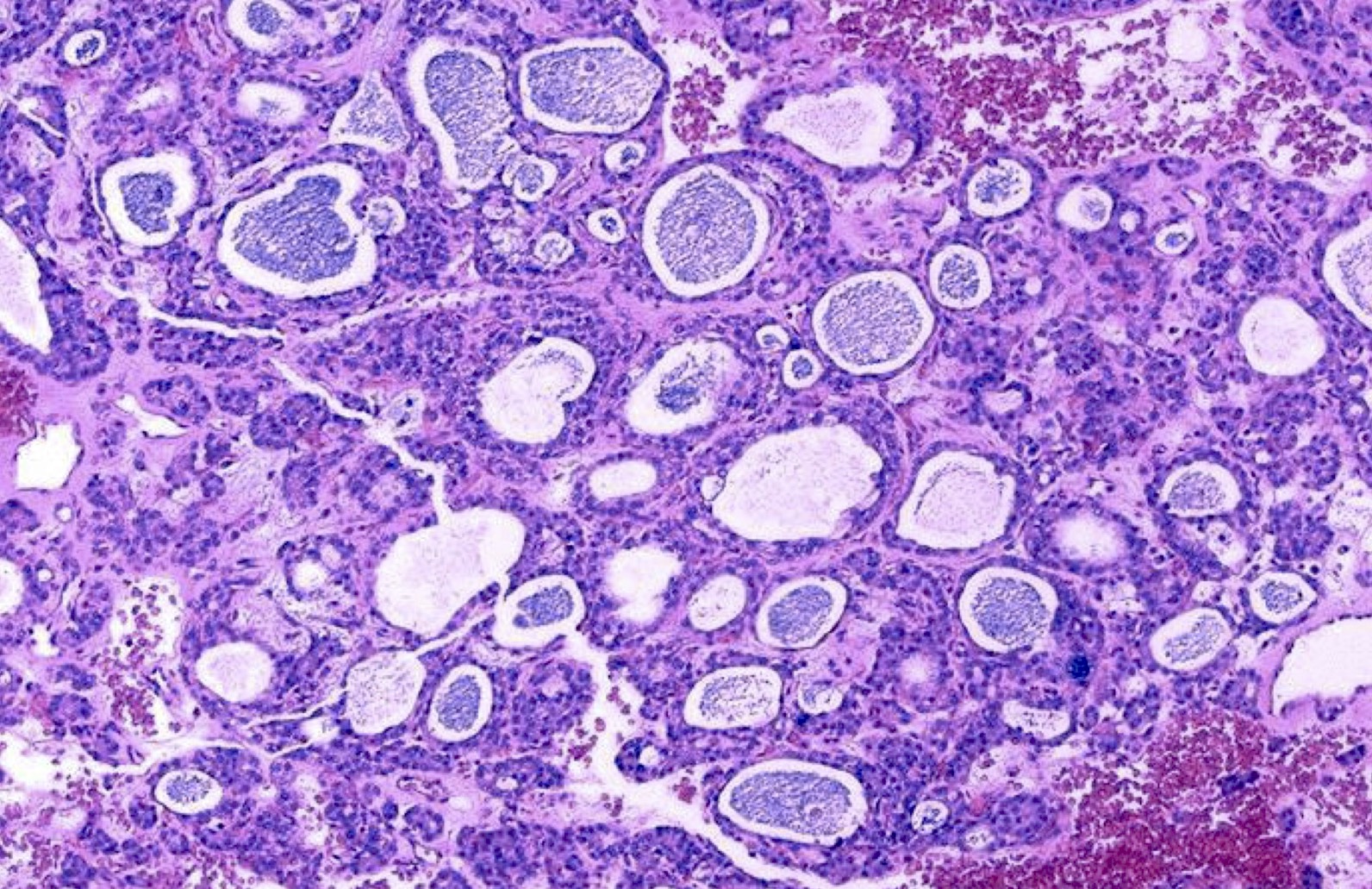
- Architectural patterns (can be seen in any combination)
- Normofollicular (simple): size similar to normal thyroid follicles
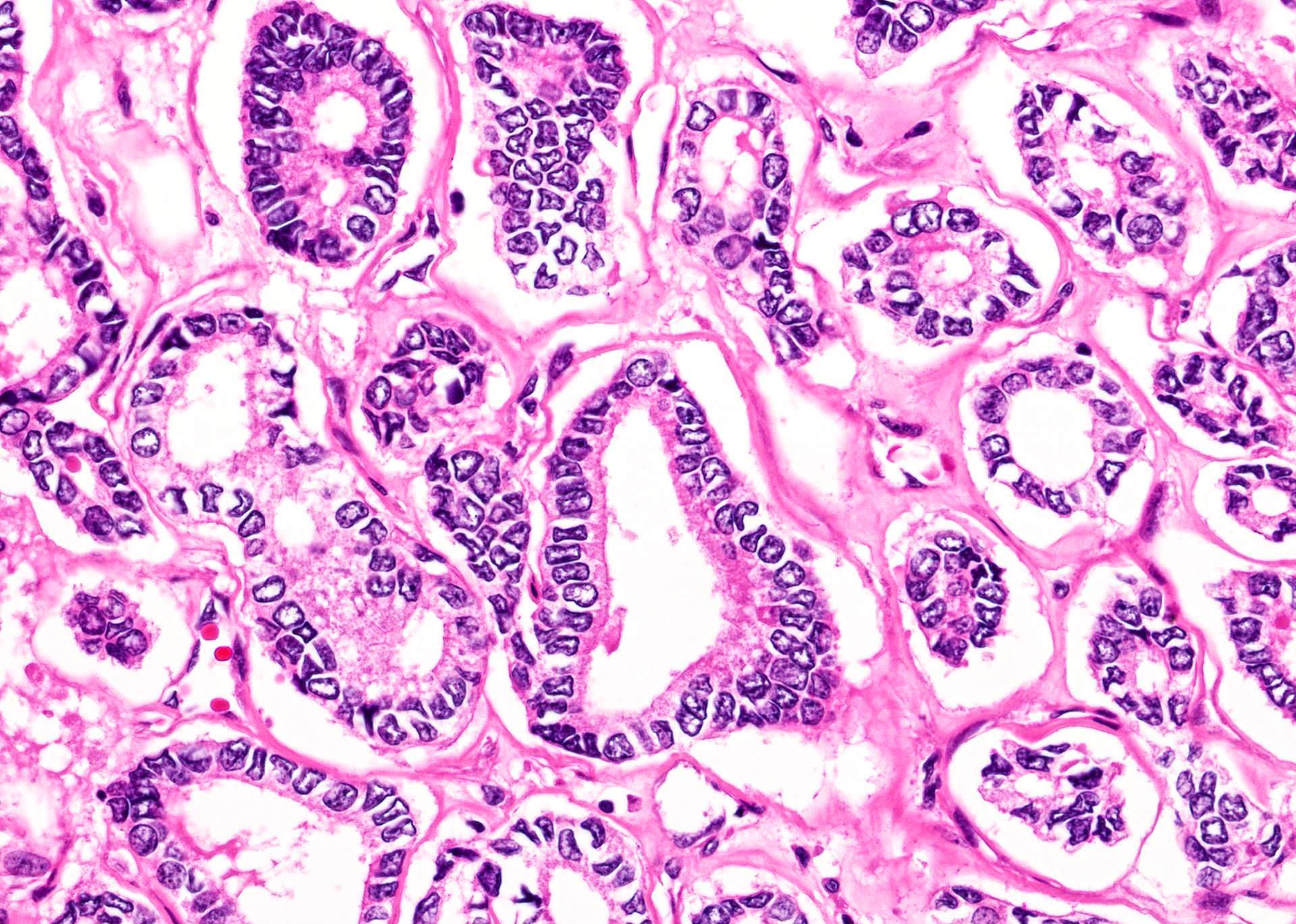
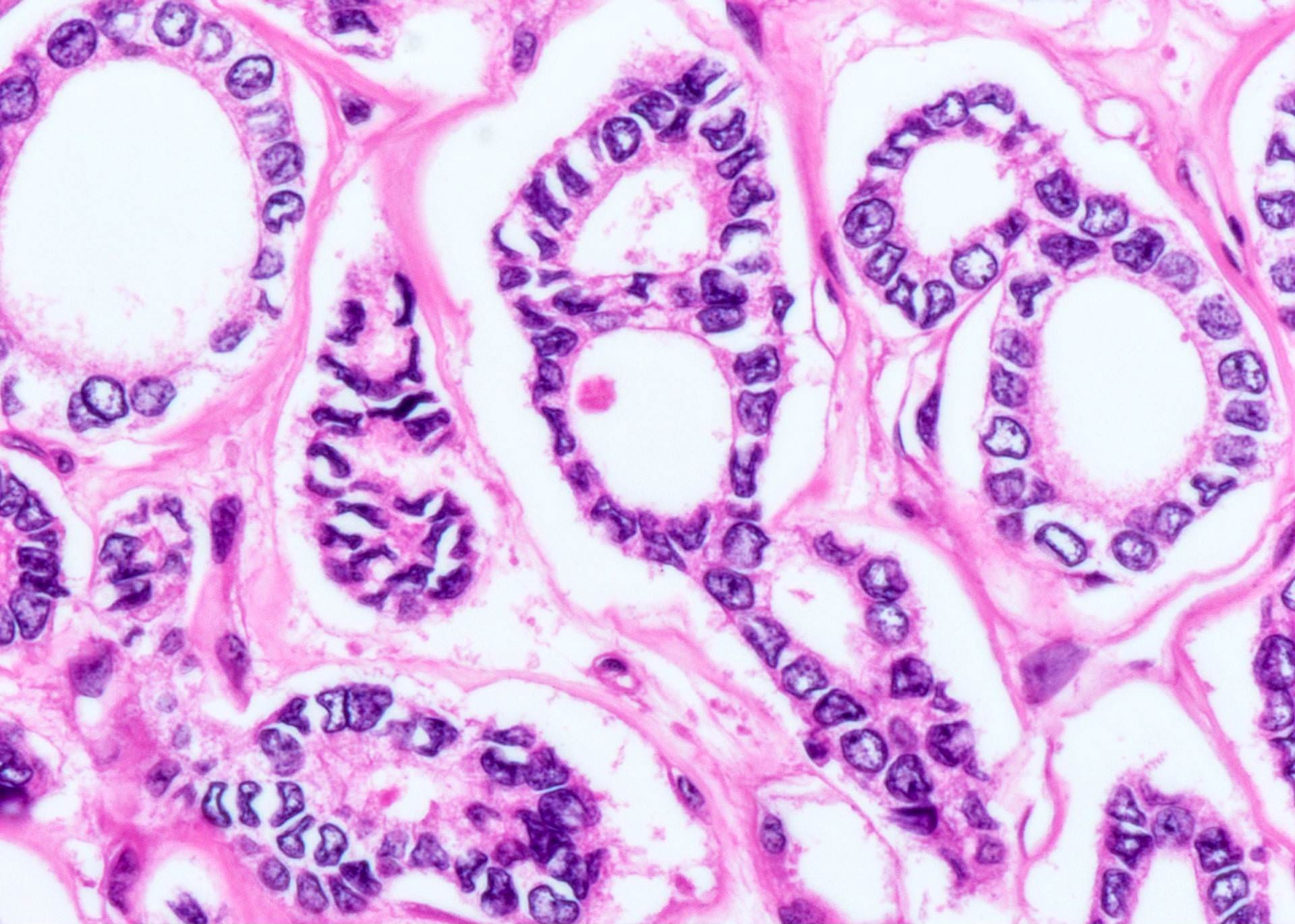
- Microfollicular (fetal): smaller follicles, small amount of intraluminal colloid
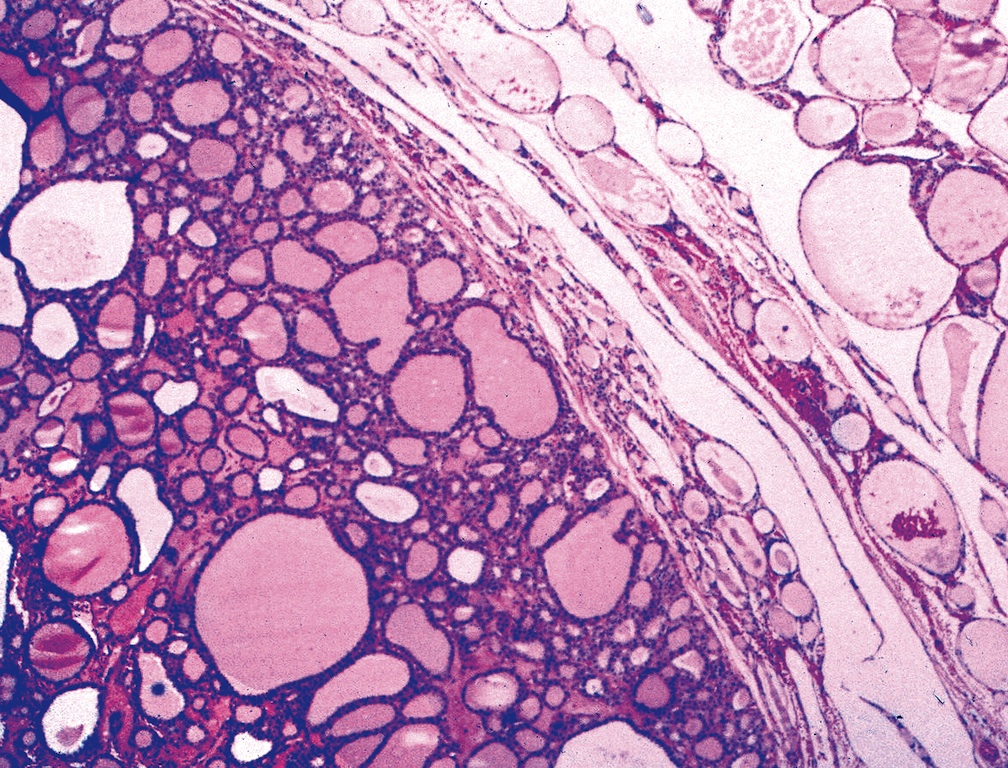
- Macrofollicular (colloid): large follicles, flattened epithelium, abundant colloid
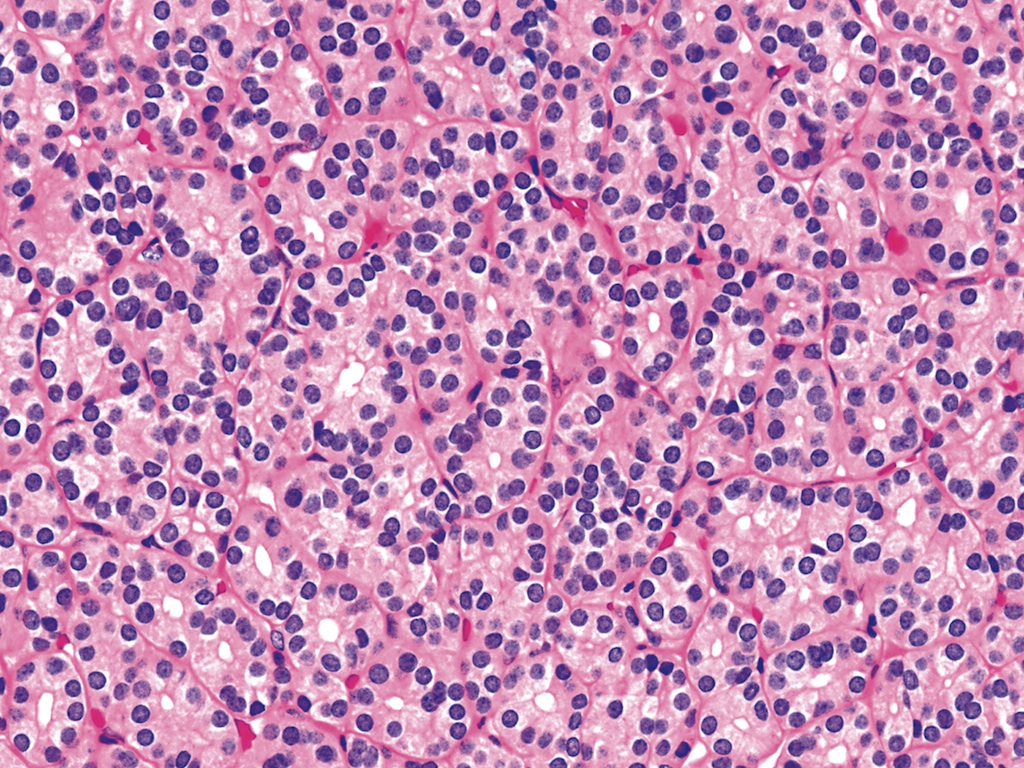
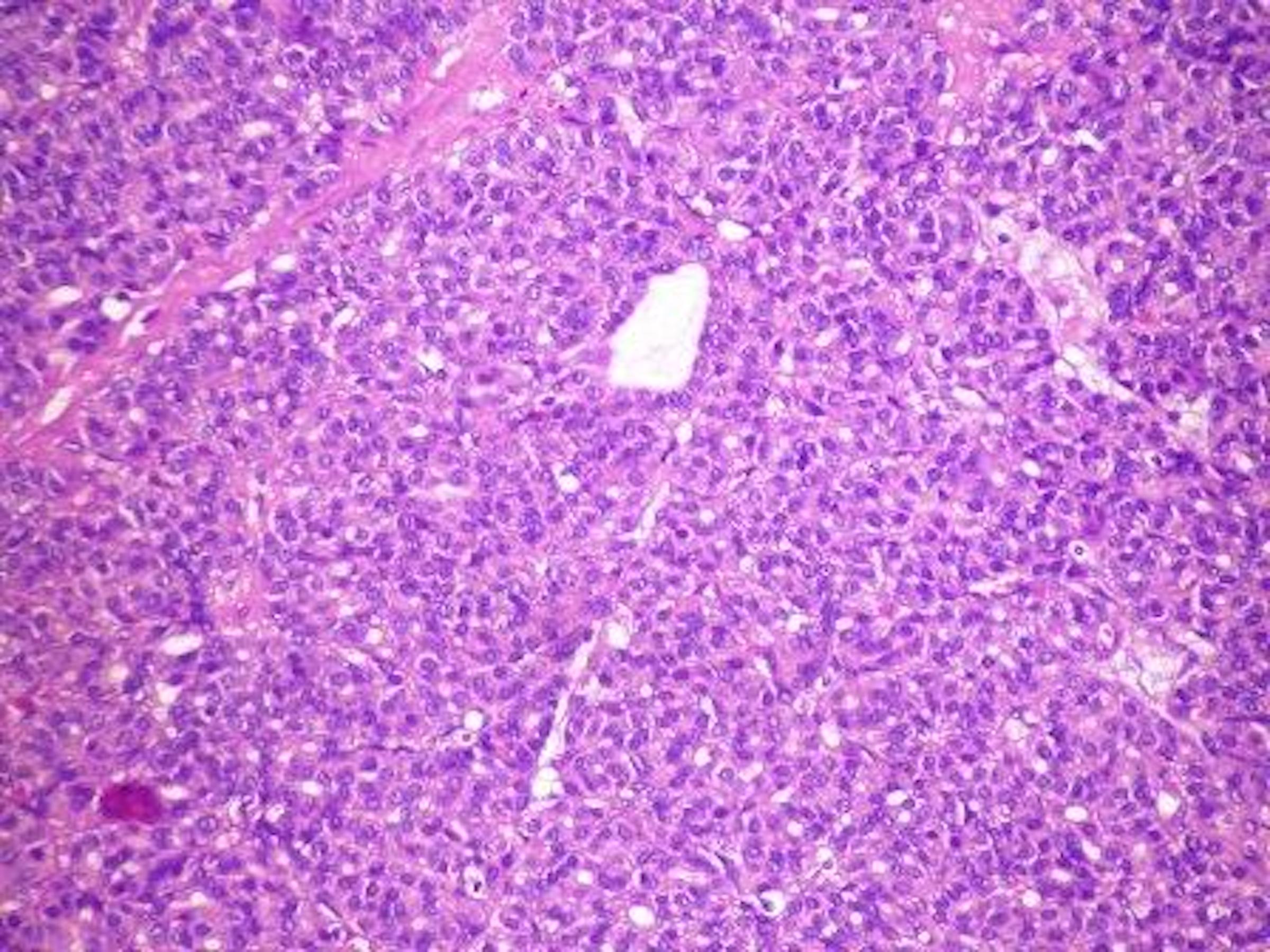
- Solid / trabecular (embryonal): minimal or no colloid
- Focal papillary pattern, occasionally; especially in hyperfunctioning adenoma and follicular adenoma with papillary hyperplasia
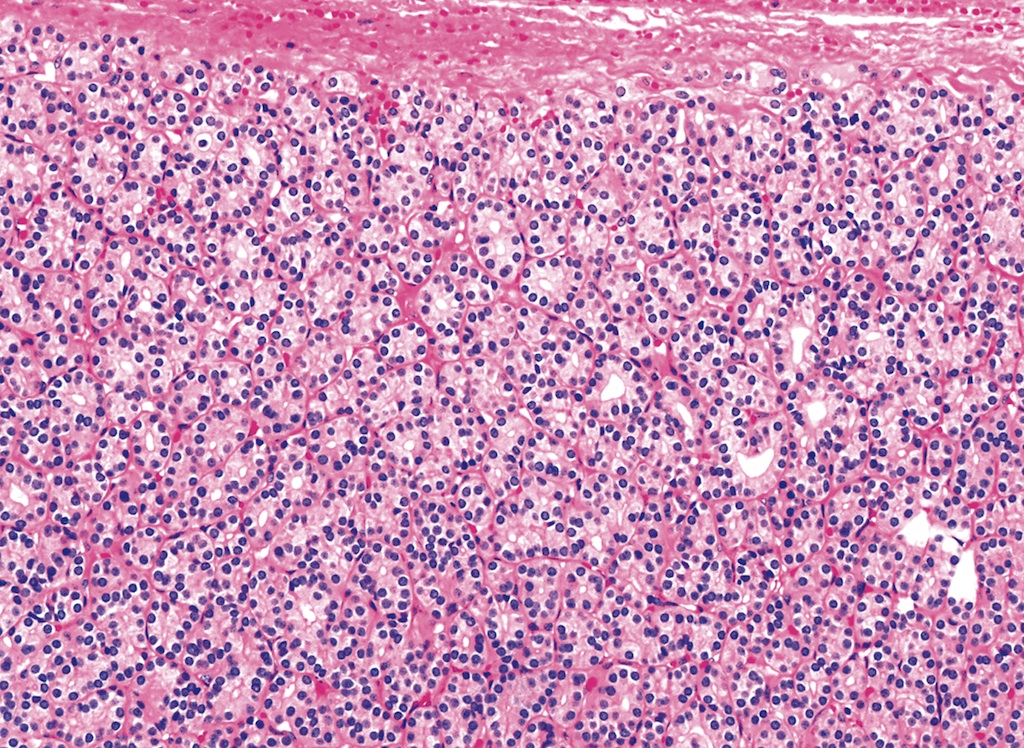
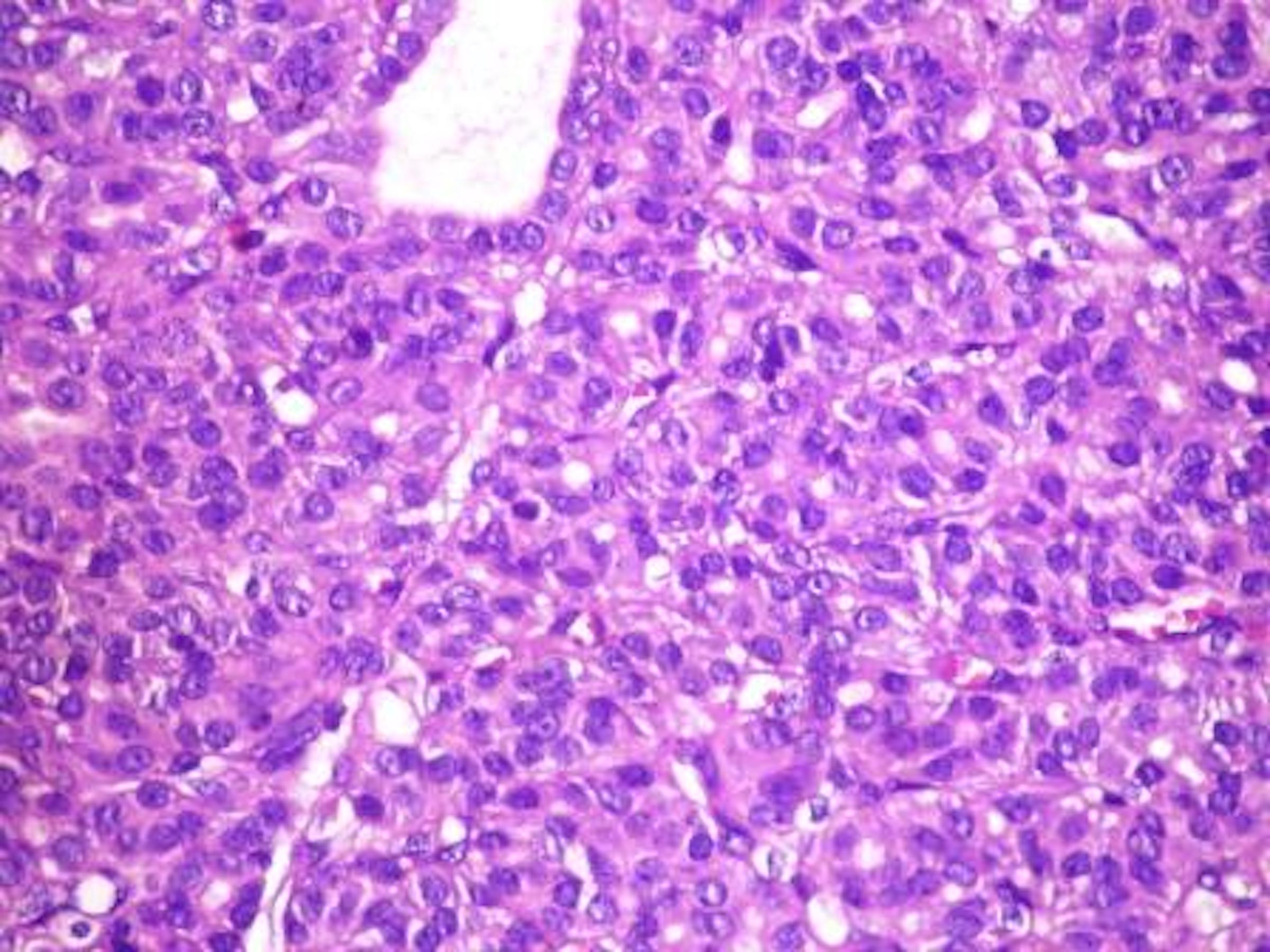
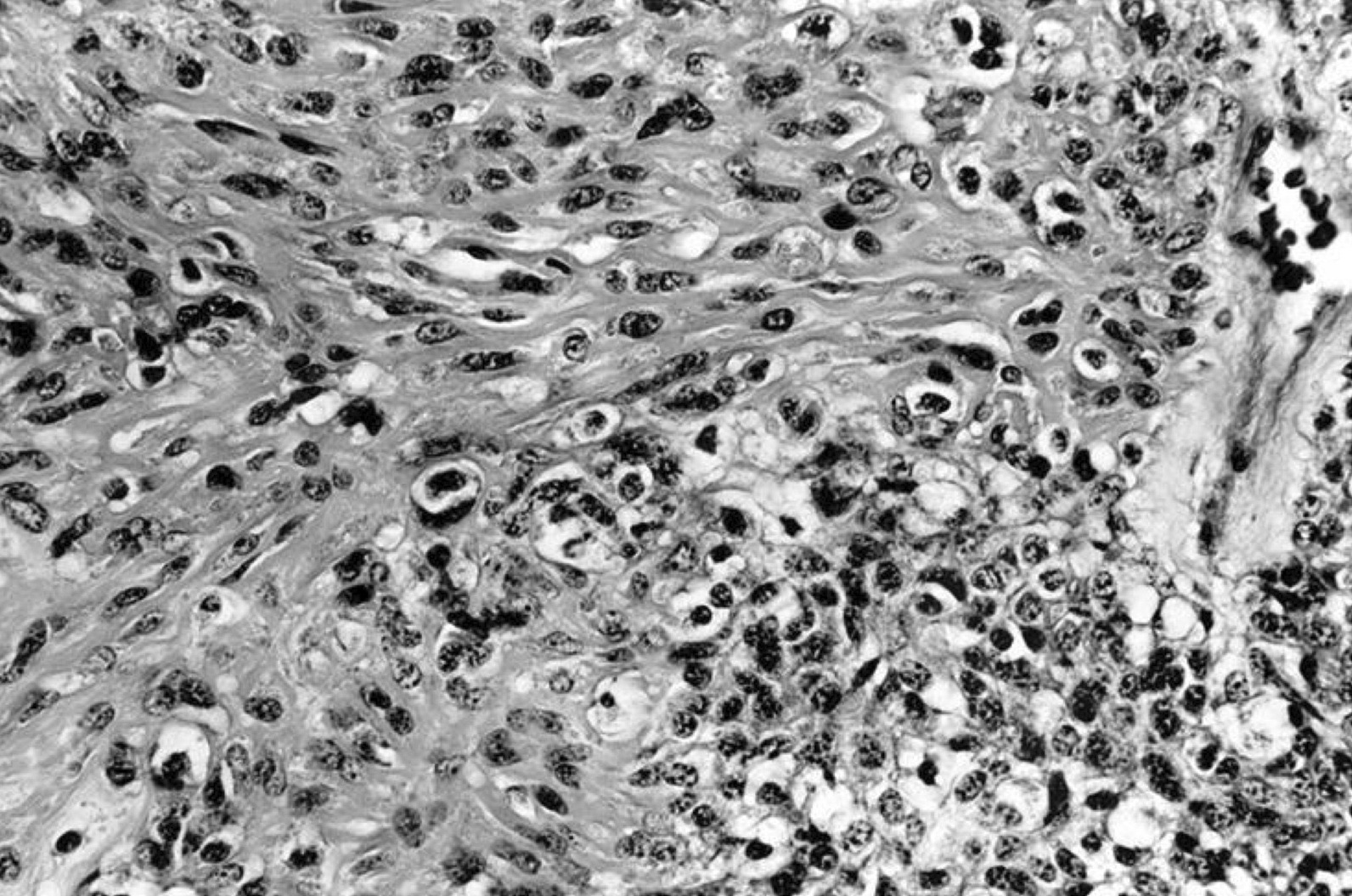
- Cuboidal to low columnar cells
- Small round nuclei, smooth nuclear boundary, uniformly hyperchromatic or euchromatic, dense chromatin, absent nuclear features of papillary thyroid carcinoma, nuclear score 0 or 1 (JAMA Oncol 2016;2:1023)
- Inconspicuous nucleoli
- Rarely, lipid filled vacuoles in cytoplasm
- Mitoses are uncommon
- Scant stroma
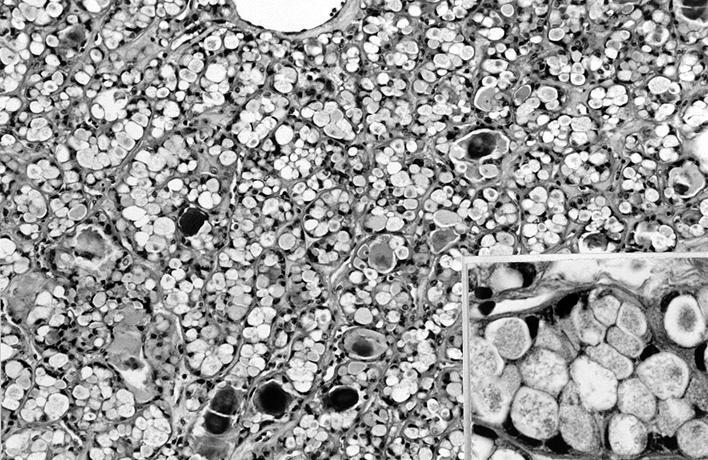
- Secondary changes: fibrosis, hyalinization, hemorrhage, hemosiderin deposition, edema, cystic degeneration, calcification, osseous or cartilaginous metaplasia
- Variants
- Hyperfunctioning adenoma (Plummer adenoma): tall columnar epithelium, papillary infoldings, vacuolated cytoplasm, watery colloid showing scalloping
- Follicular adenoma with papillary hyperplasia: cystically dilated follicles, intraluminal papillae
- Lipoadenoma: adipocytic metaplasia of the follicular adenoma
- Follicular adenoma with bizarre nuclei: may be seen after radiation exposure and in hyperfunctioning adenoma
- Signet ring cell follicular adenoma: signet ring cell change
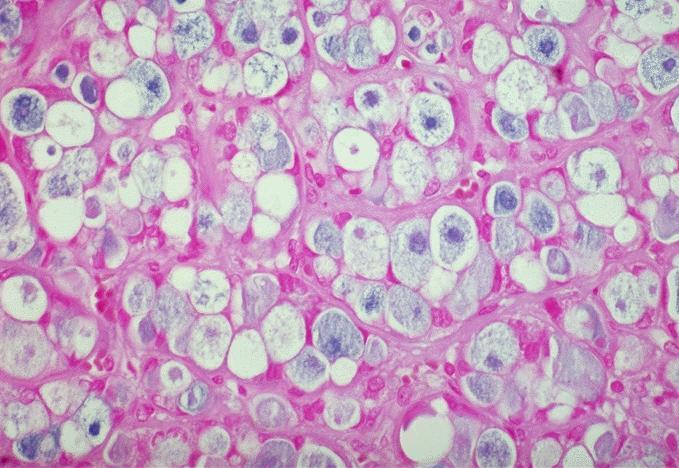
- Clear cell follicular adenoma: follicular adenoma with clear cell change
- Spindle cell follicular adenoma: spindle cell metaplasia
- Black follicular adenoma (black pigment in tumor cell cytoplasm; in patients on minocycline therapy)
- No capsular or vascular invasion after thorough sampling (at least 10 blocks)
Contributed by Shipra Agarwal, M.D., Andrey Bychkov, M.D., Ph.D., Mark R. Wick, M.D., Asmaa Gaber Abdou, M.D. and AFIP
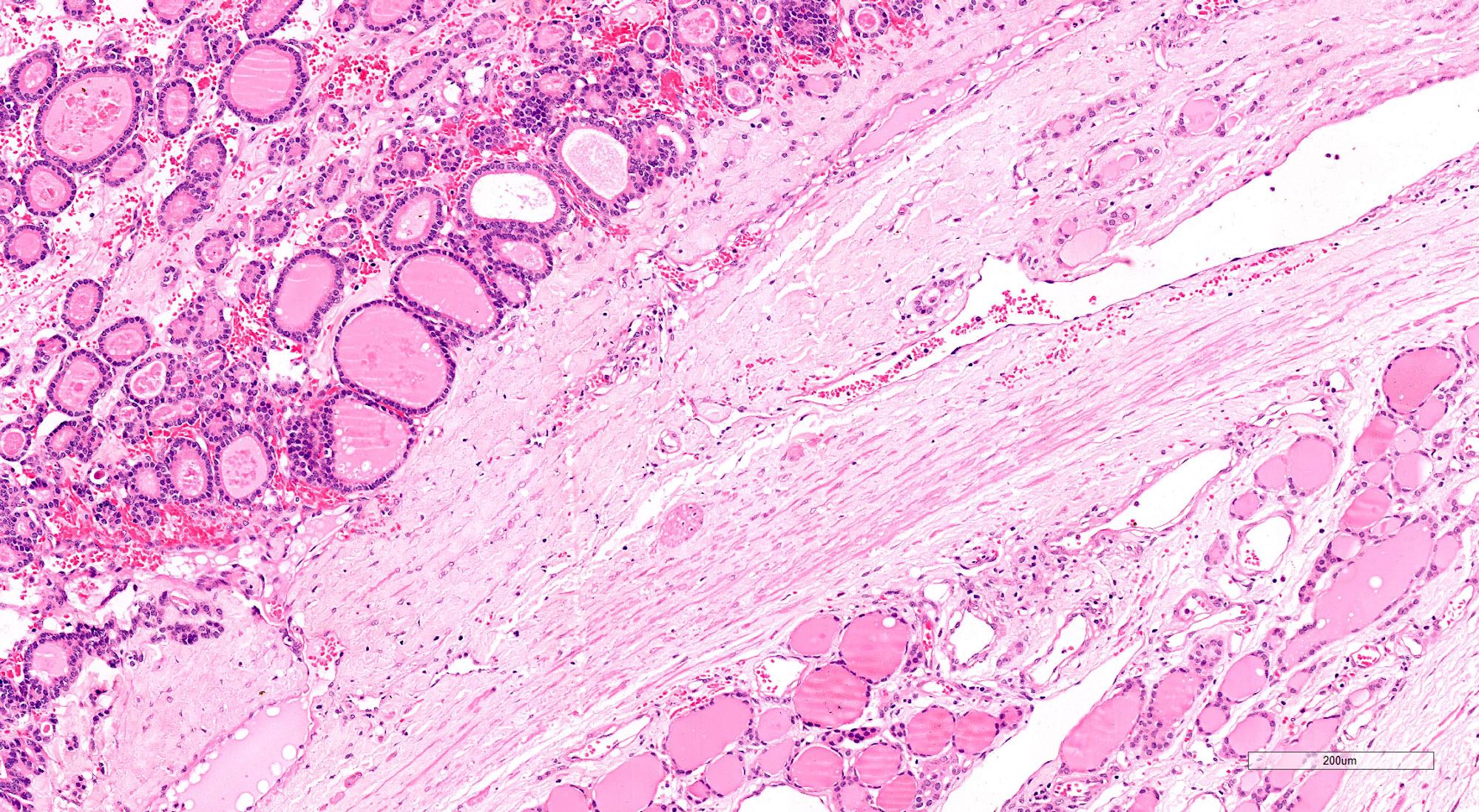
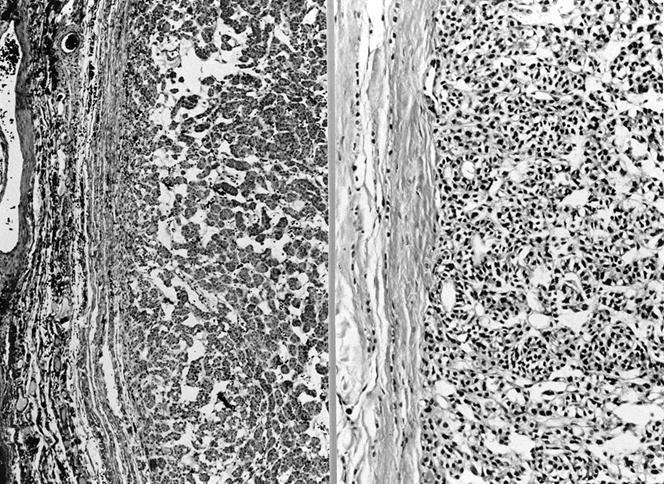
Capsule & compressed thyroid
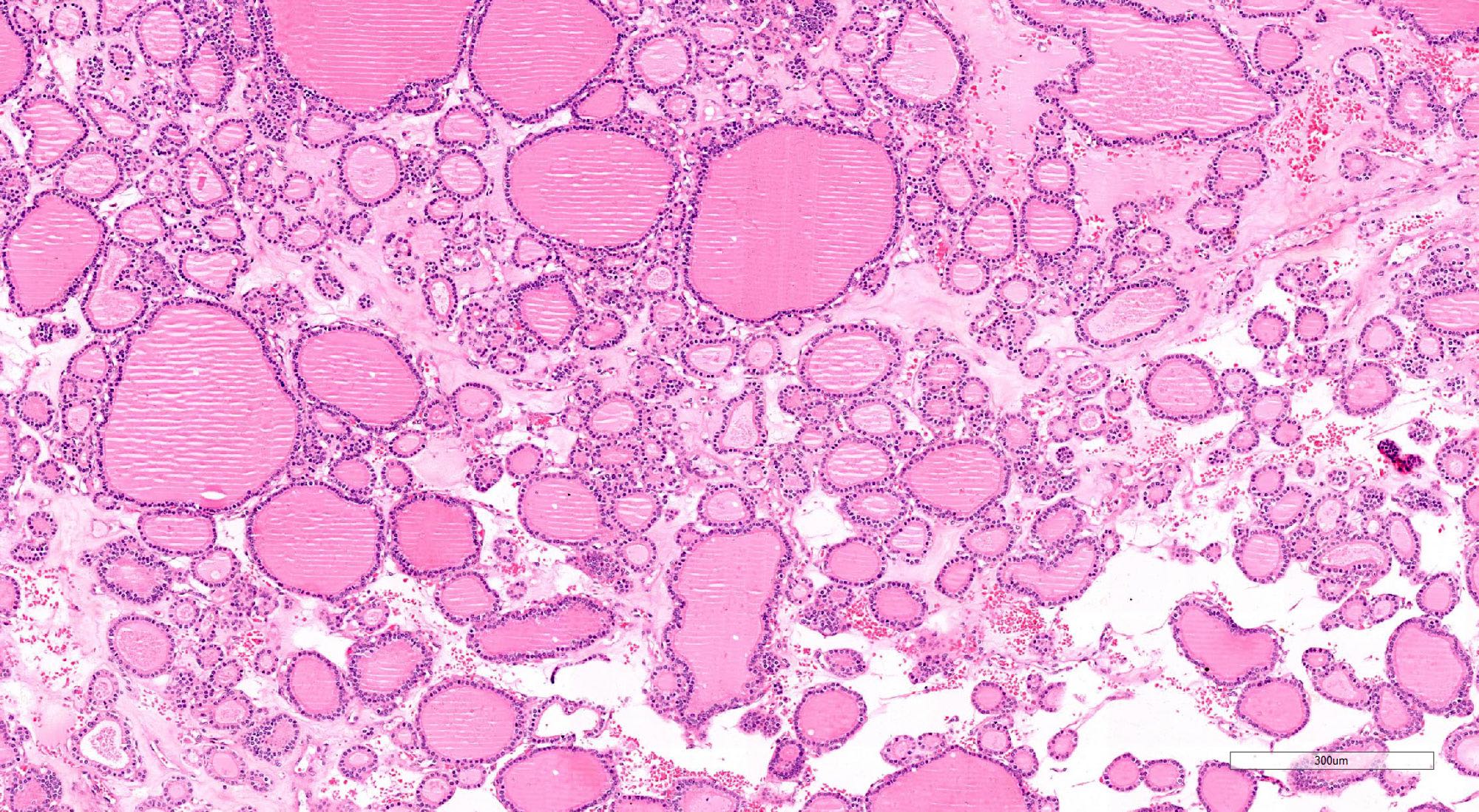
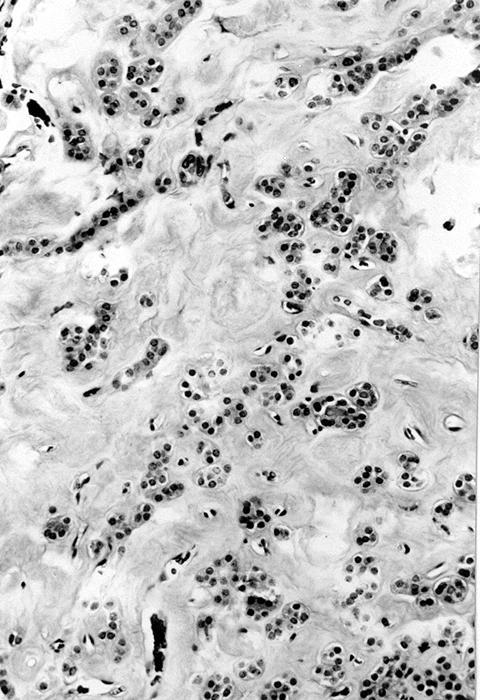
Mixed micro and normofollicular pattern
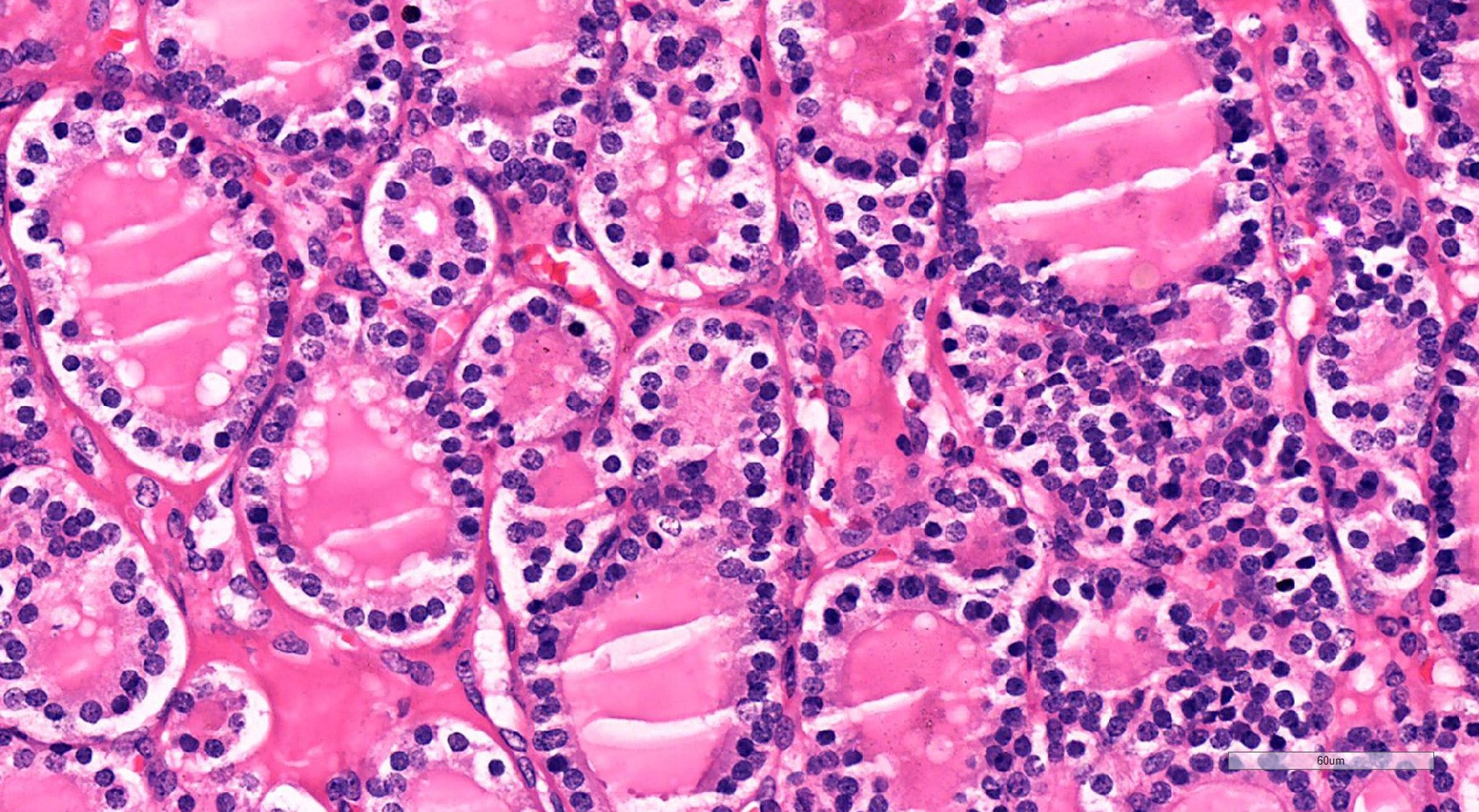
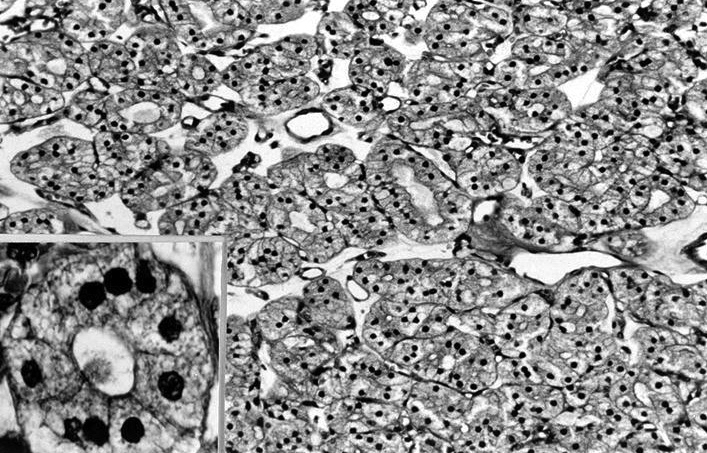
Hyperchromatic, small round nuclei
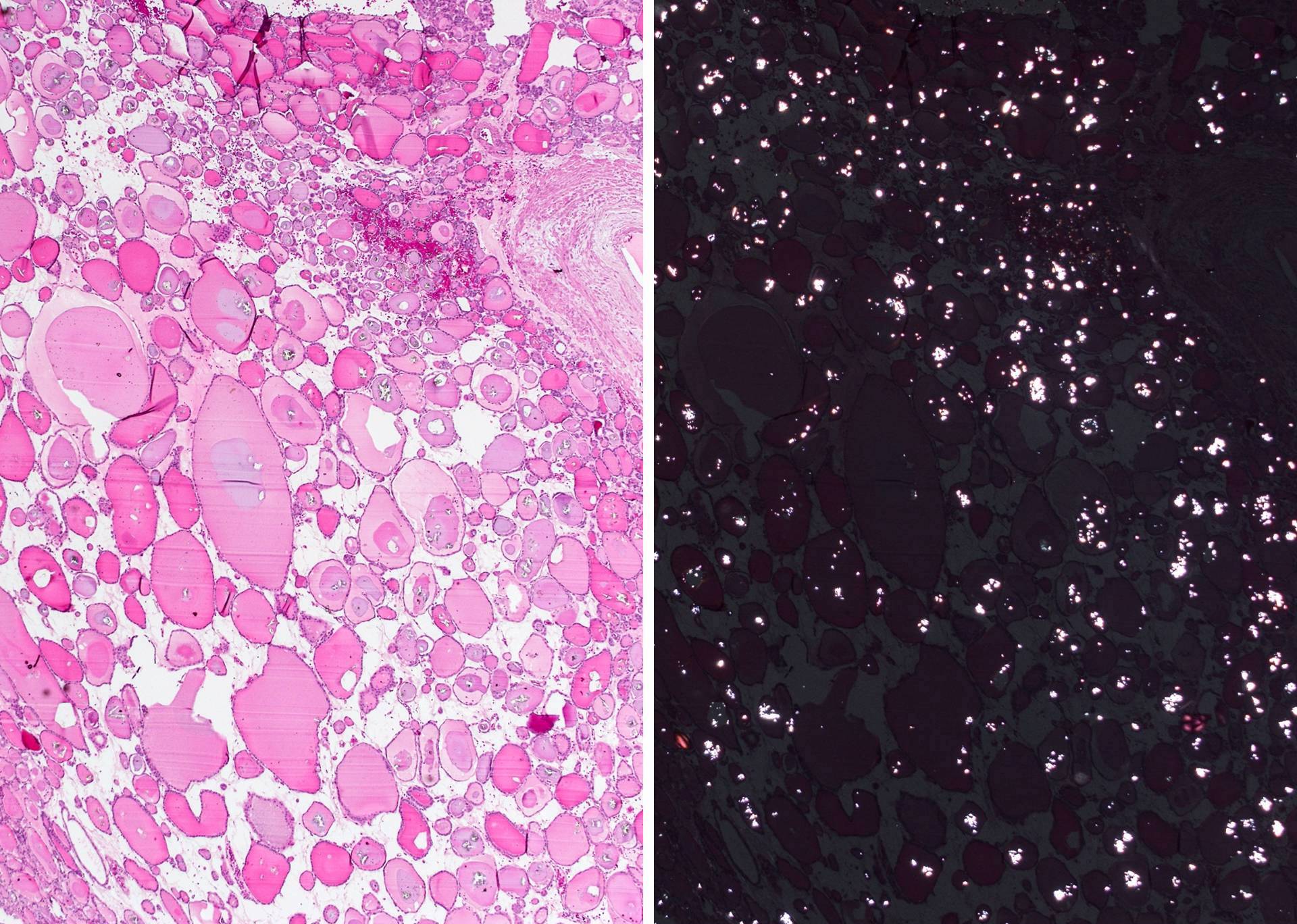
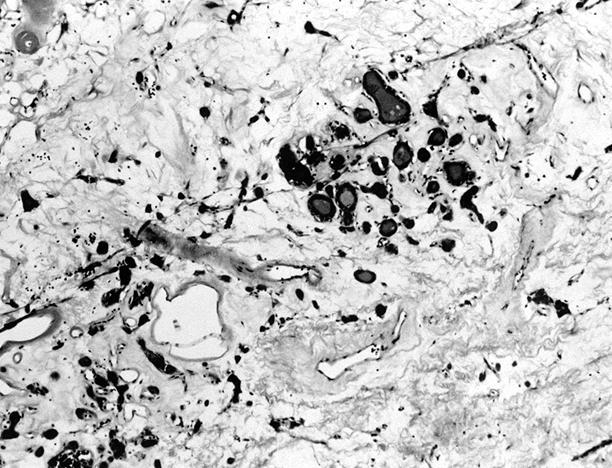
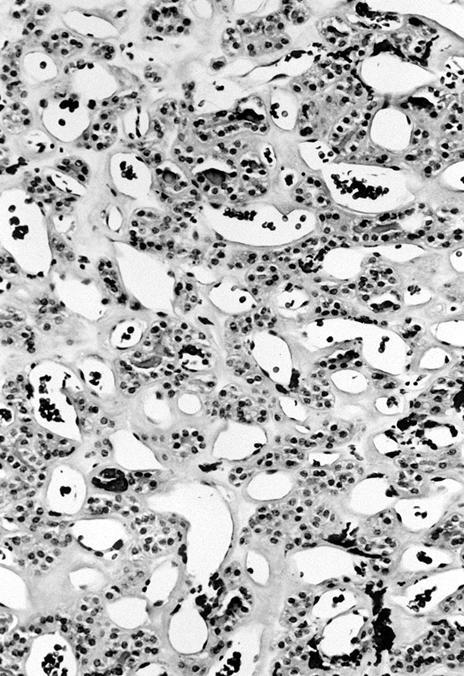
Abundant crystals of calcium oxalate
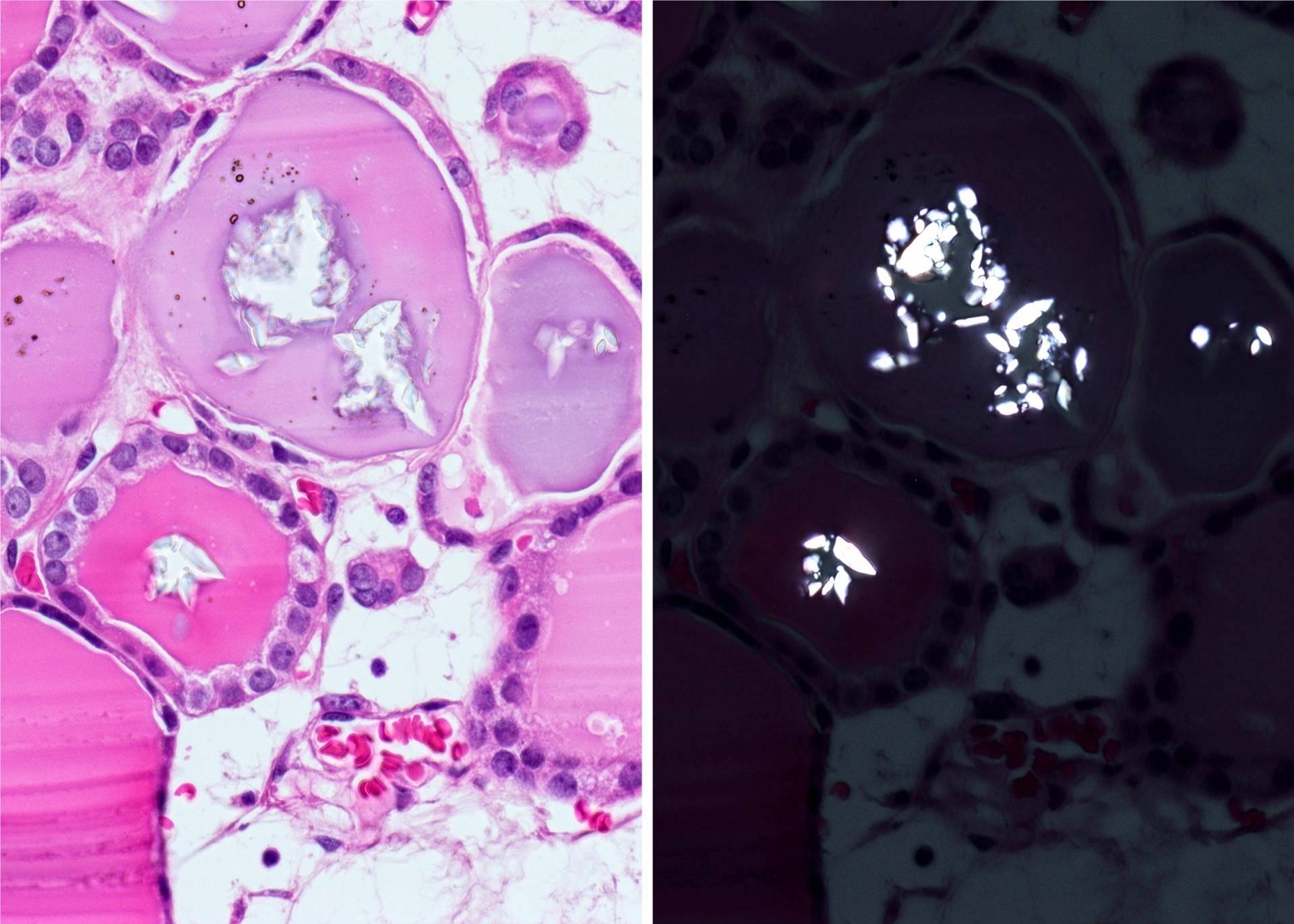
Calcium oxalate crystals
Processing artifact with distorted nuclei
Distorted nuclei due to technical / processing artifact
Tissue degeneration
Circumscribed thyroid nodule
Cellular follicular adenoma
Cellular follicular adenoma

Trabecular type
Trabecular type
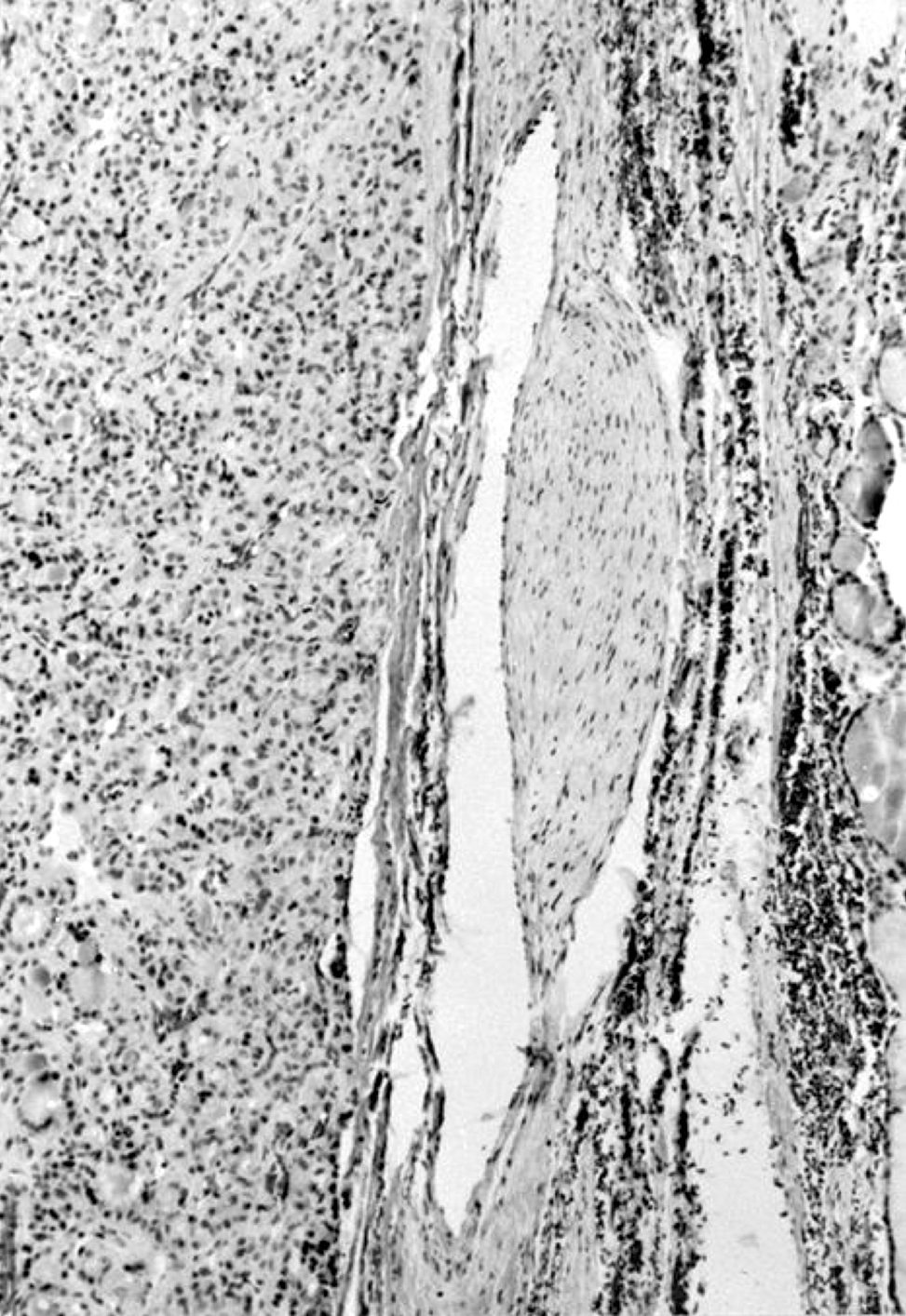
Thin and uniform fibrous capsule
Marked fibrosis and stromal hyalinization
Marked hyaline thickening of vessel walls
Marked fibrosis, hyalinization and calcium deposition
Marked vascularization
Capsular vessel with smooth muscle cells

Bizarre nuclei
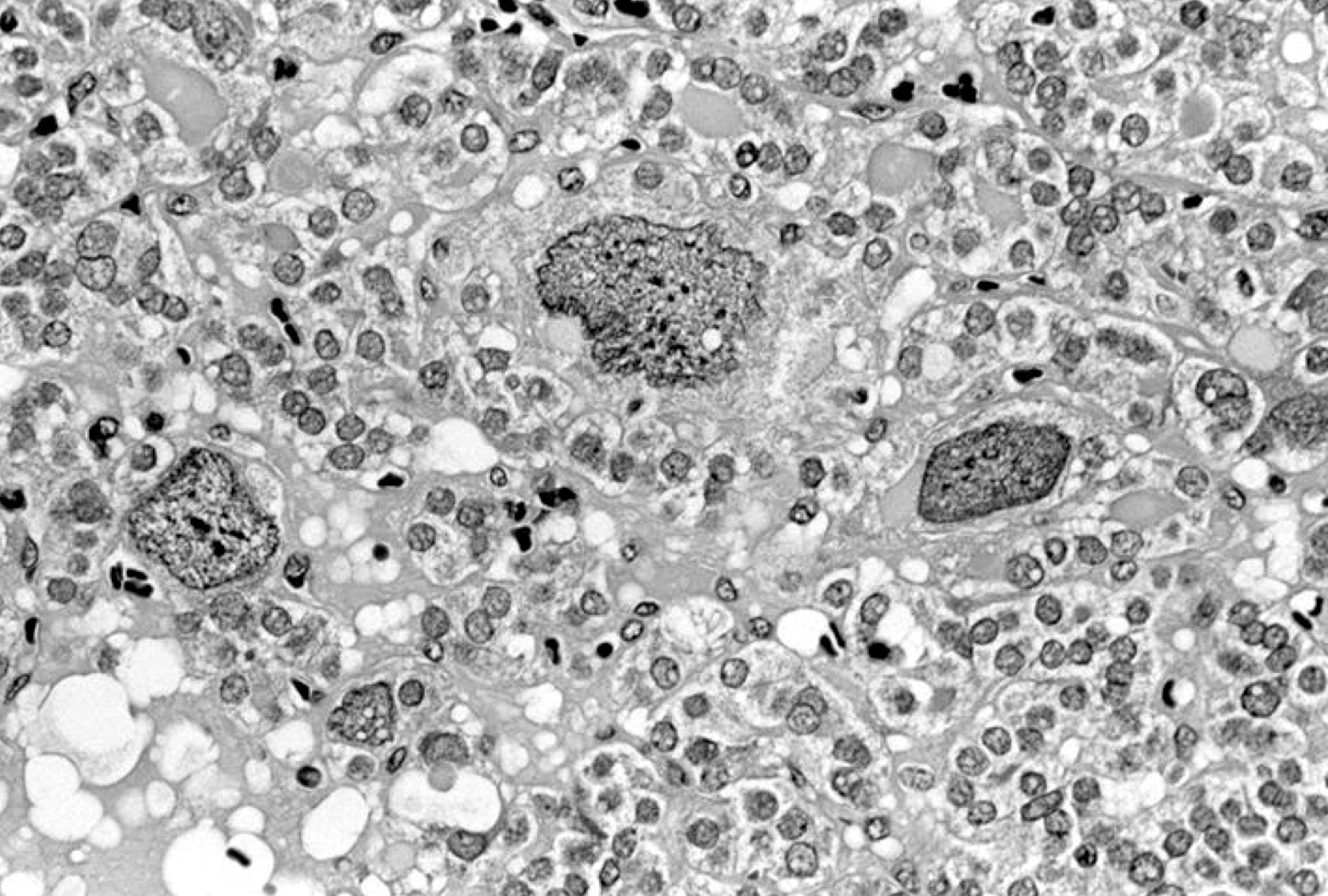
Large, extremely irregular nuclei
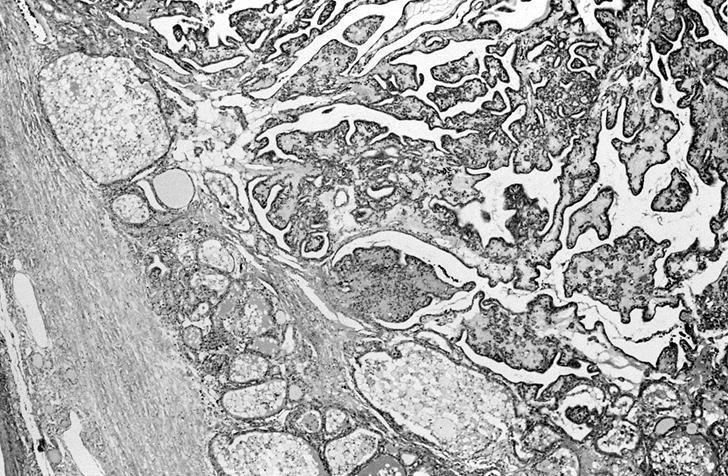
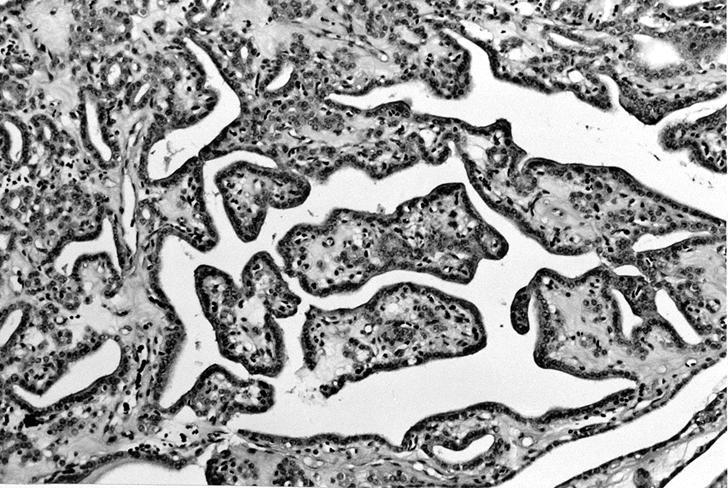
With papillary hyperplasia
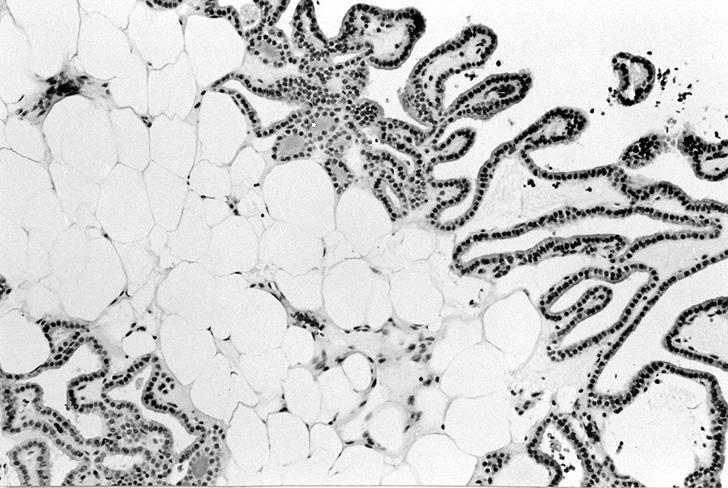
With papillary hyperplasia and adipose metaplasia
Cartilaginous metaplasia (adenochondroma)
Prominent, clear cell change

Squamous metaplasia
Mucin production
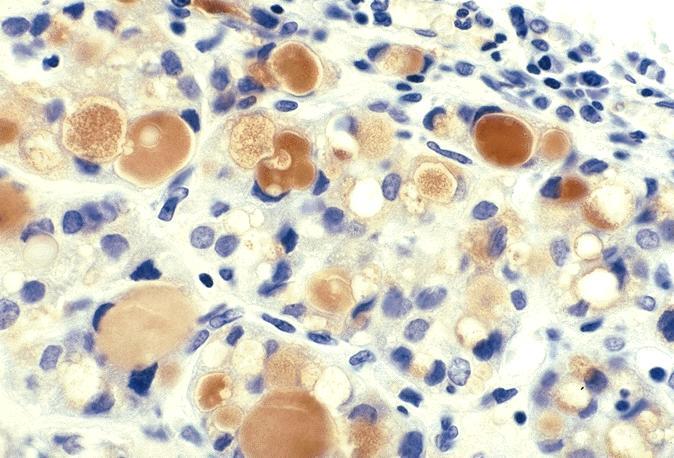
Thyroglobulin+
Alcian blue+
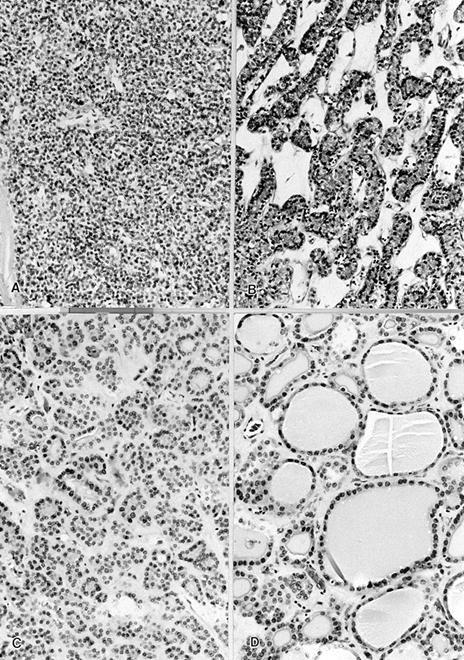
Solid, trabecular, microfollicular, macrofollicular patterns
Left: macrofollicular, right: solid pattern
Signet ring
Markedly cellular with irregular growth
Well formed follicles merge with solid pattern
Spindle cells mix with round cells
Not invasion:
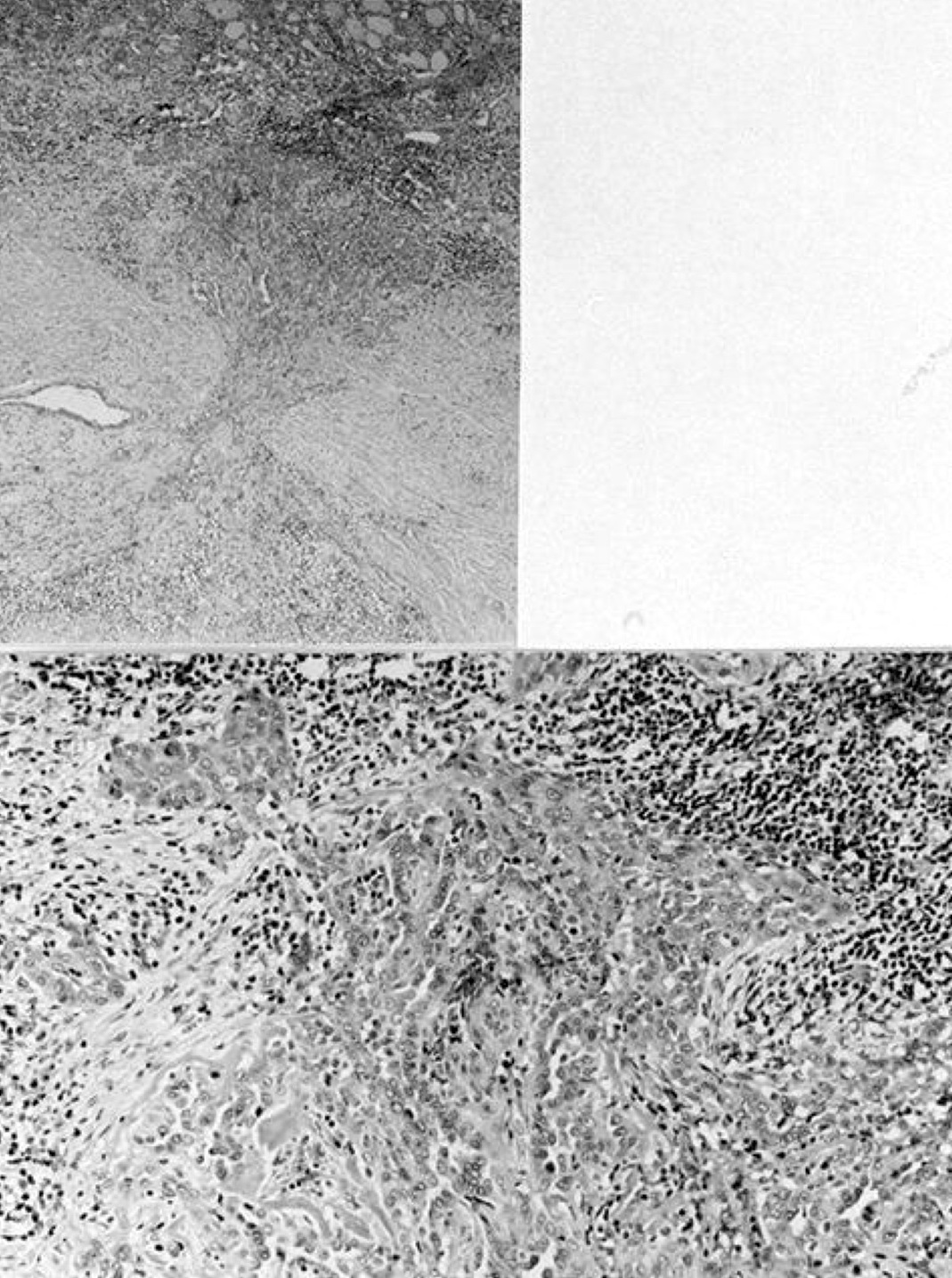
Fine needle
induced changes
resemble invasion
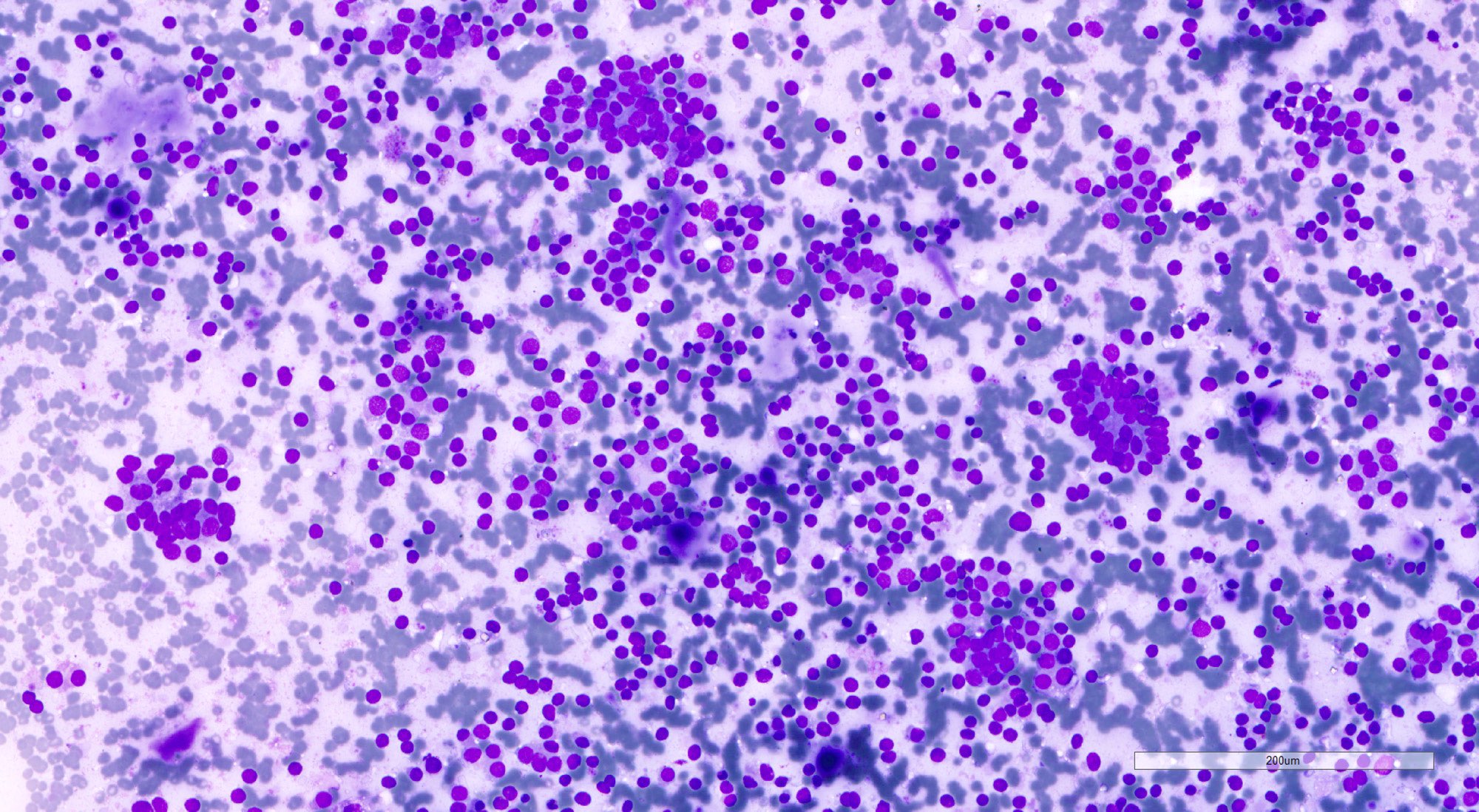
- Cellular aspirate (Korean J Pathol 2013;47:61, J Pathol Transl Med 2018;52:110)
- Cellular crowding
- Variable number of singly dispersed cells
- Microfollicular and solid / trabecular variants: numerous microfollicles, may have scant luminal colloid; absent or minimal background colloid
- Normofollicular and macrofollicular variants: monolayer sheets of follicular cells, abundant colloid; may mimic benign follicular nodule
- Hyperfunctioning follicular adenoma and follicular adenoma with papillary hyperplasia: monolayer sheets of polygonal cells with abundant cytoplasm, flame cells and occasionally, papillary fragments
- Uniform small round to ovoid nuclei, smooth nuclear margin, fine nuclear chromatin
- Absent nuclear features of papillary thyroid carcinoma
- The Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) IV (follicular neoplasm / suspicious for a follicular neoplasm [FN / SFN]), III (atypia of undetermined significance [AUS A]) or II (benign) (Thyroid 2017;27:1341, Clin Endocrinol (Oxf) 2018;88:936)
- Cannot rule out follicular thyroid carcinoma based on cytologic findings
Contributed by Shipra Agarwal, M.D. and Ayana Suzuki, C.T.
Cellular aspirate
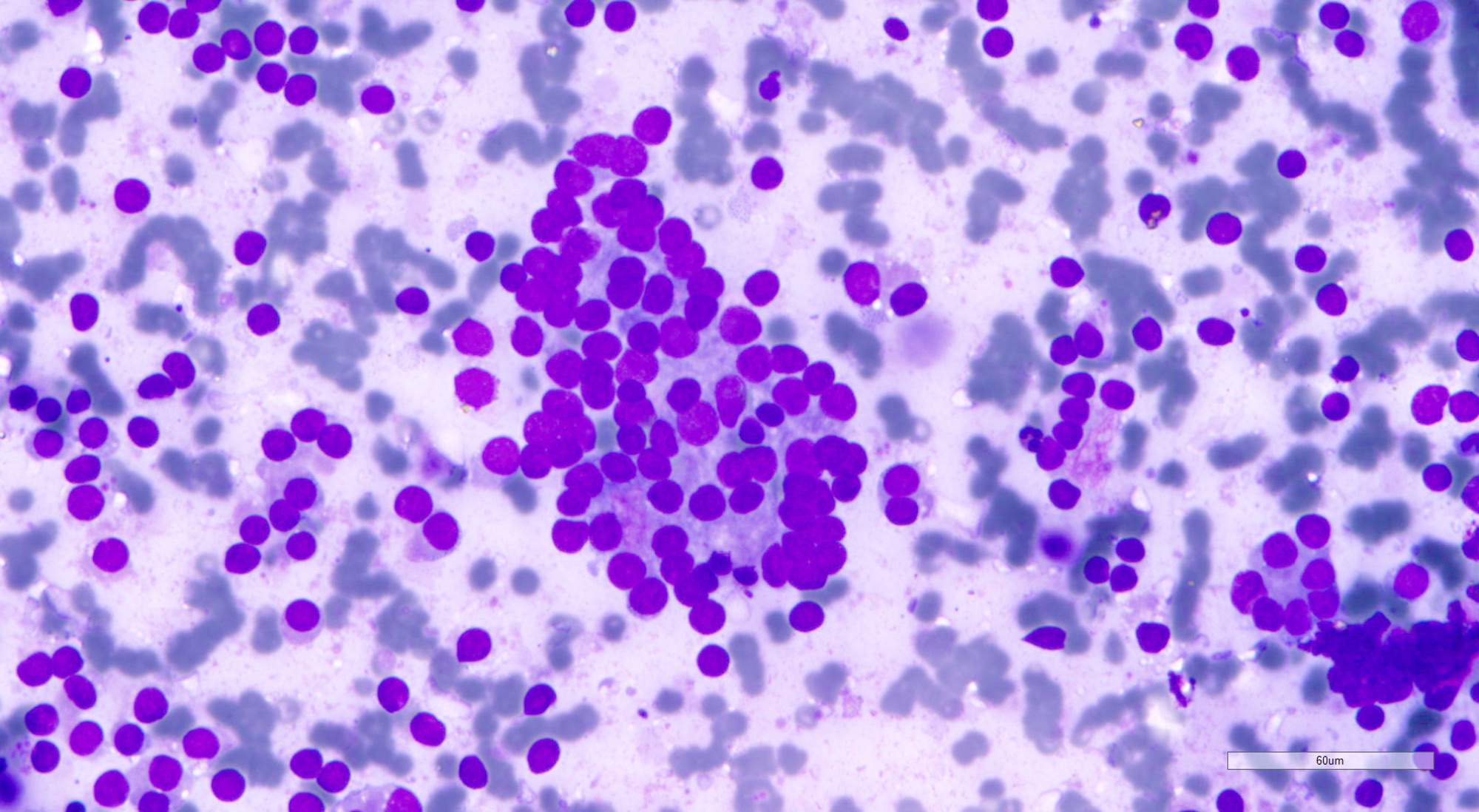
Microfollicles and small round nuclei

Microfollicles
Images hosted on other servers:


Microfollicular


Microfollicular

Microfollicular

FNA

Round hyperchromatic nuclei

FNAC

Thyroid neoplasms
- Thyroid lineage specific markers
- PAX8
- Low molecular weight cytokeratin
- CD56
- Low proliferative index (Ki67 proliferative index < 5%)
- PPARG: rare; correlates with PAX8::PPARG translocation (Am J Surg Pathol 2002;26:1016)
- CK19: usually negative, may be weak and focal (Acta Endocrinol (Buchar) 2016;12:387)
- Chromogranin
- Synaptophysin
- Calcitonin
- CK20
- Rarely galectin3, HBME-1 and CITED1; up to 1 of these can be positive when used as a panel
- Can rarely be positive
- Similar to normal thyroid gland and hyperplastic nodules
- Hyperfunctioning follicular adenomas: organelle rich cytoplasm, especially rough endoplasmic reticulum; numerous, long microvilli on surface (Am J Clin Pathol 1982;78:299)
- Clear cell follicular adenomas: cytoplasmic vesicles of variable size; these may be dilated cisternae of the rough endoplasmic reticulum or mitochondria, lysosomes or endocytic vesicles (Virchows Arch A Pathol Anat Histol 1978;380:205)
AFIP images
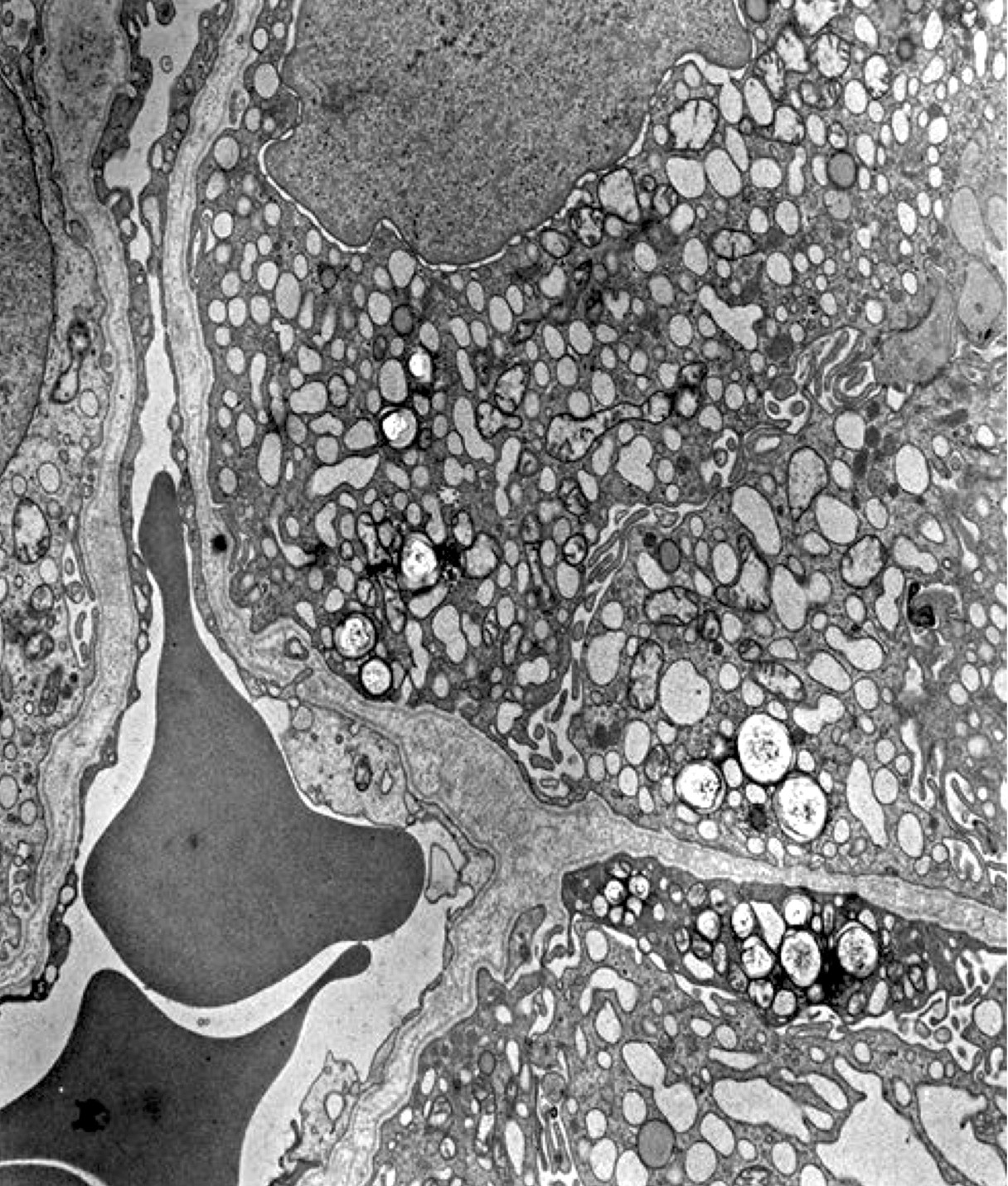
Abundant dilated endoplasmic reticulum
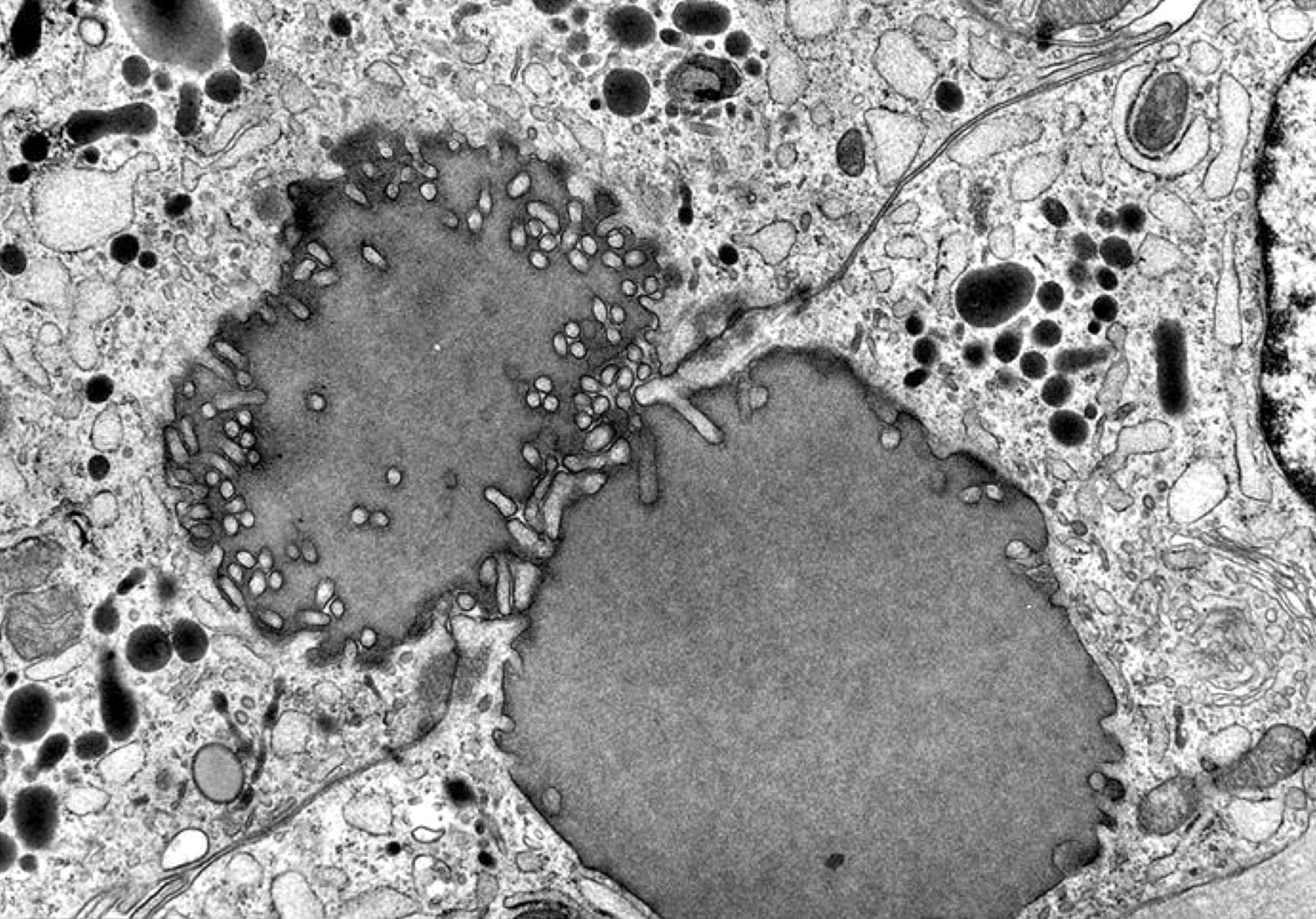
Microvilli project into well developed lumina
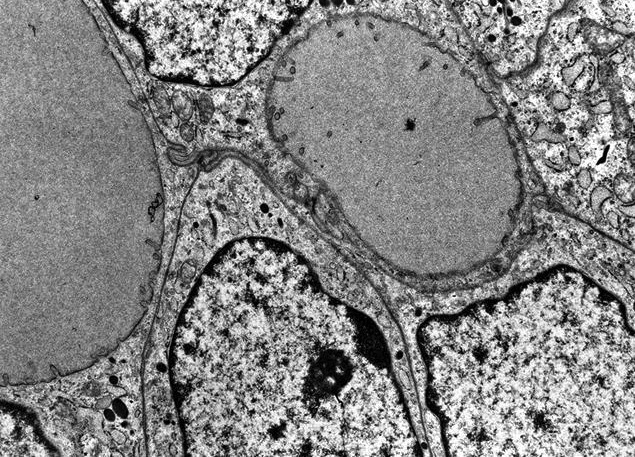
Signet ring follicular adenoma
- Clonal tumor
- RAS gene mutations (20 - 30%), most commonly codon 61 of NRAS, followed by codon 61 of HRAS and least frequently KRAS mutations (Oncotarget 2016;7:69638, PLoS Genet 2016;12:e1006239)
- EIF1AX alterations (10 - 15%) (Endocr Relat Cancer 2016;23:295, PLoS Genet 2016;12:e1006239)
- 13% (Diagn Pathol 2019;14:39)
- Microsatellite instability (MSI) (Mol Diagn Ther 2019;23:369)
- PTEN (5 - 20%) (Cancer Res 1997;57:4710)
- DICER1 (10%)
- BRAF K601E (< 1%)
- PIK3CA
- SPOP (Oncotarget 2016;7:69638)
- KMT2C
- KDM5C
- NF1
- TSHR mutations in 50 - 80% hyperfunctioning adenomas (J Clin Invest 2016;126:3383, J Mol Med (Berl) 2001;78:684)
- GNAS mutations in ~5% of hyperfunctioning adenomas
- EZH1 mutations in 20 - 30% of hyperfunctioning adenomas, usually in combination with TSHR or GNAS mutations
- THADA fusion (Thyroid 2021;31:1212)
- PAX8::PPARG fusion (~10%) (Cancer Genet Cytogenet 2010;196:7)
- Clonal cytogenetic abnormalities and copy number variations (~50%) (Cancer Genet Cytogenet 1998;101:42, PLoS Genet 2016;12:e1006239)
- Gene expression profile partially overlaps with minimally invasive follicular thyroid carcinoma and encapsulated follicular variant of papillary thyroid carcinoma; limited evidence (PLoS Genet 2016;12:e1006239, Oncotarget 2017;9:10343)
- Differential gene expression can help in differential diagnosis between follicular adenoma and follicular thyroid carcinoma (Int J Mol Sci 2017;18:1184, Endocr Connect 2018;7:124)
- Differential expression of miRNAs (miR-146-5p, miR-221-5p, miR-222-3p, miR-30e-3p, miR-152-3p, miR-185-5p, miR-1915-3p, miR-199b-5p, 199a-5p, miR-574-3p, miR-4516 and miR-148b-3p) in follicular adenoma in comparison to noninvasive follicular thyroid neoplasm with papillary-like nuclear features and infiltrative follicular variant of papillary thyroid carcinoma (Mod Pathol 2017;30:39)
Images hosted on other servers:

Gene expression analysis

CNV landscape of thyroid tumors

Driver mutations in thyroid tumors

Driver mutations and pathway analyses

Microarray and qRT PCR

Expression ratios of CRABP1, FABP4 and HMGA2

Clinicopathological features and mutation spectrum



Hierarchical clustering
Solitary thyroid nodule
Thyroid: compare and contrast
Histopathology thyroid: follicular adenoma (microfollicular)
- Thyroid, right lobectomy:
- Follicular adenoma, right lobe, 3.2 cm
- Nodular hyperplasia with dominant nodule:
- Hyperplastic changes elsewhere in gland
- Often not encapsulated or incomplete capsule of variable thickness
- Variable architectural patterns
- May be multiple; lack of compression signs in adjacent thyroid gland
- Minimally invasive follicular thyroid carcinoma:
- Thick capsule
- Vascular or capsular invasion
- May show increased mitotic activity; may have foci of necrosis
- Immunoreactivity for > 1 of the following markers: galectin3, HBME-1, CITED1 and PPARG
- Presence of PAX8::PPARG or THADA fusions (Diagn Pathol 2010;5:9, Clin Chem 2010;56:391)
- Follicular variant of papillary carcinoma:
- Nuclear features of papillary thyroid carcinoma
- Invasive features, vascular or capsular invasion
- Immunopositive for multiple markers, namely CK19, galectin3, HBME-1, CITED1 and RET; immunonegative for CD56 (Acta Endocrinol (Buchar) 2016;12:387, Diagn Pathol 2010;5:9, Pathol Res Pract 2009;205:303)
- Noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP):
- Nuclear features of papillary thyroid carcinoma with a nuclear score of 2 or 3 (JAMA Oncol 2016;2:1023)
- Well differentiated tumor of uncertain malignant potential (WDT-UMP):
- Encapsulated tumor
- Equivocal nuclear features of papillary thyroid carcinoma
- Questionable blood vessel or capsular invasion
- Follicular tumor of uncertain malignant potential (FT-UMP):
- Encapsulated tumor
- Questionable vascular or capsular invasion
- Lacks nuclear features of papillary thyroid carcinoma
- Papillary thyroid carcinoma, encapsulated variant:
- Among differential diagnosis of follicular adenoma with papillary hyperplasia
- Nuclear features of papillary thyroid carcinoma
- Papillary thyroid carcinoma, tall cell variant:
- Intrathyroidal parathyroid adenoma / hyperplasia:
- Can mimic follicular adenoma of microfollicular, clear cell type
- Positive for PTH, GATA3, chromogranin, synaptophysin
- Negative for thyroglobulin, TTF1
- Encapsulated medullary thyroid carcinoma of solid or trabecular pattern or with spindle or clear cells:
- Invasive features
- Amyloid deposition
- Salt and pepper chromatin
- Calcitonin positive, thyroglobulin negative
Which of the following best describes this thyroid tumor?
- Benign, completely encapsulated, lacks nuclear features of papillary thyroid carcinoma, absent capsular and vascular invasion
- Benign, partially encapsulated, lacks nuclear features of papillary thyroid carcinoma, absent capsular and vascular invasion
- Malignant, encapsulated, lacks nuclear features of papillary thyroid carcinoma, capsular invasion present
- Uncertain malignant potential, completely encapsulated, lacks nuclear features of papillary thyroid carcinoma, questionable capsular invasion
- Uncertain malignant potential, completely encapsulated, nuclear score 2, lacks capsular and vascular invasion
Comment Here
Reference: Follicular adenoma
- Galectin3+, HBME-1+, CITED1+
- PAX8-, calcitonin+, chromogranin+
- TTF1+, CD56+, PAX8+
- TTF1+, CK19+, HBME-1+
- TTF1-, synaptophysin+, GATA3+
Comment Here
Reference: Follicular adenoma

