
28 September 2005 - Case #22
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Drs. Elizabeth I. Johnston and Sanjay Logani, Emory University Department of Pathology, Atlanta, Georgia, USA.
Case #22
Clinical history:
A 51 year old man presented to the Emergency Room with fatigue, shortness of breath and dizziness. A complete blood count demonstrated mild anemia and a stool guaiac test was positive for occult blood. Upper and lower gastrointestinal endoscopy showed polypoid gastric masses in the cardia, fundus and antrum. Biopsies revealed the pathology described below. CT scan additionally demonstrated an enlarged lymph node in the gastrohepatic ligament, a 2.5 cm right adrenal mass and an intramucosal lipoma in the jejunum. The patient had a subsequent gastrectomy, esophagojejunostomy and proximal jejunum segmental resection.
Gross description:
The gastrectomy specimen revealed 3 soft, hemorrhagic, polypoid submucosal masses in the cardia, fundus and antrum (figure 1). The masses ranged from 2.3 cm to 9.5 cm in greatest dimension.
Microscopic description:
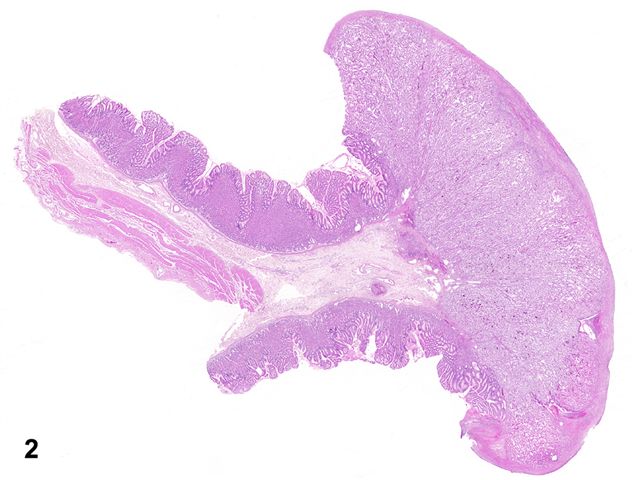
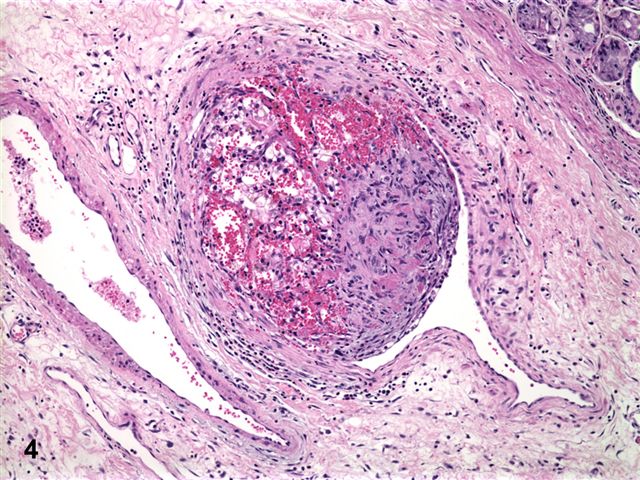
On histopathologic examination, the masses were confined to the mucosa and submucosa (figure 2) and consisted of sheets and nests of large, polygonal, clear cells, with distinct cell borders, medium sized round to irregular nuclei with moderate pleomorphism and prominent nucleoli (figure 3). Vascular invasion was present (figure 4). The surrounding gastric mucosa showed ulceration, reactive changes and chronic gastritis.
Gross and microscopic images:


What is your diagnosis?
Diagnosis: Metastatic renal cell carcinoma, clear cell type
Discussion:
Metastatic tumors to the stomach are rare. The most common primary tumors are melanoma, carcinoma of the lung, breast and esophagus (World J Surg 2004;28:548, Arch Otolaryngol Head Neck Surg 2004;130:892). The tumors generally spread by hematogenous route and result in submucosal masses, as in this case (World J Surg 2004;28:548). Metastatic tumors from breast or uterine primaries classically mimic linitis plastica; however, polypoid and ulcerated tumor masses may also be seen (World J Surg 2004;28:548, Cancer 1990;65:1596). Patients with metastatic tumors to the stomach are often asymptomatic and the lesions may be found on surveillance imaging. Symptomatic patients most frequently present with gastrointestinal bleeding and anemia (World J Surg 2004;28:548).
The most frequent sites of metastasis of renal cell carcinoma (RCC) include the lungs, bones, brain and liver (Arch Otolaryngol Head Neck Surg 2004;130:892, J Clin Gastroenterol 1998;26:153). RCC has also been reported to metastasize to the small intestine, pancreas and thyroid (Kaohsiung J Med Sci 2004;20:137, Arch Otolaryngol Head Neck Surg 2004;130:892, J La State Med Soc 2004;156:40). Although RCC has a propensity to metastasize to unusual sites, cases of metastatic RCC to the stomach are very rare. Previous cases of metastatic renal cell carcinoma to the stomach have been reported and have presented as discrete and ulcerated gastric masses (J Clin Gastroenterol 1998;26:153, Urology 2001;57:168, Gut 1995;37:835).
The differential diagnosis of clear cell tumors in the stomach, especially in small endoscopic biopsies, can be challenging. Diagnoses to consider include paraganglioma, melanoma, clear cell carcinoid, clear cell carcinoma (metastatic or primary gastric adenocarcinoma with clear cell differentiation) and rarely alveolar soft part sarcoma. A panel of immunohistochemical stains may differentiate between the various entities in small biopsy specimens. Paraganglioma is almost always positive for neuroendocrine markers such as neuron specific enolase, synaptophysin and chromogranin and S100 protein highlights the sustentacular cells. Cytokeratins are generally negative, in contrast to clear cell carcinoid tumors, which express neuroendocrine markers (Weiss: Enzinger and Weiss's Soft Tissue Tumors, 4th Edition, 2001). Melanoma is one of the most common metastatic tumors to the stomach and this diagnosis can be easily confirmed by positive expression for S100, as well as the more specific markers such as HMB45 and MelanA. The rare alveolar soft part sarcoma may be S100 positive; a more specific marker is the nuclear expression of TFE3 (Weiss: Enzinger and Weiss's Soft Tissue Tumors, 4th Edition, 2001, Immunohistochemistry vade mecum [Accessed 26 October 2023]). Finally, metastatic clear cell renal cell carcinoma is usually positive for epithelial membrane antigen (EMA), RCC antigen and CD10 (Weiss: Enzinger and Weiss's Soft Tissue Tumors, 4th Edition, 2001, Immunohistochemistry vade mecum [Accessed 26 October 2023]).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Drs. Elizabeth I. Johnston and Sanjay Logani, Emory University Department of Pathology, Atlanta, Georgia, USA.
Case #22
Clinical history:
A 51 year old man presented to the Emergency Room with fatigue, shortness of breath and dizziness. A complete blood count demonstrated mild anemia and a stool guaiac test was positive for occult blood. Upper and lower gastrointestinal endoscopy showed polypoid gastric masses in the cardia, fundus and antrum. Biopsies revealed the pathology described below. CT scan additionally demonstrated an enlarged lymph node in the gastrohepatic ligament, a 2.5 cm right adrenal mass and an intramucosal lipoma in the jejunum. The patient had a subsequent gastrectomy, esophagojejunostomy and proximal jejunum segmental resection.
Gross description:
The gastrectomy specimen revealed 3 soft, hemorrhagic, polypoid submucosal masses in the cardia, fundus and antrum (figure 1). The masses ranged from 2.3 cm to 9.5 cm in greatest dimension.
Microscopic description:
On histopathologic examination, the masses were confined to the mucosa and submucosa (figure 2) and consisted of sheets and nests of large, polygonal, clear cells, with distinct cell borders, medium sized round to irregular nuclei with moderate pleomorphism and prominent nucleoli (figure 3). Vascular invasion was present (figure 4). The surrounding gastric mucosa showed ulceration, reactive changes and chronic gastritis.
Gross and microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Metastatic renal cell carcinoma, clear cell type
Discussion:
Metastatic tumors to the stomach are rare. The most common primary tumors are melanoma, carcinoma of the lung, breast and esophagus (World J Surg 2004;28:548, Arch Otolaryngol Head Neck Surg 2004;130:892). The tumors generally spread by hematogenous route and result in submucosal masses, as in this case (World J Surg 2004;28:548). Metastatic tumors from breast or uterine primaries classically mimic linitis plastica; however, polypoid and ulcerated tumor masses may also be seen (World J Surg 2004;28:548, Cancer 1990;65:1596). Patients with metastatic tumors to the stomach are often asymptomatic and the lesions may be found on surveillance imaging. Symptomatic patients most frequently present with gastrointestinal bleeding and anemia (World J Surg 2004;28:548).
The most frequent sites of metastasis of renal cell carcinoma (RCC) include the lungs, bones, brain and liver (Arch Otolaryngol Head Neck Surg 2004;130:892, J Clin Gastroenterol 1998;26:153). RCC has also been reported to metastasize to the small intestine, pancreas and thyroid (Kaohsiung J Med Sci 2004;20:137, Arch Otolaryngol Head Neck Surg 2004;130:892, J La State Med Soc 2004;156:40). Although RCC has a propensity to metastasize to unusual sites, cases of metastatic RCC to the stomach are very rare. Previous cases of metastatic renal cell carcinoma to the stomach have been reported and have presented as discrete and ulcerated gastric masses (J Clin Gastroenterol 1998;26:153, Urology 2001;57:168, Gut 1995;37:835).
The differential diagnosis of clear cell tumors in the stomach, especially in small endoscopic biopsies, can be challenging. Diagnoses to consider include paraganglioma, melanoma, clear cell carcinoid, clear cell carcinoma (metastatic or primary gastric adenocarcinoma with clear cell differentiation) and rarely alveolar soft part sarcoma. A panel of immunohistochemical stains may differentiate between the various entities in small biopsy specimens. Paraganglioma is almost always positive for neuroendocrine markers such as neuron specific enolase, synaptophysin and chromogranin and S100 protein highlights the sustentacular cells. Cytokeratins are generally negative, in contrast to clear cell carcinoid tumors, which express neuroendocrine markers (Weiss: Enzinger and Weiss's Soft Tissue Tumors, 4th Edition, 2001). Melanoma is one of the most common metastatic tumors to the stomach and this diagnosis can be easily confirmed by positive expression for S100, as well as the more specific markers such as HMB45 and MelanA. The rare alveolar soft part sarcoma may be S100 positive; a more specific marker is the nuclear expression of TFE3 (Weiss: Enzinger and Weiss's Soft Tissue Tumors, 4th Edition, 2001, Immunohistochemistry vade mecum [Accessed 26 October 2023]). Finally, metastatic clear cell renal cell carcinoma is usually positive for epithelial membrane antigen (EMA), RCC antigen and CD10 (Weiss: Enzinger and Weiss's Soft Tissue Tumors, 4th Edition, 2001, Immunohistochemistry vade mecum [Accessed 26 October 2023]).
