
14 February 2018 - Case of the Week #475
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Week page. To subscribe or unsubscribe to Case of the Week or our other email lists, click here.
Thanks to Drs. Saroona Haroon and Saifaldin M. Alzain, King Fahad Specialist Hospital, Dammam (Saudi Arabia) for contributing this case and Dr. Raul S. Gonzalez, Beth Israel Deaconess Medical Center, Boston, Massachusetts (USA) for writing the discussion. To contribute a Case of the Week, first make sure that we are currently accepting cases, then follow the guidelines on our main Case of the Week page.
Advertisement
Case of the Week #475
Clinical history:
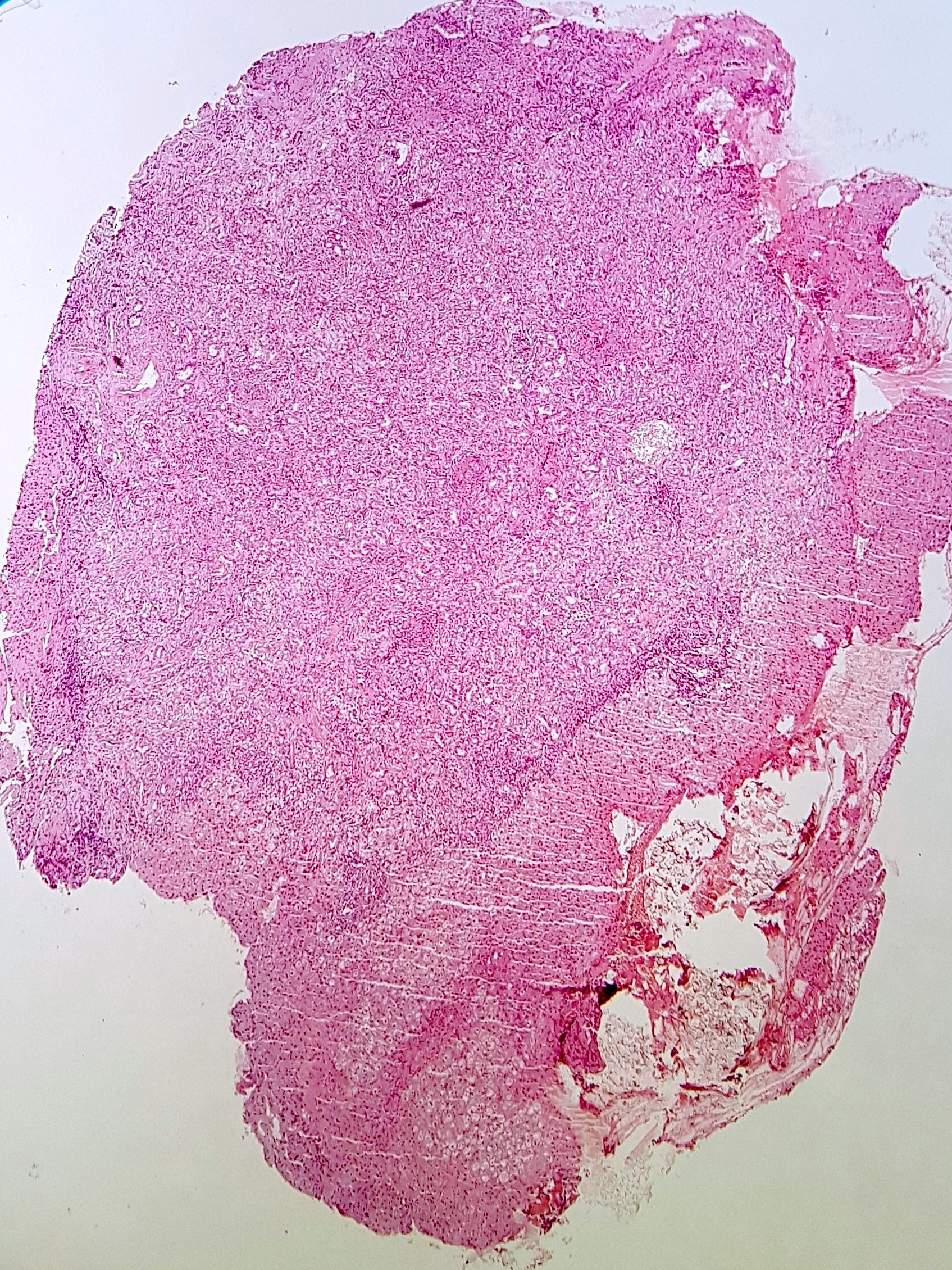
A 44 year old man had a laparoscopic cholecystectomy for gallstones. An incidental nodule on the anterior surface of the liver was excised.
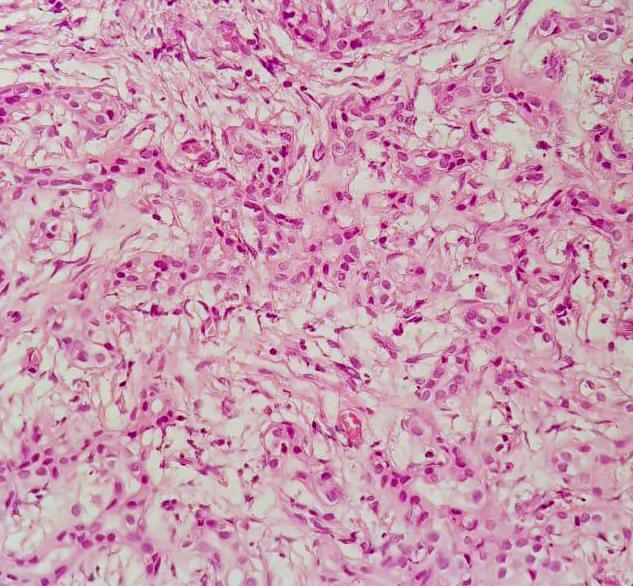
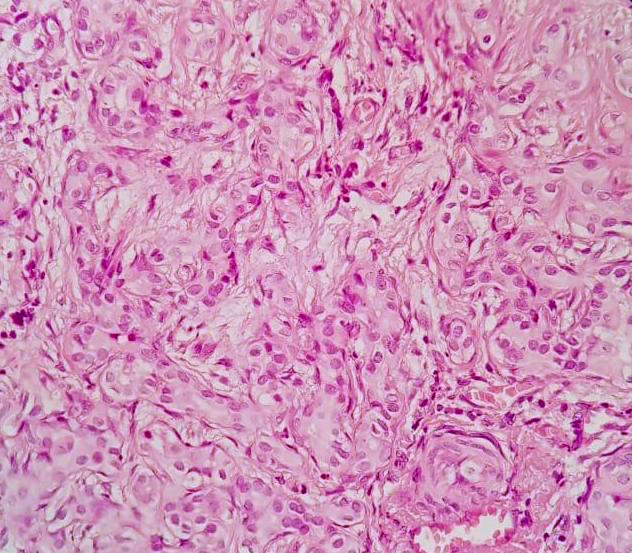
Histopathology images:



What is your diagnosis?
Diagnosis:
Bile duct adenoma
Test question (answer at the end):
Which of the following is true about these lesions?
A. May show a lymphocytic cuff
B. May show prominent nuclear atypia
C. Typically >1 cm in size
D. Typically multifocal
Stains:
Discussion:
Bile duct adenoma is also termed peribiliary gland hamartoma, although it may actually be a localized response to injury (Am J Surg Pathol 2010;34:1312). It is benign, often solitary and generally an incidental mass in the liver, most commonly seen in adults. It is often a small (1 cm or less), subcapsular whitish nodule on the surface of the liver.
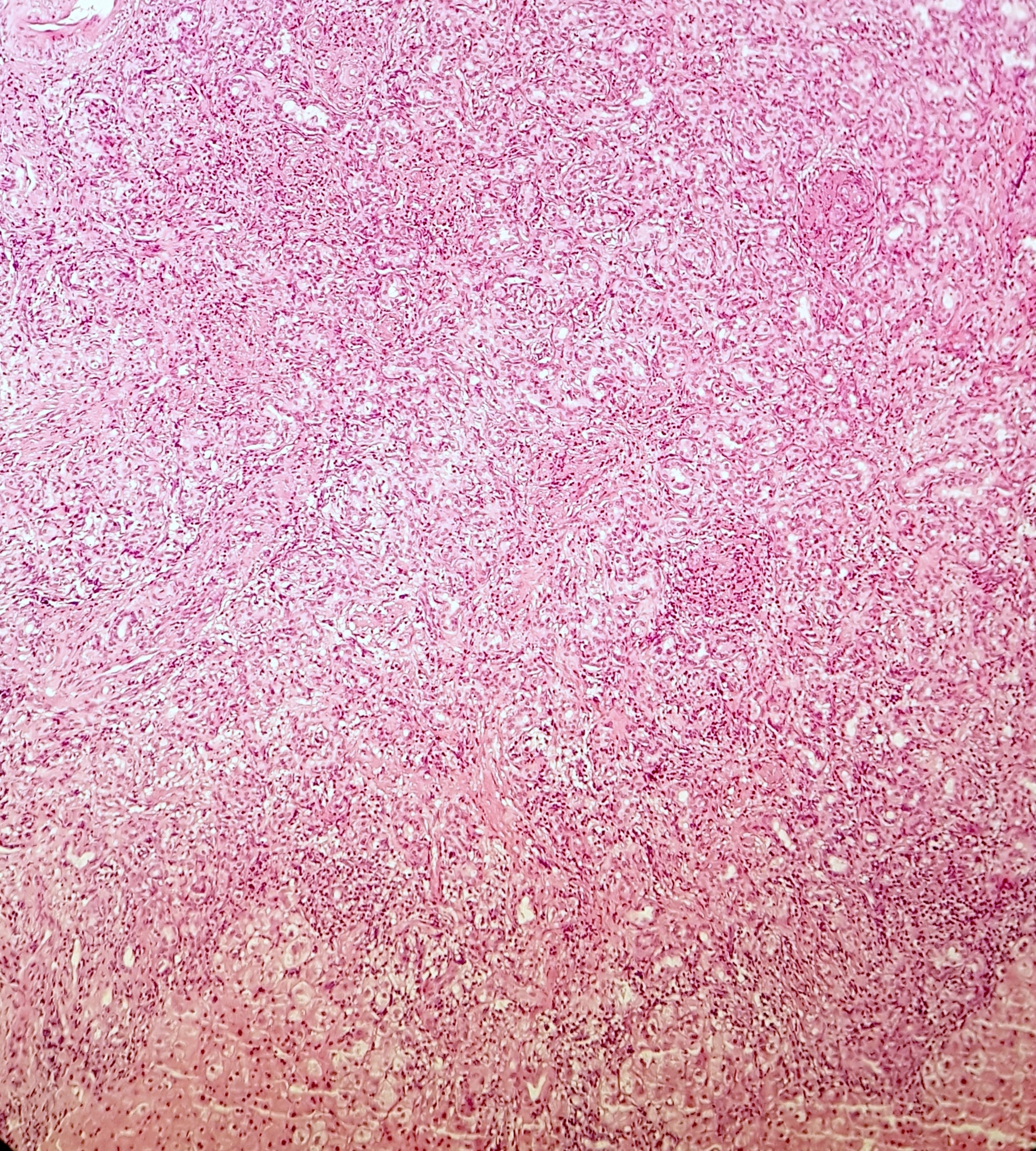
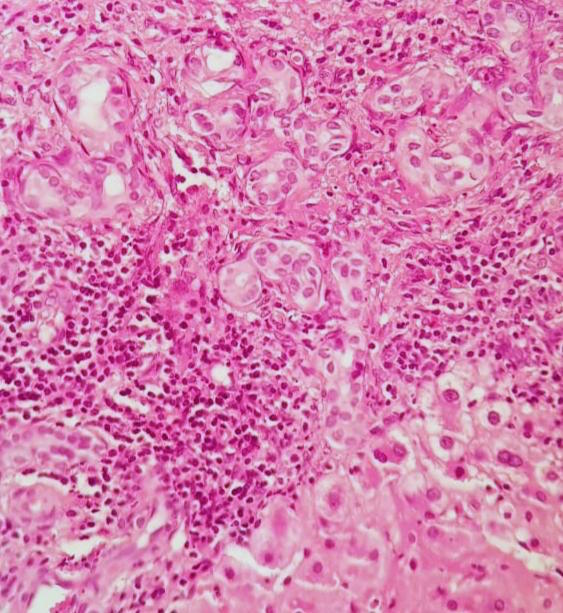
Histologically, bile duct adenoma has well circumscribed nests of bland, curvilinear ducts / ductules with minimal lumens. The cells show abundant cytoplasm and pale nuclei and the background is fibrotic but not desmoplastic. A lymphocytic response may be seen cuffing or infiltrating the mass. Rarely, globules of alpha-1-antitrypsin may be present (Int J Surg Pathol 2008;16:218).
By immunohistochemistry, the epithelial cells are positive for CK7, CK19 and EMA, with a wild type p53 staining pattern (occasional scattered positive cells). Features suggesting malignancy (cytologic atypia, necrosis, architectural complexity) are generally absent, though "atypical bile duct adenoma" with mild nuclear atypia, cleared out cytoplasm and focal parenchymal infiltration has been described (Am J Surg Pathol 2001;25:956).
Bile duct adenoma is generally easy to diagnose on routine histology but can be confused with well differentiated cholangiocarcinoma on frozen section. These are usually larger than 1 cm and are typically not circumscribed. Bile duct hamartoma (von Meyenburg complex) is typically even smaller (< 0.5 cm) and shows glands that are angulated, less densely packed and filled with inspissated bile.
Test question answer:
A. May show a lymphocytic cuff
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Week page. To subscribe or unsubscribe to Case of the Week or our other email lists, click here.
Thanks to Drs. Saroona Haroon and Saifaldin M. Alzain, King Fahad Specialist Hospital, Dammam (Saudi Arabia) for contributing this case and Dr. Raul S. Gonzalez, Beth Israel Deaconess Medical Center, Boston, Massachusetts (USA) for writing the discussion. To contribute a Case of the Week, first make sure that we are currently accepting cases, then follow the guidelines on our main Case of the Week page.
Advertisement
Case of the Week #475
Clinical history:
A 44 year old man had a laparoscopic cholecystectomy for gallstones. An incidental nodule on the anterior surface of the liver was excised.
Histopathology images:
What is your diagnosis?
Diagnosis:
Bile duct adenoma
Test question (answer at the end):
Which of the following is true about these lesions?
A. May show a lymphocytic cuff
B. May show prominent nuclear atypia
C. Typically >1 cm in size
D. Typically multifocal
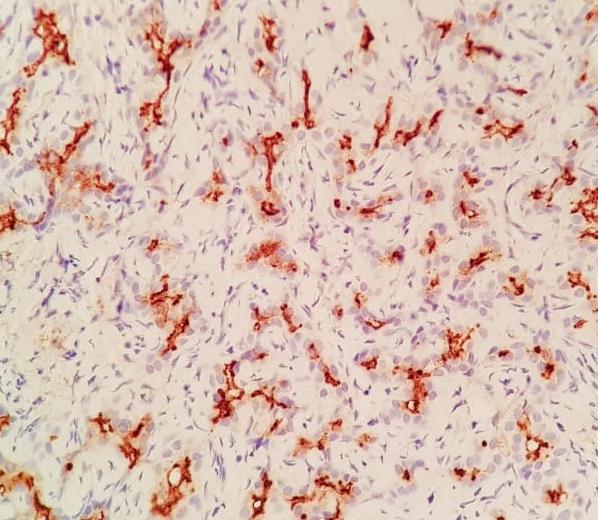
Stains:
EMA
Discussion:
Bile duct adenoma is also termed peribiliary gland hamartoma, although it may actually be a localized response to injury (Am J Surg Pathol 2010;34:1312). It is benign, often solitary and generally an incidental mass in the liver, most commonly seen in adults. It is often a small (1 cm or less), subcapsular whitish nodule on the surface of the liver.
Histologically, bile duct adenoma has well circumscribed nests of bland, curvilinear ducts / ductules with minimal lumens. The cells show abundant cytoplasm and pale nuclei and the background is fibrotic but not desmoplastic. A lymphocytic response may be seen cuffing or infiltrating the mass. Rarely, globules of alpha-1-antitrypsin may be present (Int J Surg Pathol 2008;16:218).
By immunohistochemistry, the epithelial cells are positive for CK7, CK19 and EMA, with a wild type p53 staining pattern (occasional scattered positive cells). Features suggesting malignancy (cytologic atypia, necrosis, architectural complexity) are generally absent, though "atypical bile duct adenoma" with mild nuclear atypia, cleared out cytoplasm and focal parenchymal infiltration has been described (Am J Surg Pathol 2001;25:956).
Bile duct adenoma is generally easy to diagnose on routine histology but can be confused with well differentiated cholangiocarcinoma on frozen section. These are usually larger than 1 cm and are typically not circumscribed. Bile duct hamartoma (von Meyenburg complex) is typically even smaller (< 0.5 cm) and shows glands that are angulated, less densely packed and filled with inspissated bile.
Test question answer:
A. May show a lymphocytic cuff
