
30 November 2005 - Case #29
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Jason Hicks, Harris Methodist H.E.B., Bedford, Texas, USA.
Case #29
Clinical history:
A 33 year old woman had a 2.4 cm soft tissue mass of the cheek. Her past medical history was remarkable only for a remote mitral valve replacement. The mass had been present for a while but recently grew in size prompting a visit to her doctor.
Gross description:
The specimen contained a 2.4 cm, subcutaneous, rubbery, pink-tan mass with an elliptical strip of pale overlying skin.
Immunohistochemistry:
CD34 positive; negative for factor XIIIa and CD68
Microscopic images:

What is your diagnosis?
Diagnosis: Solitary fibrous tumor of the dermis
Discussion:
Solitary fibrous tumor was originally reported in the pleura but has since been reported at almost all organ and body sites. In the skin, they are well circumscribed dermal lesions, composed of spindle cells in a patternless pattern of short and narrow fascicles. There are intermixed bundles of thick collagen and numerous blood vessels, which may have a hemangiopericytoma-like, staghorn pattern. Variable features include hypocellular and hypercellular areas and myxoid areas. Tumor cells are immunoreactive for CD34, vimentin and BCL2 and negative for factor XIIIa, CD68, neural, smooth muscle and epithelial markers. Excision is curative, as these tumors almost always have benign behavior.
The differential diagnosis includes other spindled tumors of the skin. One uncommon mimic is a CD34 reactive dermal dendrocytoma, which is also a benign, well circumscribed tumor composed of CD34+ spindle cells and collagen fibers, with a loose fascicular pattern. However, the collagen fibers are thin, not thick and the background is invariably myxoid. In addition, its tumor cells are CD68+, in contrast to CD68- tumor cells in solitary fibrous tumor (Am J Dermatopathol 2002;24:50).
Reference: Am J Dermatopathol 1999;21:213
Case repors: 30 month old girl with aggressive scalp lesion (Pediatr Dev Pathol 2001;4:267), 37 year old woman with scalp lesion (Am J Dermatopathol 1997;19:515), 56 year old woman with nodule in cheek (J Am Acad Dermatol 2002;46:S37)
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Jason Hicks, Harris Methodist H.E.B., Bedford, Texas, USA.
Case #29
Clinical history:
A 33 year old woman had a 2.4 cm soft tissue mass of the cheek. Her past medical history was remarkable only for a remote mitral valve replacement. The mass had been present for a while but recently grew in size prompting a visit to her doctor.
Gross description:
The specimen contained a 2.4 cm, subcutaneous, rubbery, pink-tan mass with an elliptical strip of pale overlying skin.
Immunohistochemistry:
CD34 positive; negative for factor XIIIa and CD68
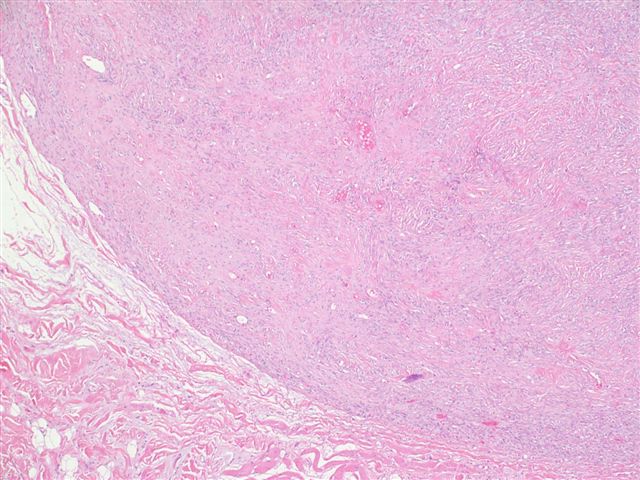
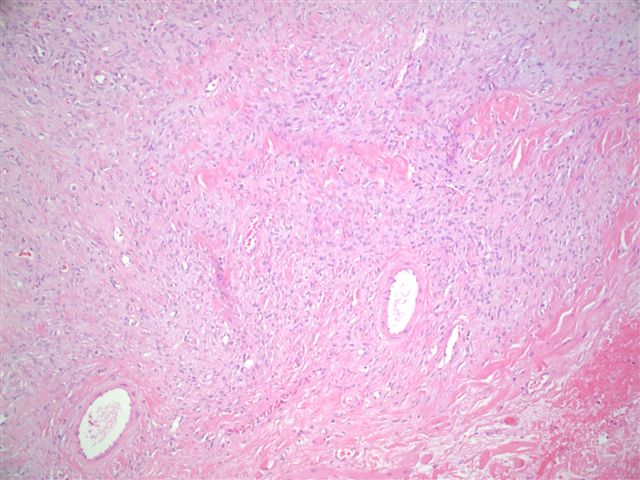
Microscopic images:
Low power #1
#2
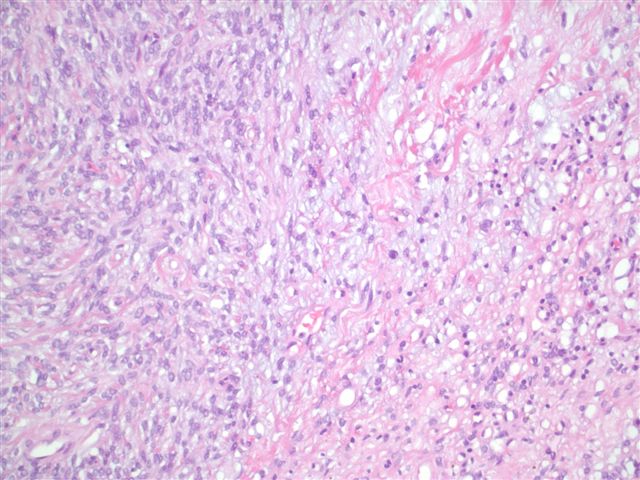
#3
High power
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Solitary fibrous tumor of the dermis
Discussion:
Solitary fibrous tumor was originally reported in the pleura but has since been reported at almost all organ and body sites. In the skin, they are well circumscribed dermal lesions, composed of spindle cells in a patternless pattern of short and narrow fascicles. There are intermixed bundles of thick collagen and numerous blood vessels, which may have a hemangiopericytoma-like, staghorn pattern. Variable features include hypocellular and hypercellular areas and myxoid areas. Tumor cells are immunoreactive for CD34, vimentin and BCL2 and negative for factor XIIIa, CD68, neural, smooth muscle and epithelial markers. Excision is curative, as these tumors almost always have benign behavior.
The differential diagnosis includes other spindled tumors of the skin. One uncommon mimic is a CD34 reactive dermal dendrocytoma, which is also a benign, well circumscribed tumor composed of CD34+ spindle cells and collagen fibers, with a loose fascicular pattern. However, the collagen fibers are thin, not thick and the background is invariably myxoid. In addition, its tumor cells are CD68+, in contrast to CD68- tumor cells in solitary fibrous tumor (Am J Dermatopathol 2002;24:50).
Reference: Am J Dermatopathol 1999;21:213
Case repors: 30 month old girl with aggressive scalp lesion (Pediatr Dev Pathol 2001;4:267), 37 year old woman with scalp lesion (Am J Dermatopathol 1997;19:515), 56 year old woman with nodule in cheek (J Am Acad Dermatol 2002;46:S37)
