
4 January 2006 - Case #32
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Khaldoon Aljerian, University of Toronto, Ontario, Canada.
Case #32
Clinical history:
A 44 year old woman with biliary colic had an ultrasound that revealed gallstones and an incidental 3 cm solid mass in the left kidney, which was confirmed by CT and MRI. A complete nephrectomy was performed due to the central location of the mass and its proximity to the major renal vessels.
The mass was 2.5 cm, solid, well circumscribed and brown-red. There was no gross necrosis, hemorrhage or renal venous involvement. The remaining kidney was unremarkable.
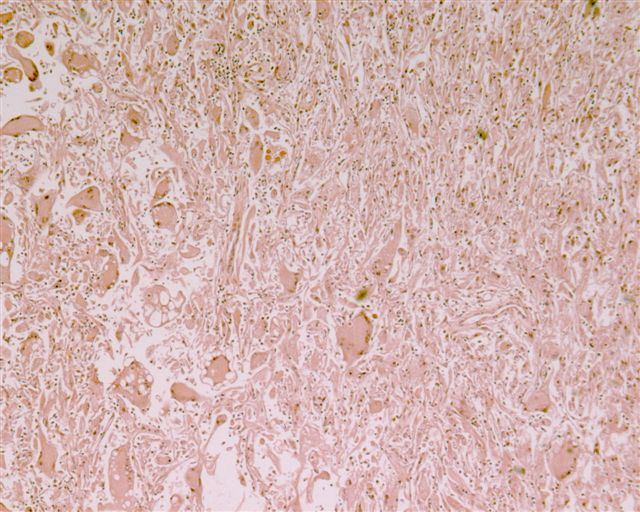
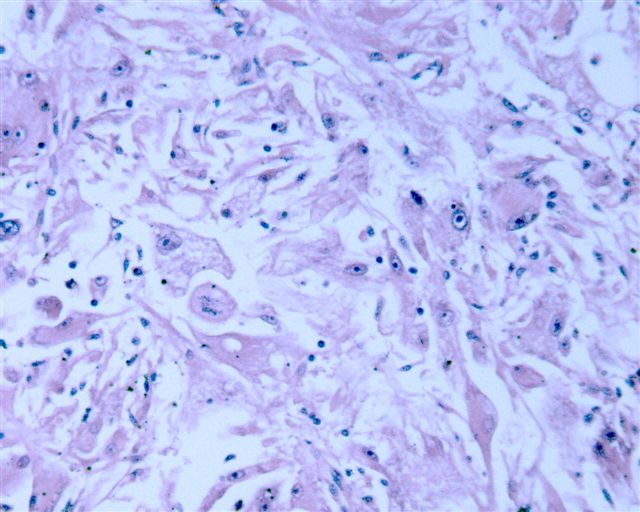
Microscopic images (low to high power):


What is your diagnosis?
Diagnosis: Atypical epithelioid angiomyolipoma
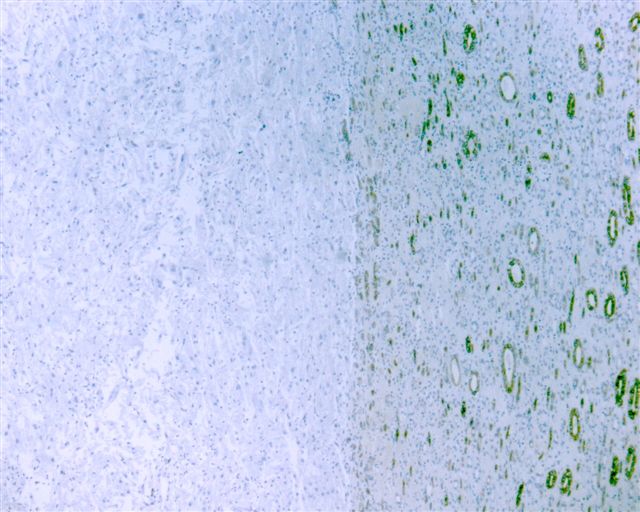
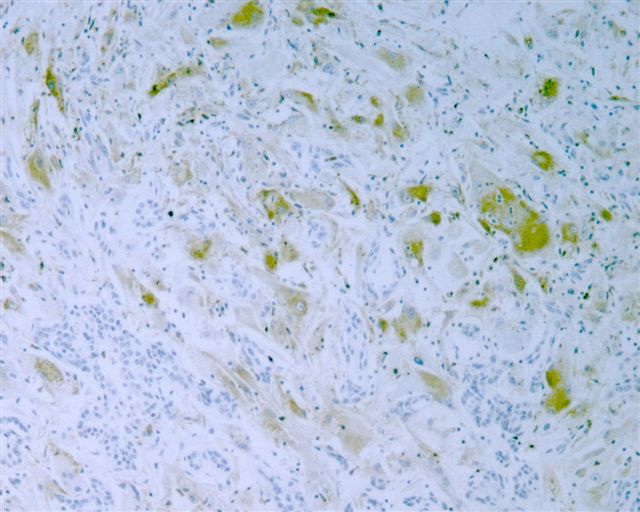
Immunostain images:




Discussion:
The most striking feature of this tumor was the strap-like (similar to rhabdomyosarcoma), bizarre, huge epithelioid cells with abundant eosinophilic cytoplasm and multiple peripheral nuclei with coarse chromatin and prominent nucleoli. Although not obvious in these images, they were often concentrated around blood vessels. The tumor cells had focal spindled areas that were SMA+ and only rare mitotic figures. The tumor cells were immunoreactive for HMB45, MelanA and focally for CD68. They were negative (with an internal positive control in normal kidney) for CD10, RCC and AE1 / AE3 and were also negative for S100, PAS and desmin.
Angiomyolipomas are benign kidney neoplasms often associated with tuberous sclerosis (OMIM: Tuberous Sclerosis 1; TSC1 [Accessed 8 December 2023]), an autosomal dominant neurocutaneous disorder. The tumors are composed of thick walled blood vessels, smooth muscle spindle cells that appear to spin off vessel walls and lipid distended cells. Typically, they have benign behavior. The cell of origin is the perivascular epithelioid cell, which also causes lymphangioleiomyomatosis and sugar tumors in the lung, clear cell tumors of the pancreas and uterus and other PEComas. These tumors are immunoreactive for melanocytic markers (HMB45, MelanA, NCI-C3) and negative for keratins.
An important variant is epithelioid angiomyolipoma, also called atypical or oncocytoid. They have a predominance of epithelioid cells ranging from uniform polygonal cells with mild atypia to the bizarre, multinucleated, strap-like cells seen in this case. There may be no recognizable adipose tissue and sclerosed vessels may appear as hyaline cords. Mitotic activity is usually minimal. However, they may have aggressive behavior, which to date, cannot be predicted based on morphology or other clinicopathologic factors. In this patient, at 1 year postexcision, there has been no recurrence.
The differential diagnosis includes tumors that usually demonstrate marked mitotic activity or necrosis (sarcomatoid renal cell carcinoma, adrenocortical carcinoma, primary renal sarcoma, melanoma) and oncocytoma, which may have degenerative atypia.
References: Am J Surg Pathol 1997;21:1123 (report of 5 cases), Arch Pathol Lab Med 2004;128:1176 (this case but different photos), Am J Surg Pathol 1998;22:663 (resemble sarcomatoid renal cell carcinoma)
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Khaldoon Aljerian, University of Toronto, Ontario, Canada.
Case #32
Clinical history:
A 44 year old woman with biliary colic had an ultrasound that revealed gallstones and an incidental 3 cm solid mass in the left kidney, which was confirmed by CT and MRI. A complete nephrectomy was performed due to the central location of the mass and its proximity to the major renal vessels.
The mass was 2.5 cm, solid, well circumscribed and brown-red. There was no gross necrosis, hemorrhage or renal venous involvement. The remaining kidney was unremarkable.
Microscopic images (low to high power):
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Atypical epithelioid angiomyolipoma
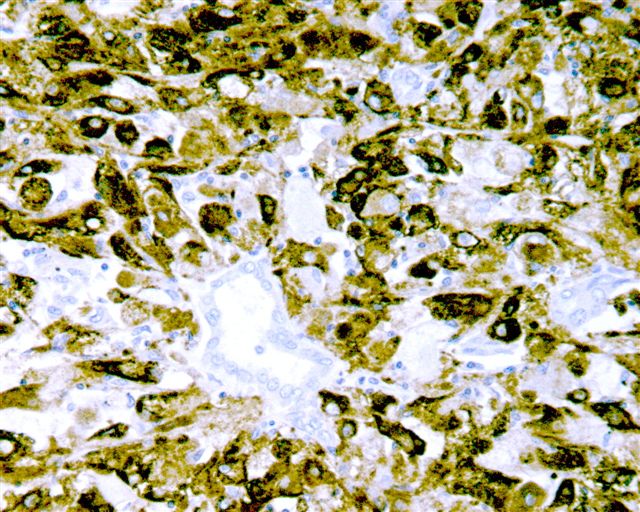
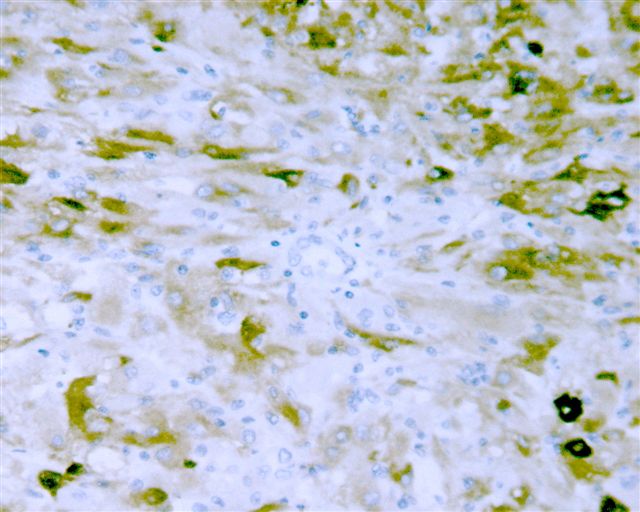
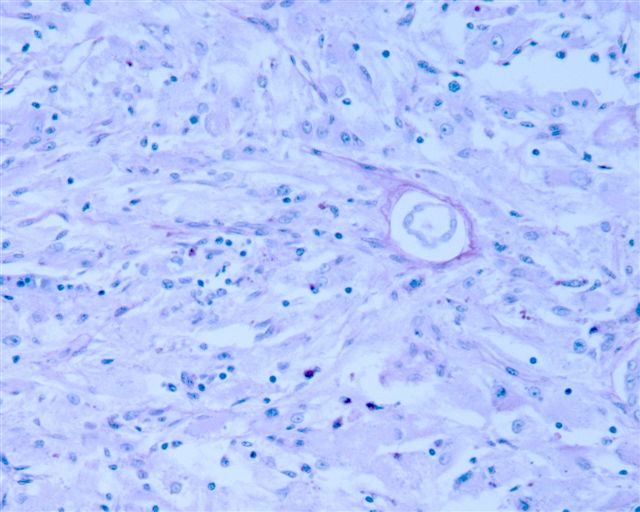
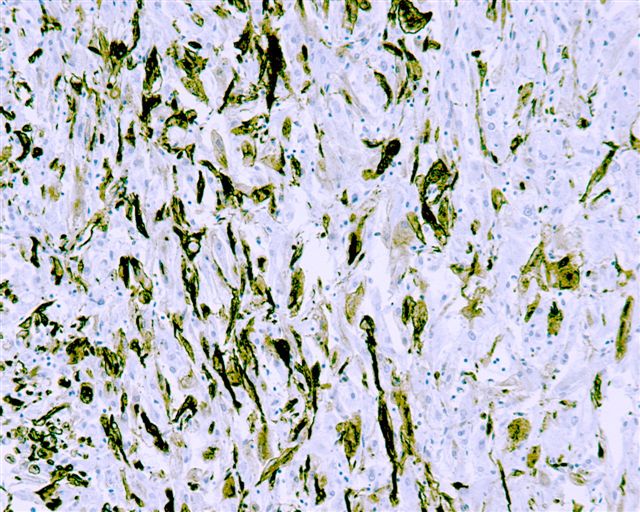
Immunostain images:
AE1 / AE3
CD10
CD68
Desmin
HMB45
MelanA
PAS
RCC
S100
Smooth muscle actin
Discussion:
The most striking feature of this tumor was the strap-like (similar to rhabdomyosarcoma), bizarre, huge epithelioid cells with abundant eosinophilic cytoplasm and multiple peripheral nuclei with coarse chromatin and prominent nucleoli. Although not obvious in these images, they were often concentrated around blood vessels. The tumor cells had focal spindled areas that were SMA+ and only rare mitotic figures. The tumor cells were immunoreactive for HMB45, MelanA and focally for CD68. They were negative (with an internal positive control in normal kidney) for CD10, RCC and AE1 / AE3 and were also negative for S100, PAS and desmin.
Angiomyolipomas are benign kidney neoplasms often associated with tuberous sclerosis (OMIM: Tuberous Sclerosis 1; TSC1 [Accessed 8 December 2023]), an autosomal dominant neurocutaneous disorder. The tumors are composed of thick walled blood vessels, smooth muscle spindle cells that appear to spin off vessel walls and lipid distended cells. Typically, they have benign behavior. The cell of origin is the perivascular epithelioid cell, which also causes lymphangioleiomyomatosis and sugar tumors in the lung, clear cell tumors of the pancreas and uterus and other PEComas. These tumors are immunoreactive for melanocytic markers (HMB45, MelanA, NCI-C3) and negative for keratins.
An important variant is epithelioid angiomyolipoma, also called atypical or oncocytoid. They have a predominance of epithelioid cells ranging from uniform polygonal cells with mild atypia to the bizarre, multinucleated, strap-like cells seen in this case. There may be no recognizable adipose tissue and sclerosed vessels may appear as hyaline cords. Mitotic activity is usually minimal. However, they may have aggressive behavior, which to date, cannot be predicted based on morphology or other clinicopathologic factors. In this patient, at 1 year postexcision, there has been no recurrence.
The differential diagnosis includes tumors that usually demonstrate marked mitotic activity or necrosis (sarcomatoid renal cell carcinoma, adrenocortical carcinoma, primary renal sarcoma, melanoma) and oncocytoma, which may have degenerative atypia.
References: Am J Surg Pathol 1997;21:1123 (report of 5 cases), Arch Pathol Lab Med 2004;128:1176 (this case but different photos), Am J Surg Pathol 1998;22:663 (resemble sarcomatoid renal cell carcinoma)
