
8 October 2009 Case of the Week #159
This email is only sent to subscribers. To subscribe or unsubscribe to this or our other email lists, email subscribePath@gmail.com, indicating subscribe or unsubscribe to [name of email]. Our email lists are:
- Case of the Week - 3 weeks/month
- Pathologist/PhD jobs - biweekly
- Other laboratory jobs - biweekly
- Pathology fellowships - biweekly
- Pathology website news - monthly
- Pathology new books - monthly
- The Detroit College Promise - the scholarship for Detroiters that we sponsor (monthly)
For our DermatologyOutlines.com website, we have these email lists:
- Dermatologist jobs / Practice openings - monthly
- Dermatology fellowships - monthly
- Dermatology website news - monthly
- Dermatology new books - monthly

We offer dermatopathology, head and neck and ophthalmic pathology consultations for pathology organizations worldwide. Visit our website or call (617) 549-1168 to find out how we can help your practice to establish, grow and promote your subspecialty outreach program and effectively compete with reference laboratories.
Our services, supported by custom-designed digital pathology-ready workflow solution, range from second opinion consultations on difficult cases to providing daily subspecialty signout and short-term coverage.
Find out how recognized experts in the field can support your practice at a fraction of the cost of hiring a full-time dermatopathologist.
Website News:
(1) We have almost completed updating the Breast-malignant chapter with our new format that has thumbnails and better formatting.
(2) Visit us at CAP, booth #102 - let us know how we can make our website more useful to you.
To view the images or references in this Case of the Week, you must click on the links in blue. Links in green are to journals with free full text-no registration. You can also access these cases by visiting our Home Page, then click on the Case of the Week button on the left hand side.
Thanks to Alia Albawardi, McGill University Health Center, Montreal, Quebec (Canada) for contributing this case. To contribute a Case of the Week, email khpathology@gmail.com with the clinical history and your diagnosis. Please also email us diagnostic microscopic images (textbook quality) in JPG, GIF or TIFF format (send as attachments, we will shrink if necessary), and include any other images (gross, immunostains, etc.) that may be helpful or interesting. We will write the discussion (unless you want to), list you as the contributor, and send you $35 (US dollars) by check or PayPal for your time after we post the case. Please only send cases with high quality images and a diagnosis that is somewhat unusual (or a case with unusual features).
Case of the Week #159
Clinical History
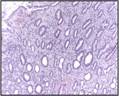
An otherwise healthy 31-year-old woman presented to a hospital in Montreal, Canada with an enlarged stomach lesion by endoscopy. A gastric biopsy was performed.
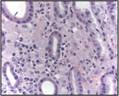
Micro images:

Stains:
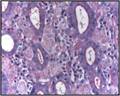

PAS GMS
What is your diagnosis?
Diagnosis:
Histoplasmosis of the stomach
Discussion:
Histoplasma capsulatum is a fungus commonly found throughout the world. In the U.S., it is endemic in the Ohio and Mississippi River valleys (eMedicine), particularly in caves and bat and bird droppings. It is frequently found in the lungs, but can affect any site. In the G.I. tract, it may cause nausea, vomiting, diarrhea, hepatosplenomegaly and possibly perforation and peritonitis. Histoplasma often infects patients with AIDS or other immunosuppressive disorders (Dis Col Rect 1991;34:185) and is often severe or fatal (Microbes Infect 2008;10:973).
Patients may present with mucosal ulceration, hemorrhage or submucosal plaques or nodules, but 25% of patients have no endoscopic findings. Microscopically, there are intracellular spores up to 4 microns with rigid walls and retracted cytoplasm. The organisms have a clear zone around a central blue nucleus, which gives the cell membrane the appearance of a capsule - hence the name of the organism.
Diagnosis is based on histology and culture, as well as rapid antigen / antibody tests of blood, urine or tissue (Curr Opin Infect Dis 2008;21:421). Skin tests confirm exposure, but not infection. A bone marrow biopsy may be helpful in early diagnosis, which is particularly important in disseminated disease (Arch Pathol Lab Med 2006;130:120).
Histoplasmosis of the stomach may clinically resemble a gastric ulcer (Rev Gastroenterol Peru 2003;23:221). The microscopic differential diagnosis includes Candida glabrata, the second most common Candida species in U.S. hospitalized patients. In tissue, it present as yeasts, 3-5 microns in size, which are difficult to visualize on H&E stained slides but can be detected with GMS. Typically no hyphal elements are found (Dermatol Online J 2008;14:15). It can differentiated from Histoplasma based on H&E appearance (histoplasma spores are identifiable) and culture. Other disorders that may appear similar include Leishmania infection, Mycobacterium avium-intracellulare, Whipples disease, Cryptococcosis and malakoplakia.
Treatment for Histoplasmosis is generally a course of antibiotics from 3 to 18 months. Relapses are common.
Additional references: Am Surg 1996;62:369, Am J Med 1985;78:203, Bone Marrow chapter - PathologyOutlines.com, AFIP Atlas of Nontumor Pathology, Fascicle 5, 2007.
Nat Pernick, M.D., President,
and Kara Hamilton, M.S., Assistant Medical Editor
PathologyOutlines.com, Inc.
30100 Telegraph Road, Suite 408
Bingham Farms, Michigan (USA) 48025
Telephone: 248/646-0325
Email: NatPernick@Hotmail.com
Alternate email: NatPernick@gmail.com