
7 December 2006 - Case #66
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Ronald M. Angeles, University of Pittsburgh, Pennsylvania, USA.
Case #66
Clinical history:
A 71 year old man complained of a slowly growing mass in the left popliteal fossa. CT scans and MRI studies showed a well circumscribed mass without invasion of the surrounding neurovascular bundle, bone or soft tissues.
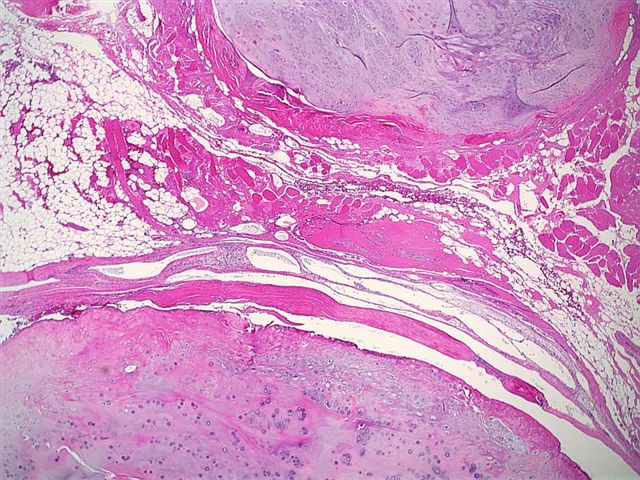
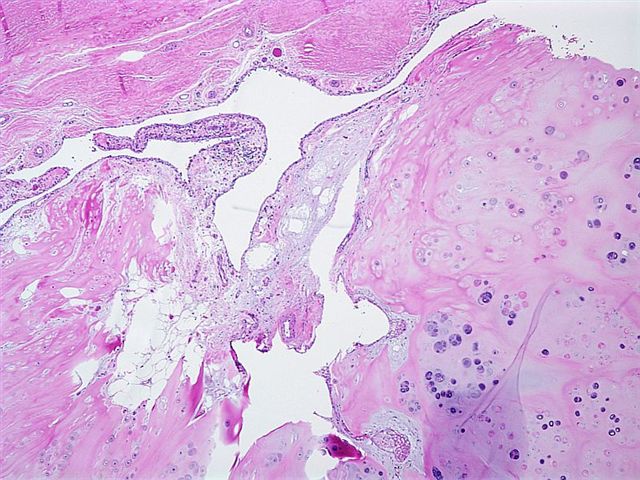
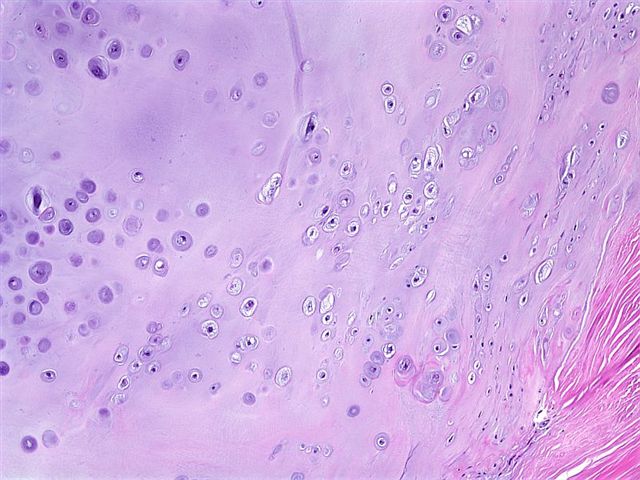
The mass consists mostly of confluent and occasionally discrete lobules of moderately cellular hyaline cartilage. There is focal endochondral ossification. Cellular atypia is mild. No mitotic figures or necrosis are identified.
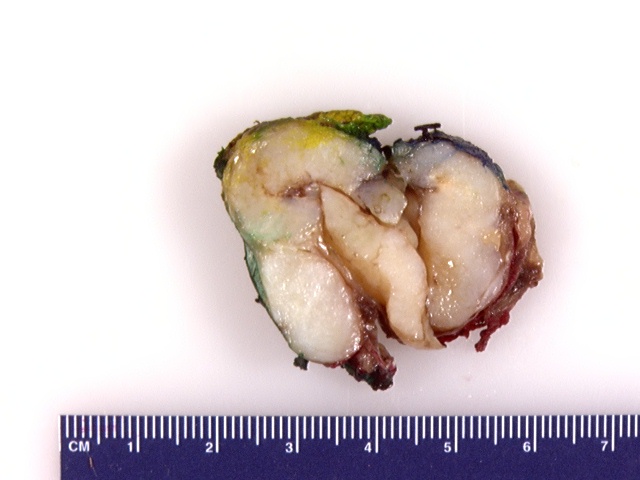
Gross images:

Microscopic images:
What is your diagnosis?
Diagnosis: Synovial chondromatosis of the popliteal fossa
Discussion:
Synovial chondromatosis is also called synovial chondrometaplasia or synovial osteochondromatosis. It may be primary or secondary to other joint disease. It typically affects men, with a mean age of 41 years but a range of 17 to 64 years.
Primary cases are uncommon and often aggressive. They are typically monoarticular and affect the knee, hip, elbow and their communicating bursae, with occasional infiltration into adjacent soft tissue (Pathologica 2001;93:132). Radiographs usually show calcific densities within a joint, although they may also be negative.
Secondary cases occur due to degenerative joint disease, neuropathic arthropathy or osteochondritis dissecans (Hum Pathol 1979;10:439).
On gross exam, numerous round osteocartilaginous nodules cover a thickened synovial surface or float freely within the joint space. Microscopically, there are cartilaginous cells with variable atypia or binucleated forms within synovium.
The differential diagnosis includes benign chondroma of soft tissue and low grade chondrosarcoma. The extra-articular form of synovial chondromatosis, called tenosynovial chondromatosis, resembles chondroma of soft tissue, in that both occur in the soft tissue of the hands and feet and both lack a connection to bone (Am J Surg Pathol 2003;27:1260). However, chondromas lack a synovial or tenosynovial layer or subsynovial connective tissue that is present in chondromatosis. Chondrosarcomas typically do not arise from within a joint. They lack a characteristic clustering pattern and have marked myxoid change and spindling of nuclei.
Treatment of synovial chondromatosis consists of excision but it frequently recurs. These tumors become malignant in about 5% of cases (Hum Pathol 1998;29:683).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
This case was contributed by Dr. Ronald M. Angeles, University of Pittsburgh, Pennsylvania, USA.
Website news:
(1) With the holiday season upon us, we recommend you consider purchasing gifts and books online at Amazon.com through the links on our Home Page (footer), on the Books page (click on any Book title) or by clicking here. Most Amazon.com shoppers have a good shopping experience. You can buy new or used products from various companies for competitive prices. There is free shipping for many products and they have a good return policy. In addition, purchases made through links on our website help us continue to expand our free website, without costing you anything and may even save you money through Amazon's discounts.
Visit and follow our Blog to see recent updates to the website.
(1) With the holiday season upon us, we recommend you consider purchasing gifts and books online at Amazon.com through the links on our Home Page (footer), on the Books page (click on any Book title) or by clicking here. Most Amazon.com shoppers have a good shopping experience. You can buy new or used products from various companies for competitive prices. There is free shipping for many products and they have a good return policy. In addition, purchases made through links on our website help us continue to expand our free website, without costing you anything and may even save you money through Amazon's discounts.
Visit and follow our Blog to see recent updates to the website.
Case #66
Clinical history:
A 71 year old man complained of a slowly growing mass in the left popliteal fossa. CT scans and MRI studies showed a well circumscribed mass without invasion of the surrounding neurovascular bundle, bone or soft tissues.
The mass consists mostly of confluent and occasionally discrete lobules of moderately cellular hyaline cartilage. There is focal endochondral ossification. Cellular atypia is mild. No mitotic figures or necrosis are identified.
Gross images:
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Synovial chondromatosis of the popliteal fossa
Discussion:
Synovial chondromatosis is also called synovial chondrometaplasia or synovial osteochondromatosis. It may be primary or secondary to other joint disease. It typically affects men, with a mean age of 41 years but a range of 17 to 64 years.
Primary cases are uncommon and often aggressive. They are typically monoarticular and affect the knee, hip, elbow and their communicating bursae, with occasional infiltration into adjacent soft tissue (Pathologica 2001;93:132). Radiographs usually show calcific densities within a joint, although they may also be negative.
Secondary cases occur due to degenerative joint disease, neuropathic arthropathy or osteochondritis dissecans (Hum Pathol 1979;10:439).
On gross exam, numerous round osteocartilaginous nodules cover a thickened synovial surface or float freely within the joint space. Microscopically, there are cartilaginous cells with variable atypia or binucleated forms within synovium.
The differential diagnosis includes benign chondroma of soft tissue and low grade chondrosarcoma. The extra-articular form of synovial chondromatosis, called tenosynovial chondromatosis, resembles chondroma of soft tissue, in that both occur in the soft tissue of the hands and feet and both lack a connection to bone (Am J Surg Pathol 2003;27:1260). However, chondromas lack a synovial or tenosynovial layer or subsynovial connective tissue that is present in chondromatosis. Chondrosarcomas typically do not arise from within a joint. They lack a characteristic clustering pattern and have marked myxoid change and spindling of nuclei.
Treatment of synovial chondromatosis consists of excision but it frequently recurs. These tumors become malignant in about 5% of cases (Hum Pathol 1998;29:683).
