
12 June 2019 - Case of the Month #480 (revised 15 June 2020)
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Aung Phyo, Mawlamyine General Hospital (Myanmar) for contributing this case; Dr. Katrina Krogh, Northwestern University McGaw Medical Center and Feinberg School of Medicine, Chicago, Illinois (USA), for writing the discussion; and Dr. Debra Zynger, The Ohio State University, Columbus, Ohio (USA), for the Editorial Board review. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.
Case of the Month #480
Clinical history:
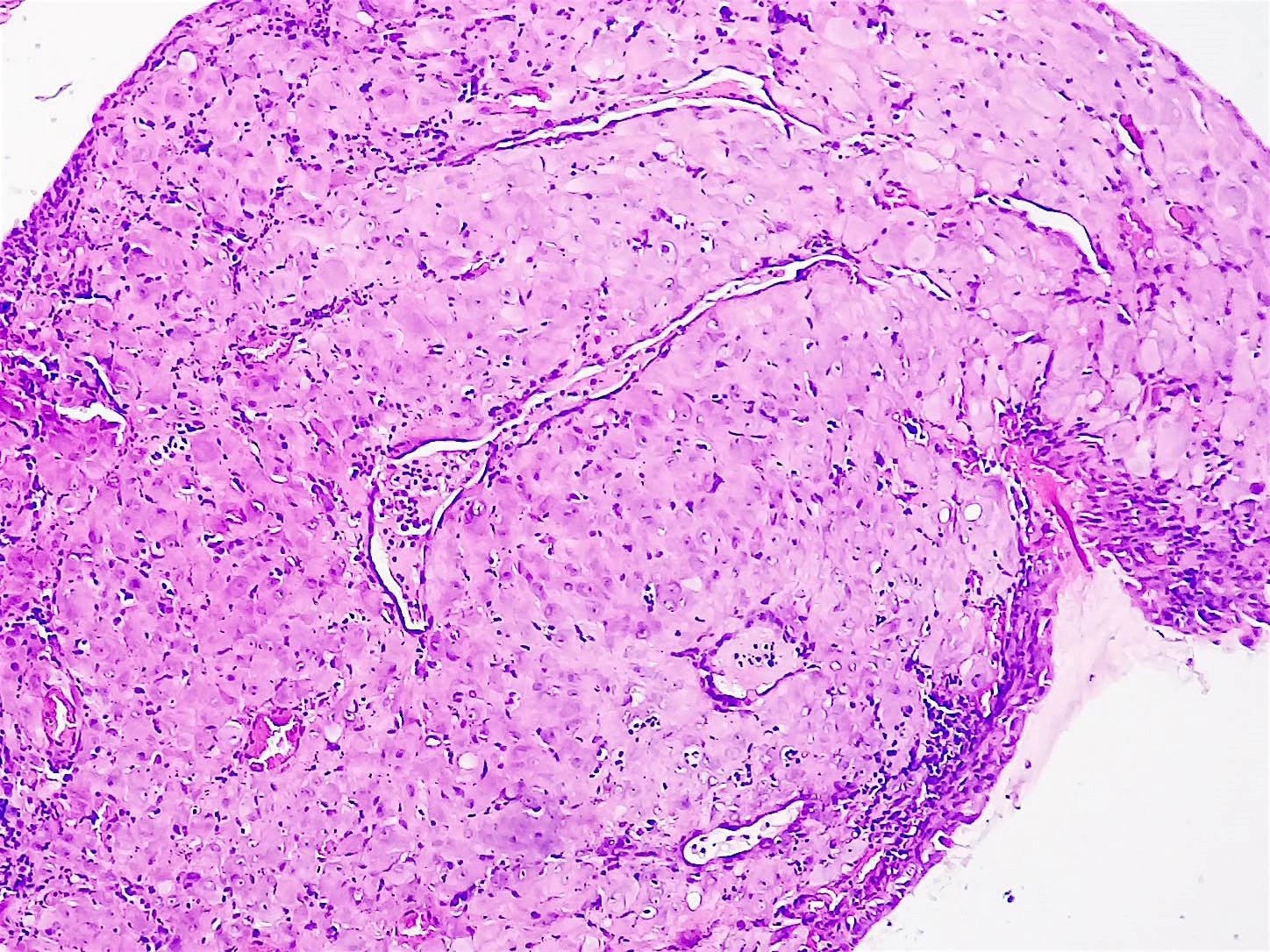
A 35 year old pregnant woman presented with a growing nodule on the cervix.
Histopathology images:
What is your diagnosis?
Diagnosis:
Cervical deciduosis
Test question (answer at the end):
Which of the following is true about cervical deciduosis?
A. Cervical deciduosis is a dysplastic change in the cervix.
B. The true incidence of cervical deciduosis is unknown but it is thought to be common during pregnancy.
C. Gross examination allows a straightforward assessment of cervical deciduosis versus other entities in the cervix.
D. Deciduosis, also known as ectopic deciduosis, has only been reported in gynecologic organs.
Discussion:
Cervical deciduosis, also called ectopic decidua of the cervix, refers to the benign histologic finding of decidualized cervical stromal cells that sometimes occurs during normal pregnancy and usually resolves 4 - 6 weeks postpartum. Patients typically present with small, elevated, vascular nodules or, less commonly, sessile polyps. Often no symptoms are present. The presence of cervical deciduosis can mimic dysplasia or invasive carcinoma in both gross and microscopic appearance; therefore, it is an important entity to recognize (BMJ Case Rep 2015;2015).
Decidual change in the uterine stroma is a normal progesterone induced adaption to allow implantation during pregnancy. The etiology of ectopic deciduosis is unclear but multiple theories have been proposed. The most accepted theory is that cervical stroma undergoes metaplasia in response to progesterone stimulation (J Natl Med Assoc 1979;71:787). Endometriosis with subsequent stromal decidualization is also a possible source. Another theory is that a primordial stromal cell that undergoes decidualization is already present in multiple locations (Am J Surg Pathol 1987;11:526).
Decidual changes in locations other than the endometrium are most commonly reported in the cervix, vagina (Am J Obstet Gynecol 1949;58:743) and ovary (Obstet Gynecol 1954;3:399). However, decidual changes have also been reported in the omentum, appendix, lymph nodes, uterine viscera, peritoneum and diaphragm (Orv Hetil 2008;149:329, Am J Gastroenterol 1990;85:841, Pathol Res Pract 1993;189:352, American Journal of Obstetrics and Gynecology 1929;17:603, J Reprod Med 1983;28:430). The prevalence of ectopic deciduosis is not well known but it is thought to be common. One study found ectopic decidual reaction in 30.8% of 191 uteri removed during pregnancy based on histology (Acta Cytol 1981;25:616).
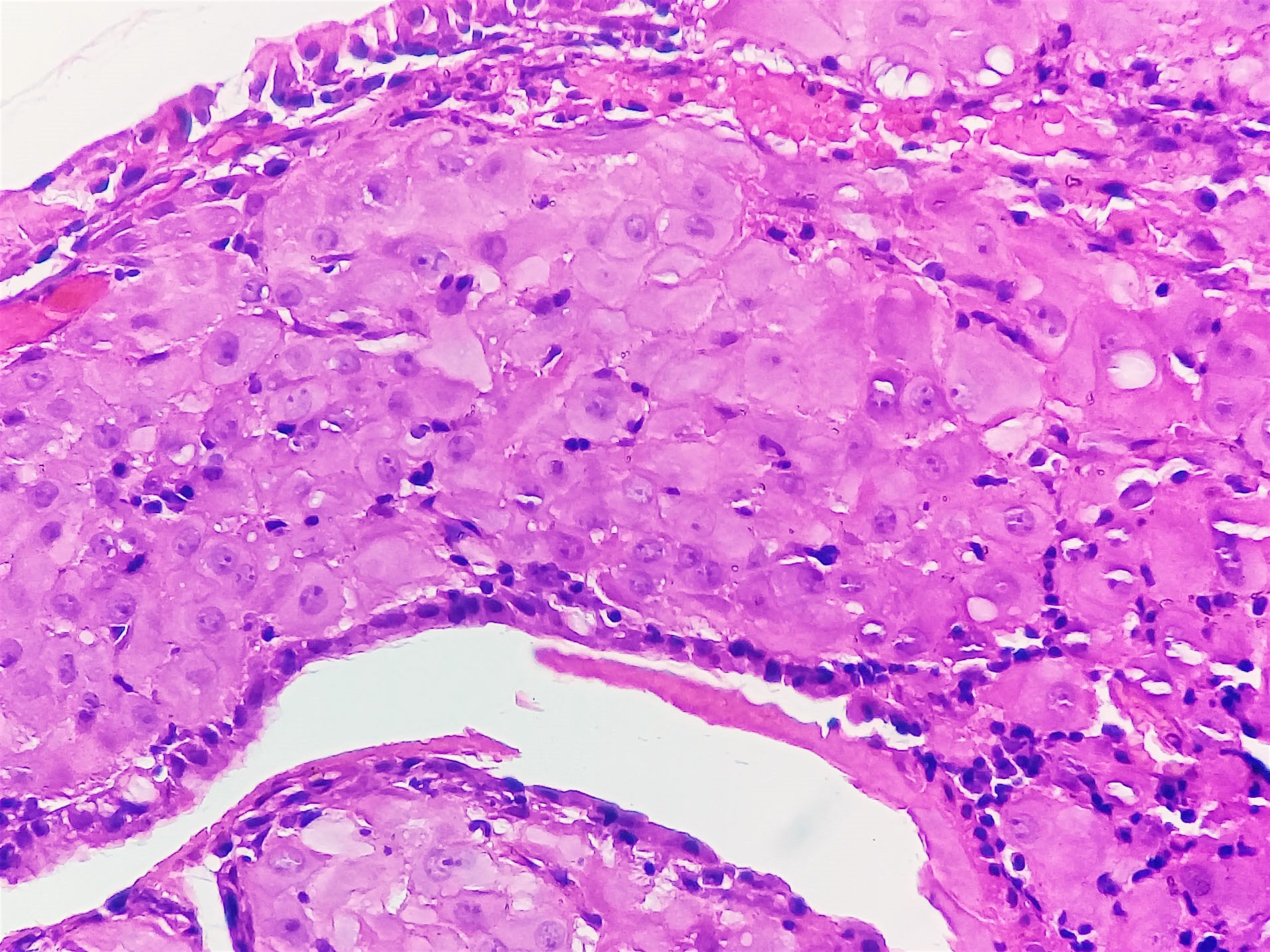
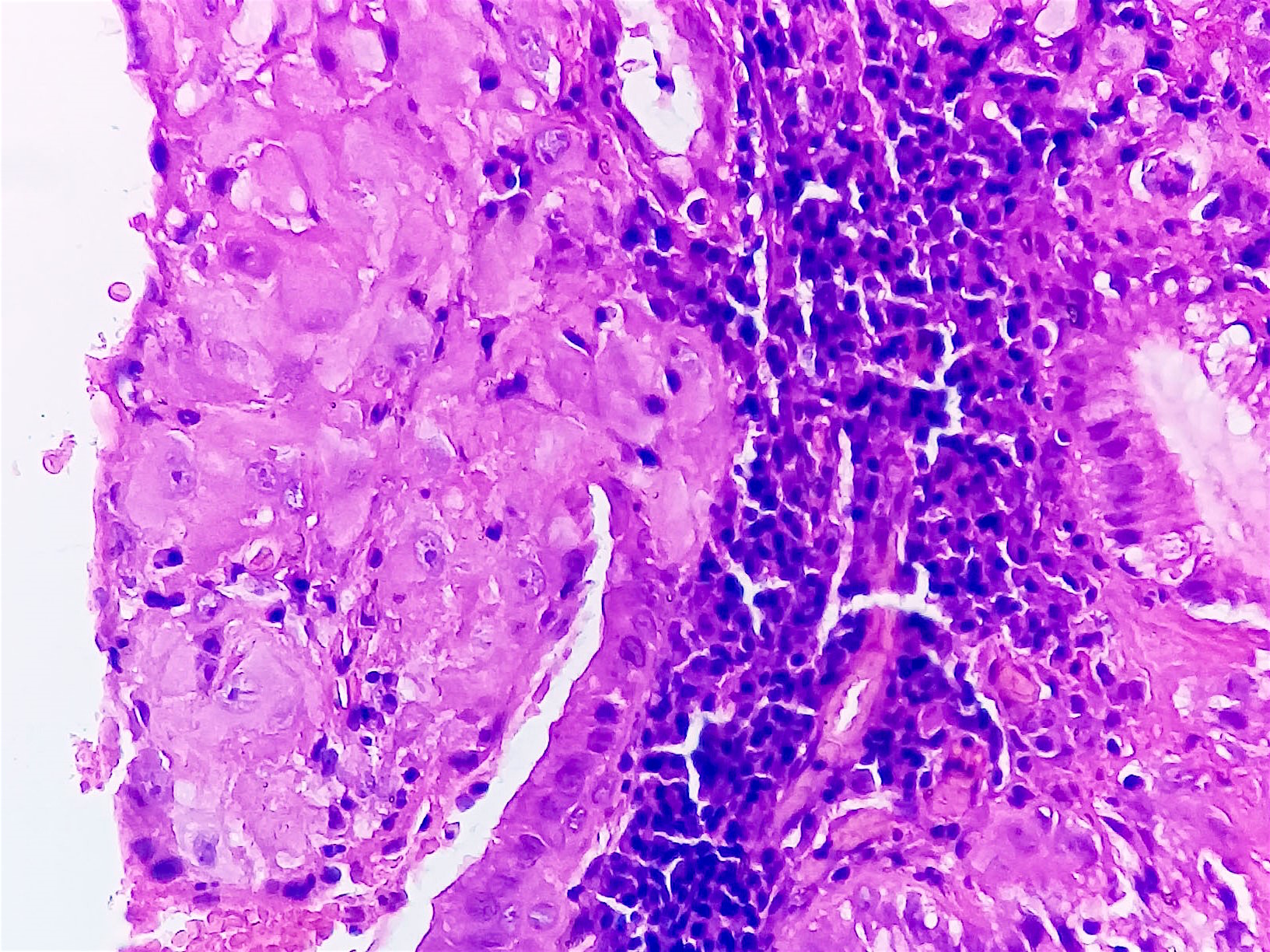
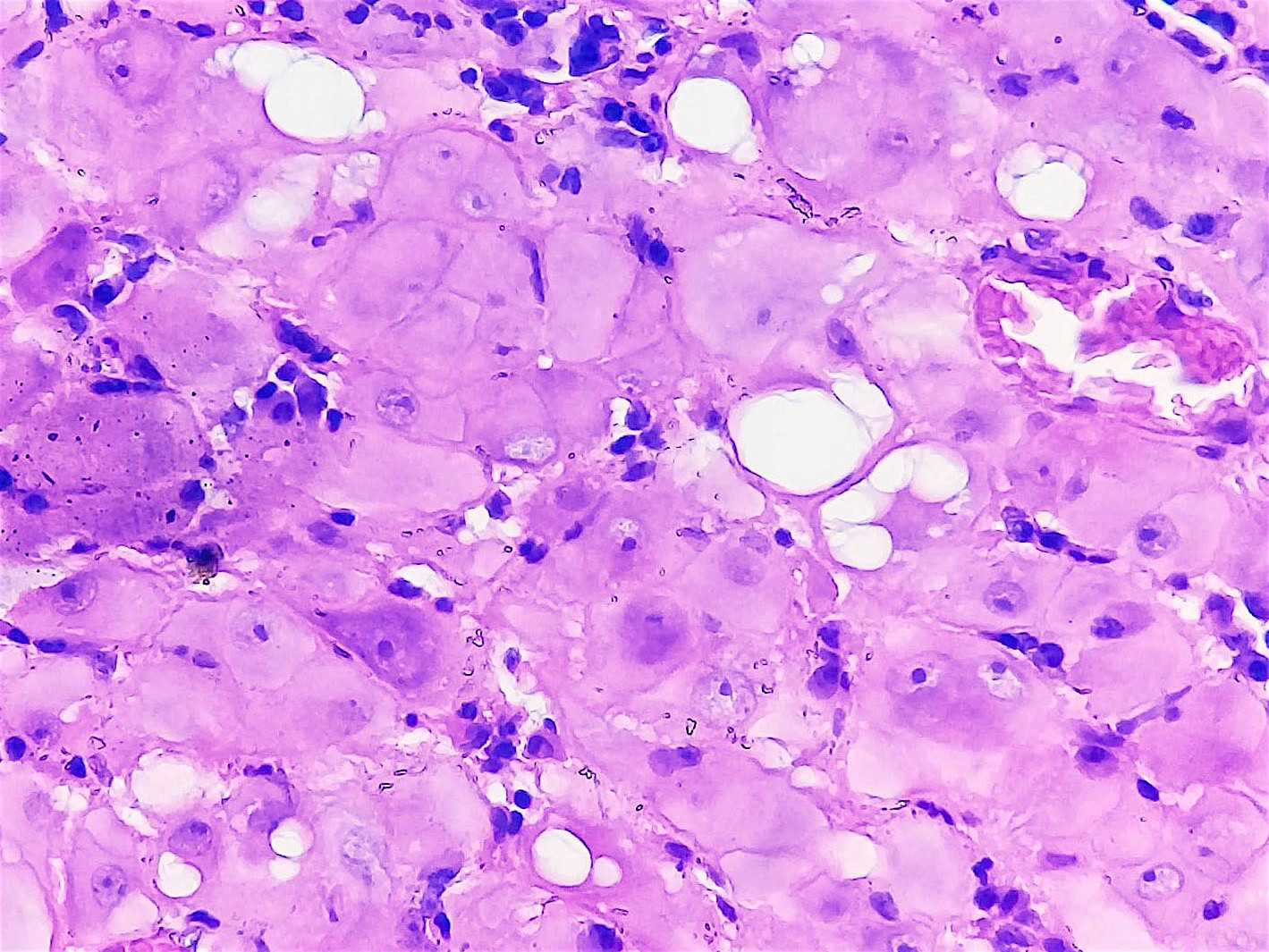
Ectopic deciduosis is usually found incidentally during pregnancy, such as during cesarean delivery, appendectomy or Pap smear. Histologic examination usually confirms the final diagnosis. Histologic examination of the lesions can sometimes be difficult to interpret and can look very similar to invasive carcinoma (BJOG 2000;107:573). Furthermore, cervical intraepithelial neoplasia can coexist with deciduosis (BMJ Case Rep 2015;2015). Characteristic histologic features are poorly demarcated clusters of enlarged stromal cells with abundant eosinophilic-to-amphophilic cytoplasm (with or without vacuoles) within the cervical wall (usually subepithelial). There is frequent disruption of the overlying epithelium. Characteristic cytologic findings are aggregates of small nucleoli and marked nuclear enlargement (Acta Cytol 1981;25:616).
The differential diagnosis for cervical deciduosis includes tissue repair, cervical polyp or adenoma, squamous intraepithelial lesions (LSIL and HSIL) and squamous cell carcinoma. Several features point to cervical deciduosis versus dysplasia or carcinoma. These include: 1) normal cervical cytology, 2) the absence of abnormalities during colposcopy, 3) uniform nuclear cytomorphology, 4) absence of mitoses and 5) location outside the transformation zone (BMJ Case Rep 2015;2015). In addition, stains can help rule out other entities. Decidual changes are positive for CD10 and negative for EMA and cytokeratin. Other entities to consider are squamous cell carcinoma (EMA, cytokeratin positive), placental site trophoblastic tumor (cytokeratin, inhibin and MEL-CAM (CD146) positive), signet ring cell carcinoma (EMA and cytokeratin positive) and granulomatous inflammation (CD10 negative, CD68 positive).
Test question answer:
B. Since cervical deciduosis is often detected incidentally and is usually asymptomatic, the true incidence is unknown. However, studies have shown the incidence may be as high as 34% of pregnancies.
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Dr. Aung Phyo, Mawlamyine General Hospital (Myanmar) for contributing this case; Dr. Katrina Krogh, Northwestern University McGaw Medical Center and Feinberg School of Medicine, Chicago, Illinois (USA), for writing the discussion; and Dr. Debra Zynger, The Ohio State University, Columbus, Ohio (USA), for the Editorial Board review. This case was reviewed in May 2020 by Dr. Jennifer Bennett, University of Chicago and Dr. Carlos Parra-Herran, University of Toronto.

Advertisement
Case of the Month #480
Clinical history:
A 35 year old pregnant woman presented with a growing nodule on the cervix.
Histopathology images:
What is your diagnosis?
Diagnosis:
Cervical deciduosis
Test question (answer at the end):
Which of the following is true about cervical deciduosis?
A. Cervical deciduosis is a dysplastic change in the cervix.
B. The true incidence of cervical deciduosis is unknown but it is thought to be common during pregnancy.
C. Gross examination allows a straightforward assessment of cervical deciduosis versus other entities in the cervix.
D. Deciduosis, also known as ectopic deciduosis, has only been reported in gynecologic organs.
Discussion:
Cervical deciduosis, also called ectopic decidua of the cervix, refers to the benign histologic finding of decidualized cervical stromal cells that sometimes occurs during normal pregnancy and usually resolves 4 - 6 weeks postpartum. Patients typically present with small, elevated, vascular nodules or, less commonly, sessile polyps. Often no symptoms are present. The presence of cervical deciduosis can mimic dysplasia or invasive carcinoma in both gross and microscopic appearance; therefore, it is an important entity to recognize (BMJ Case Rep 2015;2015).
Decidual change in the uterine stroma is a normal progesterone induced adaption to allow implantation during pregnancy. The etiology of ectopic deciduosis is unclear but multiple theories have been proposed. The most accepted theory is that cervical stroma undergoes metaplasia in response to progesterone stimulation (J Natl Med Assoc 1979;71:787). Endometriosis with subsequent stromal decidualization is also a possible source. Another theory is that a primordial stromal cell that undergoes decidualization is already present in multiple locations (Am J Surg Pathol 1987;11:526).
Decidual changes in locations other than the endometrium are most commonly reported in the cervix, vagina (Am J Obstet Gynecol 1949;58:743) and ovary (Obstet Gynecol 1954;3:399). However, decidual changes have also been reported in the omentum, appendix, lymph nodes, uterine viscera, peritoneum and diaphragm (Orv Hetil 2008;149:329, Am J Gastroenterol 1990;85:841, Pathol Res Pract 1993;189:352, American Journal of Obstetrics and Gynecology 1929;17:603, J Reprod Med 1983;28:430). The prevalence of ectopic deciduosis is not well known but it is thought to be common. One study found ectopic decidual reaction in 30.8% of 191 uteri removed during pregnancy based on histology (Acta Cytol 1981;25:616).
Ectopic deciduosis is usually found incidentally during pregnancy, such as during cesarean delivery, appendectomy or Pap smear. Histologic examination usually confirms the final diagnosis. Histologic examination of the lesions can sometimes be difficult to interpret and can look very similar to invasive carcinoma (BJOG 2000;107:573). Furthermore, cervical intraepithelial neoplasia can coexist with deciduosis (BMJ Case Rep 2015;2015). Characteristic histologic features are poorly demarcated clusters of enlarged stromal cells with abundant eosinophilic-to-amphophilic cytoplasm (with or without vacuoles) within the cervical wall (usually subepithelial). There is frequent disruption of the overlying epithelium. Characteristic cytologic findings are aggregates of small nucleoli and marked nuclear enlargement (Acta Cytol 1981;25:616).
The differential diagnosis for cervical deciduosis includes tissue repair, cervical polyp or adenoma, squamous intraepithelial lesions (LSIL and HSIL) and squamous cell carcinoma. Several features point to cervical deciduosis versus dysplasia or carcinoma. These include: 1) normal cervical cytology, 2) the absence of abnormalities during colposcopy, 3) uniform nuclear cytomorphology, 4) absence of mitoses and 5) location outside the transformation zone (BMJ Case Rep 2015;2015). In addition, stains can help rule out other entities. Decidual changes are positive for CD10 and negative for EMA and cytokeratin. Other entities to consider are squamous cell carcinoma (EMA, cytokeratin positive), placental site trophoblastic tumor (cytokeratin, inhibin and MEL-CAM (CD146) positive), signet ring cell carcinoma (EMA and cytokeratin positive) and granulomatous inflammation (CD10 negative, CD68 positive).
Test question answer:
B. Since cervical deciduosis is often detected incidentally and is usually asymptomatic, the true incidence is unknown. However, studies have shown the incidence may be as high as 34% of pregnancies.
