
25 January 2013 - Case #264
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Jitendra Khedkar, Krishna Institute of Health Sciences University, India, for contributing this case and the discussion. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.
Advertisement
Case #264
Clinical history:
A 22 year old primigravida woman with 25 weeks of amenorrhea presented with a rapidly enlarging abdomen and discomfort. Ultrasound at 25 weeks revealed twins. One twin had severe oligohydramnios, intrauterine growth restriction and was considered a "stuck" twin (donor) with gestational age of 20 weeks. The other twin (considered recipient) had polyhydramnios and gestational age of 25 weeks.
At 30 weeks, amniocentesis was performed to correct the polyhydramnios. At 35 weeks, caesarian section was performed to save the twin with polyhydramnios (the other twin suffered intrauterine death). The placentas were received for histopathological examination.
Gross images:



Microscopic images:

What is your diagnosis?
Diagnosis: Twin transfusion syndrome
Discussion:
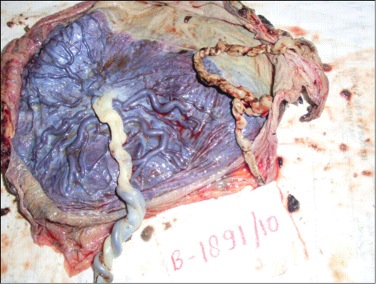
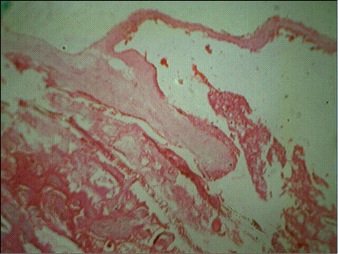
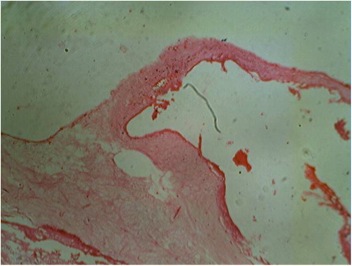
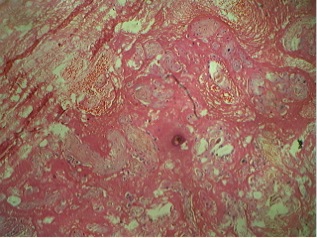
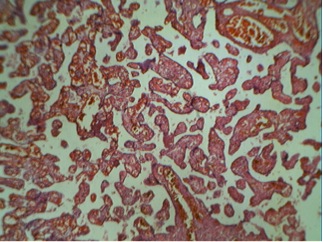
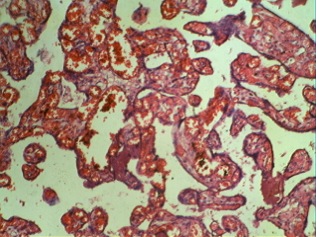
Figures 1 and 2 show a single placental disc with two amniotic sacs of dissimilar size separated by a thin, wispy dividing membrane. The external surface shows tortuous anastomotic vessels, with the donor placenta showing velamentous insertion of the cord. Figures 3 and 4: the cut section of the recipient territory shows extreme congestion and tortuous vessels. The cut section of the donor territory shows extreme pallor and collapsed vessels. Figures 5 and 6: microscopy through the "T" section of the placenta shows a monochorionic diamniotic placenta. Figure 7 and 11: microscopy of the donor placenta shows collapsed vessels and features of intrauterine death. Figure 8 and 12: microscopy of the recipient placenta shows tortuous anastomotic vessels.
Twin transfusion syndrome (TTS) is a serious condition that affects 10 - 15% of twin pregnancies with monochorionic placentation (Semin Perinatol 2012;36:182, Wikipedia: Twin-to-Twin Transfusion Syndrome [Accessed 8 April 2024]). It occurs due to intrauterine blood transfusion from one twin (donor) to another twin (recipient) through placental vascular anastomoses from shared placental cotyledons. This results in increased fetal and neonatal mortality, premature delivery and neurologic complications in the surviving twin(s).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Jitendra Khedkar, Krishna Institute of Health Sciences University, India, for contributing this case and the discussion. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.


February 4-8, 2013
The Canyons Resort
Park City, Utah (USA)
26th Annual Park City
Combined AP/CP Pathology Update

Website
Schedule
Hotel
Registration
For more information, contact:
Leita Rogers
Telephone: (801) 581-2034
Email: Leita.Rogers@aruplab.com
Website news:
(1) We posted a new article on our Management Page: A Managed Care Contracting Plan for Independent / Outreach Labs, Or How to stay profitable even if Medicare cuts your rates - Part One, by Mick Raich, President, Vachette Pathology.
(2) We have updated the Lung tumor chapter based on reviews by Drs. Deepali Jain and Fulvio Lonardo.
(3) New updates to our CME / Apps page include an advertisement for BoardVitals Pathology Question Bank and a free Apple app - Boardvitals Review for Clinical Pathology
Visit and follow our Blog to see recent updates to the website.
(1) We posted a new article on our Management Page: A Managed Care Contracting Plan for Independent / Outreach Labs, Or How to stay profitable even if Medicare cuts your rates - Part One, by Mick Raich, President, Vachette Pathology.
(2) We have updated the Lung tumor chapter based on reviews by Drs. Deepali Jain and Fulvio Lonardo.
(3) New updates to our CME / Apps page include an advertisement for BoardVitals Pathology Question Bank and a free Apple app - Boardvitals Review for Clinical Pathology
Visit and follow our Blog to see recent updates to the website.
Case #264
Clinical history:
A 22 year old primigravida woman with 25 weeks of amenorrhea presented with a rapidly enlarging abdomen and discomfort. Ultrasound at 25 weeks revealed twins. One twin had severe oligohydramnios, intrauterine growth restriction and was considered a "stuck" twin (donor) with gestational age of 20 weeks. The other twin (considered recipient) had polyhydramnios and gestational age of 25 weeks.
At 30 weeks, amniocentesis was performed to correct the polyhydramnios. At 35 weeks, caesarian section was performed to save the twin with polyhydramnios (the other twin suffered intrauterine death). The placentas were received for histopathological examination.
Gross images:
Placental discs
Cut section of recipient and donor territory
Microscopic images:
Microscopy through T section of placenta
Microscopy of donor placenta
Microscopy of recipient placenta
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Twin transfusion syndrome
Discussion:
Figures 1 and 2 show a single placental disc with two amniotic sacs of dissimilar size separated by a thin, wispy dividing membrane. The external surface shows tortuous anastomotic vessels, with the donor placenta showing velamentous insertion of the cord. Figures 3 and 4: the cut section of the recipient territory shows extreme congestion and tortuous vessels. The cut section of the donor territory shows extreme pallor and collapsed vessels. Figures 5 and 6: microscopy through the "T" section of the placenta shows a monochorionic diamniotic placenta. Figure 7 and 11: microscopy of the donor placenta shows collapsed vessels and features of intrauterine death. Figure 8 and 12: microscopy of the recipient placenta shows tortuous anastomotic vessels.
Twin transfusion syndrome (TTS) is a serious condition that affects 10 - 15% of twin pregnancies with monochorionic placentation (Semin Perinatol 2012;36:182, Wikipedia: Twin-to-Twin Transfusion Syndrome [Accessed 8 April 2024]). It occurs due to intrauterine blood transfusion from one twin (donor) to another twin (recipient) through placental vascular anastomoses from shared placental cotyledons. This results in increased fetal and neonatal mortality, premature delivery and neurologic complications in the surviving twin(s).
