
9 January 2014 - Case #296
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Wafaey Mohamed, Sharurah Armed Forces Hospital (Saudi Arabia), for contributing this case.
Advertisement
Case #296
Clinical history:
A 28 year old woman presented with a tender, firm nodule on her right big toe measuring 2 x 2 cm, with normal colored overlying skin. An Xray showed no bony changes of the big toe. An excisional biopsy was performed, and received as 2 irregular grayish pieces of tissue.
Microscopic images:


What is your diagnosis?
Diagnosis: Acral myxoinflammatory fibroblastic sarcoma (myxoinflammatory fibroblastic sarcoma of soft tissue)
Discussion:
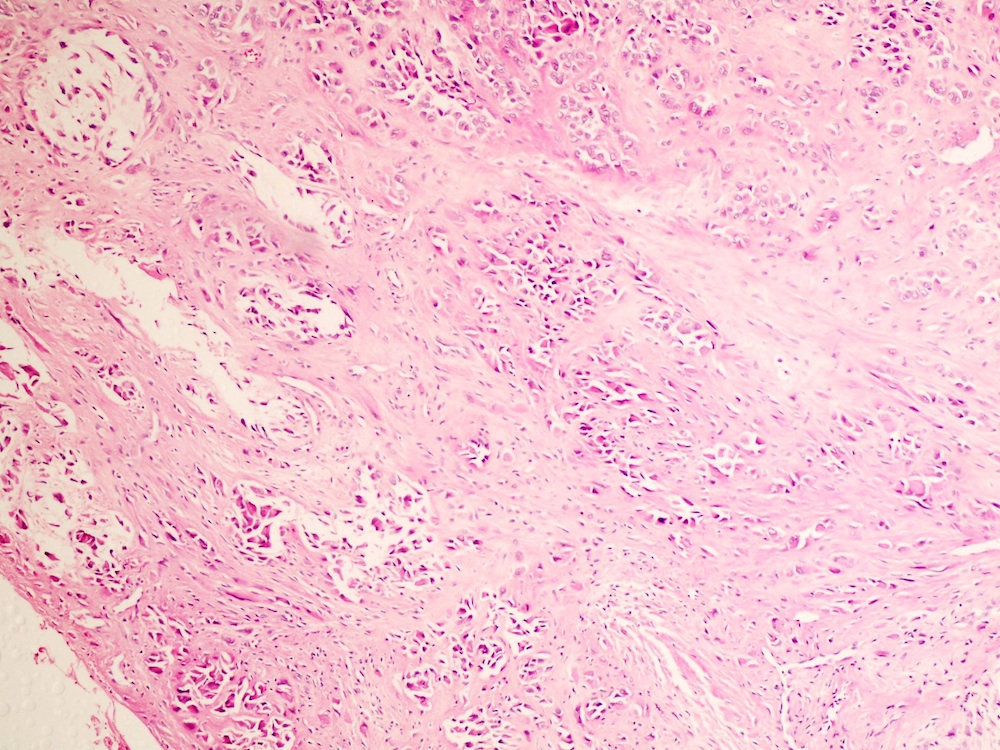
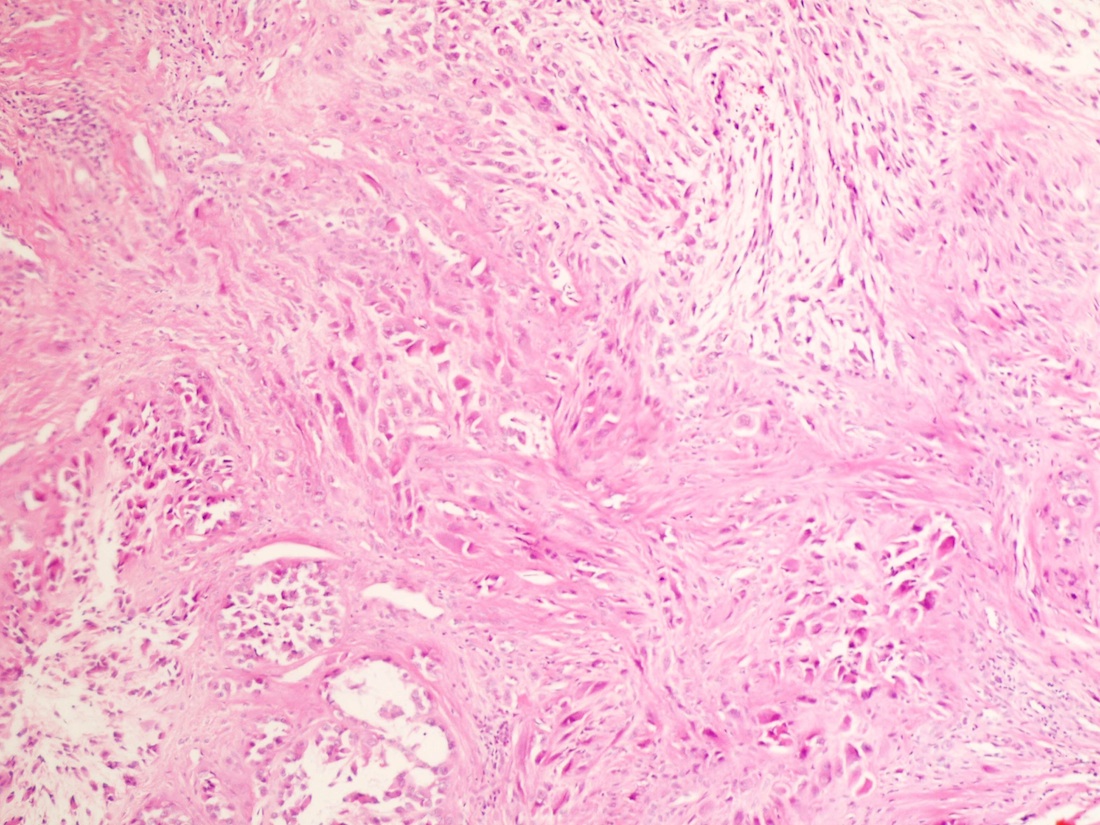
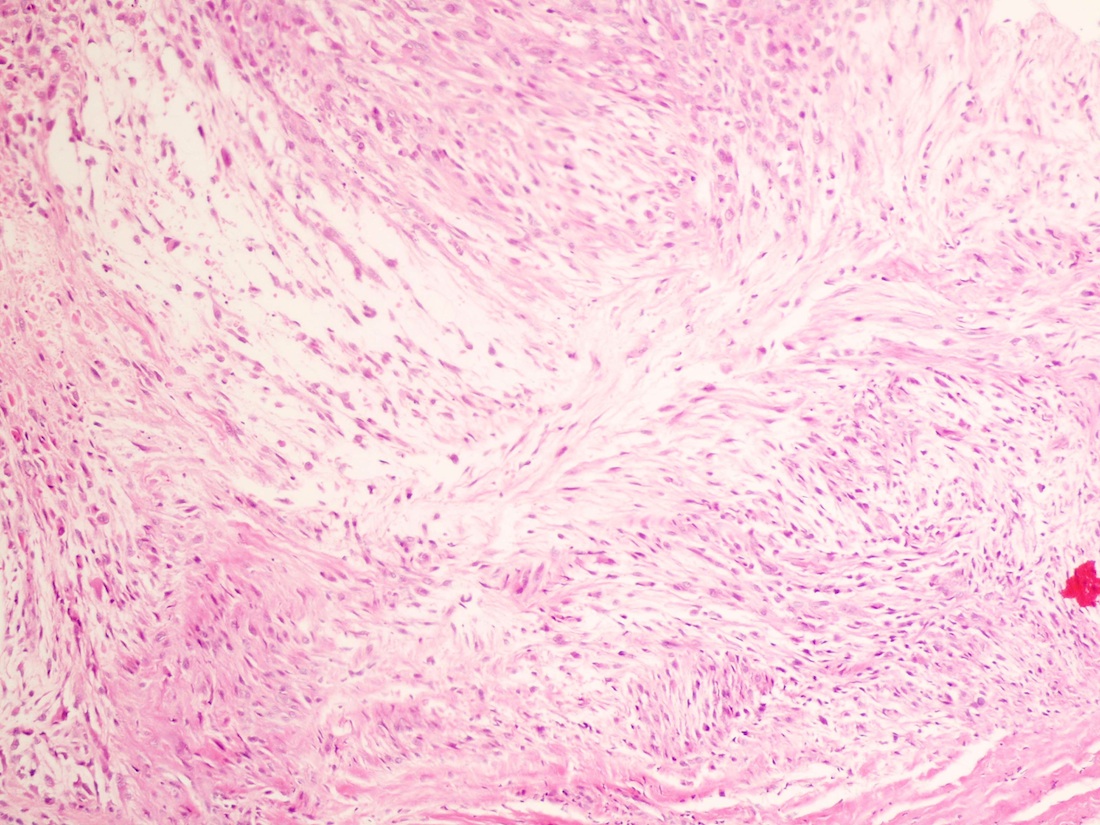
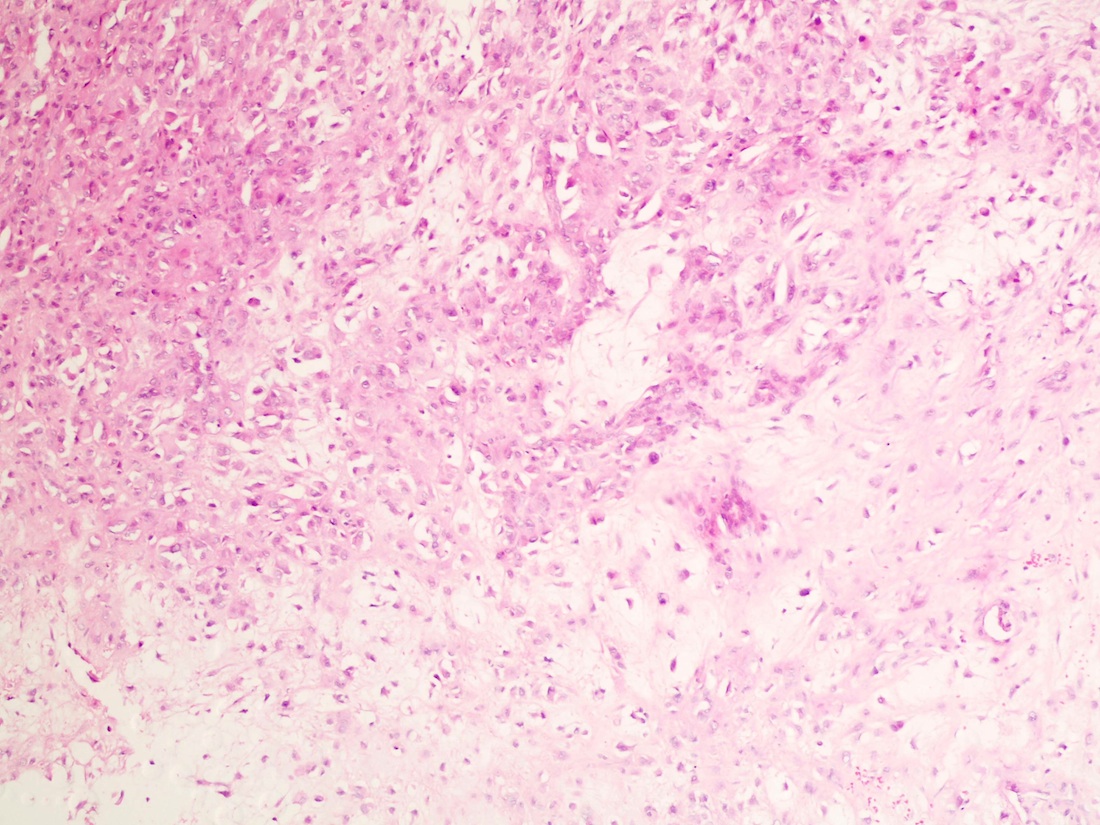
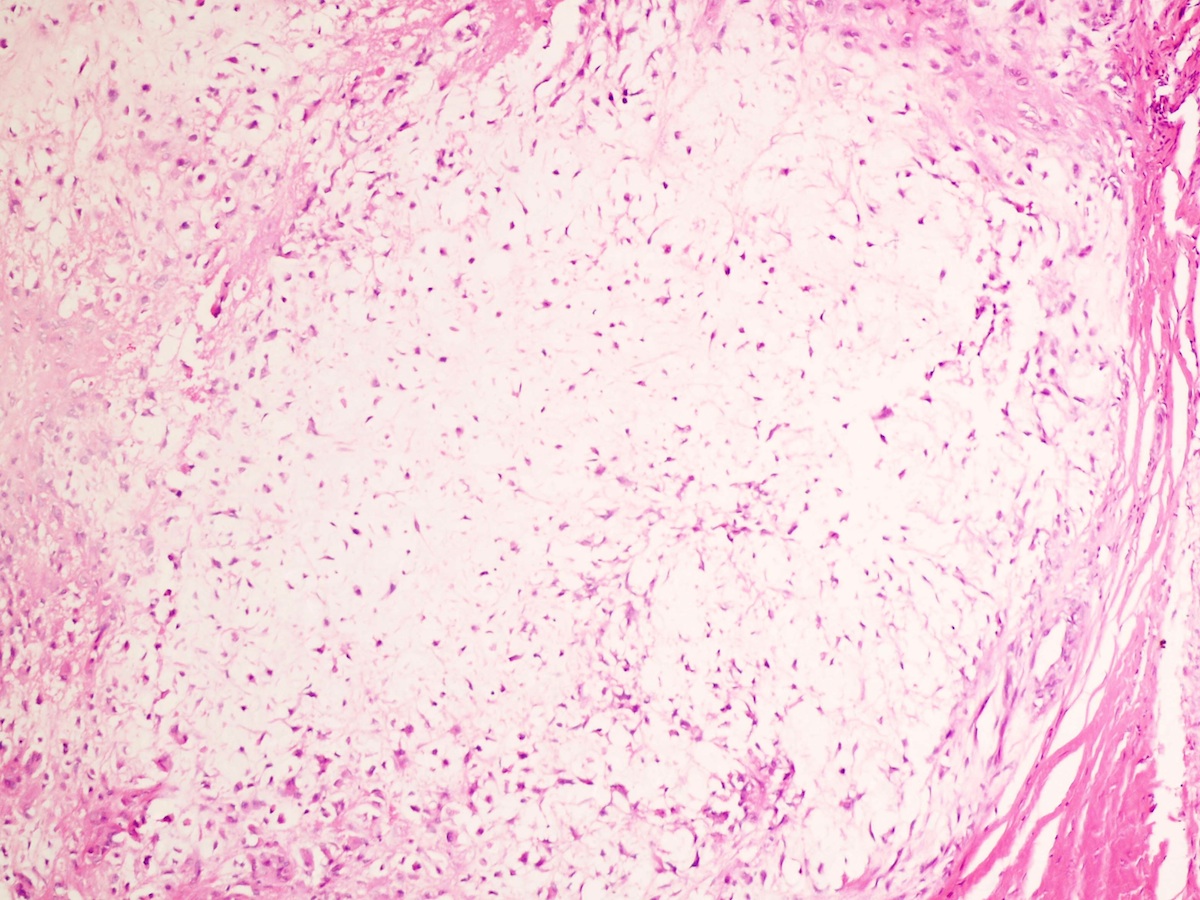
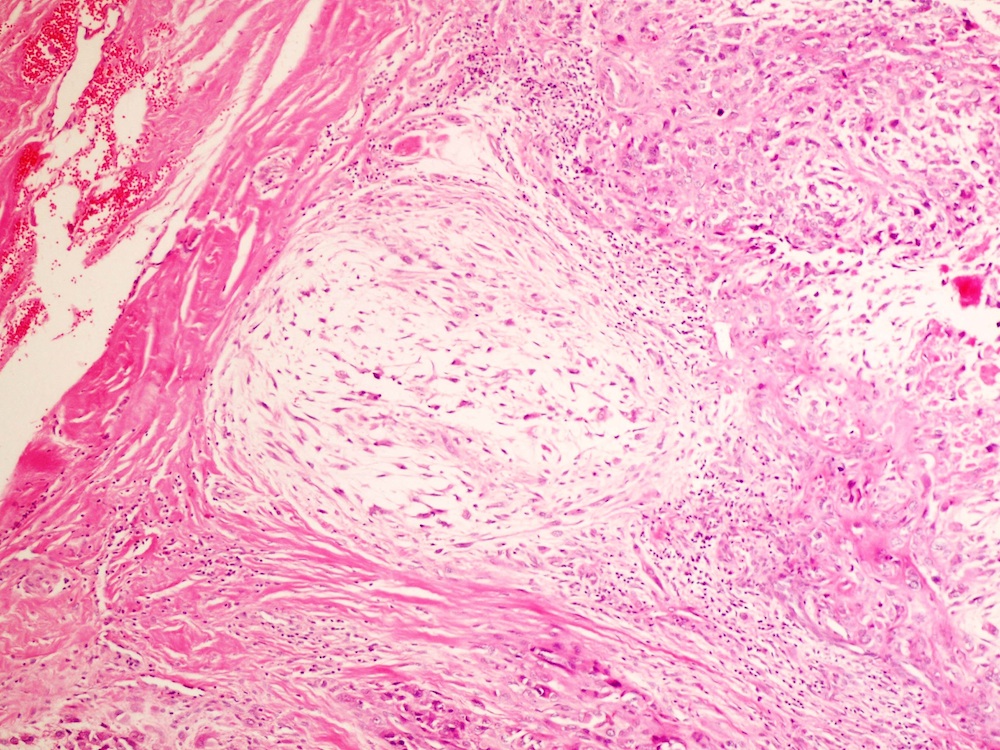
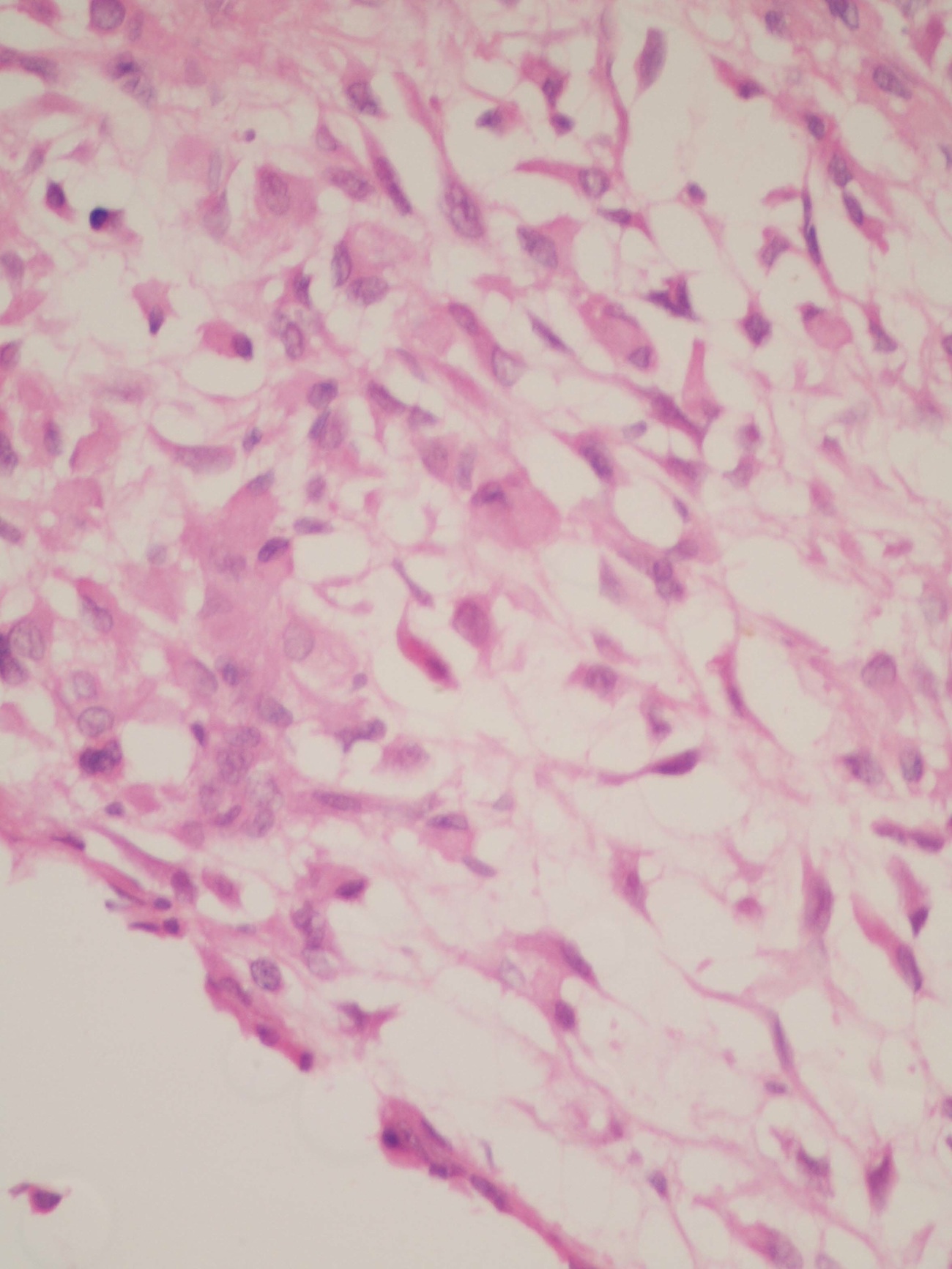
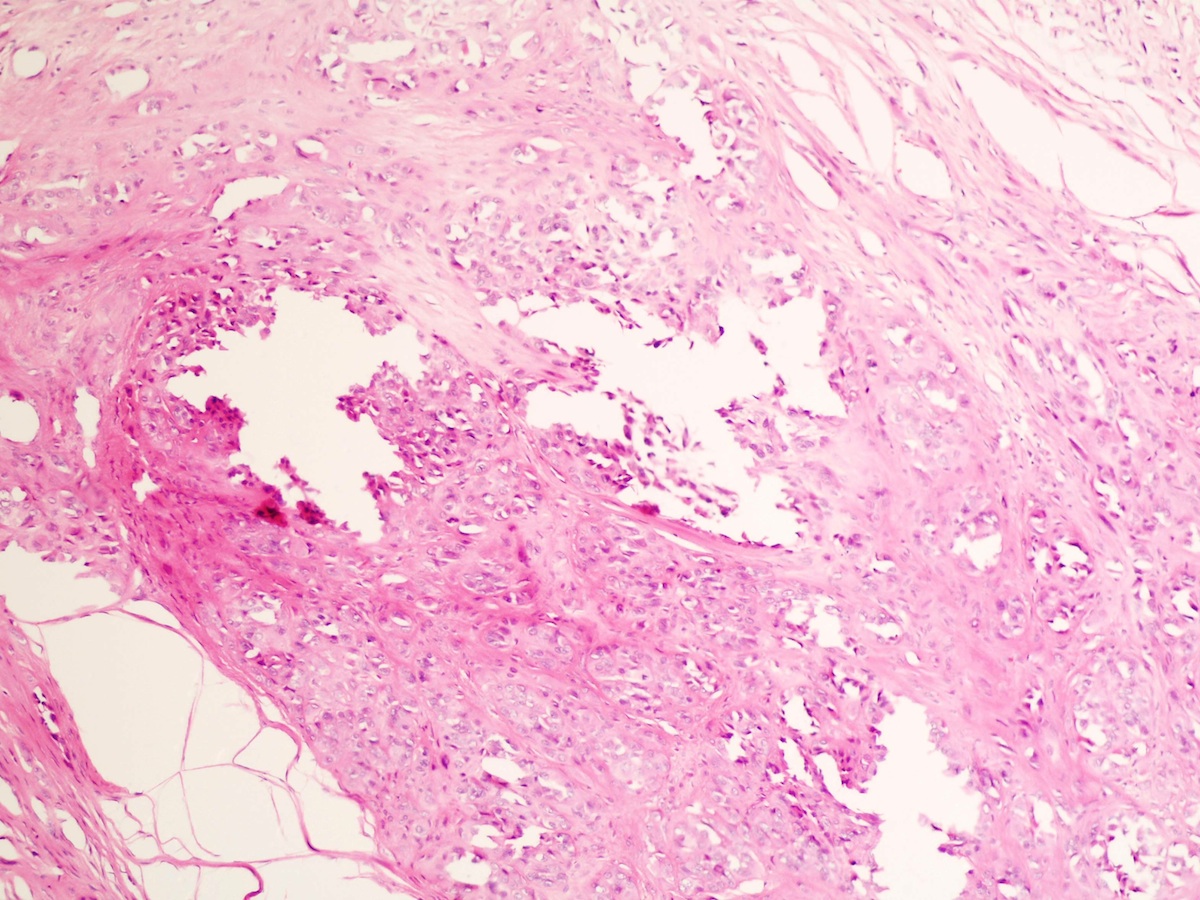
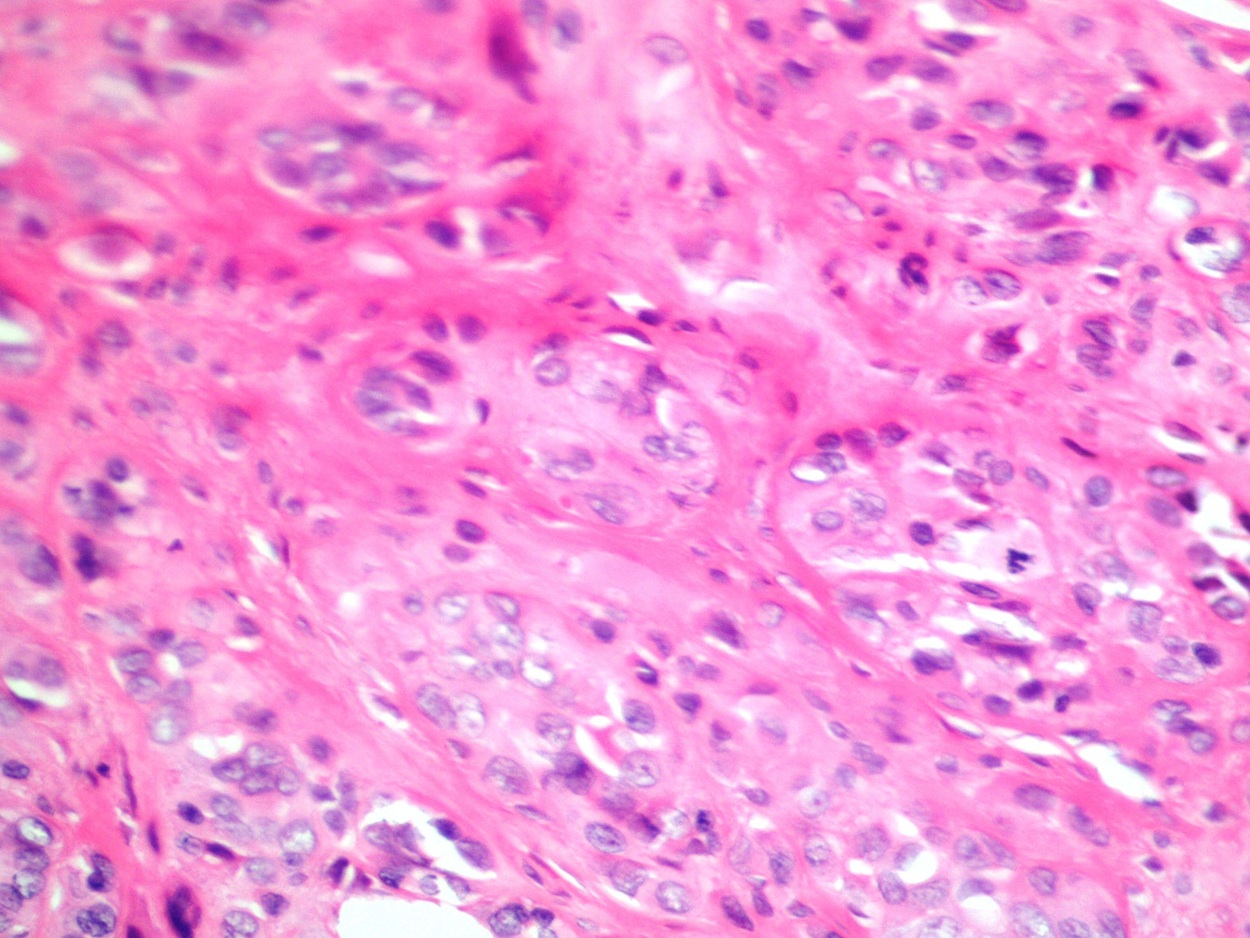
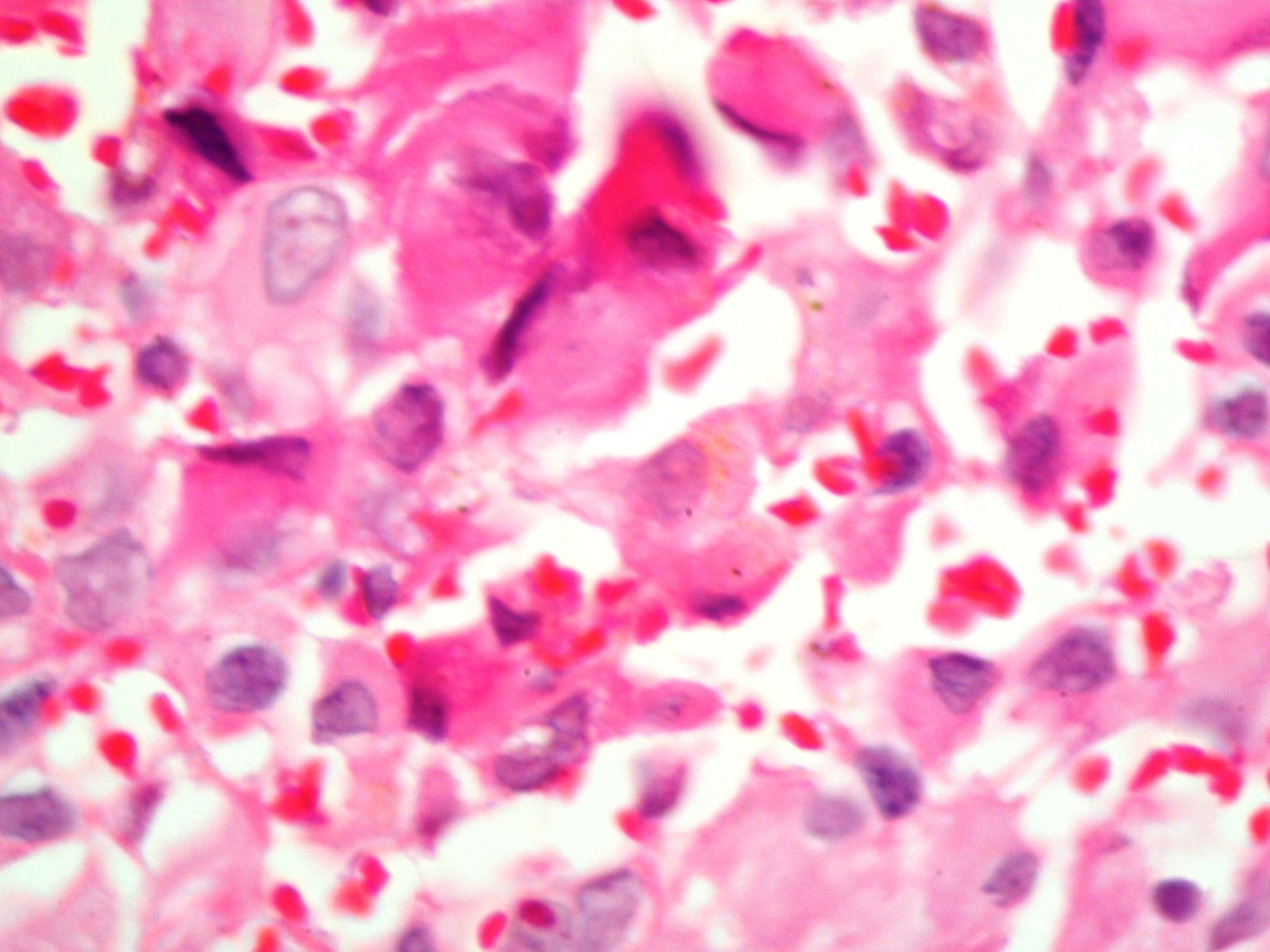
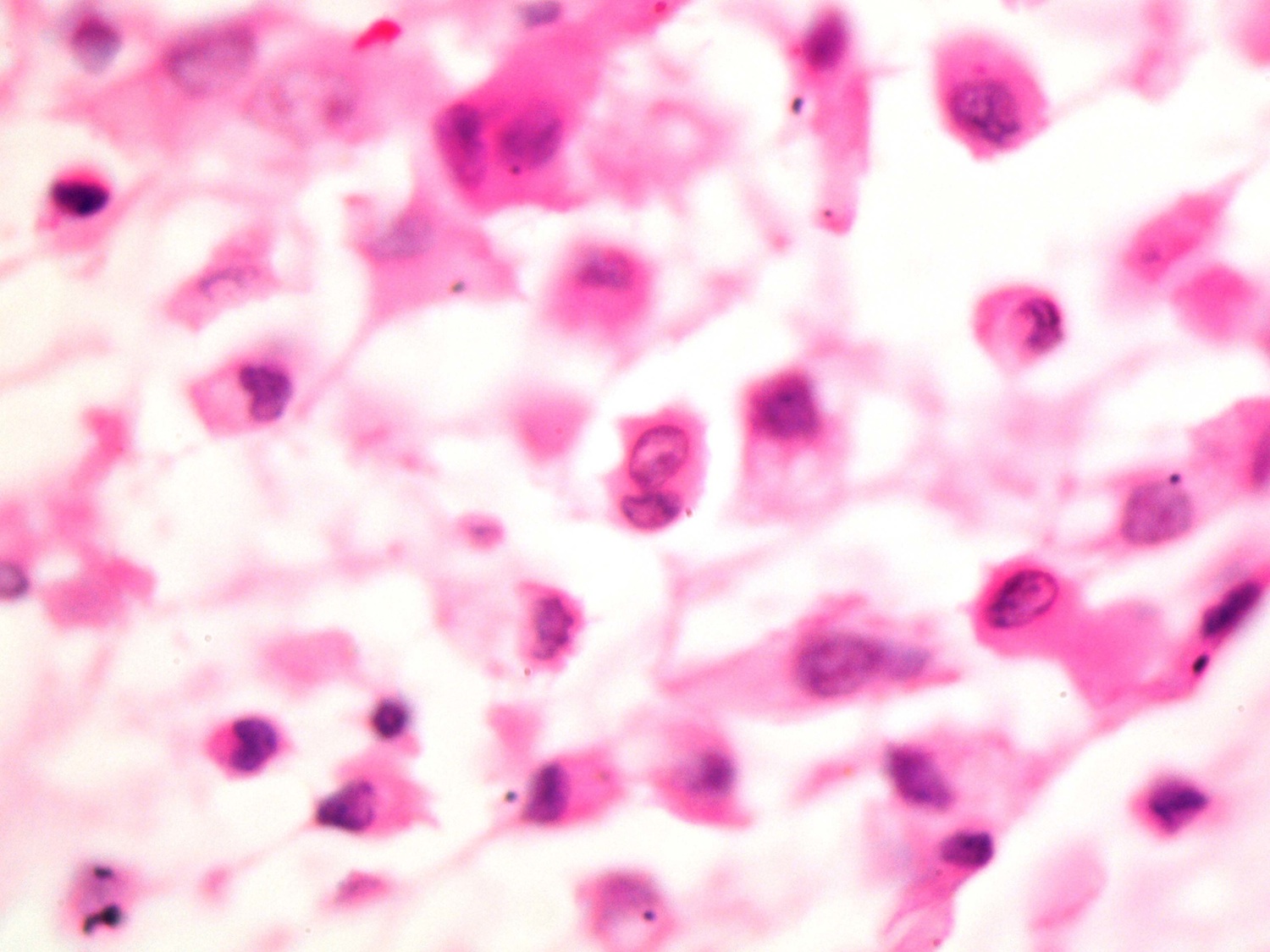
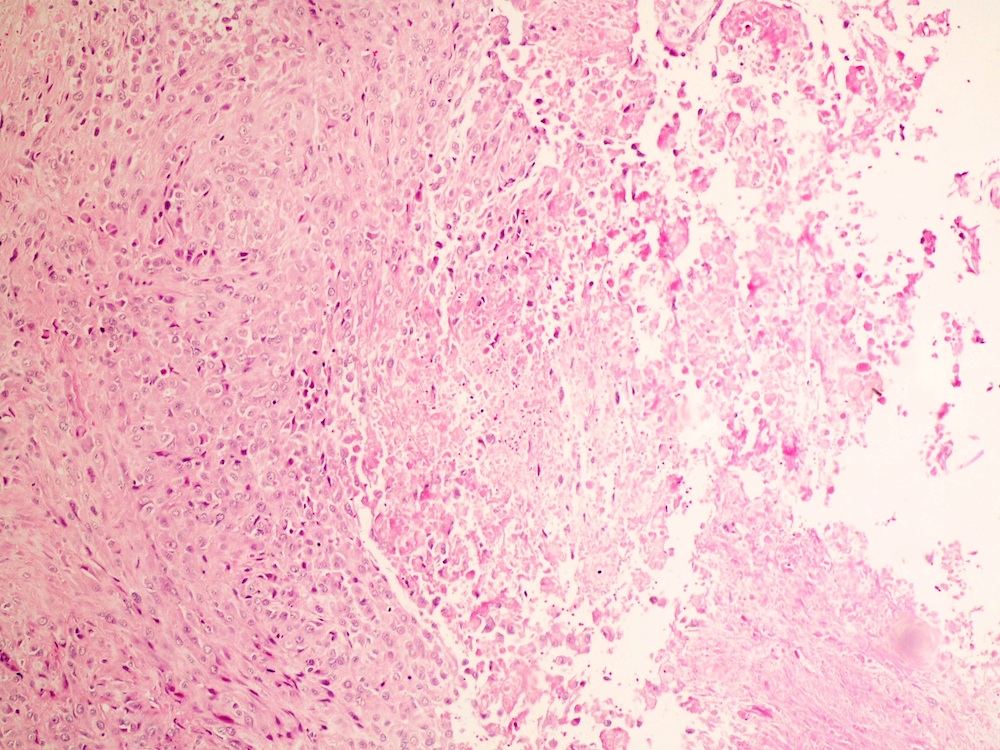
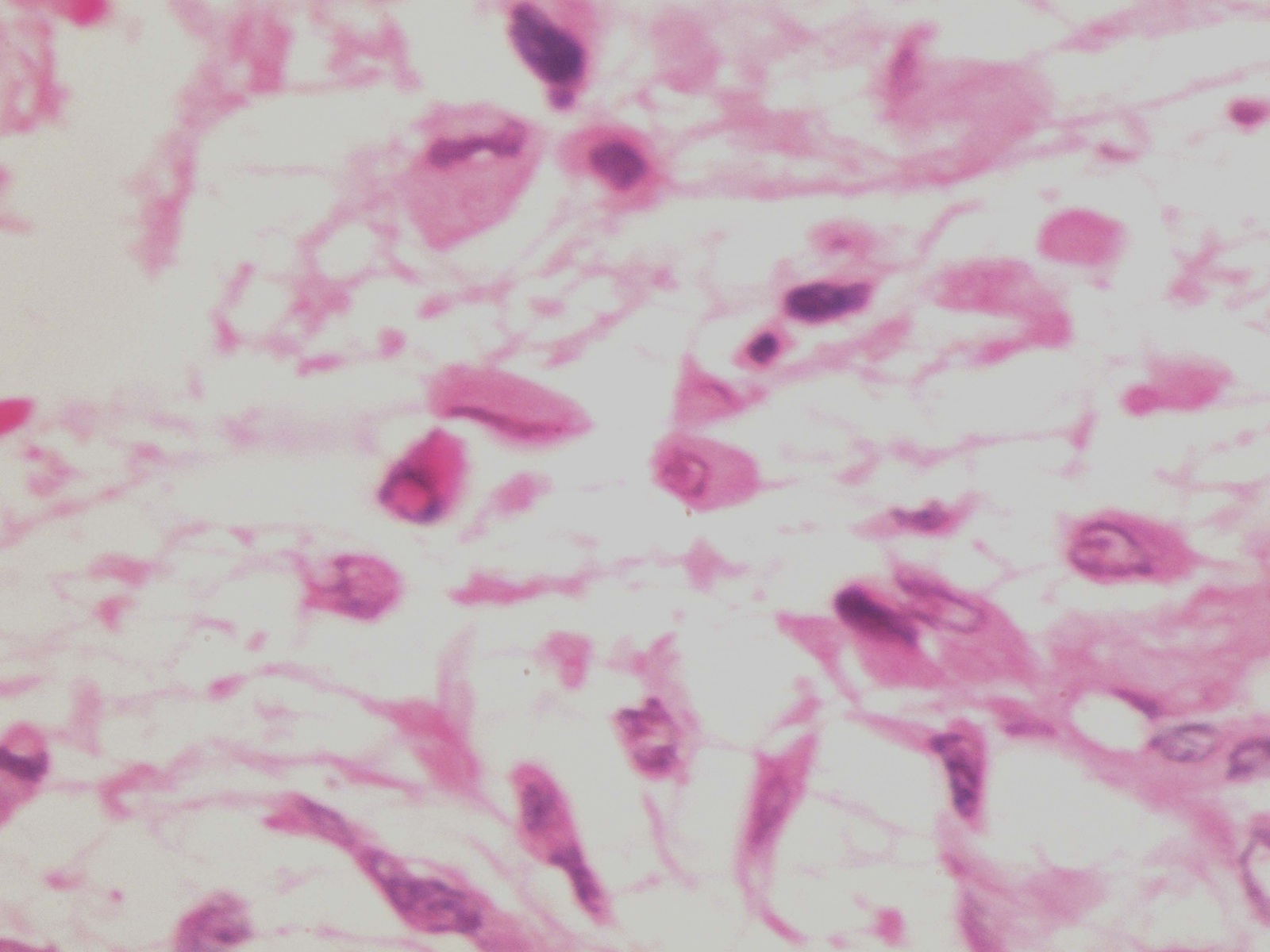
The excisional biopsy showed a multinodular tumor with dense and loose myxoid areas, hyaline stroma and chronic inflammatory cells. Pleomorphic epithelioid cells with irregular smudgy and vesicular nuclei were also seen (images 10 - 13, 15). Focal necrosis was noted (image 14).
Acral myxoinflammatory fibroblastic sarcoma is an uncommon low grade sarcoma of the hands and feet, first described in 1998 by Montgomery et al and Meis-Kindblom and Kindblom (Mod Pathol 1998;11:384, Am J Surg Pathol 1998;22:911). It is composed of myxoid stroma, inflammation and virocyte-like cells. It is also called inflammatory myxohyaline tumor of the distal extremities with virocyte or Reed-Sternberg-like cells. It affects men and women of all ages with a slow growing mass, usually in the hands or feet (J Cutan Pathol 2008;35:192).
Grossly, it is usually small, multinodular and poorly defined, often involving the joints and tendons. The cut surface is white and gelatinous with fibrous and myxoid zones. The distinctive histologic feature is myxoid extracellular matrix with various types of tumor cells:
In addition, there are acute or chronic inflammatory cells and areas of fibrosis or hyalinized stroma. Recently a consistent translocation t(1;10) with rearrangements of TGFBR3 and MGEA5 was found in both myxoinflammatory fibroblastic sarcoma and hemosiderotic fibrolipomatous tumor, suggesting a shared pathogenetic relationship (Genes Chromosomes Cancer 2011;50:757).
The differential diagnosis includes:
Treatment is wide local excision with or without radiation therapy. Acral myxoinflammatory fibroblastic sarcoma frequently recurs locally but distant metastases are rare (Am J Surg Pathol 2014;38:1).
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Wafaey Mohamed, Sharurah Armed Forces Hospital (Saudi Arabia), for contributing this case.

Save the Date!
Saturday, February 22, 2014
The Townsend Hotel
Birmingham, Michigan (USA)
Current Concepts in
GYN Oncology and Pathology

Sponsored by Karmanos Cancer Institute, Henry Ford Health System,
Wayne State University School of Medicine and the Detroit Medical Center

Course Director:
Rouba Ali-Fehmi, M.D.
Website
Hotel
Registration
For more information, please call (313) 745-3594 or
email wsupathology@gmail.com
Website news:
(1) Happy New Year! In 2013, we again had record traffic, with 4.9 million visits, an increase of 24% from the prior record in 2012. We also had a 52% increase in website page views to 15.6 million. Finally, we sold a record 1396 books (including 64 Kindle eBooks) totaling $180,000 through our affiliation with Amazon.com. Thanks for your support and suggestions on how to make PathologyOutlines.com a better resource for the pathology community.
(2) How is the Pathologist Job Market? Click here or on the Jobs Page link to see our new Pathology Jobs Report. This report contains an analysis of the 72 job ads posted at PathologyOutlines.com for the 4th quarter of 2013, including Job requirements, jobs by regions and specialties sought. We will continue to issue reports quarterly, but also to add reports from prior quarters for comparison.
(3) Thanks to Dr. Abdulaziz Mohamed, Nairobi, Kenya for contributing cytology images of Breast ductal carcinoma, NOS.
(4) We continue to add new Board Review questions every 1 - 2 months, courtesy of BoardVitals, which are accessible via our CME page.
Visit and follow our Blog to see recent updates to the website.
(1) Happy New Year! In 2013, we again had record traffic, with 4.9 million visits, an increase of 24% from the prior record in 2012. We also had a 52% increase in website page views to 15.6 million. Finally, we sold a record 1396 books (including 64 Kindle eBooks) totaling $180,000 through our affiliation with Amazon.com. Thanks for your support and suggestions on how to make PathologyOutlines.com a better resource for the pathology community.
(2) How is the Pathologist Job Market? Click here or on the Jobs Page link to see our new Pathology Jobs Report. This report contains an analysis of the 72 job ads posted at PathologyOutlines.com for the 4th quarter of 2013, including Job requirements, jobs by regions and specialties sought. We will continue to issue reports quarterly, but also to add reports from prior quarters for comparison.
(3) Thanks to Dr. Abdulaziz Mohamed, Nairobi, Kenya for contributing cytology images of Breast ductal carcinoma, NOS.
(4) We continue to add new Board Review questions every 1 - 2 months, courtesy of BoardVitals, which are accessible via our CME page.
Visit and follow our Blog to see recent updates to the website.
Case #296
Clinical history:
A 28 year old woman presented with a tender, firm nodule on her right big toe measuring 2 x 2 cm, with normal colored overlying skin. An Xray showed no bony changes of the big toe. An excisional biopsy was performed, and received as 2 irregular grayish pieces of tissue.
Microscopic images:
What is your diagnosis?
Click here for diagnosis and discussion:
Diagnosis: Acral myxoinflammatory fibroblastic sarcoma (myxoinflammatory fibroblastic sarcoma of soft tissue)
Discussion:
The excisional biopsy showed a multinodular tumor with dense and loose myxoid areas, hyaline stroma and chronic inflammatory cells. Pleomorphic epithelioid cells with irregular smudgy and vesicular nuclei were also seen (images 10 - 13, 15). Focal necrosis was noted (image 14).
Acral myxoinflammatory fibroblastic sarcoma is an uncommon low grade sarcoma of the hands and feet, first described in 1998 by Montgomery et al and Meis-Kindblom and Kindblom (Mod Pathol 1998;11:384, Am J Surg Pathol 1998;22:911). It is composed of myxoid stroma, inflammation and virocyte-like cells. It is also called inflammatory myxohyaline tumor of the distal extremities with virocyte or Reed-Sternberg-like cells. It affects men and women of all ages with a slow growing mass, usually in the hands or feet (J Cutan Pathol 2008;35:192).
Grossly, it is usually small, multinodular and poorly defined, often involving the joints and tendons. The cut surface is white and gelatinous with fibrous and myxoid zones. The distinctive histologic feature is myxoid extracellular matrix with various types of tumor cells:
- Epithelioid or spindled: occasionally large with bizarre nuclei and prominent nucleoli resembling viral inclusions or Reed-Sternberg cells
- Pseudolipoblasts: multivacuolated cells resembling pleomorphic lipoblasts due to cytoplasmic vacuoles containing myxoid material
- Giant cells with emperipolesis: minimal mitotic activity (0 - 1 MF/10 HPF), no atypical forms, no / rare necrosis.
In addition, there are acute or chronic inflammatory cells and areas of fibrosis or hyalinized stroma. Recently a consistent translocation t(1;10) with rearrangements of TGFBR3 and MGEA5 was found in both myxoinflammatory fibroblastic sarcoma and hemosiderotic fibrolipomatous tumor, suggesting a shared pathogenetic relationship (Genes Chromosomes Cancer 2011;50:757).
The differential diagnosis includes:
- Epithelioid sarcoma: most cells are round with dense eosinophilic cytoplasm, strongly keratin+, loss of INI1 (SMARCB)
- Hodgkin lymphoma: lacks giant cells and lipoblast-like cells, tumor cells have different staining patterns (CD15+ and CD30+ in classic Hodgkin lymphoma)
- Myxofibrosarcoma: (formerly called myxoid MFH); rare in soft tissues of hands and feet, more frequent mitotic figures with atypical forms, no inflammatory infiltrate
- Pleomorphic liposarcoma: true pleomorphic lipoblasts, rare in soft tissues of hands and feet, more frequent mitotic figures with atypical forms, no inflammatory infiltrate
- Rosai-Dorfman disease: emperipolesis, but no intranuclear viral-like inclusions, S100+, usually not myxoid
- Tenosynovitis: no enlarged atypical cells
Treatment is wide local excision with or without radiation therapy. Acral myxoinflammatory fibroblastic sarcoma frequently recurs locally but distant metastases are rare (Am J Surg Pathol 2014;38:1).
