
Salivary glands
Primary salivary gland neoplasms
Benign
Pleomorphic adenoma

Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed search: Pleomorphic adenoma
- Benign triphasic salivary gland neoplasm composed of epithelial (ductal) cells, myoepithelial cells and chondromyxoid stroma
- Triphasic salivary gland tumors with ductal cells, myoepithelial cells and stromal component
- Most common salivary gland neoplasm
- Benign mixed tumor
- Most common salivary gland tumor in both children and adults (Hum Pathol 2018;73:194, El-Naggar: WHO Classification of Head and Neck Tumours, 4th Edition, 2017)
- Affects patients of all ages, most commonly in 30s - 60s
- F > M (2:1)
- Most commonly affected site is the parotid gland (84% of cases)
- May also occur in other major salivary glands (submandibular and sublingual glands), lacrimal gland and minor salivary glands of upper aerodigestive tract (El-Naggar: WHO Classification of Head and Neck Tumours, 4th Edition, 2017)
- Prior radiation increases the risk of developing pleomorphic adenoma
- Slow growing, painless, well circumscribed mass involving salivary gland
- Diagnosis can be rendered on preoperative cytology or biopsy, showing typical metachromatic fibrillary stroma (in cytology) or triphasic growth pattern (on biopsy)
- Rare, controversial clinical entity with late metastasis (6 - 52 years) after tumor excision
- Metastatic sites include bone, CNS, kidney, liver, lung, lymph nodes, maxilla, pharynx, skin, sphenoid sinus
- Benign morphology in original and metastatic tumor
- Associated with incomplete pleomorphic adenoma surgery / local recurrence, post cardiac transplant patient / immunosuppression (Mod Pathol 1998;11:1142)
- Mass with well defined or bosselated border, hyperintense on T2 MRI
Images hosted on other servers:

MRI parotid tumor
- Benign tumor: surgical resection with negative margin is considered curative
- Enucleation is associated with 15 - 25% risk of local recurrence
- Recurrences are usually within 18 months but can be up to 50 years later (Arch Pathol Lab Med 2008;132:1445)
- Risk of malignant transformation is ~5%
- Risk factors for malignant transformation: multiple recurrences, submandibular location, older age, larger size, prominent hyalinization, increased mitotic rate (if present, sample tumor more thoroughly), radiation exposure
- 6 year old girl with pleomorphic adenoma of the parotid gland (Children (Basel) 2018;5:E127)
- 28 year old man with submandibular mass (Case #243)
- 54 year old man with painless swelling over left half of upper lip for past 10 years (Case #392)
- 84 year old man, a former smoker, with enlarging parotid gland lesion (Case #404)
- Metastasizing pleomorphic adenoma with recurrent PLAG1 or HMGA2 fusion (Am J Surg Pathol 2019;43:1145)
- Complete surgical resection with negative margin is the mainstream treatment
- Enucleation is not advocated given the high risk of local recurrence
- Radiation therapy may be considered in symptomatic recurrent cases not amenable to surgical treatment (El-Naggar: WHO Classification of Head and Neck Tumours, 4th Edition, 2017)
Images hosted on other servers:

Minor salivary gland tumor

Mass over mandible

Parotid tumor

Large submandibular mass

Parotid tumor
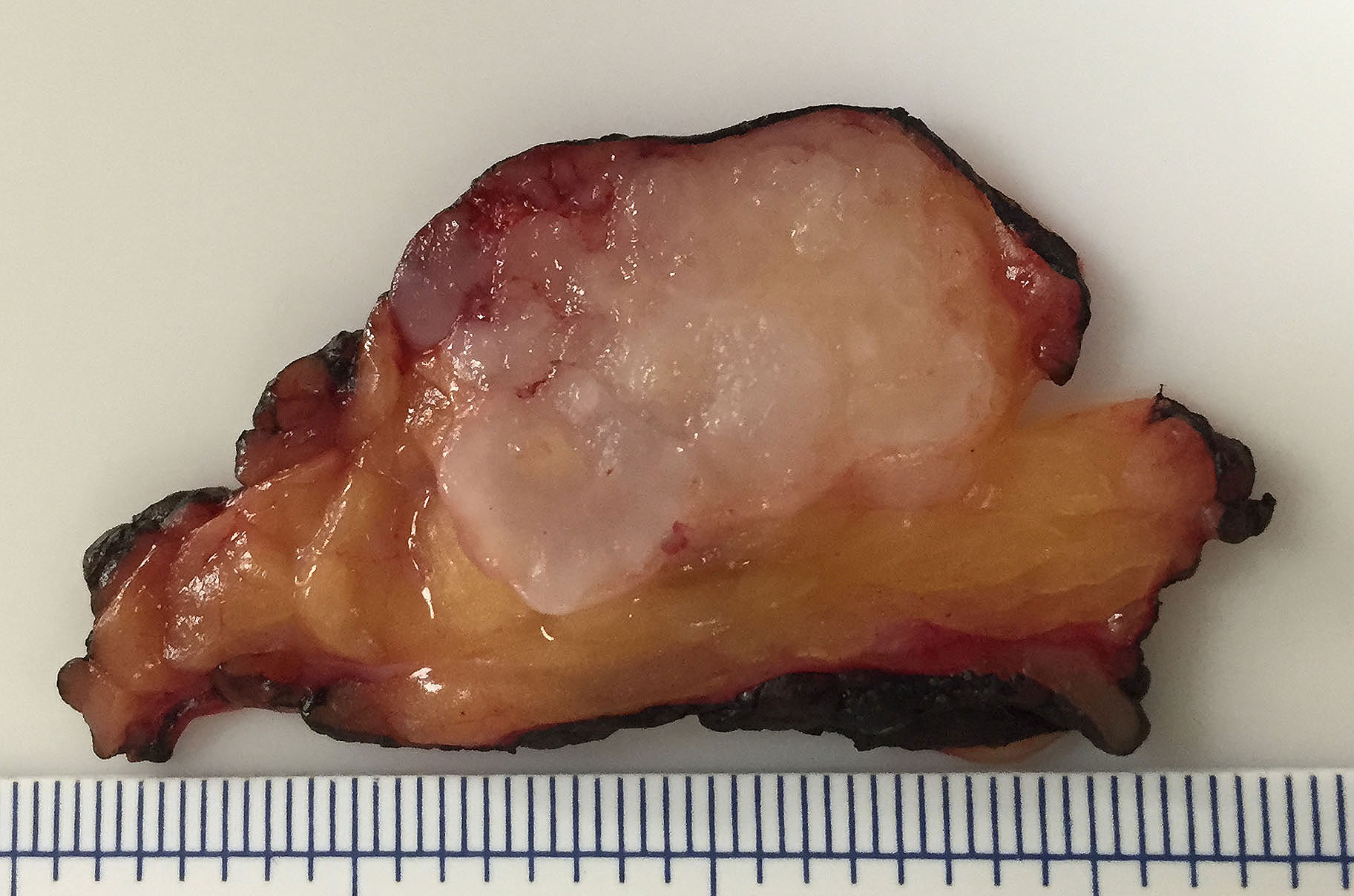
- Primary tumor: well demarcated, bosselated gray-white myxoid mass
- Recurrent tumor: numerous myxoid to fibrotic nodules of various size, giving a shotgun bullet appearance
Contributed by Bin Xu, M.D., Ph.D. and Kelly Magliocca D.D.S., M.P.H.


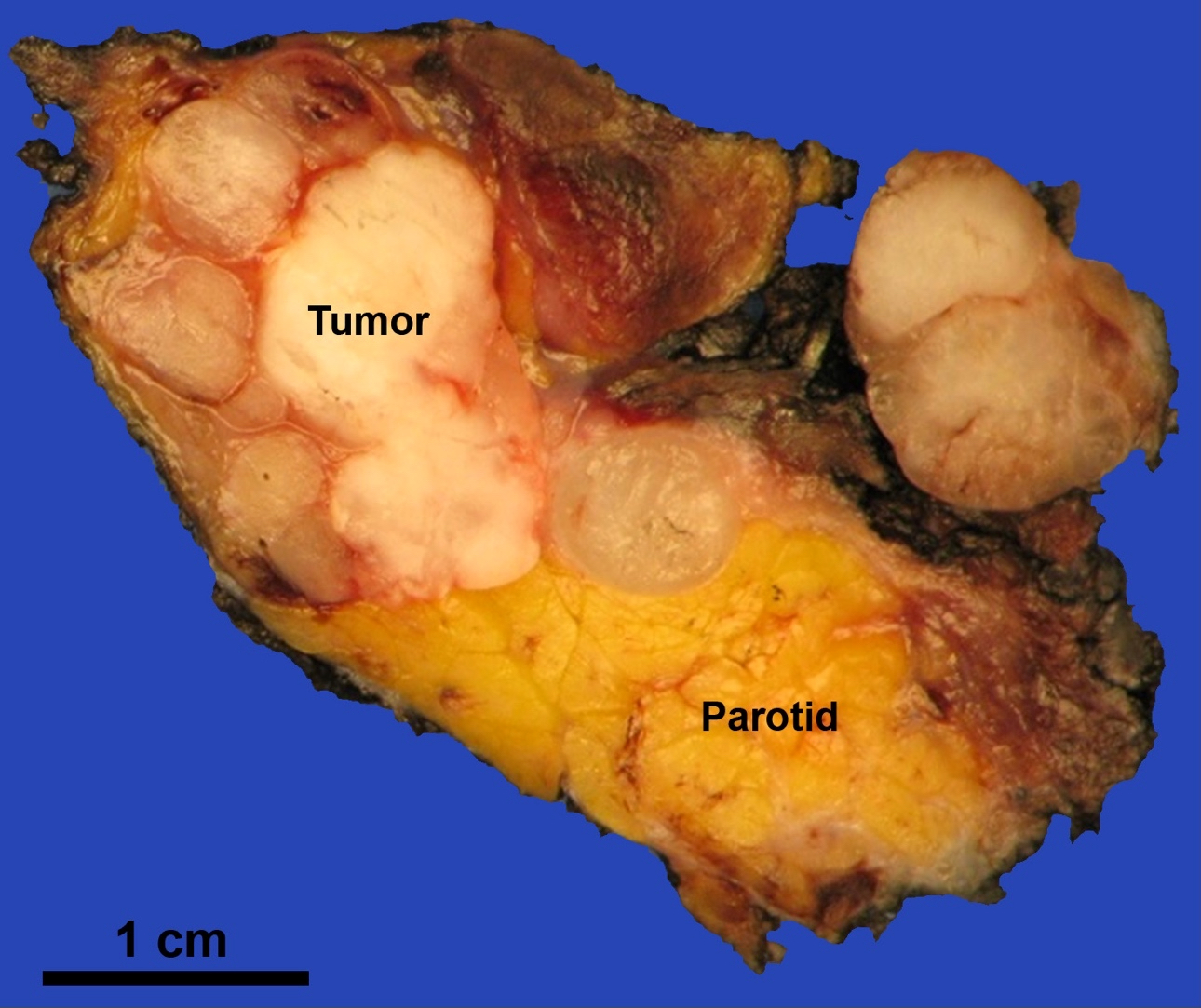
Primary pleomorphic adenoma
Recurrent pleomorphic adenoma


Pleomorphic adenoma
Case #392

External surface

Cut surface
- Bosselated outer surface, often with tongue-like protrusions (pseudopods)
- Typically has 3 components:
- Epithelial (ductal) component forming the inner layer of cysts and tubules
- Myoepithelial cells as the outer layer of cysts and tubules and scattered within the myxoid stroma
- Cytology of myoepithelial cells can be plasmacytoid, spindled, epithelioid, clear or stellate shaped
- Stromal component is typically myxoid, chondroid or myxochondroid
- It can also be hyalinized or fibrotic
- Metaplastic changes may be seen, e.g. adipose metaplasia, osseous metaplasia, squamous metaplasia (sometimes with keratinization), sebaceous metaplasia and mucinous metaplasia
- Intravascular permeation has been reported in a small percentage of cases and does not increase the risk of recurrence or distant metastasis
- It is proposed to be a phenomenon associated with surgical manipulation (Am J Surg Pathol 2012;36:1674)
- Other features that may be seen in pleomorphic adenoma include
- Tyrosine crystal: dense amorphous eosinophilic floret shaped crystal
- Increased cellularity: so called cellular pleomorphic adenoma
- Increased mitotic activity
- Myoepithelial rich area or tumor
Contributed by Bin Xu, M.D., Ph.D. and Andrey Bychkov, M.D., Ph.D.

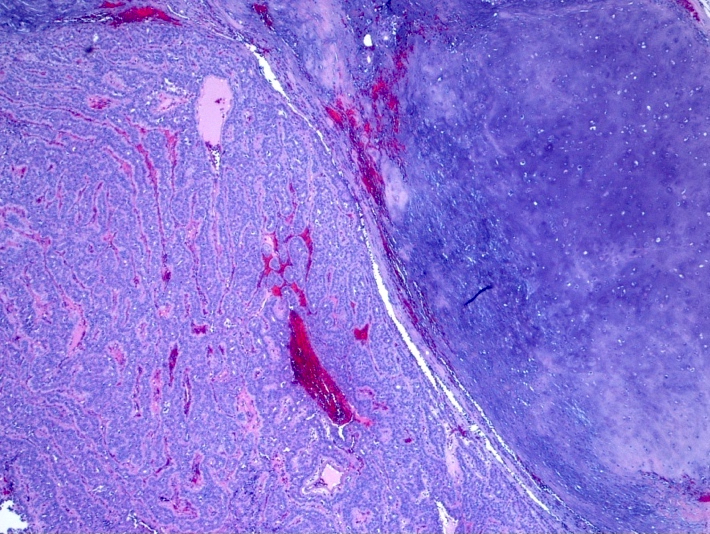
Encapsulated mass

Bosselated interface
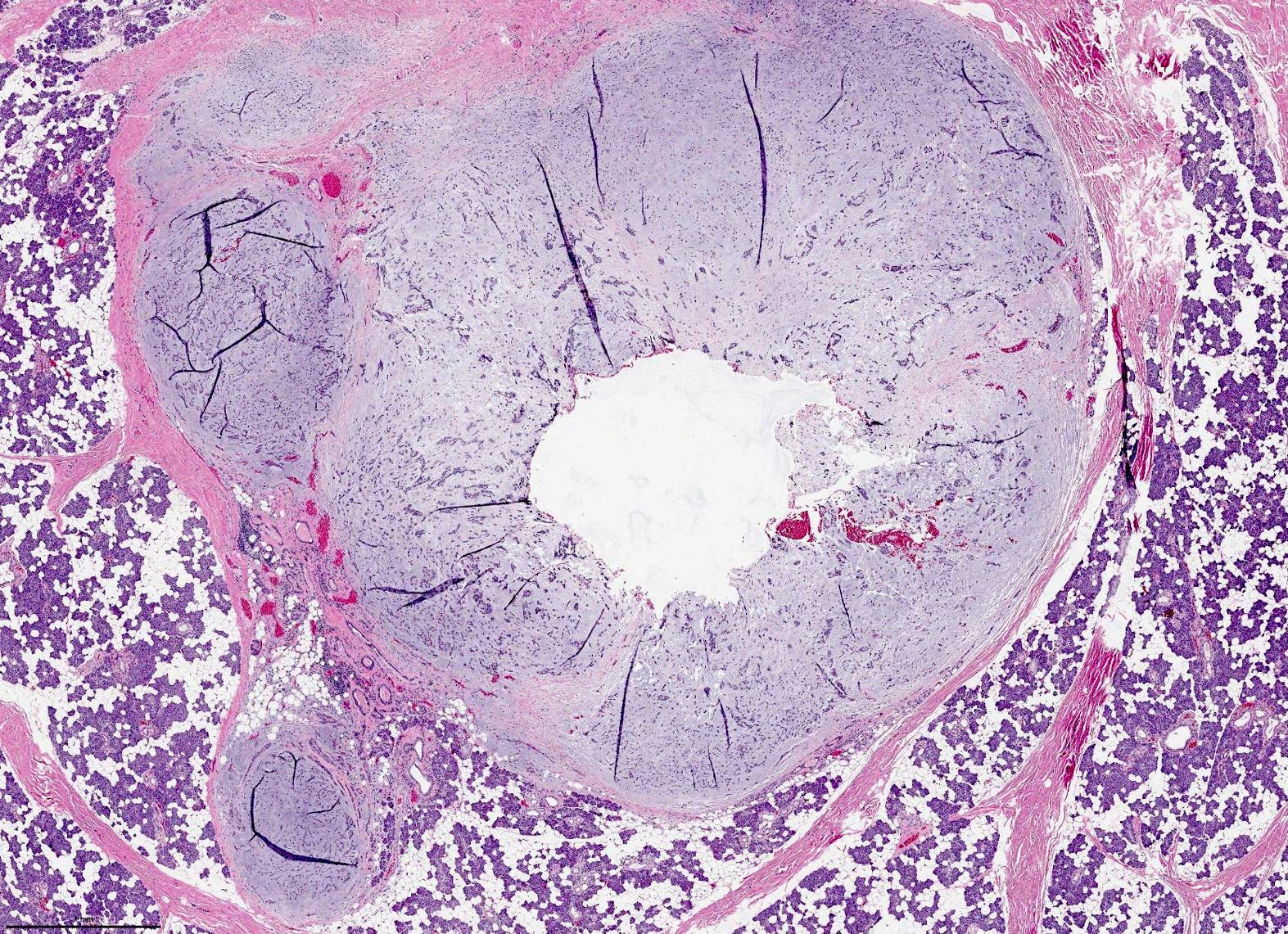
Pseudopods
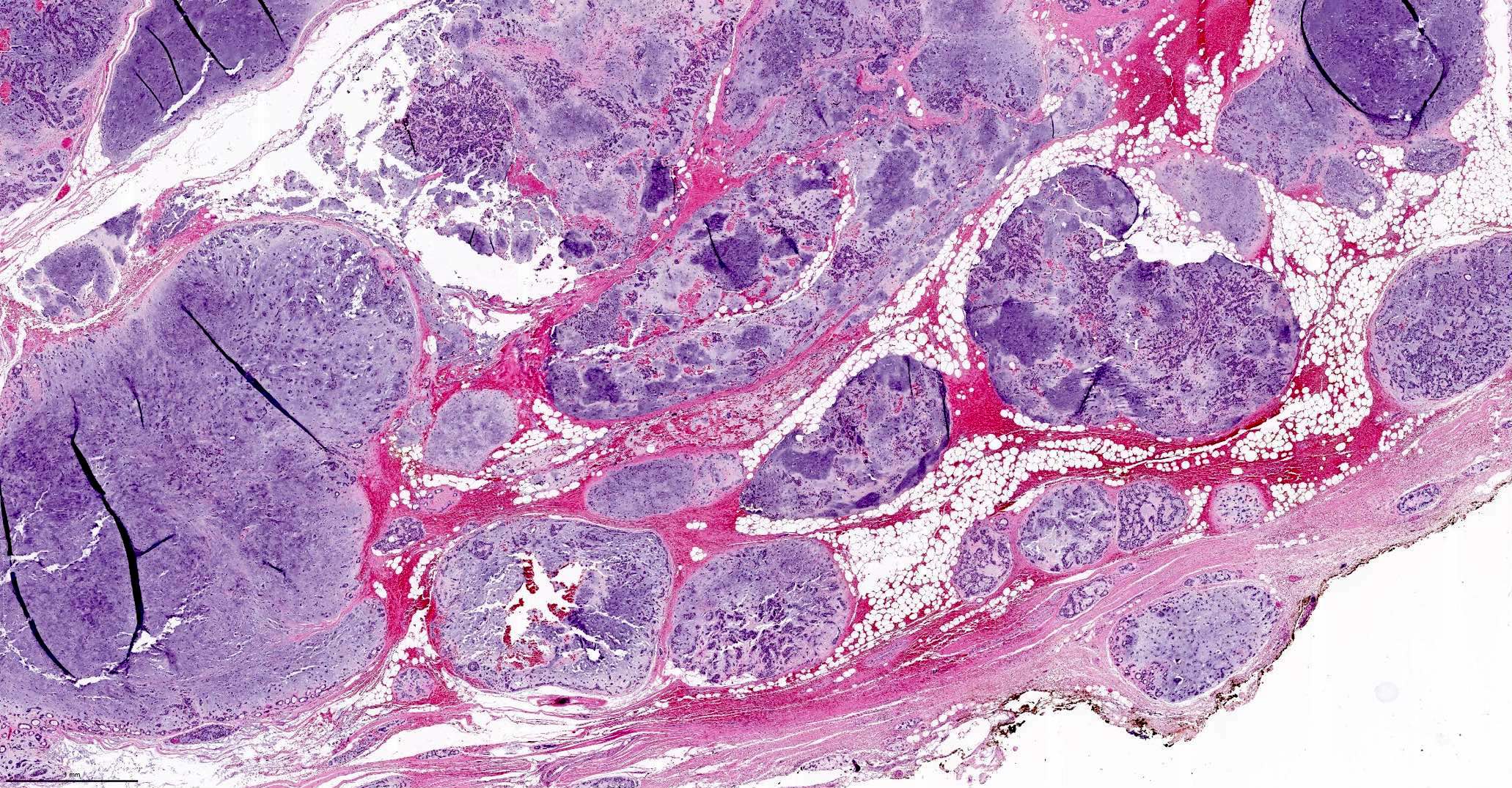
Recurrent pleomorphic adenoma
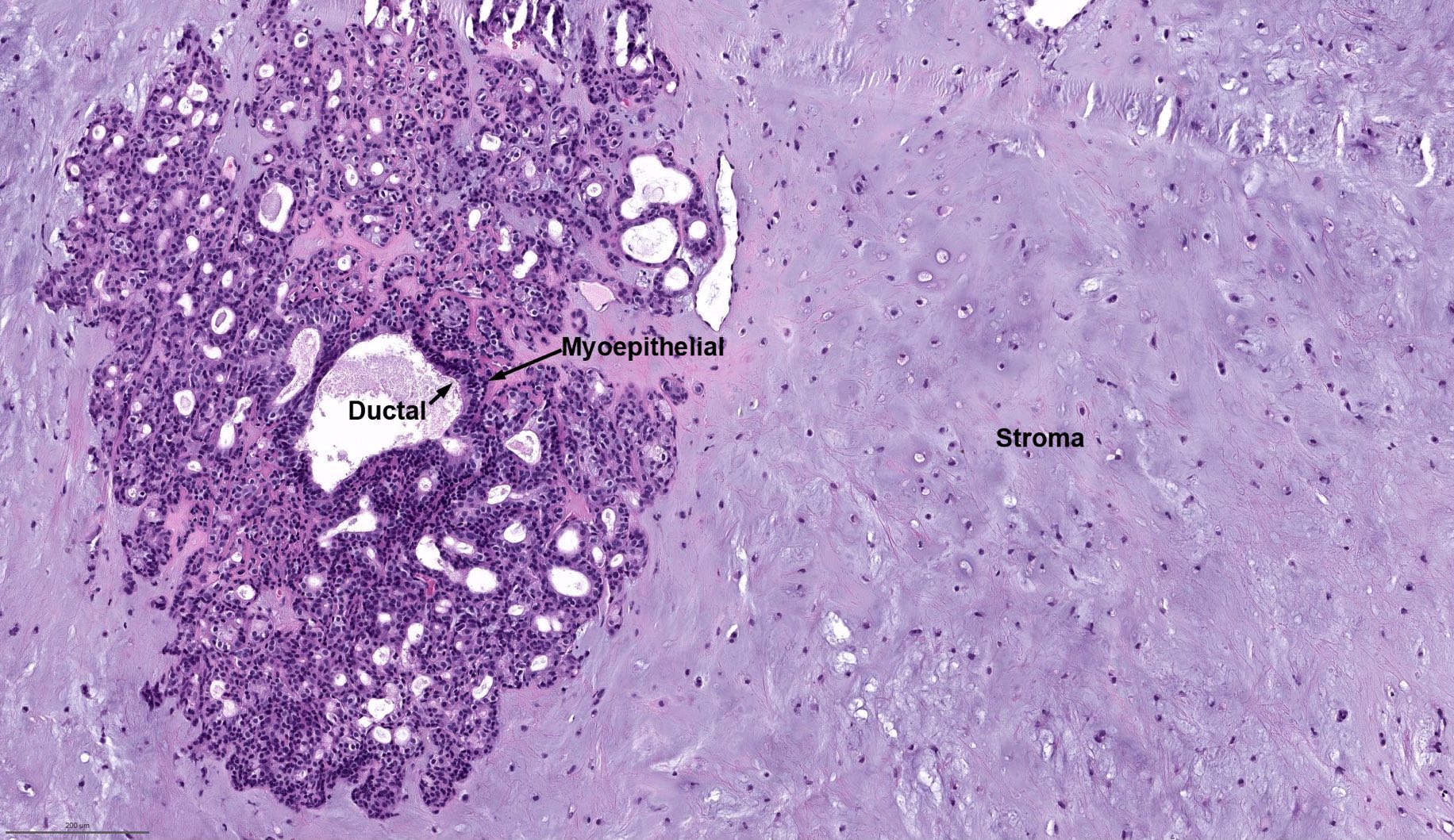
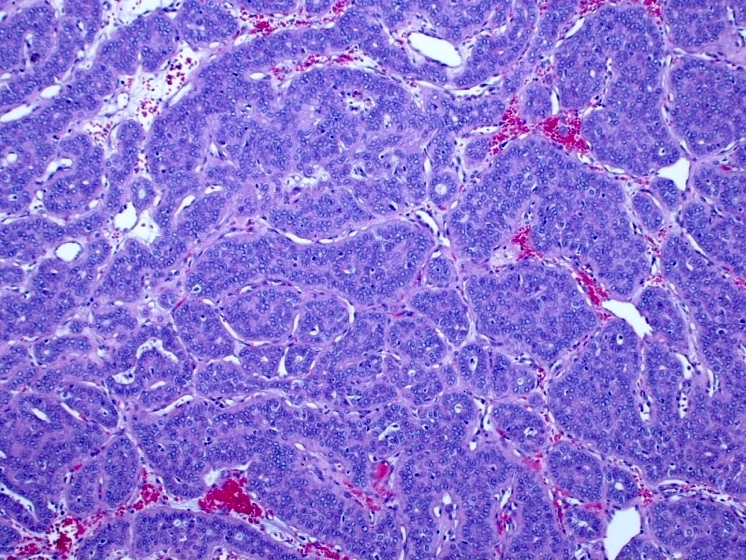
Triphasic tumor
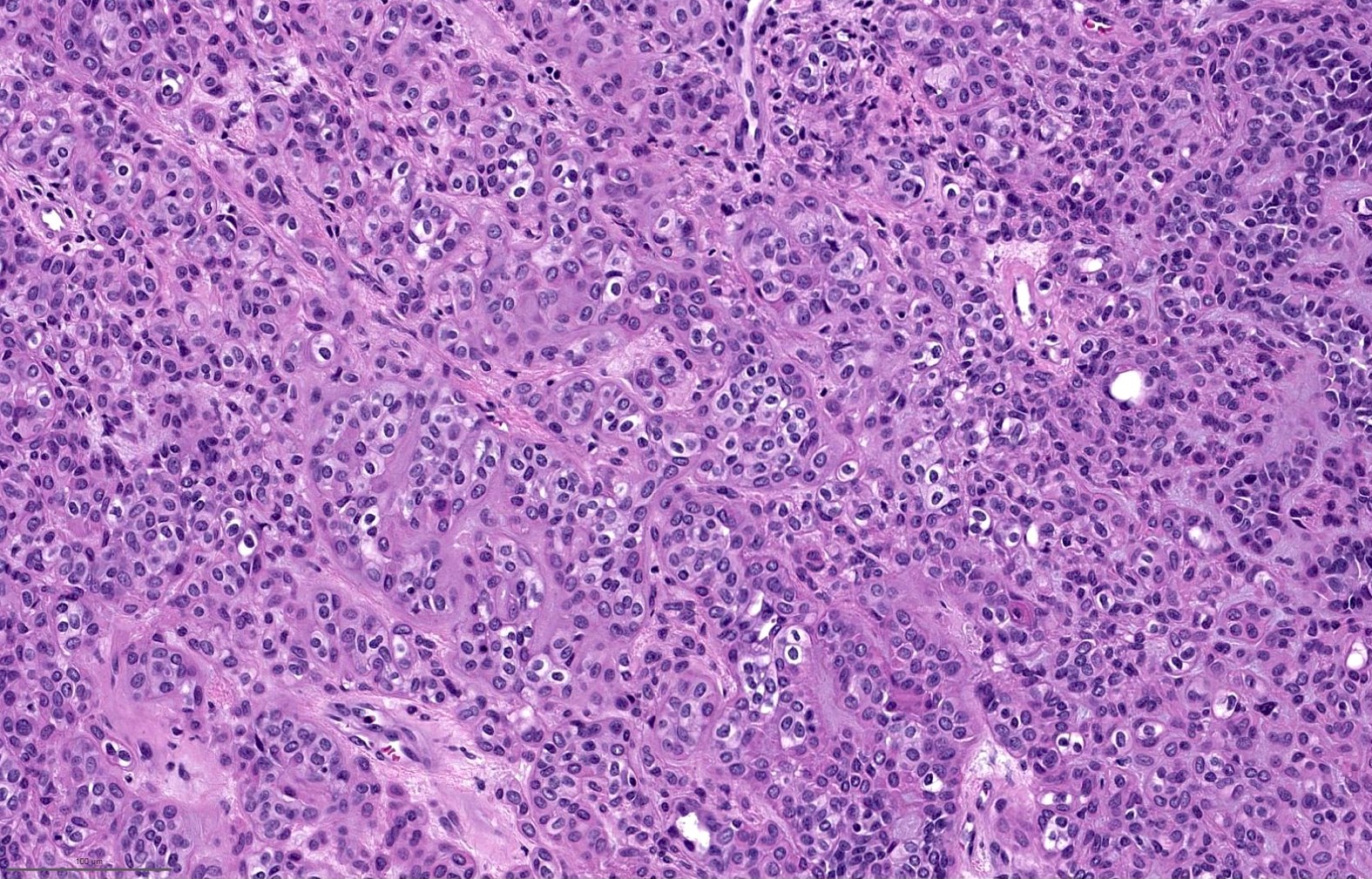
Clear myoepithelial cells

Plasmacytoid myoepithelial cells

Spindle myoepithelial cells

Squamous and mucinous metaplasia

Adipose and osseous metaplasia
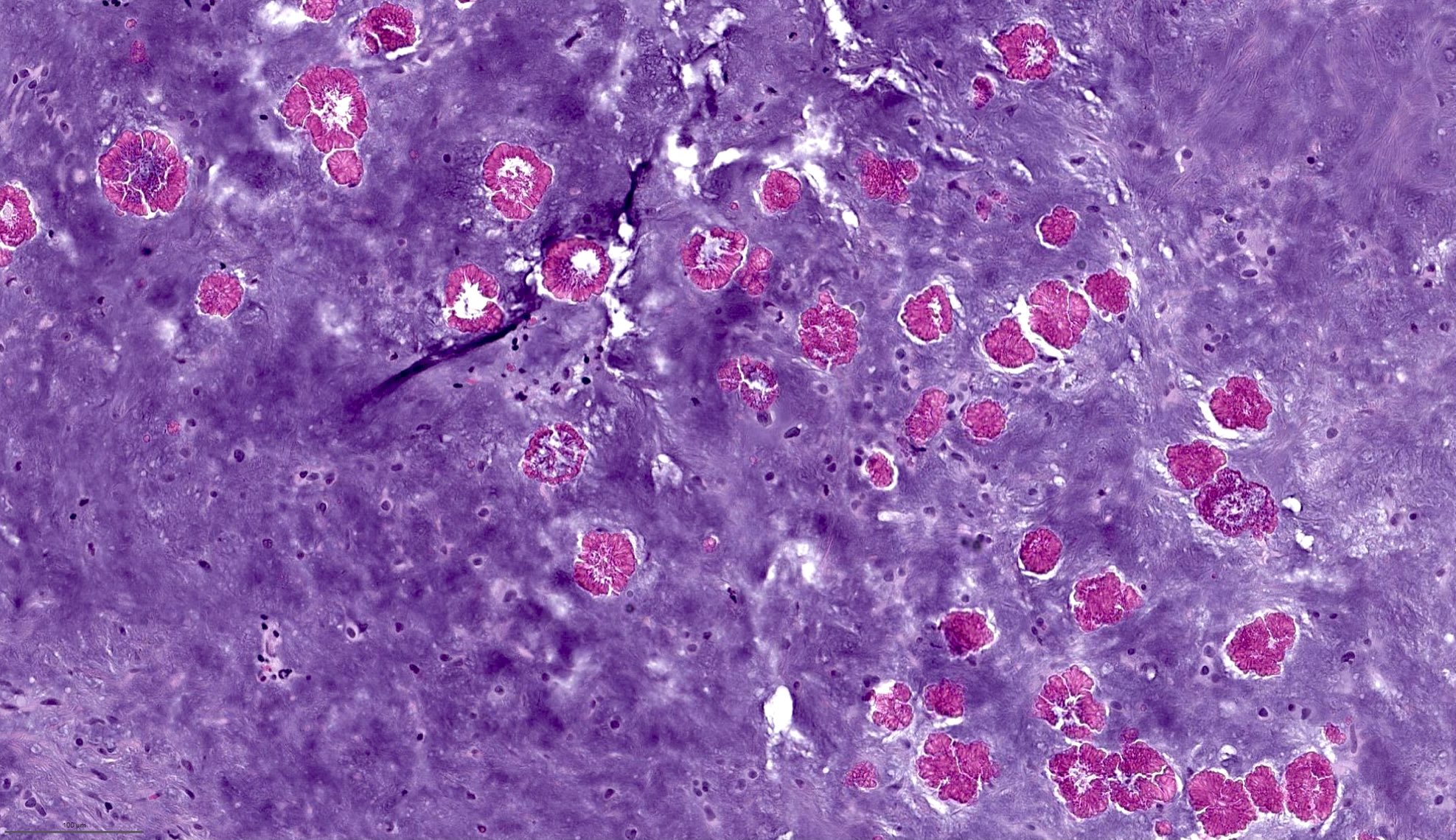
Tyrosine crystals
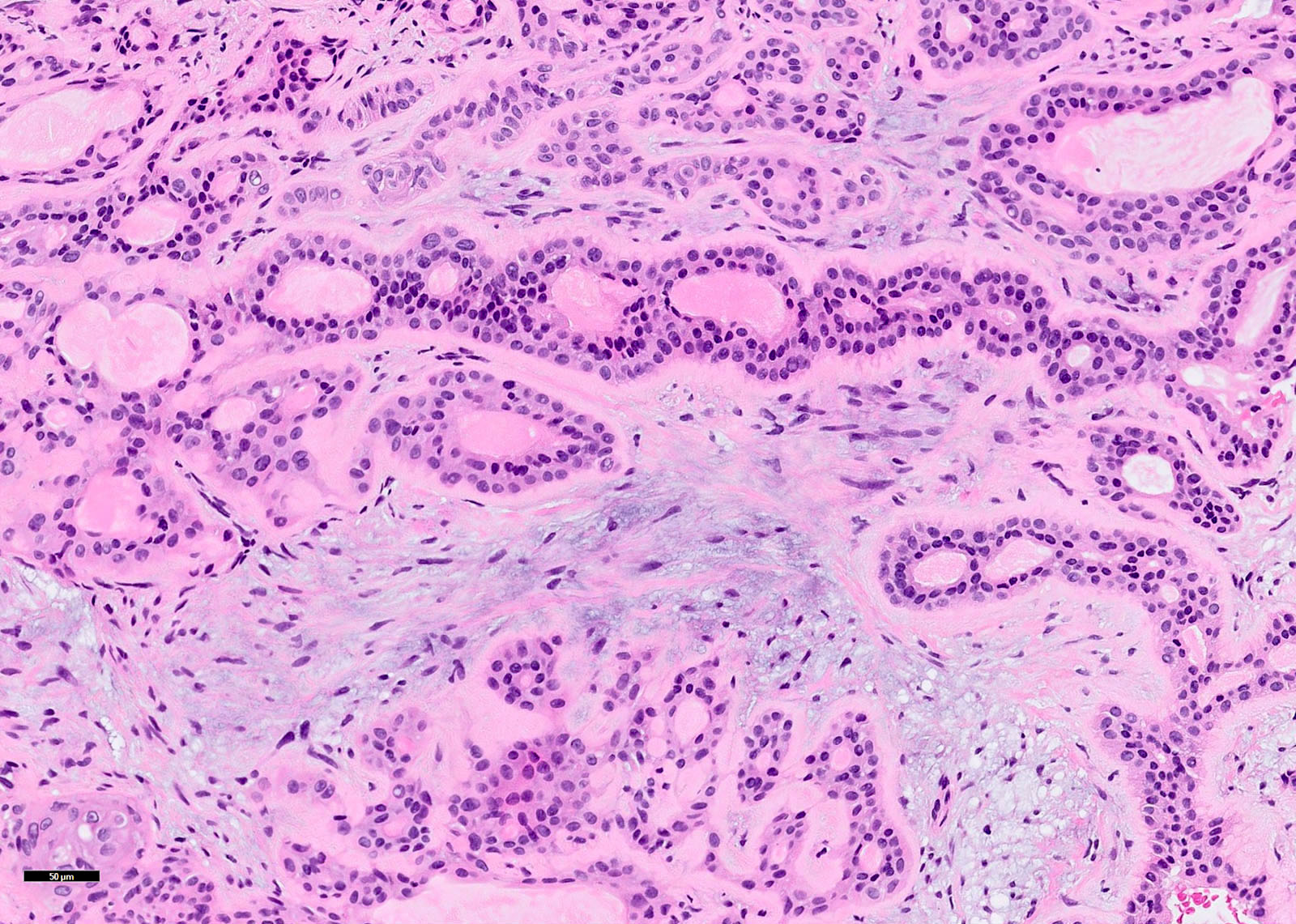
Biphasic population
Case #404
Pleomorphic adenoma
Myoepithelial cells
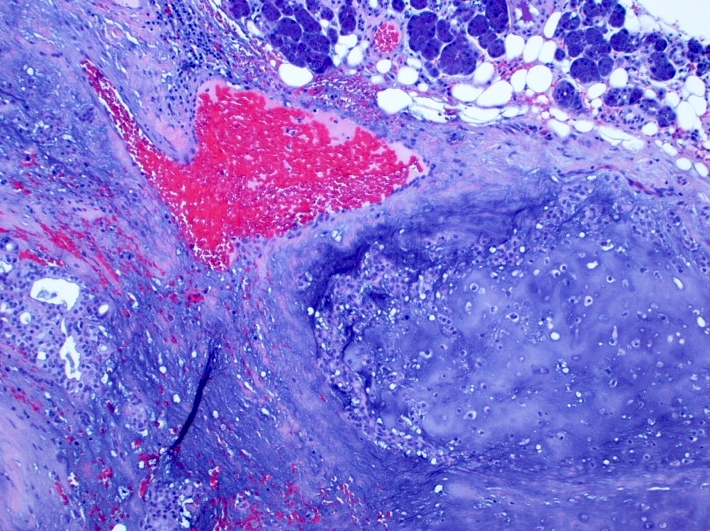
Chondroid stroma
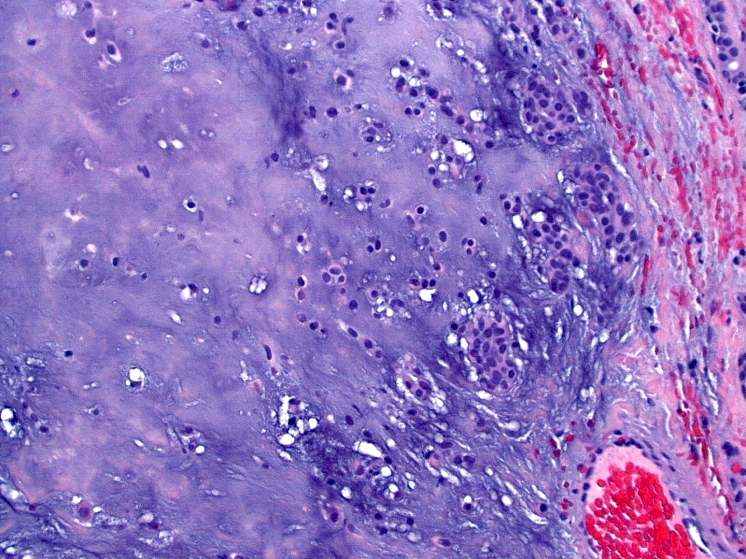
Myoepithelial cells
Contributed by Andrey Bychkov, M.D., Ph.D.

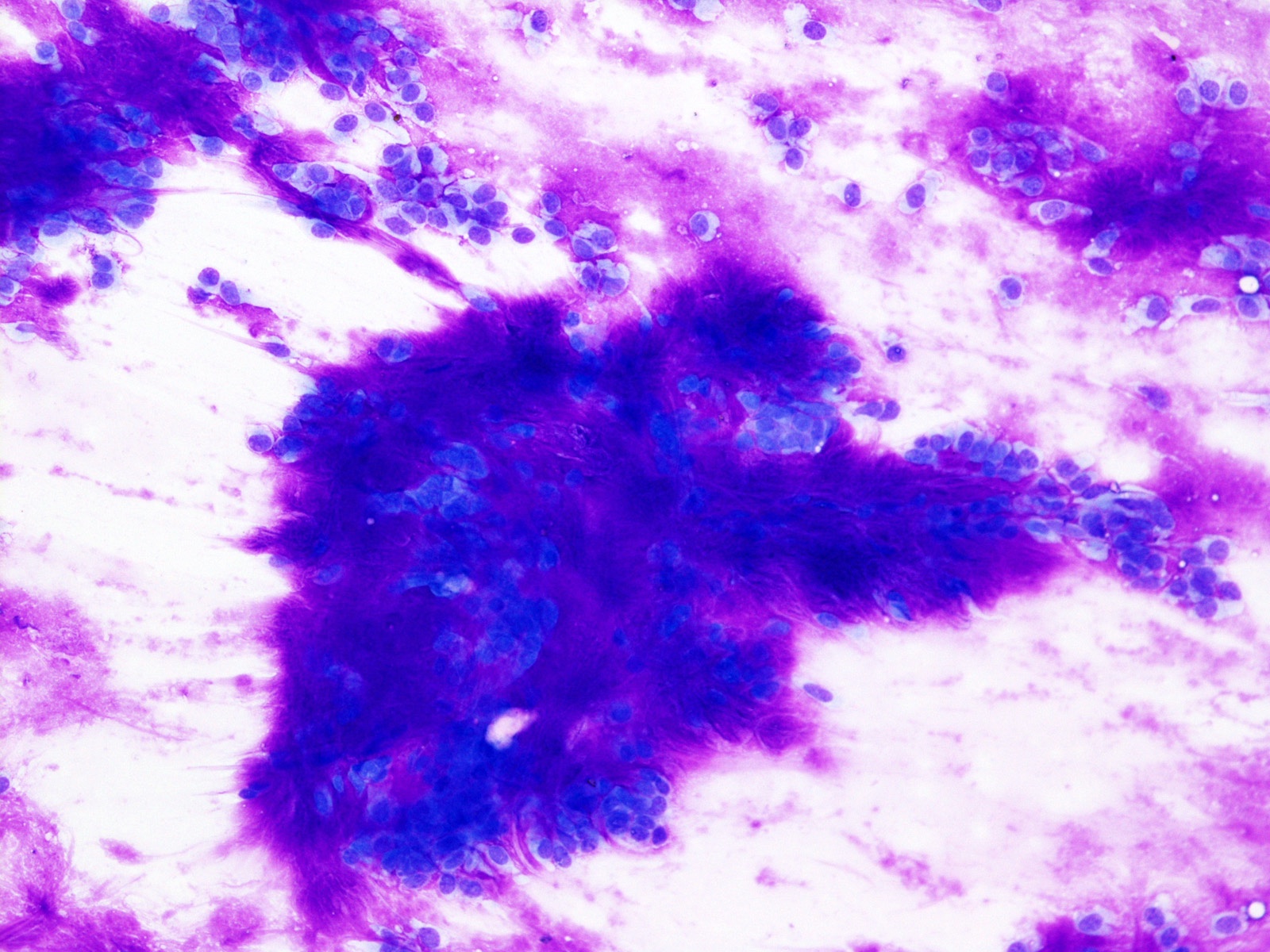
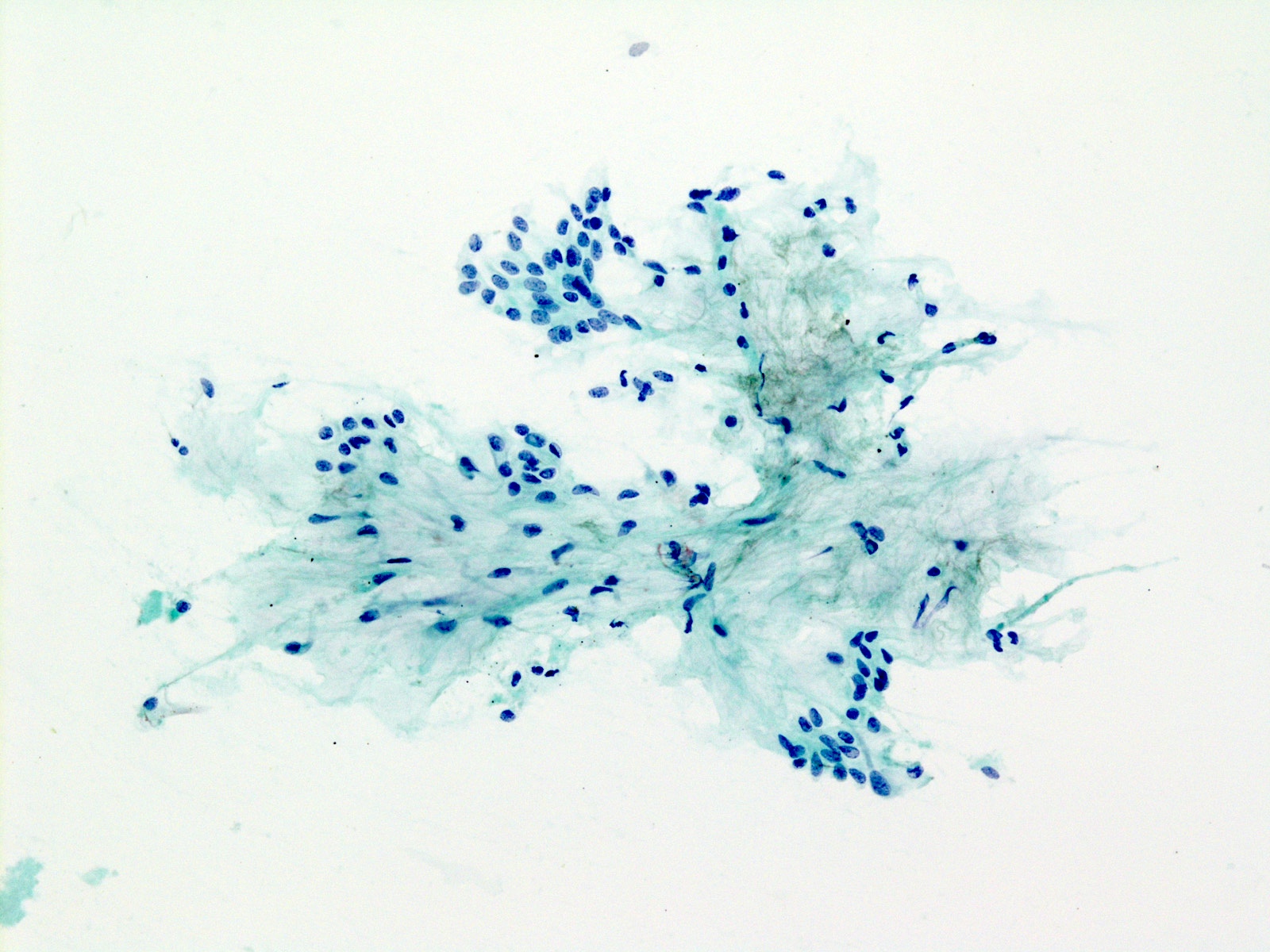
Pleomorphic adenoma
- Matrix containing tumor
- Typical feature is its unique fibrillary stroma
- Mixture of myoepithelial cells, ductal cells and extracellular stroma
- Myoepithelial cells are usually the predominant cell type with various cytomorphology, including round, polygonal, plasmacytoid, spindle, etc.
- Ductal cells show bland cytologic features with organized honeycombing or ductal arrangement
- Extracellular matrix shows characteristic feathery / fibrillary borders and bright magenta color on Romanowsky type stain and gray-green chondromyxoid features on Papanicolaou stain
Contributed by Bin Xu, M.D., Ph.D. and Jen-Fan Hang, M.D.
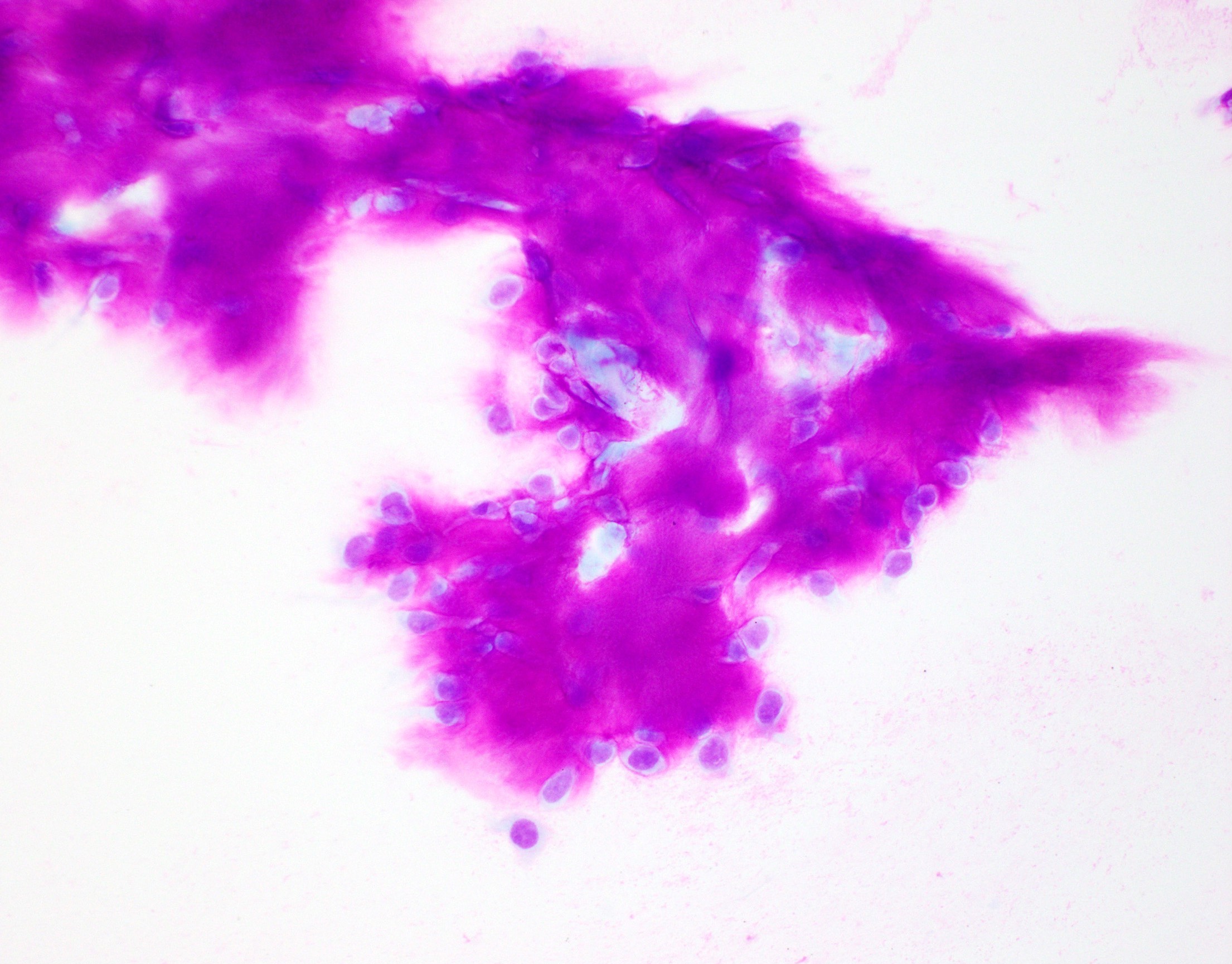
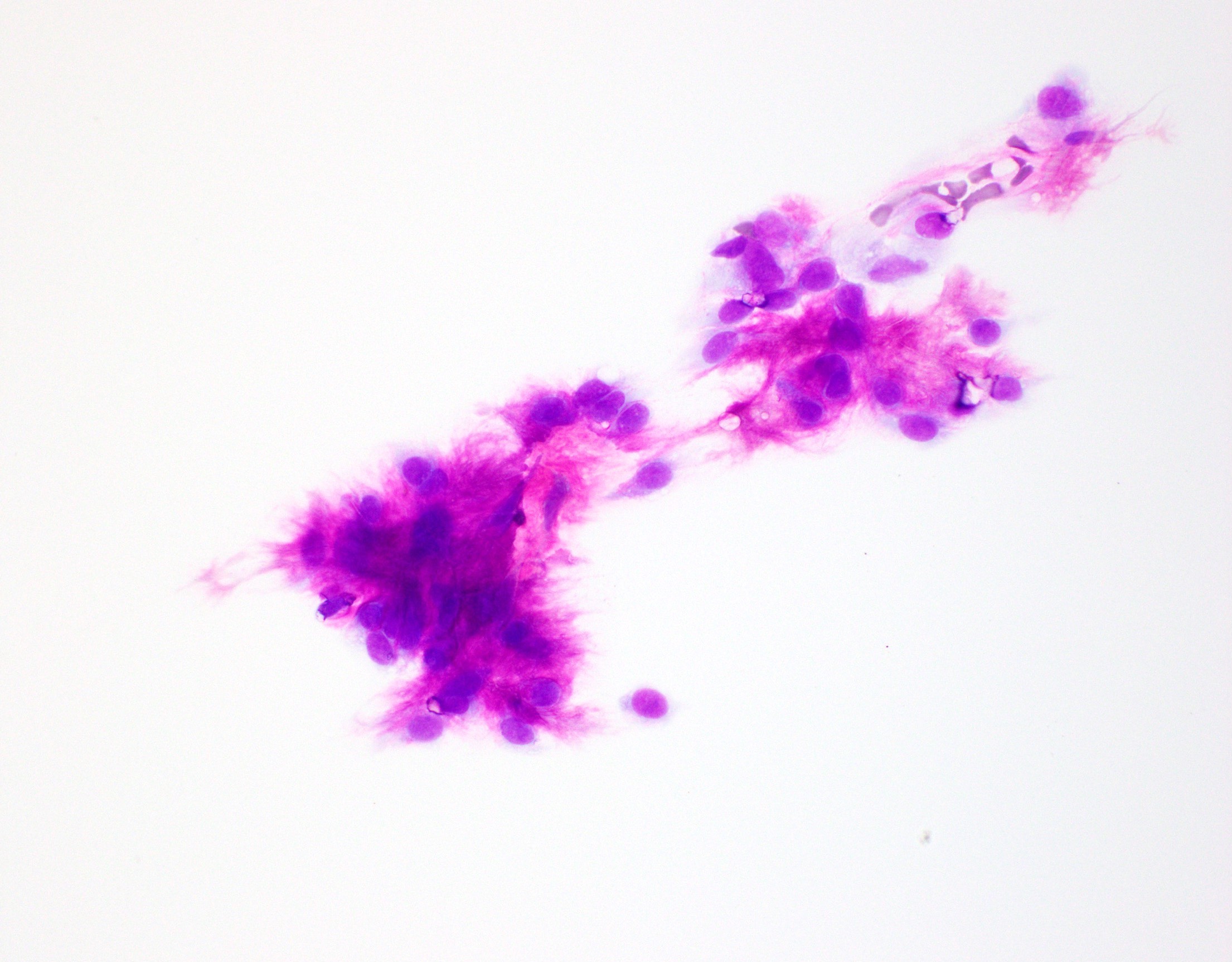
Diff-Quik smear
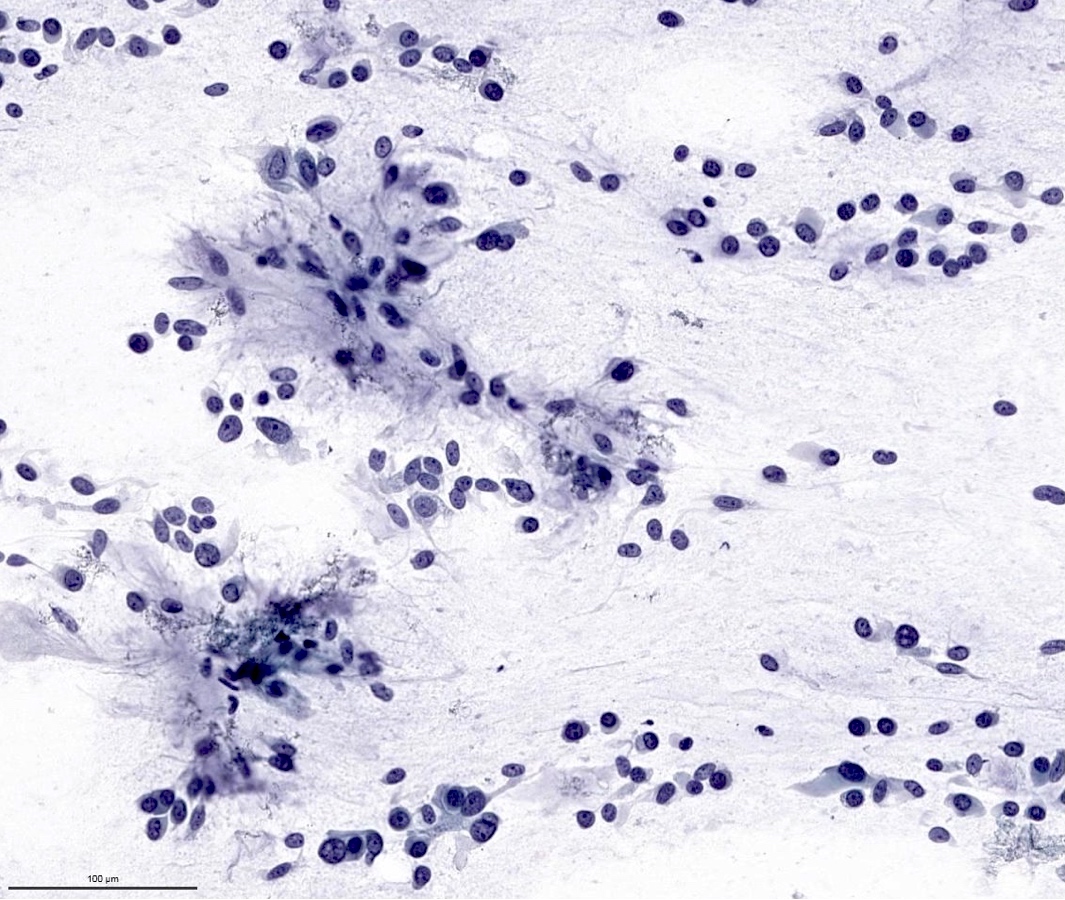
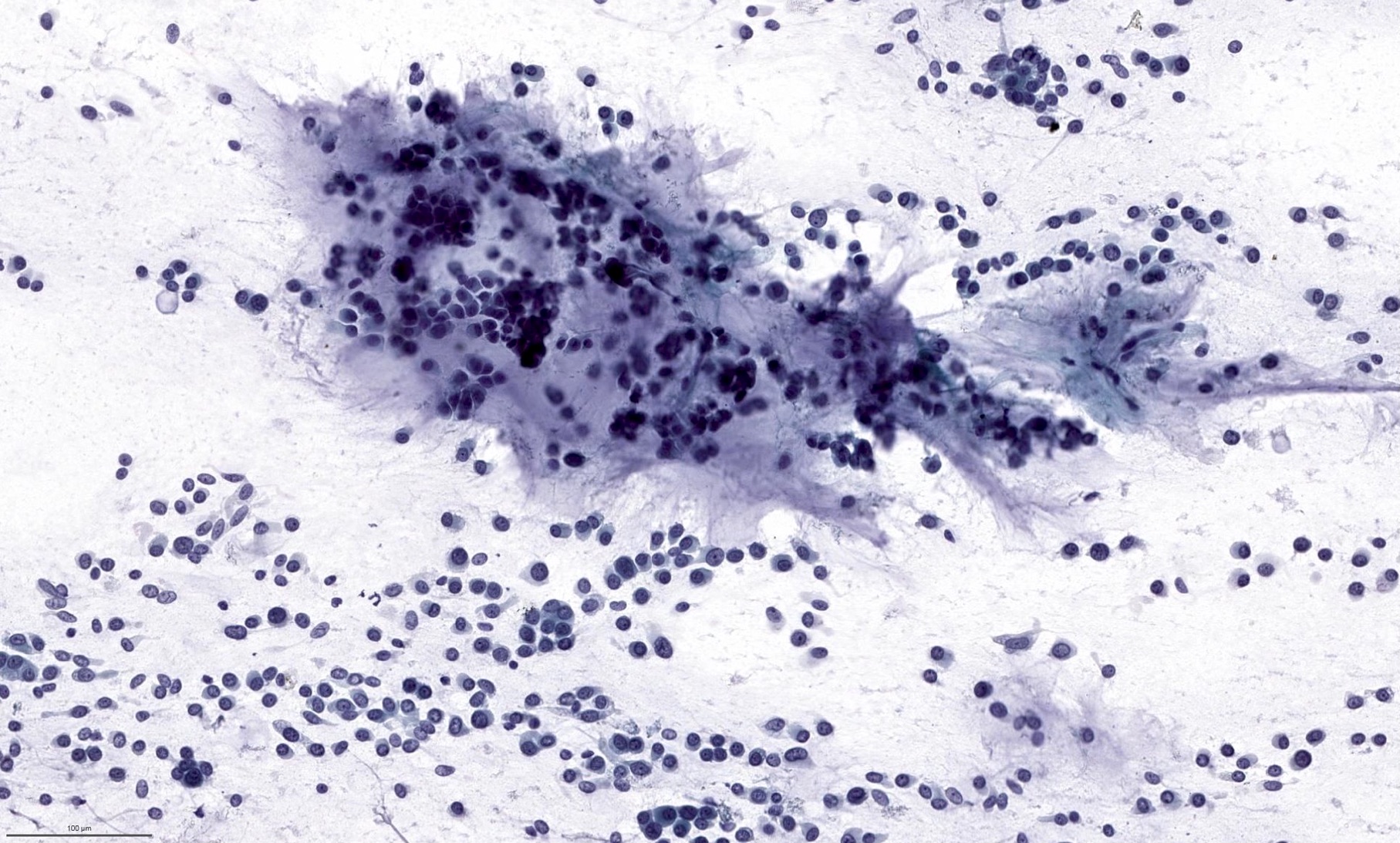
Papanicolaou stain
Fibrillary extracellular matrix
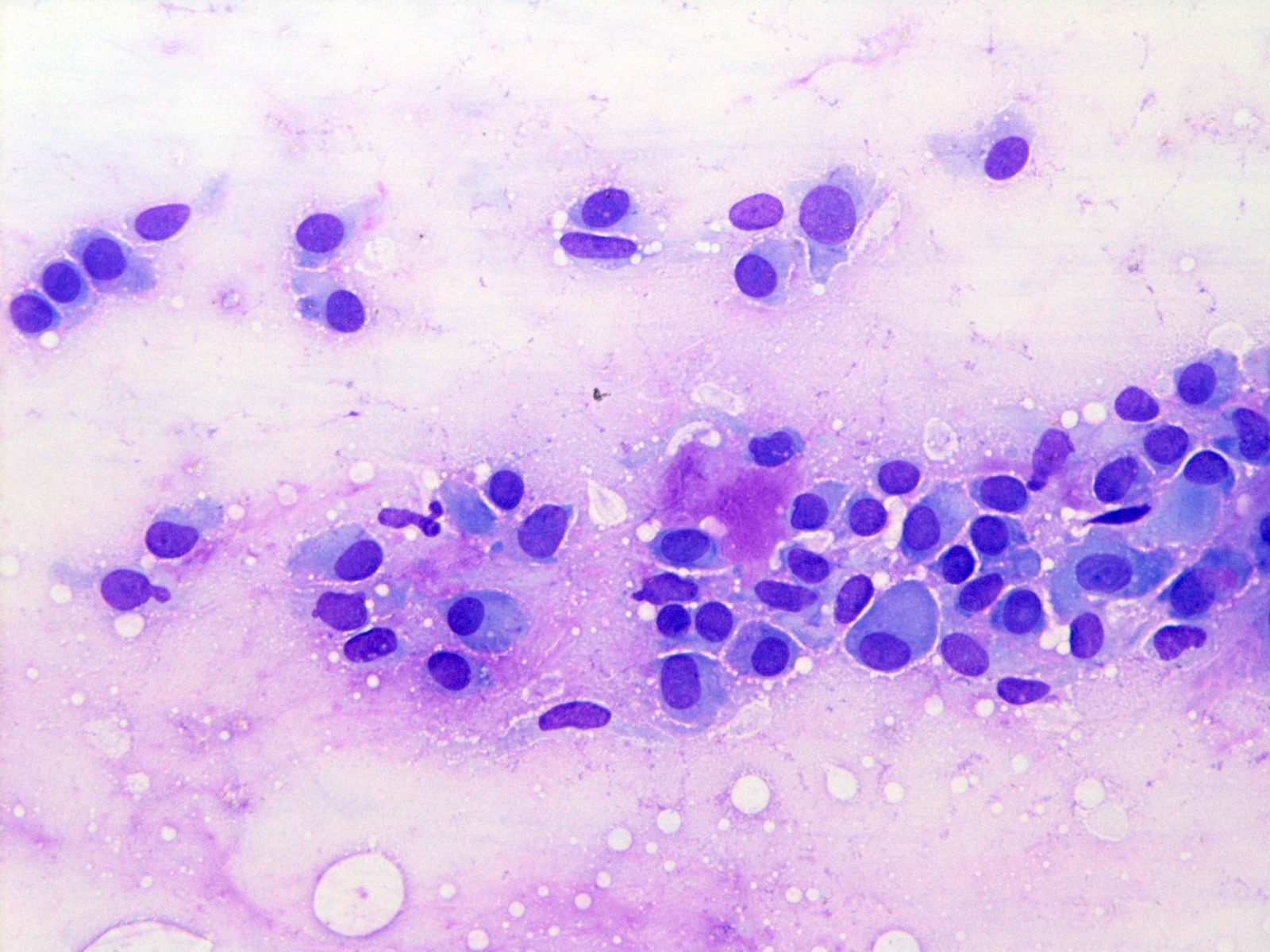
Plasmacytoid
myoepithelial cells
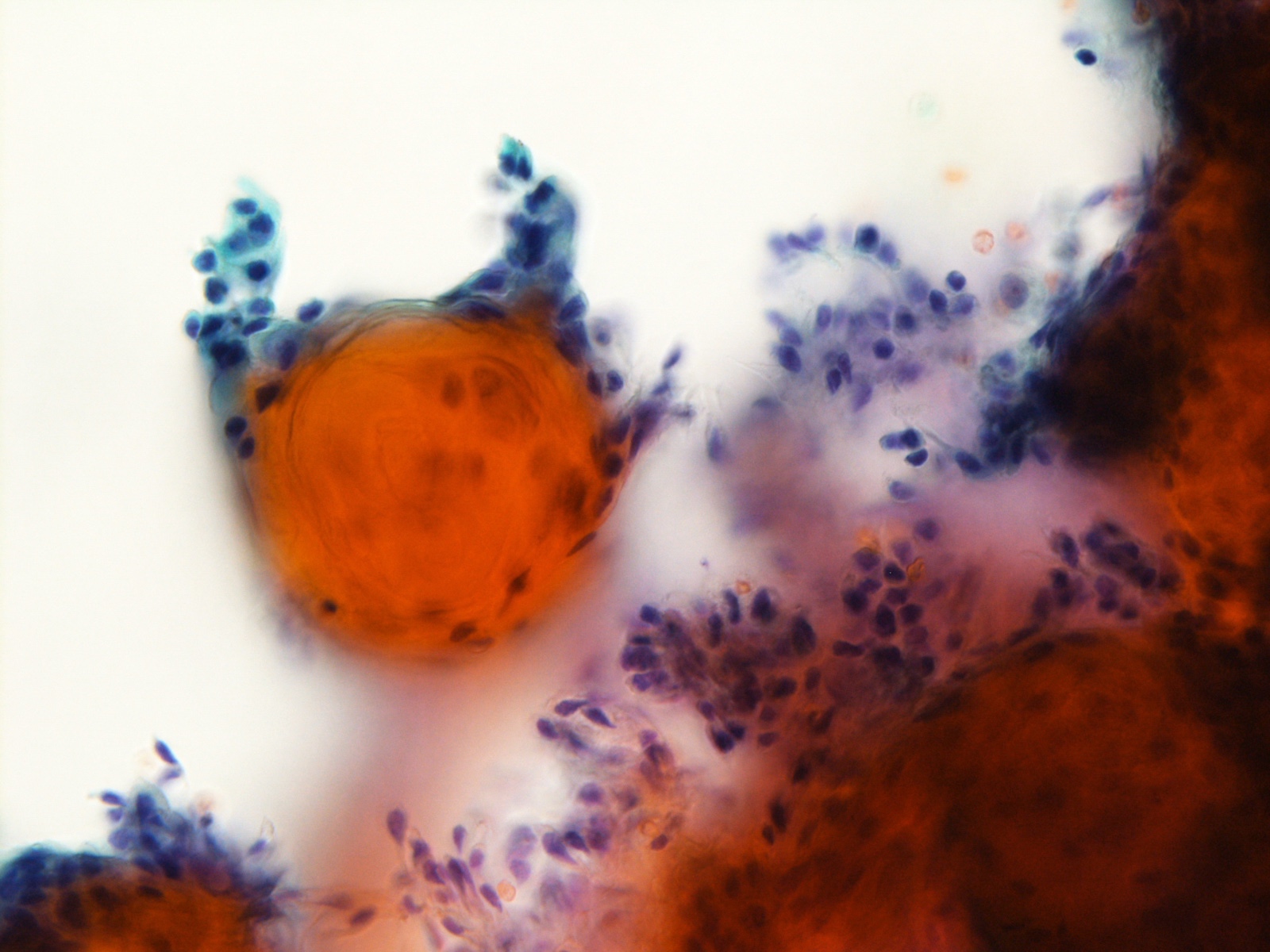
Squamous metaplasia
- Ductal (epithelial) cells are typically positive for cytokeratins (e.g. AE1 / AE3, CAM5.2 and CK7)
- Myoepithelial cells are positive for GFAP, S100, SOX10, actin - alpha smooth muscle, calponin, p40 and p63
- PLAG1 and HMGA2 can be used as surrogate immunohistochemical markers for underlying PLAG1 or HMGA2 fusion (Histopathology 2018;72:285, Histopathology 2017;71:511)
- PLAG1 fusion (chromosome 8q12) or HMGA2 fusion (chromosome 12q14-15) is present in ~70% of pleomorphic adenomas (Oncogene 1998;16:1409, Cancer Res 1997;57:13)
Images hosted on other servers:

FISH for PLAG1
- Parotid, left, parotidectomy:
- Pleomorphic adenoma, 2.0 cm, margins negative for tumor
- Carcinoma ex pleomorphic adenoma (malignant mixed tumor):
- Demonstrates frank evidence of malignancy, e.g. marked nuclear pleomorphism, frank necrosis, invasion beyond pre-existing capsule, perineural or lymphovascular invasion
- Both may contain PLAG1 or HMGA2 fusion (Hum Pathol 2015;46:26)
- Myoepithelioma and myoepithelial carcinoma:
- Contain (nearly) exclusively myoepithelial cells
- Ductal (epithelial) component is scant or absent
- Other salivary gland neoplasms (adenoid cystic carcinoma, polymorphous adenocarcinoma, epithelial myoepithelial carcinoma):
- Pleomorphic adenoma may show various architectural and cytologic features that resemble other salivary tumors
- Identifying areas typical of pleomorphic adenoma with triphasic ductal, myoepithelial and stromal components is helpful to establish the diagnosis
- Squamous cell carcinoma:
- Both may contain squamous epithelium with keratinization and may be difficult to differentiate in small biopsy or cytology material
- Is not triphasic; identification of ductal, epithelial and stromal components typical of pleomorphic adenoma rules out squamous cell carcinoma

A 2.5 cm parotid tumor is resected. The most common molecular alteration of this tumor is
- ETV6-NTRK3 fusion
- MYB-NFIB fusion
- PLAG1 fusion
- PRKD1 mutation
- Carries nearly zero risk of recurrence or malignant transformation
- Characterized by architectural diversity and is composed of one single type of cells
- Is the most common salivary gland neoplasm
- Typically treated with enucleation
Comment Here
Reference: Pleomorphic adenoma
A 45 year old man presented with a 2.8 cm, slow growing mass at left parotid region. He underwent ultrasound guided FNA for evaluation. What is the best diagnosis?
- Basal cell adenoma
- Oncocytoma
- Pleomorphic adenoma
- Warthin tumor
Magenta colored extracellular matrix with feathery / fibrillary borders and intermingled bland myoepithelial cells are characteristic features for a pleomorphic adenoma.
Comment Here
Reference: Pleomorphic adenoma
