
10 August 2005 - Case #16
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Professor D. Y. Cohen, Department of Pathology, Herzliyah Medical Center, Israel.

Case #16
Clinical history:
A 56 year old man had a retroperitoneal mass behind the pancreas and in front of the inferior vena cava. The clinical impression was schwannoma versus sarcoma.
Gross description:
The specimen consisted of 3 irregular fibrofatty fragments, the largest 5 cm and the others being very small. Sectioning revealed a well circumscribed yellow-gray myxoid mass measuring 3 x 2 x 2 cm.
Microscopic images:
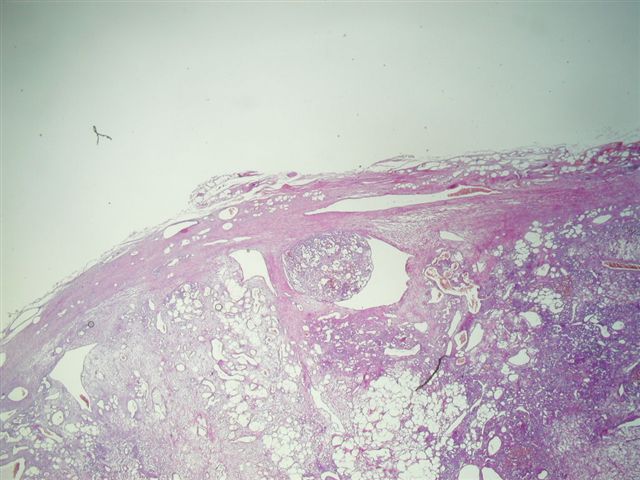
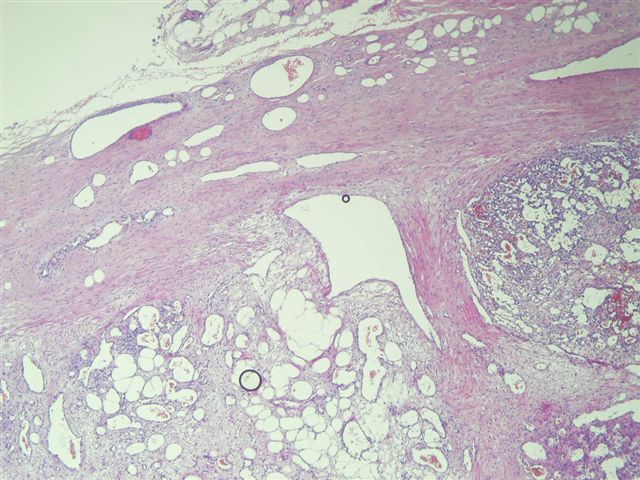
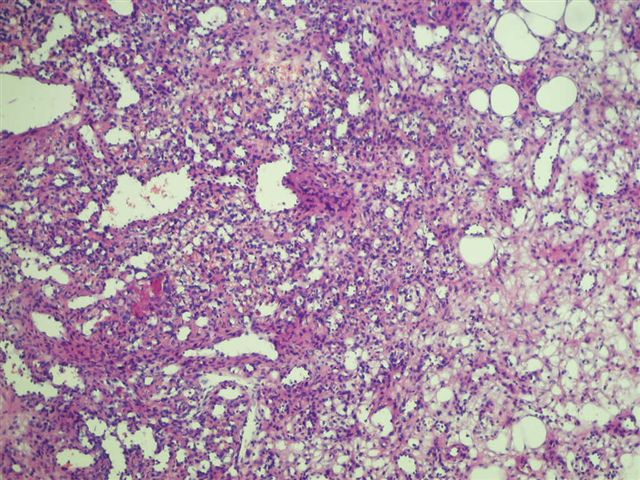
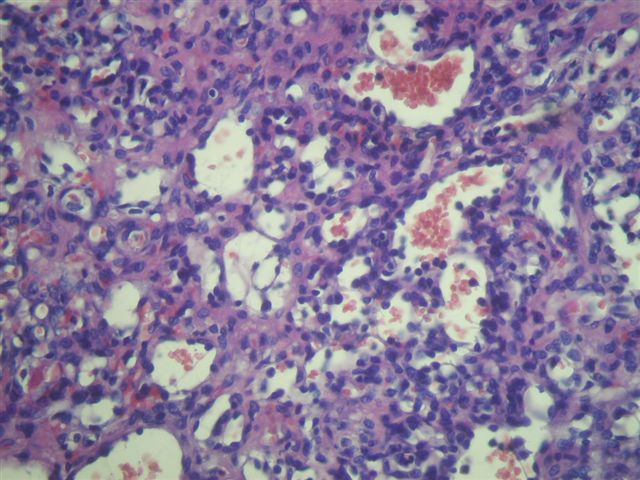
What is your diagnosis?
Diagnosis: Lipomatous hemangiopericytoma
Discussion:
Lipomatous hemangiopericytoma was first described in 1990 by Theunissen et al. and later by Nielsen et al. (Pathologe 1990;11:346, Am J Surg Pathol 1995;19:748). In 1999, it was described in detail by Weiss et al. as a histologically benign hemangiopericytoma containing a variable amount of mature fat as an intrinsic part of the tumor (Am J Surg Pathol 1999;23:1201). These tumors occur primarily in men, with a mean age of 54 years (range: 33 - 74 years), usually in the deep soft tissue of the retroperitoneum or leg. Grossly, they average 10 cm in size, are tan-yellow and have a well circumscribed border. Microscopically, they have typical features of hemangiopericytoma, including round / oval cells, a sinusoidal or staghorn vasculature and often perivascular hyalinization. The tumors contain 25 - 75% admixed fat. There is usually no / low mitotic activity and variable nuclear atypia, ranging from none to moderate. No lipoblasts or atypical hyperchromatic cells are present. These tumors are positive for vimentin and CD99, usually positive for CD34, positive for BCL2 in half of cases and negative for keratin, inhibin, CD117 / KIT, CD31 and desmin. Clinically, they have benign behavior, without recurrence or metastatic spread.
The differential diagnosis includes well differentiated liposarcoma, spindle cell lipoma and solitary fibrous tumor. Well differentiated liposarcoma also occurs in the retroperitoneum and deep soft tissue. It is composed of variably sized cells with large, deep staining nuclei and atypia. In a small biopsy, it may resemble areas of lipomatous hemangiopericytoma with focal atypia. Spindle cell lipoma occurs almost exclusively in the head and neck in subcutaneous tissue. It typically has bland spindle cells in short packets or fascicles between dense collagen bundles in a background of mature adipose tissue. It may have a hemangiopericytoma-like vascular pattern and also has similar immunohistochemistry as lipomatous hemangiopericytoma. Since both have benign behavior, the distinction is not critical. Solitary fibrous tumor has areas resembling classic hemangiopericytoma but also has areas of haphazard growth, distinct fascicles of spindle cells, hyalinized stroma with a cracking artifact and growth of single cells or short chains of cells. Some authors consider lipomatous hemangiopericytoma to represent a fat containing variant of solitary fibrous tumor (Hum Pathol 2000;31:1108).
Reference: Arch Pathol Lab Med 1999;123:941 (case report of thigh tumor with images)
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Professor D. Y. Cohen, Department of Pathology, Herzliyah Medical Center, Israel.
Website news:
(1) This week's case is sponsored by Invitrogen. Invitrogen offers Zymed total system solution for pathology reagents and automation. From antibodies, kits and probes for IHC and CISH to immunostainers for automation, you can be confident that Zymed products will always deliver high quality staining results and offer the cutting edge pathology solutions you need. Note: sponsors do NOT have access to email addresses or other personal information in the possession of PathologyOutlines.com.
Visit and follow our Blog to see recent updates to the website.
(1) This week's case is sponsored by Invitrogen. Invitrogen offers Zymed total system solution for pathology reagents and automation. From antibodies, kits and probes for IHC and CISH to immunostainers for automation, you can be confident that Zymed products will always deliver high quality staining results and offer the cutting edge pathology solutions you need. Note: sponsors do NOT have access to email addresses or other personal information in the possession of PathologyOutlines.com.
Visit and follow our Blog to see recent updates to the website.
Case #16
Clinical history:
A 56 year old man had a retroperitoneal mass behind the pancreas and in front of the inferior vena cava. The clinical impression was schwannoma versus sarcoma.
Gross description:
The specimen consisted of 3 irregular fibrofatty fragments, the largest 5 cm and the others being very small. Sectioning revealed a well circumscribed yellow-gray myxoid mass measuring 3 x 2 x 2 cm.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Lipomatous hemangiopericytoma
Discussion:
Lipomatous hemangiopericytoma was first described in 1990 by Theunissen et al. and later by Nielsen et al. (Pathologe 1990;11:346, Am J Surg Pathol 1995;19:748). In 1999, it was described in detail by Weiss et al. as a histologically benign hemangiopericytoma containing a variable amount of mature fat as an intrinsic part of the tumor (Am J Surg Pathol 1999;23:1201). These tumors occur primarily in men, with a mean age of 54 years (range: 33 - 74 years), usually in the deep soft tissue of the retroperitoneum or leg. Grossly, they average 10 cm in size, are tan-yellow and have a well circumscribed border. Microscopically, they have typical features of hemangiopericytoma, including round / oval cells, a sinusoidal or staghorn vasculature and often perivascular hyalinization. The tumors contain 25 - 75% admixed fat. There is usually no / low mitotic activity and variable nuclear atypia, ranging from none to moderate. No lipoblasts or atypical hyperchromatic cells are present. These tumors are positive for vimentin and CD99, usually positive for CD34, positive for BCL2 in half of cases and negative for keratin, inhibin, CD117 / KIT, CD31 and desmin. Clinically, they have benign behavior, without recurrence or metastatic spread.
The differential diagnosis includes well differentiated liposarcoma, spindle cell lipoma and solitary fibrous tumor. Well differentiated liposarcoma also occurs in the retroperitoneum and deep soft tissue. It is composed of variably sized cells with large, deep staining nuclei and atypia. In a small biopsy, it may resemble areas of lipomatous hemangiopericytoma with focal atypia. Spindle cell lipoma occurs almost exclusively in the head and neck in subcutaneous tissue. It typically has bland spindle cells in short packets or fascicles between dense collagen bundles in a background of mature adipose tissue. It may have a hemangiopericytoma-like vascular pattern and also has similar immunohistochemistry as lipomatous hemangiopericytoma. Since both have benign behavior, the distinction is not critical. Solitary fibrous tumor has areas resembling classic hemangiopericytoma but also has areas of haphazard growth, distinct fascicles of spindle cells, hyalinized stroma with a cracking artifact and growth of single cells or short chains of cells. Some authors consider lipomatous hemangiopericytoma to represent a fat containing variant of solitary fibrous tumor (Hum Pathol 2000;31:1108).
Reference: Arch Pathol Lab Med 1999;123:941 (case report of thigh tumor with images)
