
Uterus
Mixed epithelial and mesenchymal tumors
Atypical polypoid adenomyoma
Author: Stephanie L. Skala, M.D.
Editorial Board Member: Ricardo R. Lastra, M.D.
Deputy Editor-in-Chief: Jennifer A. Bennett, M.D.

Last author update: 26 April 2022
Last staff update: 31 August 2023
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Atypical polypoid adenomyoma

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Skala SL. Atypical polypoid adenomyoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/uterusapa.html. Accessed April 16th, 2024.
Definition / general
- Polypoid lesion composed of atypical, architecturally complex endometrial glands within benign myomatous / fibromyomatous stroma (Am J Surg Pathol 2015;39:1148)
Essential features
- Biphasic neoplasm composed of crowded atypical endometrial glands (with or without squamous morules) in myomatous / fibromyomatous stroma
- Stroma typically positive for SATB2, in contrast to most examples of myoinvasive carcinoma
- Risk of recurrence or concurrent or subsequent endometrial endometrioid carcinoma
Terminology
- Atypical polypoid adenomyofibroma
ICD coding
- ICD-11: XH7ZB1 - atypical polypoid adenomyoma
Epidemiology
- Usually diagnosed in women of reproductive age; range of 25 - 73 years (Am J Surg Pathol 1996;20:1)
- Associated with obesity, infertility, nulliparity
Sites
- Lower uterine segment > uterine corpus
Pathophysiology
- Prolonged estrogenic stimulation plays a role in some cases (Int J Gynecol Pathol 1987;6:104)
- Progesterone may have a role in development of the stroma of atypical polypoid adenomyoma (Hum Pathol 2014;45:33)
- Overlapping molecular and immunohistochemical features with atypical hyperplasia (Am J Surg Pathol 2015;39:1148)
Etiology
- Unknown
Clinical features
- Abnormal vaginal bleeding
- Incidental finding during evaluation of infertility
- May occur in the setting of Turner syndrome (Int J Gynecol Pathol 1987;6:104)
- Rare report of occurrence in patient with Cowden syndrome (Gynecol Oncol Case Rep 2012;2:29)
- Reference: Pathol Res Pract 2019;215:766
Diagnosis
- Based on histologic features
Radiology description
- T2 weighted MRI images: slightly hyperintense polypoid mass mixed with markedly hyperintense foci corresponding to endometrial glands
- T1 weighted MRI images: isointense with myometrium, occasional hyperintense cystic foci
- Solid portions, other than cystic foci, show contrast enhancement in the arterial phase and washout or plateau pattern in the late phase
- Reference: J Comput Assist Tomogr 2015;39:32
Prognostic factors
- Approximately 30 - 44% recur after conservative treatment; higher risk of recurrence if sampling is not under hysteroscopic visualization (Int J Gynaecol Obstet 2021 Dec 18 [Epub ahead of print], Medicine (Baltimore) 2020;99:e20491)
- Concurrent diagnosis of endometrial endometrioid carcinoma in ~11%; diagnosis of endometrial carcinoma during follow up in ~14% (Medicine (Baltimore) 2020;99:e20491)
- High likelihood of successful pregnancy after conservative treatment (Medicine (Baltimore) 2020;99:e20491)
Case reports
- 29 year old woman with low grade endometrioid adenocarcinoma arising from atypical polypoid adenomyoma; diagnosed in early pregnancy and managed conservatively (Gynecol Oncol Rep 2019;28:101)
- 35 year old woman with atypical polypoid adenomyoma treated by hysteroscopy with photodynamic diagnosis using 5-aminolevulinic acid (Photodiagnosis Photodyn Ther 2019;27:295)
- 36 year old woman with endometrioid adenocarcinoma developing 8 years after conservative management for atypical polypoid adenomyoma (Gynecol Oncol Case Rep 2014;8:21)
- 45 year old woman with atypical polypoid adenomyoma treated with local resection (Pathologica 2020;112:214)
Treatment
- Conservative management and close follow up can be considered for women that desire fertility preservation; addition of progestin does not seem to improve oncologic outcomes (Int J Gynaecol Obstet 2021 Dec 18 [Epub ahead of print])
- One proposed strategy: transvaginal ultrasonography plus hysteroscopic biopsy every 3 months for 2 years, every 4 - 6 months for another 3 years and then once a year (Arch Gynecol Obstet 2016;293:177)
- Small case series suggests a potential role for photodynamic therapy to ensure complete resection (Photodiagnosis Photodyn Ther 2021;36:102583)
- Hysterectomy, if peri or postmenopausal (Int J Gynaecol Obstet 2021 Dec 18 [Epub ahead of print])
Gross description
- Firm polypoid lesion
- Typically unifocal
- Average size of 2 cm
- Reference: Am J Clin Pathol 1986;86:139
Gross images
Images hosted on other servers:

Polypoid mass
Microscopic (histologic) description
- Biphasic tumor:
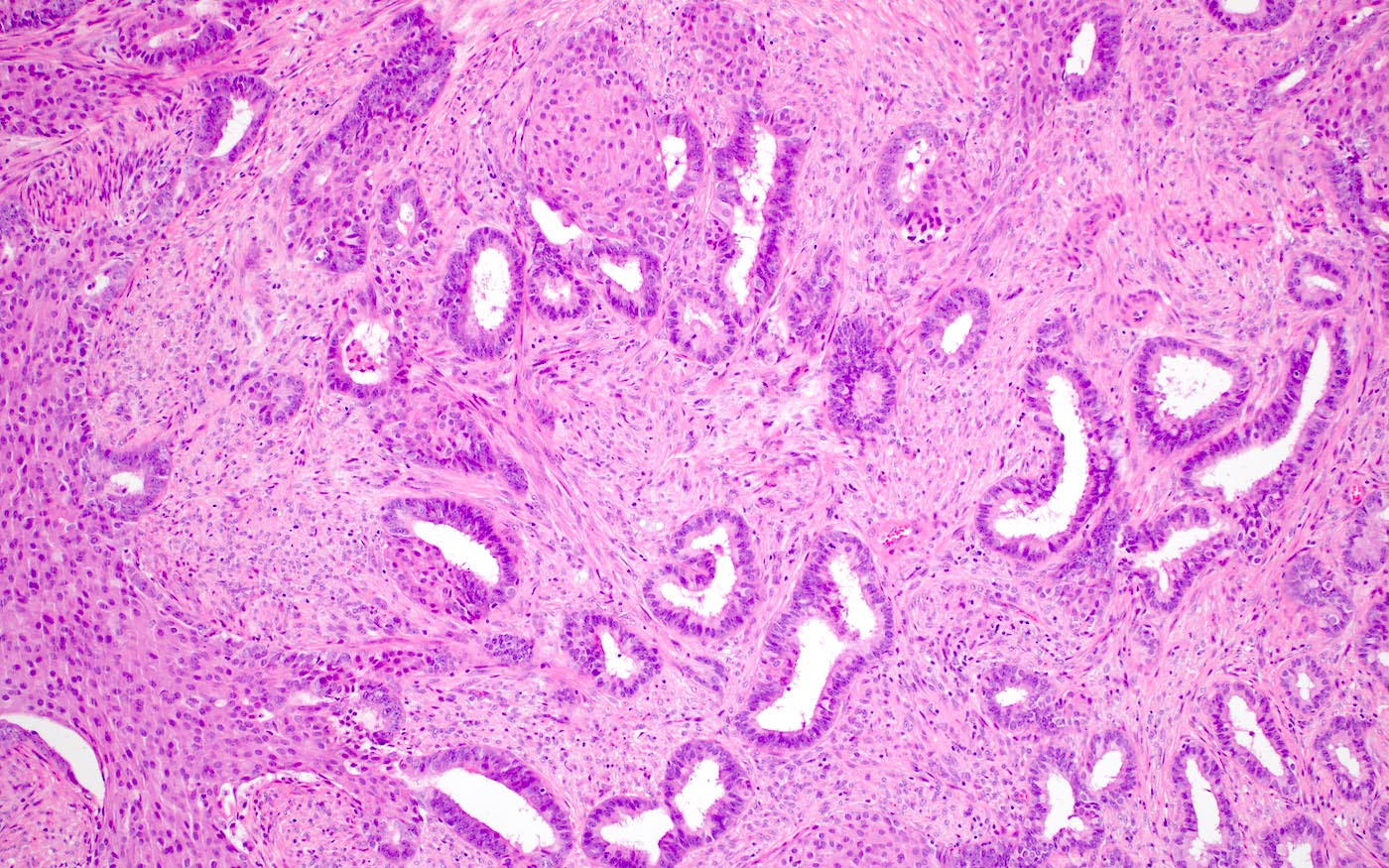
- Endometrioid glands, usually with complex architecture and sometimes with cytologic atypia
- Glandular component often shows lobulated architecture
- Benign fibromyomatous stroma, rarely with myxoid change
- Squamous morular metaplasia is frequently seen and may show central necrosis
- Well circumscribed or slightly irregular margin
- Reference: Am J Surg Pathol 2015;39:1148
Microscopic (histologic) images
Contributed by Stephanie L. Skala, M.D.
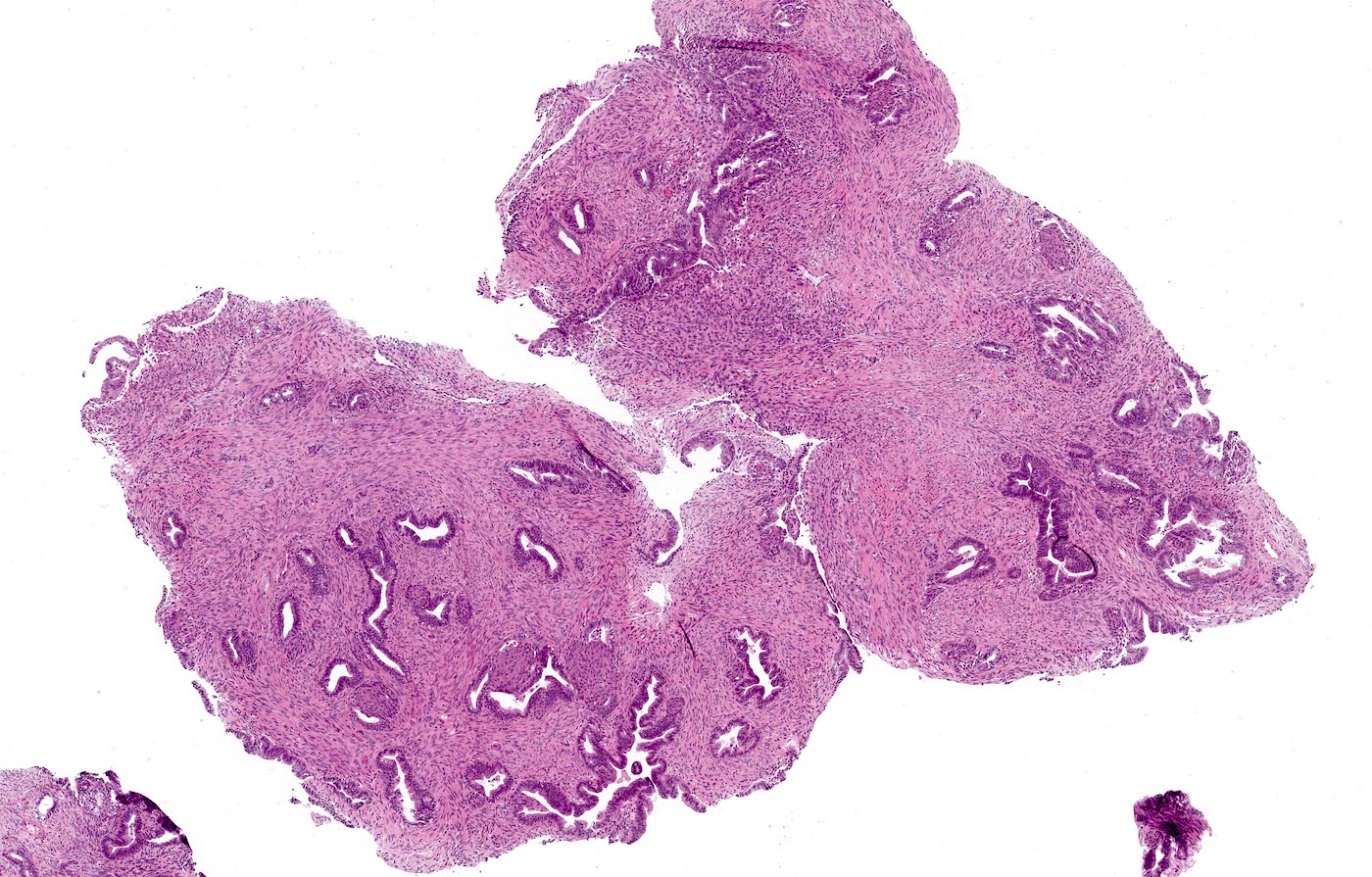
Lobulated architecture
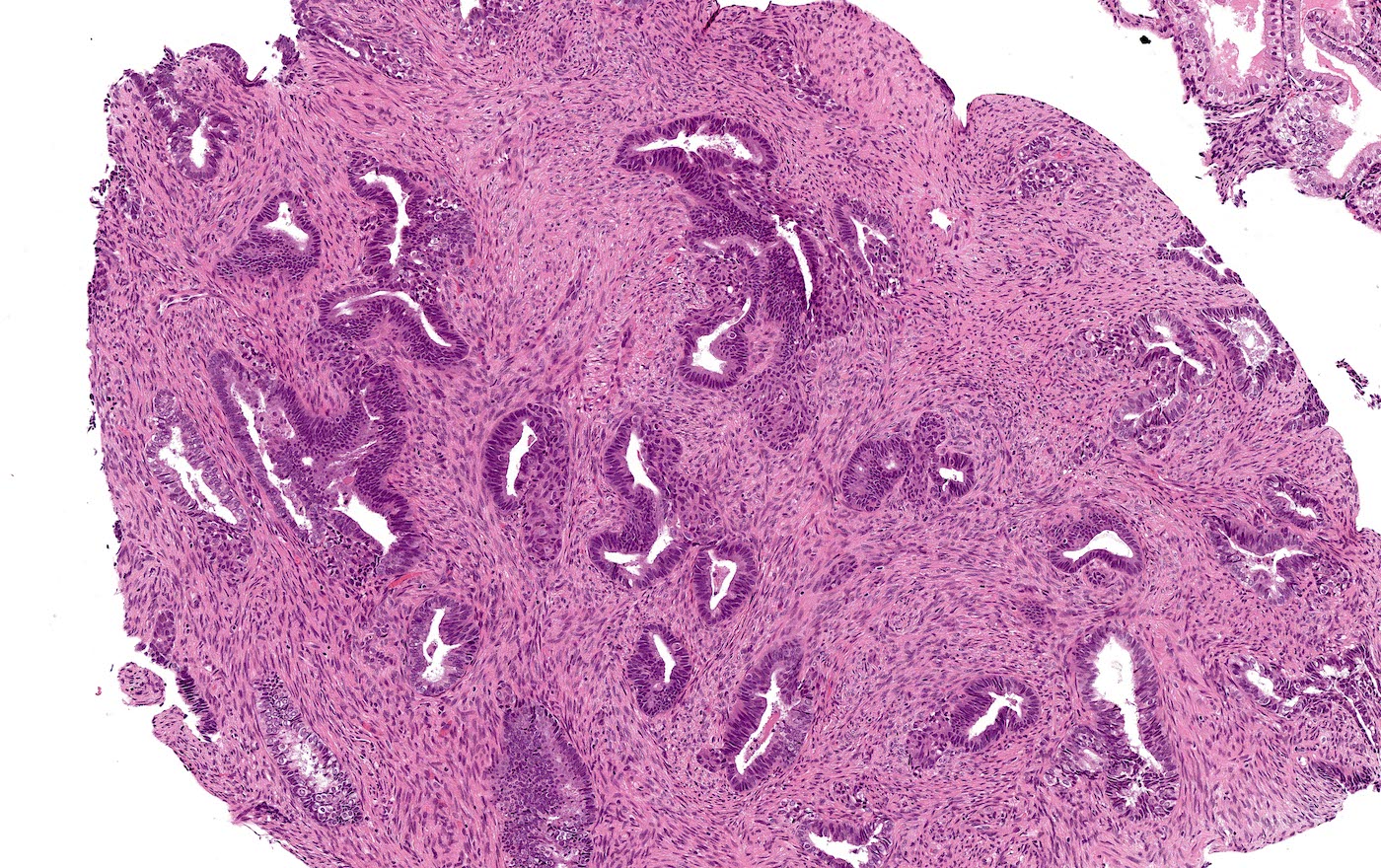
Crowded glands and muscular stroma
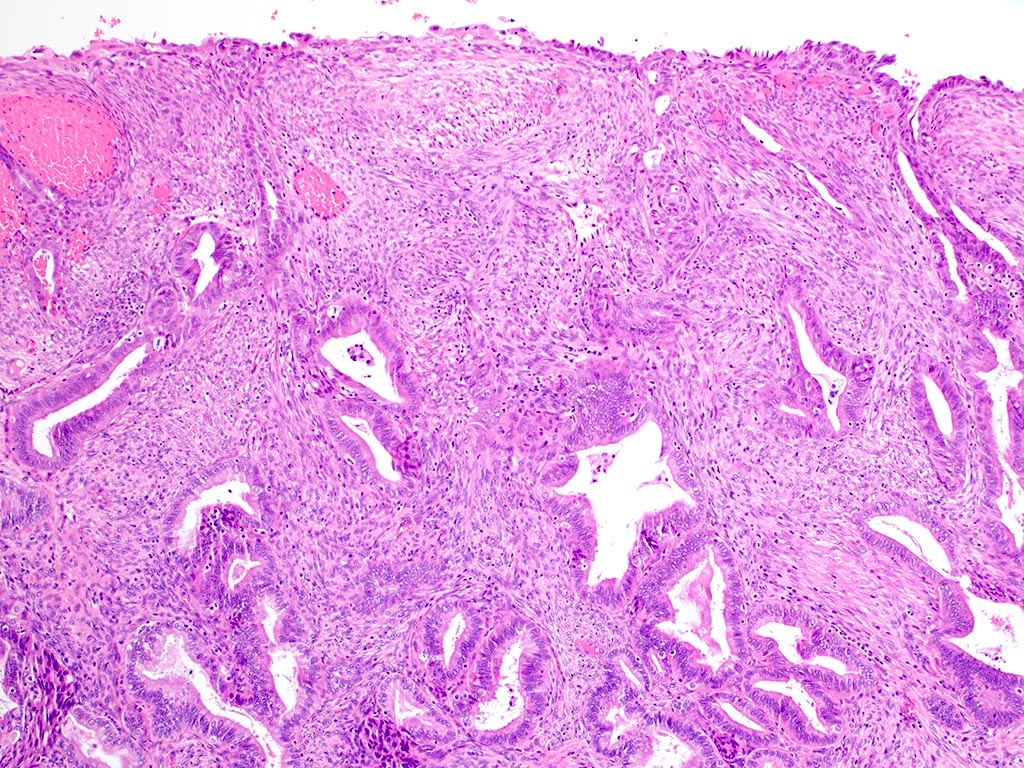
Smooth muscle underlying surface endometrium
Crowded glands and muscle bundles
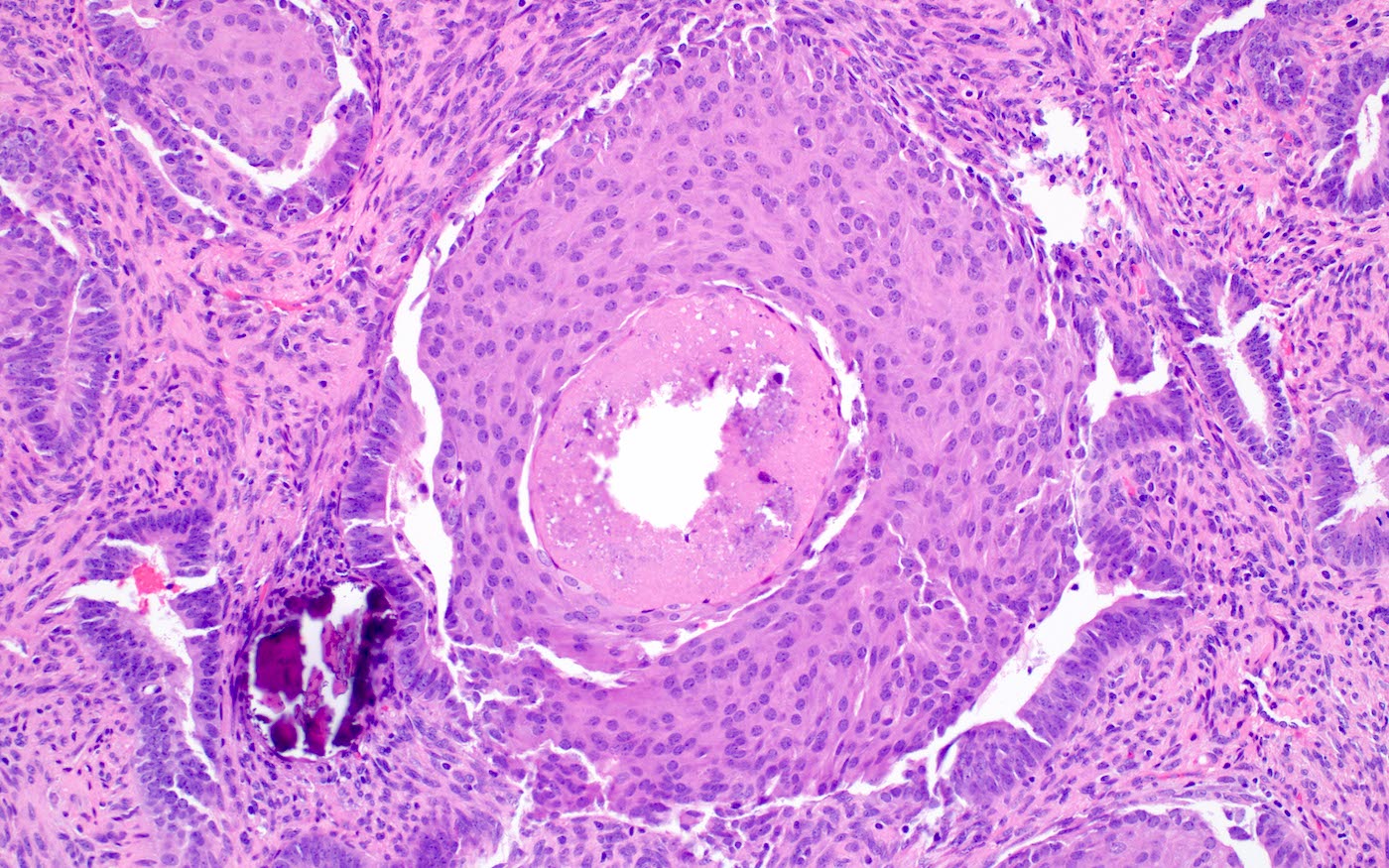
Squamous morule with central necrosis
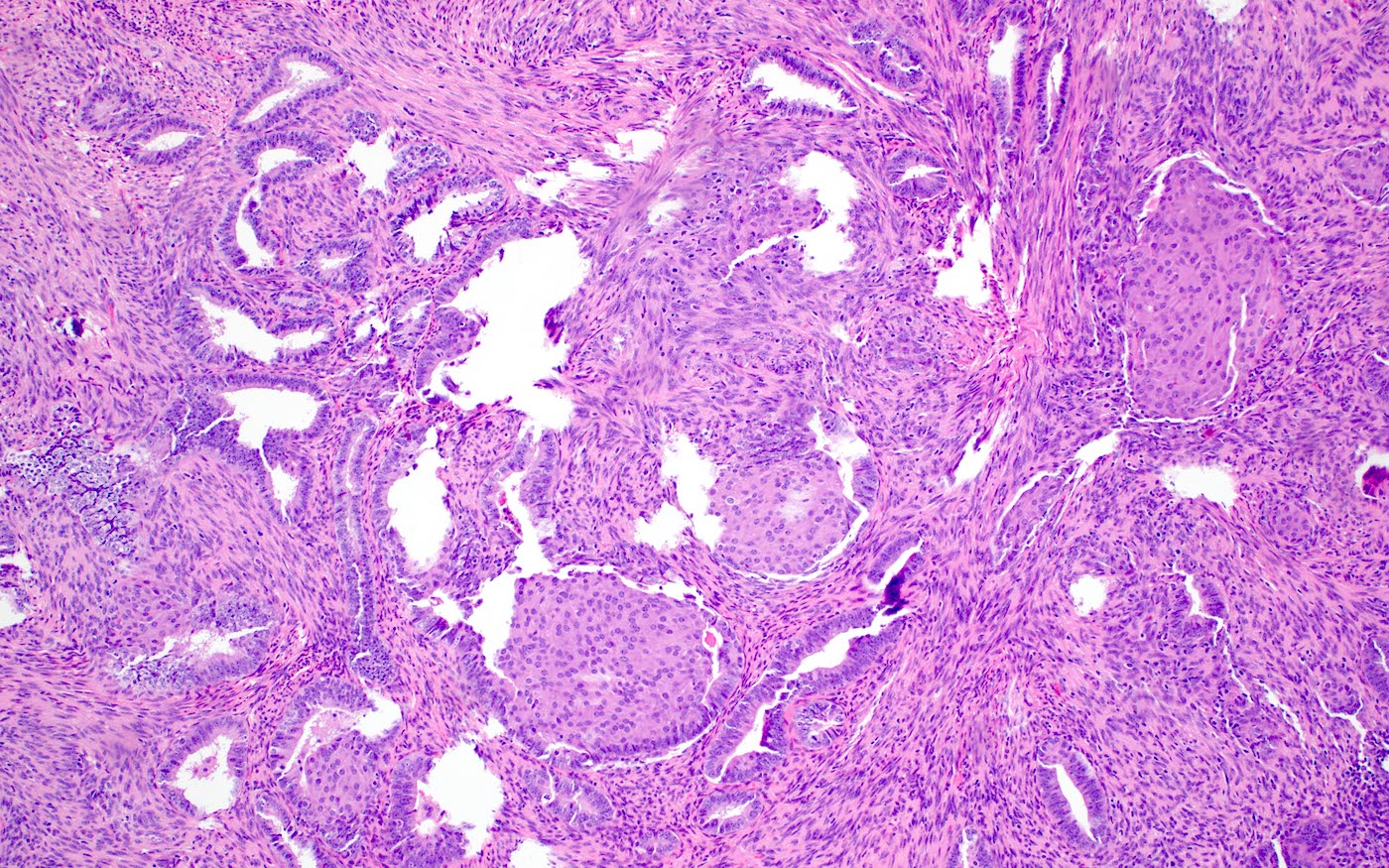
Haphazard gland arrangement

Myxoid spindled stroma
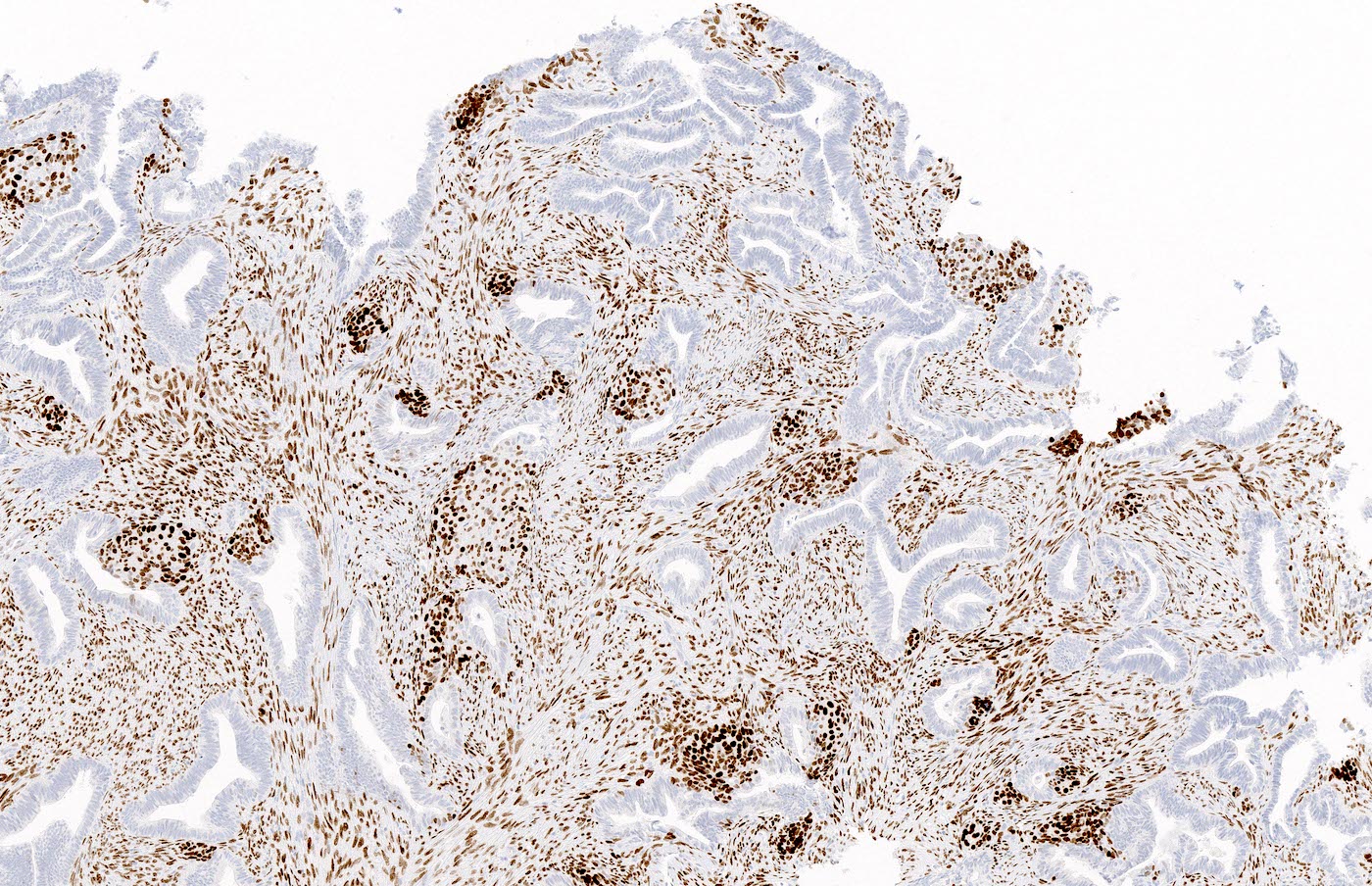

Stromal SATB2 positivity
Positive stains
- Beta catenin nuclear positivity (squamous morules > glands) (Hum Pathol 2014;45:33)
- SATB2 reactivity in the stromal component (Histopathology 2021;79:96, Int J Gynecol Pathol 2019;38:397)
- Pancytokeratin, estrogen receptor and progesterone receptor typically positive in glands
- Smooth muscle actin and desmin positive in stromal muscle (Appl Immunohistochem Mol Morphol 2020;28:646)
- CDX2 and p16 positive in squamous morules (Appl Immunohistochem Mol Morphol 2020;28:646, Histopathology 2021;79:96)
Negative stains
- CD10 and caldesmon negative in stroma (Appl Immunohistochem Mol Morphol 2020;28:646)
Molecular / cytogenetics description
- CTNNB1 mutation, PTEN deletion and KRAS mutation (Am J Surg Pathol 2015;39:1148, Hum Pathol 2014;45:33)
- MLH1 promoter hypermethylation and microsatellite instability (Hum Pathol 2003;34:784)
Sample pathology report
- Uterus, total hysterectomy:
- Atypical polypoid adenomyoma
Differential diagnosis
- Endometrial atypical hyperplasia (complex atypical hyperplasia / endometrioid intraepithelial neoplasia):
- Lacks muscular stroma
- Involves flat endometrium or polyps without myomatous stroma
- Myoinvasive endometrioid carcinoma:
- Fragments of myometrium with invasive carcinoma often admixed with separate fragments of endometrioid carcinoma
- May show desmoplasia
- Muscular stroma negative for SATB2 by immunohistochemistry
- Endometrial polyp:
- Lacks muscular stroma
- Some cases may show endometrial hyperplasia with or without squamous morules
- Adenosarcoma:
- Benign endometrial glands and malignant stroma
- Carcinosarcoma:
- Malignant endometrial glands and stroma
Board review style question #1
The tumor above is seen in endometrial curettings from a 36 year old patient. Which of the following statements is true?
- Atypical polypoid adenomyoma can progress to endometrioid carcinoma
- Atypical polypoid adenomyoma is associated with TP53 mutations
- Comedonecrosis of squamous morules implies poor prognosis
- Hysterectomy is always the first line treatment for atypical polypoid adenomyoma
- Progestin typically leads to regression of atypical polypoid adenomyoma
Board review style answer #1
A. Atypical polypoid adenomyoma can progress to endometrioid carcinoma
Comment here
Reference: Atypical polypoid adenomyoma
Comment here
Reference: Atypical polypoid adenomyoma
Board review style question #2
Patients with atypical polypoid adenomyoma that are diagnosed on endometrial biopsy are at an increased risk for which of the following?
- Carcinosarcoma
- Clear cell carcinoma
- Endometrioid carcinoma
- Endometriosis
- Serous carcinoma
Board review style answer #2
