Strategic plan to substantially reduce cancer deaths - discussion #5
The top causes of U.S. cancer deaths and lung cancer
This essay expands on our strategic plan to substantially reduce cancer deaths by discussing the top causes of U.S. cancer deaths and the lessons we have learned from them.
For 2023, the American Cancer Society projects that there will be 609,820 U.S. cancer deaths:
| Projected U.S. cancer deaths in 2023 | |
| Lung & bronchus | 127,070 |
| Colon & rectum | 52,550 |
| Pancreas | 50,550 |
| Breast | 43,700 |
| Prostate | 34,700 |
| Liver & intrahepatic bile duct | 29,380 |
| Non-Hodgkin lymphoma | 20,180 |
| Brain & other nervous system | 18,990 |
| Urinary bladder | 16,710 |
| Esophagus | 16,120 |
| Kidney & renal pelvis | 14,890 |
| Ovary | 13,270 |
| Uterine corpus | 13,030 |
| Myeloma | 12,590 |
| Oral cavity & pharynx | 11,580 |
| Acute myeloid leukemia (AML) | 11,310 |
| Stomach | 11,130 |
| Melanoma of the skin | 7,990 |
| Other leukemias (not AML, not CLL) | 7,910 |
| Soft tissue (including heart) | 5,140 |
| Gallbladder & other biliary | 4,510 |
| Chronic lymphocytic leukemia (CLL) | 4,490 |
| Other nonepithelial skin cancers | 4,480 |
| Uterine cervix | 4,310 |
| Other digestive organ | 3,830 |
| Larynx | 3,820 |
| Vulva, vagina & other female genital | 3,410 |
| Bones & joints | 2,140 |
| Thyroid | 2,120 |
| Small intestine | 2,070 |
| Anus, anal canal & anorectum | 1,870 |
| Other respiratory organs | 1,440 |
| Other endocrine | 1,120 |
| Ureter & other urinary organs | 990 |
| Testis, penis & other male genital | 940 |
| Hodgkin lymphoma | 900 |
| Eye & orbit | 430 |
| Other & unspecified | 48,160 |
| Total | 609,820 |
Modified from Table 1, Siegel 2023
We are initially focusing on the most common causes of cancer death, namely those in the lung, colorectum, pancreas, breast, prostate and liver, which comprise 55% of the projected U.S. cancer deaths in 2023.
Currently, we are making slow but steady progress in reducing cancer deaths. The number of deaths has plateaued but age adjusted cancer rates are decreasing:
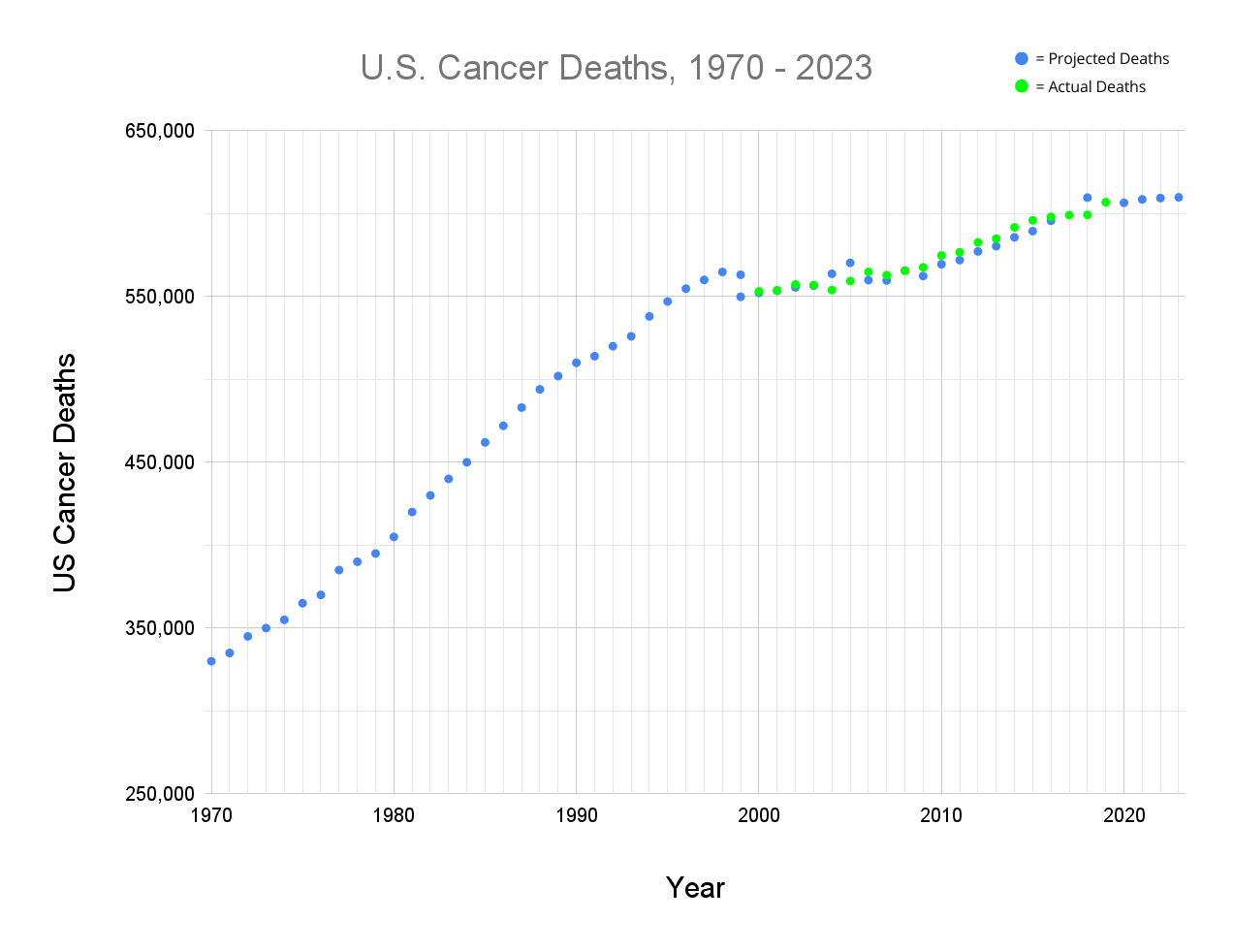
The number of U.S. cancer deaths is now essentially unchanged year to year (see table of references).
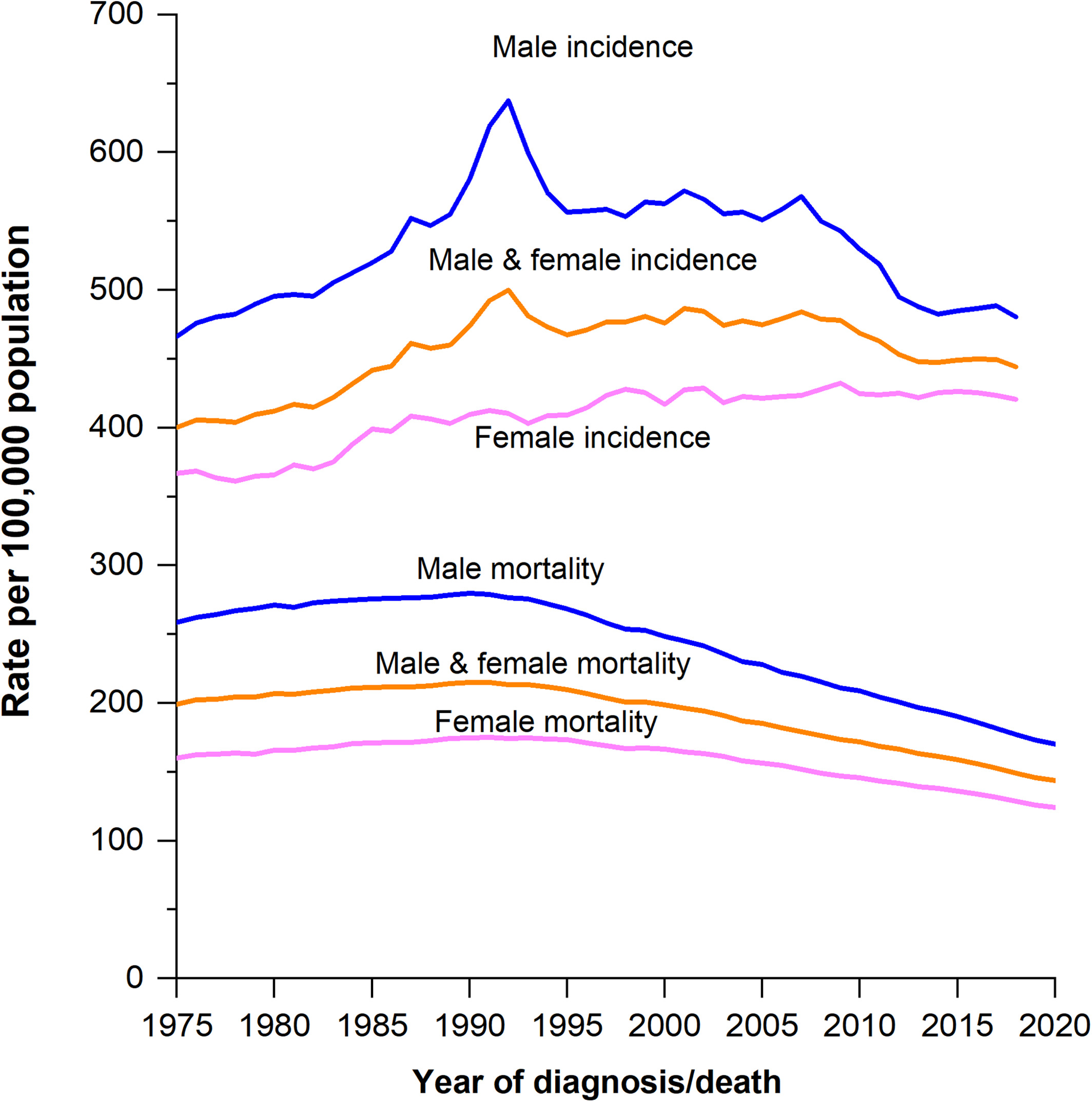
Cancer death rates per 100,000 population (bottom 3 lines) have declined from 1975 - 2020 (Siegel 2023)
The study of curable diseases, such as childhood leukemia and HIV, reveals long periods of no apparent change in the death rate followed by a period of marked improvements, likely due to a long learning curve (Pernick: What will success look like in the war on cancer 2021). Progress in reducing adult cancer deaths has been slow for decades but we predict that continuous improvement and collaboration between researchers will produce an explosion of more effective treatments.
What have we learned from studying the leading causes of cancer death that might be applicable to other types of cancer? For lung cancer, we have learned that:
- Reducing tobacco use, which causes 80% of cases, has caused a marked decrease in lung cancer deaths (Cancer Facts & Figures 2023).
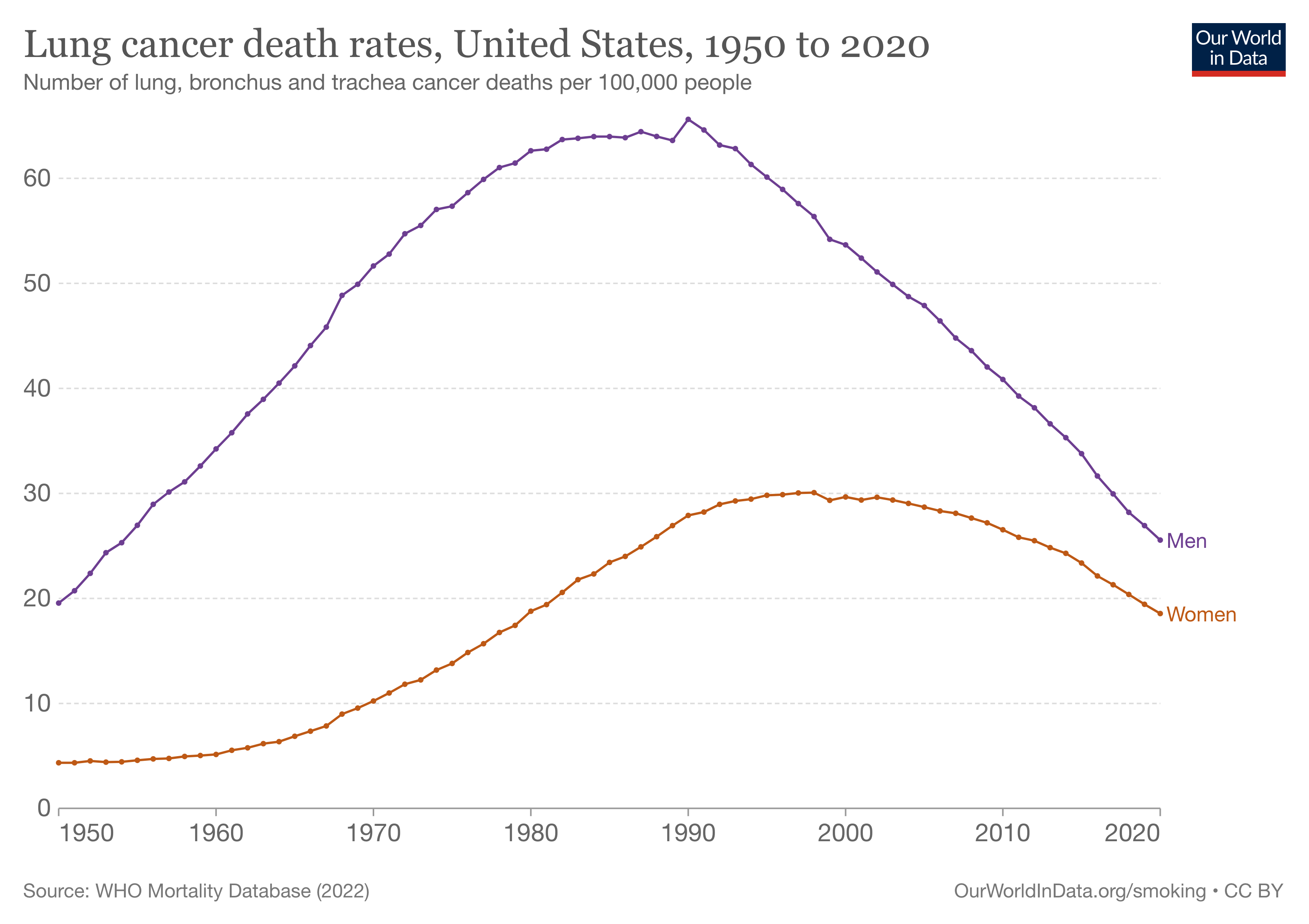
- An annual lung screening with a low dose CT scan is recommended for current or former heavy smokers aged 50 - 80 because it detects cases early and ultimately reduces lung cancer deaths.

- Lung cancer death rates did not start declining until 1990, 26 years after the landmark Surgeon General’s Report on Smoking and Health, which initiated the reduction in tobacco use.
- Lung cancer attributed primarily to tobacco use may be considered a different disease than lung cancer among nonsmokers due to different characteristics. For example, never smokers with non-small cell lung cancer (NSCLC) have higher survival rates than smokers with NSCLC.
- Targeted therapy to attack mutations present in the tumor or aspects of the tumor microenvironment (neighboring tissues, such as blood vessels) has increased survival in advanced lung cancer cases (U.S. National Cancer Institute, American Cancer Society, American Lung Association).
- Cancer risk factors promote malignant changes in widespread areas of tissue (called a field effect) through different biologic pathways. This means that multiple independent cancers may develop over time and each one may require a different treatment. Curative therapy will likely require a diverse combination of treatments.
- Our work on complexity theory also suggests that curative treatment for aggressive and advanced disease must combine multiple strategies, including killing as many tumor cells as possible, addressing tumor cell heterogeneity (variations), reducing risk factors other than tobacco use, reversing their effects (if possible) to prevent new cancers from arising, targeting the tumor microenvironment, targeting immune system dysfunction, moving cancer cells that survive treatment into less lethal networks, developing more effective screening programs and promoting more universal medical care (Pernick 2021).
- We estimate that random chronic stress or bad luck causes a baseline rate of lung cancer of 2 cases per 100,000 men and women per year compared with the current age adjusted U.S. incidence of lung cancer of 54.2 cases per 100,000 and appears to account for most cases of lung cancer in nonsmokers with no other risk factors.
- Many risk factors operate through chronic inflammation so it may be prudent to try to detect and counter any existing inflammatory process.
- In the U.S., indoor radon exposure causes double the percentage of lung cancer deaths in never smokers (men: 19-26%, women: 20-27%) compared to ever smokers (men: 9-12%, women 10-14%). However, the lifetime risk of radon induced lung cancer is much lower in never smokers: 7-18 per 1,000 compared to ever smokers: 62-150 per 1,000 (variation is based on level of radon exposure). Of note, most radon related deaths among smokers would not have occurred if the victims had not smoked.
The next essay will discuss ideas we have learned from studying colon cancer.
