
26 April 2006 - Case #43
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Choladda Vejabhuti, Baylor College of Medicine, Houston, Texas, USA.
Case #43
Clinical history:
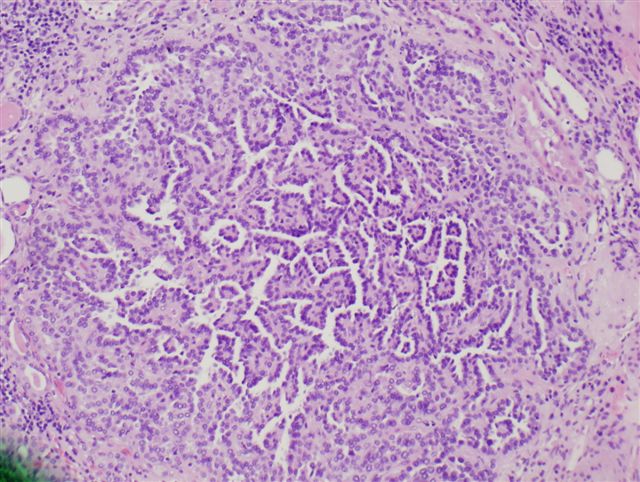
A 44 year old man with a left renal mass underwent left radical nephrectomy. An incidental lesion, 1 mm in size, was found.
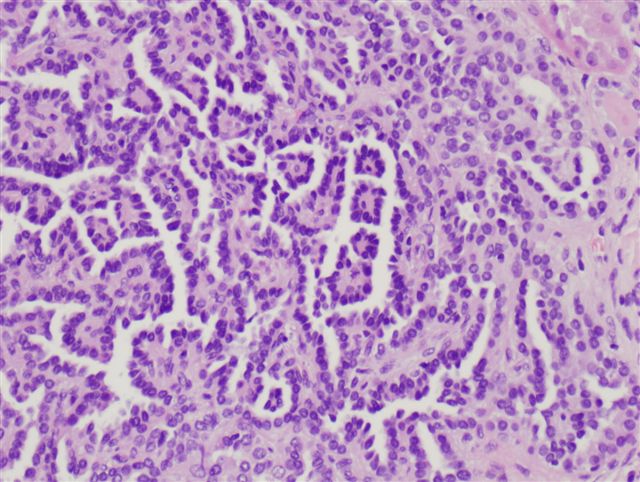
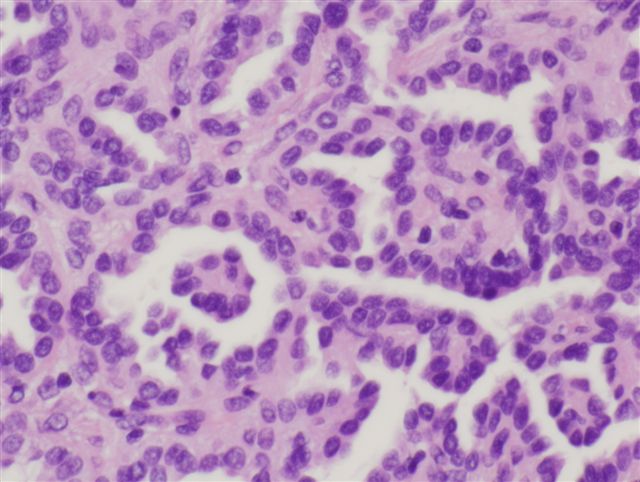
Microscopic images:
What is your diagnosis?
Diagnosis: Papillary adenoma
Discussion:
Renal cortical adenomas are commonly found at autopsy, with an incidence of 10% at age 21 - 40 years increasing to 40% at 70 - 90 years. The incidence during life is increasing due to more frequent abdominal imaging.
According to the 2016 WHO, a papillary adenoma must be ≤ 1.5 cm.
Grossly, these tumors are usually yellow-gray, well demarcated but often not encapsulated. They have papillary, tubular or mixed architecture and are composed of small cuboidal cells with variable eosinophilic cytoplasm and uniform round nuclei. No atypia is present and mitotic figures are absent / rare. There may be occasional clear cells, although tumors composed predominantly of clear cells should be designated as renal cell carcinoma, clear cell type. Occasionally, mucin production is present (Histol Histopathol 2001;16:387).
Cytogenetic studies of these small tumors show gains of chromosomes 7, 17, 16, 12 and 20 and loss of the Y chromosome (FISH image), which are identical to the changes in renal papillary carcinoma, suggesting that these changes occur early in papillary neoplasia (Mod Pathol 2003;16:1053).
References: Murphy: Tumors of the Kidney, Bladder and Related Urinary Structures, 4th Edition, 2004
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Choladda Vejabhuti, Baylor College of Medicine, Houston, Texas, USA.
Website news:
(1) This case is sponsored by Nature Publishing Group:
Check out the new section of Laboratory Investigation Summer 2006
Pathobiology in Focus
The new section will consist of:
The aims of this new section are to:
Articles will be available FREE online www.laboratoryinvestigation.org
Visit and follow our Blog to see recent updates to the website.
(1) This case is sponsored by Nature Publishing Group:
Check out the new section of Laboratory Investigation Summer 2006
Pathobiology in Focus
The new section will consist of:
- Succinct critical reviews of pathobiology
- Commentaries on major breakthroughs
- Controversies in mechanisms of human disease
- Updates on seminal technological advances
- Mechanism based illustrations prepared by Nature Publishing Groups art department
The aims of this new section are to:
- Drive discussion and present hypotheses related to disease mechanisms
- Promote translation of basic research findings into progress in diagnosis and analysis of human disease
- Make complex areas, including technological breakthroughs, accessible to practicing and investigative pathologists
Articles will be available FREE online www.laboratoryinvestigation.org
Visit and follow our Blog to see recent updates to the website.
Case #43
Clinical history:
A 44 year old man with a left renal mass underwent left radical nephrectomy. An incidental lesion, 1 mm in size, was found.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Papillary adenoma
Discussion:
Renal cortical adenomas are commonly found at autopsy, with an incidence of 10% at age 21 - 40 years increasing to 40% at 70 - 90 years. The incidence during life is increasing due to more frequent abdominal imaging.
According to the 2016 WHO, a papillary adenoma must be ≤ 1.5 cm.
Grossly, these tumors are usually yellow-gray, well demarcated but often not encapsulated. They have papillary, tubular or mixed architecture and are composed of small cuboidal cells with variable eosinophilic cytoplasm and uniform round nuclei. No atypia is present and mitotic figures are absent / rare. There may be occasional clear cells, although tumors composed predominantly of clear cells should be designated as renal cell carcinoma, clear cell type. Occasionally, mucin production is present (Histol Histopathol 2001;16:387).
Cytogenetic studies of these small tumors show gains of chromosomes 7, 17, 16, 12 and 20 and loss of the Y chromosome (FISH image), which are identical to the changes in renal papillary carcinoma, suggesting that these changes occur early in papillary neoplasia (Mod Pathol 2003;16:1053).
References: Murphy: Tumors of the Kidney, Bladder and Related Urinary Structures, 4th Edition, 2004
