
19 August 2021 - Case of the Month #506
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Drs. Christopher Metter and Rajal Shah, UT Southwestern Medical Center, Dallas, Texas (USA) and the Genitourinary Pathology Society (GUPS) for contributing this case and the discussion and to Dr. Maria Tretiakova, University of Washington, Seattle, Washington (USA), for reviewing the discussion.
Advertisement
Case of the Month #506
Clinical history:
A man in his 50s presented with multiple bilateral renal masses up to 14.5 cm (left sided) and multiple pulmonary nodules. He underwent a left radical nephrectomy.
Histopathology images:

What is your diagnosis?
Diagnosis: Epithelioid angiomyolipoma
Test question (answer at the end):
Which is a true feature of epithelioid angiomyolipoma?
A. They are a common (>10%) variant of angiomyolipoma
B. Diagnosis requires at least 20% epithelioid cells
C. Tumors are almost always associated with tuberous sclerosis
D. Tumors may have malignant behavior
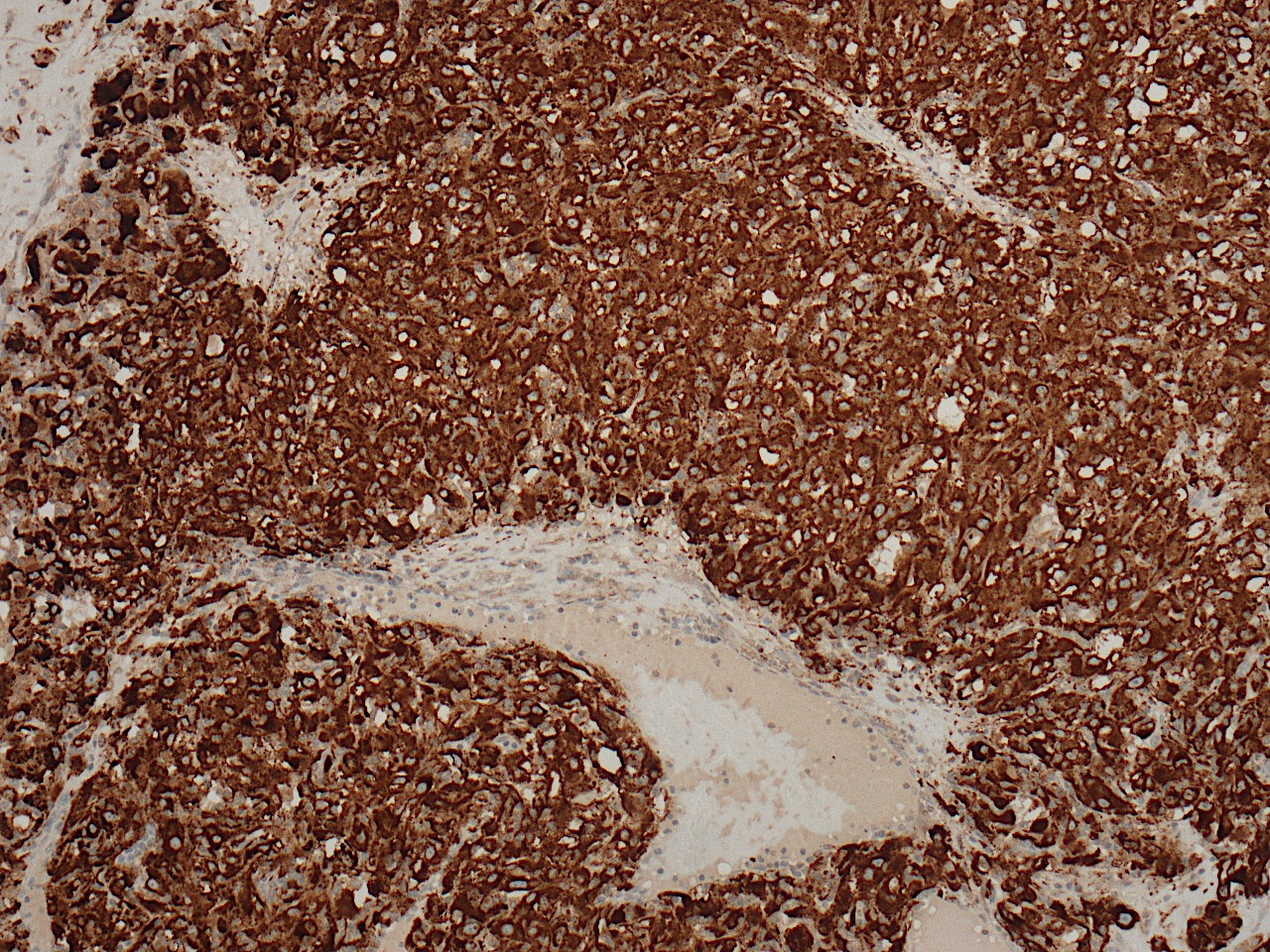
Stains:
Discussion:
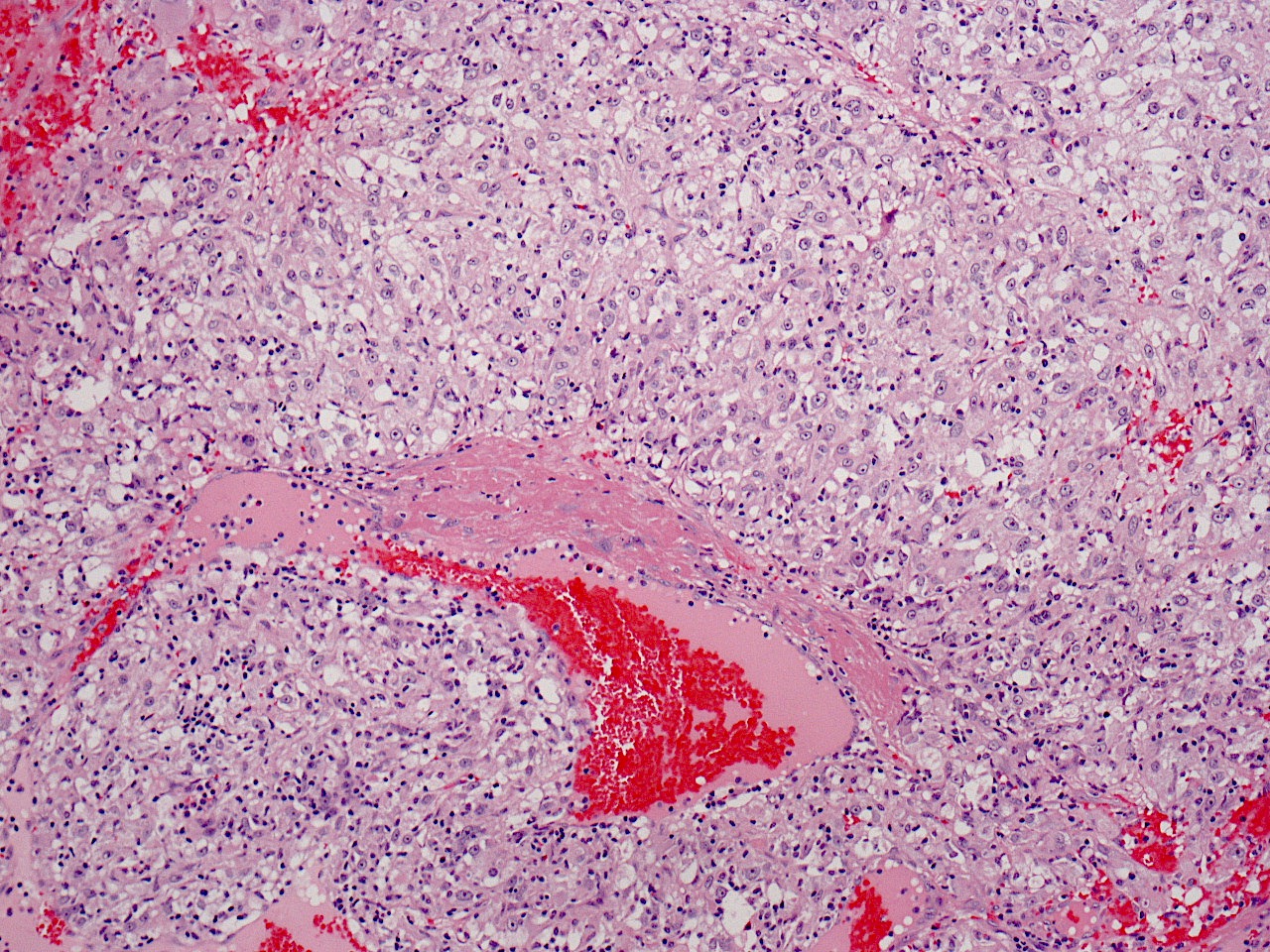
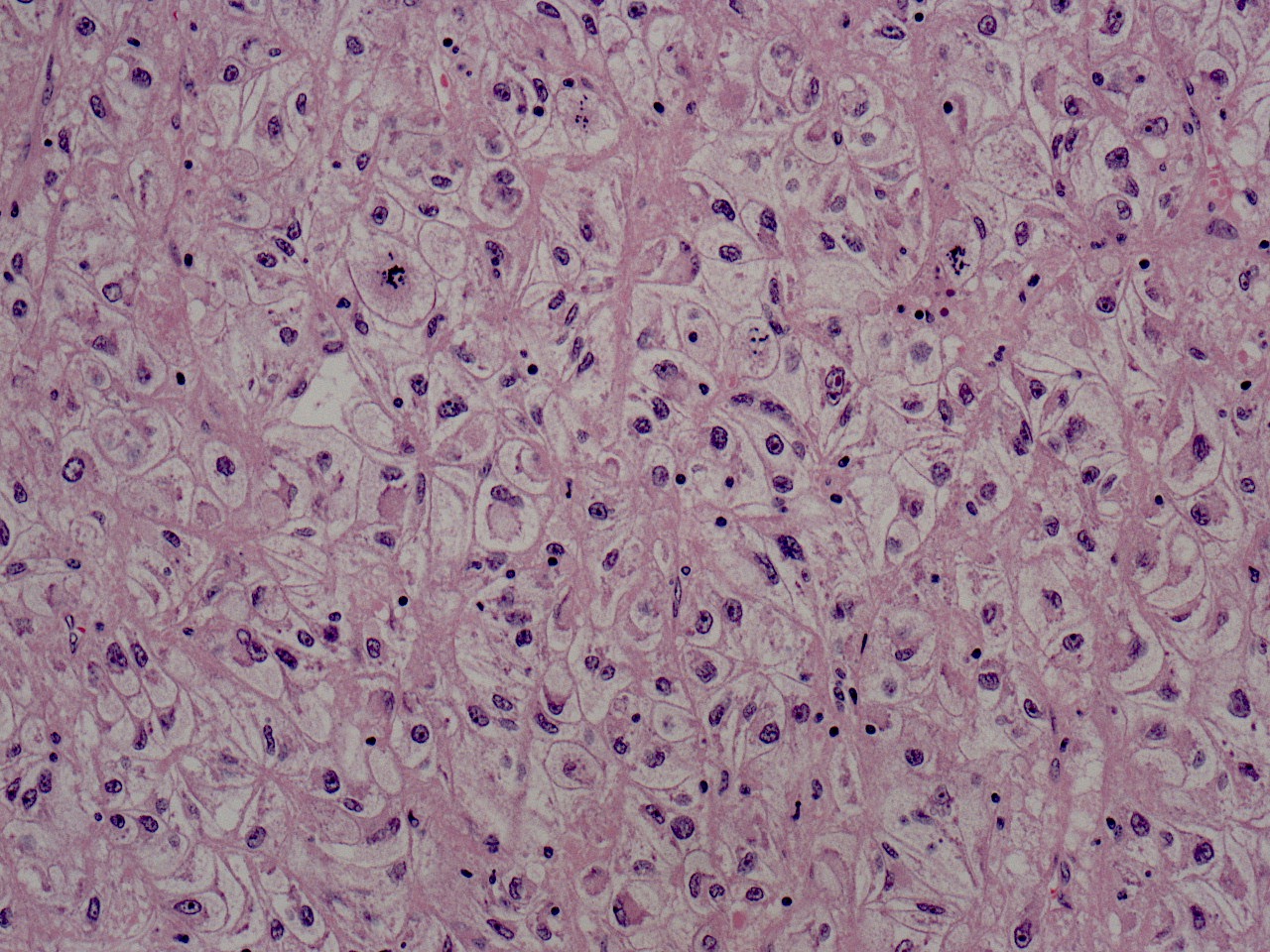
Epithelioid angiomyolipoma (eAML), also termed perivascular epithelioid cell tumor (PEComa), accounts for up to 5% of all angiomyolipomas (AML). Epithelioid cells are the defining feature of eAML, with the 2016 WHO classification requiring at least 80% of the tumor to be epithelioid to render the diagnosis. Epithelioid cells are enlarged, polygonal cells with eosinophilic or clear cytoplasm, atypical nuclei and prominent nucleoli (histopathology images 1 and 2). Two patterns of eAML have been described, the “carcinoma-like” pattern and the so called “epithelioid and plump spindled cells with diffuse growth” pattern. The “carcinoma-like” pattern (this case) manifests with a cohesive heterogeneous population of tumor cells arranged in compartmentalized sheets with intervening vasculature rich septa. When compared with the “carcinoma-like” pattern, the “epithelioid and plump spindled cells with diffuse growth” pattern is populated by a smaller in size and more monotonous collection of epithelioid and spindled cells arranged in tightly packed sheets. By immunohistochemistry, the tumors are immunoreactive for melanocytic markers (e.g. HMB45, MelanA, and microphthalmia transcription factor (MITF)), cathepsin K and smooth muscle markers.
Like classical angiomyolipoma, eAML has been described in patients both with and without evidence of tuberous sclerosis and in the TSC2/PKD1 contiguous gene syndrome. The examination of the background kidney provides important clues regarding this association. The presence of tumorlets (microscopic angiomyolipomas, H&E image 3 above) suggests an association with tuberous sclerosis in this patient.
It is important to recognize eAML because, in contrast to classical AML, it has malignant potential. Some have suggested that certain histologic features can predict the malignant potential of eAML, such as tumor size > 7 cm, presence of tuberous sclerosis syndrome, presence of the “carcinoma-like” pattern, invasion into perinephric fat or renal vein, necrosis, high mitotic count (> 2/10 HPF), older age at presentation and the presence of severely atypical cells (Am J Surg Pathol 2011;35:161). Others, more recently, have suggested that these features do not correlate with malignant potential and that the previous findings may have been related to the type of cases / population the previous studies had incorporated into their cohort (Mod Pathol 2013;26:1355, Moch: WHO Classification of Tumours of the Urinary System and Male Genital Organs, Fourth Edition, 2016).
Test question answer:
D. Tumors may have malignant behavior
All cases are archived on our website. To view them sorted by case number, diagnosis or category, visit our main Case of the Month page. To subscribe or unsubscribe to Case of the Month or our other email lists, click here.
Thanks to Drs. Christopher Metter and Rajal Shah, UT Southwestern Medical Center, Dallas, Texas (USA) and the Genitourinary Pathology Society (GUPS) for contributing this case and the discussion and to Dr. Maria Tretiakova, University of Washington, Seattle, Washington (USA), for reviewing the discussion.
Advertisement
Case of the Month #506
Clinical history:
A man in his 50s presented with multiple bilateral renal masses up to 14.5 cm (left sided) and multiple pulmonary nodules. He underwent a left radical nephrectomy.
Histopathology images:
What is your diagnosis?
Click here for diagnosis, test question and discussion:
Diagnosis: Epithelioid angiomyolipoma
Test question (answer at the end):
Which is a true feature of epithelioid angiomyolipoma?
A. They are a common (>10%) variant of angiomyolipoma
B. Diagnosis requires at least 20% epithelioid cells
C. Tumors are almost always associated with tuberous sclerosis
D. Tumors may have malignant behavior
Stains:
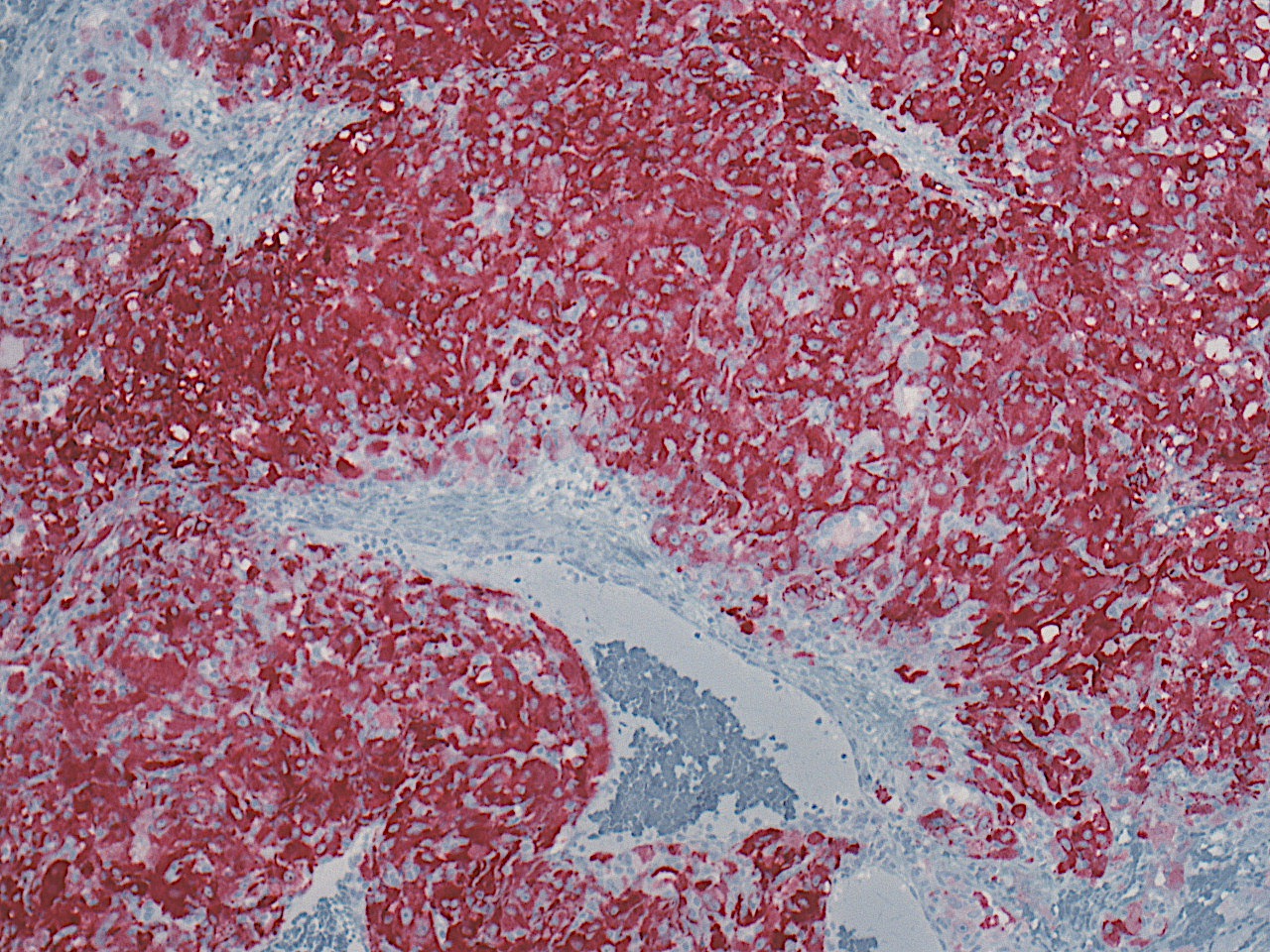
Melanoma cocktail
Cathepsin K
Discussion:
Epithelioid angiomyolipoma (eAML), also termed perivascular epithelioid cell tumor (PEComa), accounts for up to 5% of all angiomyolipomas (AML). Epithelioid cells are the defining feature of eAML, with the 2016 WHO classification requiring at least 80% of the tumor to be epithelioid to render the diagnosis. Epithelioid cells are enlarged, polygonal cells with eosinophilic or clear cytoplasm, atypical nuclei and prominent nucleoli (histopathology images 1 and 2). Two patterns of eAML have been described, the “carcinoma-like” pattern and the so called “epithelioid and plump spindled cells with diffuse growth” pattern. The “carcinoma-like” pattern (this case) manifests with a cohesive heterogeneous population of tumor cells arranged in compartmentalized sheets with intervening vasculature rich septa. When compared with the “carcinoma-like” pattern, the “epithelioid and plump spindled cells with diffuse growth” pattern is populated by a smaller in size and more monotonous collection of epithelioid and spindled cells arranged in tightly packed sheets. By immunohistochemistry, the tumors are immunoreactive for melanocytic markers (e.g. HMB45, MelanA, and microphthalmia transcription factor (MITF)), cathepsin K and smooth muscle markers.
Like classical angiomyolipoma, eAML has been described in patients both with and without evidence of tuberous sclerosis and in the TSC2/PKD1 contiguous gene syndrome. The examination of the background kidney provides important clues regarding this association. The presence of tumorlets (microscopic angiomyolipomas, H&E image 3 above) suggests an association with tuberous sclerosis in this patient.
It is important to recognize eAML because, in contrast to classical AML, it has malignant potential. Some have suggested that certain histologic features can predict the malignant potential of eAML, such as tumor size > 7 cm, presence of tuberous sclerosis syndrome, presence of the “carcinoma-like” pattern, invasion into perinephric fat or renal vein, necrosis, high mitotic count (> 2/10 HPF), older age at presentation and the presence of severely atypical cells (Am J Surg Pathol 2011;35:161). Others, more recently, have suggested that these features do not correlate with malignant potential and that the previous findings may have been related to the type of cases / population the previous studies had incorporated into their cohort (Mod Pathol 2013;26:1355, Moch: WHO Classification of Tumours of the Urinary System and Male Genital Organs, Fourth Edition, 2016).
Test question answer:
D. Tumors may have malignant behavior
