Anus & perianal area
Premalignant
Squamous dysplasia
Authors: Irene Y. Chen, M.D., Xiaoyan Liao, M.D., Ph.D.
Editorial Board Members: Claudio Luchini, M.D., Ph.D., Naziheh Assarzadegan, M.D.


Last author update: 12 February 2025
Last staff update: 12 February 2025
Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Squamous dysplasia
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Chen IY, Liao X. Squamous dysplasia. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/anusdysplasia.html. Accessed September 17th, 2025.
Definition / general
- Noninvasive neoplastic proliferation of the anal squamous epithelium with cytologic and architectural abnormalities
- Associated with human papillomavirus (HPV) infection
Essential features
- Often associated with human papillomavirus genotypes
- Low risk HPV mediates low grade lesion development
- High risk HPV mediates high grade lesion development
- Most cases are found incidentally in asymptomatic patients
- Immunocompromised patients are at increased risk
- Progression to squamous cell carcinoma is influenced by immune status and smoking
Terminology
- Squamous intraepithelial lesion (SIL)
- Anal intraepithelial neoplasia (anal IEN / AIN)
- Anal squamous intraepithelial neoplasia (ASIN)
ICD coding
- ICD-O
- ICD-11
- 2E92.5 & XH3Y37 - benign neoplasm of anus or anal canal & esophageal squamous intraepithelial neoplasia (dysplasia), low grade
- 2E61.2 & XH9ND8 - carcinoma in situ of anal canal & esophageal squamous intraepithelial neoplasia (dysplasia), high grade
Epidemiology
- Rising incidence due to evolving sexual behavior and an increase in HPV infection rates
- Immunodeficient patients (HIV and non-HIV immunosuppression) are at increased risk and present at a younger age
- Additional risk factors: anoreceptive intercourse, coinfection with other sexually transmitted diseases and cigarette smoking (Papillomavirus Res 2017;4:90, Br J Cancer 2015;112:1568)
- Incidence is higher in women and is unrelated to the prevalence of HIV, unlike in men
Sites
- Anus: anal canal, usually the transitional zone
- Also occurs in the perianal skin (< 5 cm to the anal verge / margin)
Pathophysiology
- HPV associated oncoproteins
- E6
- Inactivates p53, allowing survival of cells with genotoxic damage
- Inhibits p21, leading to loss of cyclin E / CDK2 inhibition and progression through the cell cycle
- E7
- Inhibits RB1, leading to a continuous proliferation of mutation bearing cells
- Loss of RB1 leads to overexpression of p16, which is used as a diagnostic surrogate marker
- Inhibits RB1, leading to a continuous proliferation of mutation bearing cells
- E6
- Reference: World J Gastrointest Oncol 2022;14:369
Etiology
- Human papillomavirus (HPV) (Tumour Virus Res 2022;14:200239)
- Double stranded DNA virus of Papillomaviridae family
- Infects humans only
- More than 200 types
- Low risk genotypes (6, 11, 42, 43, 44) associated with low grade lesions
- HPV 6 and 11 are most common in > 90% of condyloma acuminatum
- High risk genotypes (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, 68) associated with high grade lesions and invasive squamous cell carcinoma
- HPV 16 is most common in 28% of low grade and 68% of high grade lesions
- > 1 serotype may be found in lesions
- Low risk genotypes (6, 11, 42, 43, 44) associated with low grade lesions
- Subdivided based on tissue tropism (Cancer Epidemiol Biomarkers Prev 2008;17:1611)
- Anogenital
- Cutaneous
- Other mucosal sites
- Multicentricity is common; > 33% of women with anal HPV also have cervical HPV
- Most are asymptomatic or resolve within 12 months (J Natl Cancer Inst 2008;100:513)
- A small fraction persists or progresses to squamous dysplasia or squamous cell carcinoma
Clinical features
- Often asymptomatic; some patients present with bleeding or pruritus
- Most cases are incidental findings in benign minor surgical specimens, such as hemorrhoids
- May present as papules, plaques, polyps or mass lesions
Diagnosis
- Anal exfoliative cytology
- Sensitivity and specificity for detecting high grade squamous dysplasia are 71% and 73%, respectively (Clin Infect Dis 2018;67:1262)
- High resolution anoscopy with tissue biopsy is the gold standard (J Low Genit Tract Dis 2016;20:283)
Laboratory
Prognostic factors
- Most low grade squamous intraepithelial lesions (LSIL) will regress in immunocompetent patients (Arch Pathol Lab Med 2012;136:1266)
- Recurrence rate of high grade squamous intraepithelial lesions (HSIL) after wide local excision ranges between 9 - 63% (Dis Colon Rectum 2012;55:735)
- Recurrence rate is much higher in HIV patients
- 53 - 67% recurrence rate over 18 - 24 months in HIV+ women and 24 - 53% in HIV+ men (J Acquir Immune Defic Syndr 2020;84:66, AIDS 2017;31:1245)
- May progress to squamous cell carcinoma
- Recurrence rate is much higher in HIV patients
Case reports
- 43 year old man with HIV presented with persistent bloody stool (Int J Clin Exp Pathol 2014;7:3456)
- 45 and 57 year old men presenting with perianal and buttock Buschke-Löwenstein tumor (J West Afr Coll Surg 2020;10:42)
- 55 year old woman with constipation and hematochezia referred for colonoscopy (ACG Case Rep J 2022;9:e00792)
- 65 year old woman found to have a white flat lesion in contact with the dentate line on screening colonoscopy (Acta Gastroenterol Belg 2022;85:108)
Treatment
- Treatment modalities vary by geographic location
- Fulguration with electrocautery during anoscopy
- For lesions that are too large for office based procedures
- Office based ablation techniques
- Via infrared coagulation, hyfrecation, argon plasma coagulation or radiofrequency
- Topical therapy (Lancet Oncol 2013;14:346)
- 5-fluorouracil (5FU)
- Imiquimod
- Trichloroacetic acid (TCA)
- HPV vaccination (N Engl J Med 2011;365:1576, Hum Vaccin Immunother 2016;12:1348)
- Decreases the risk of recurrence in high grade lesions
- Effective in anal cancer prevention when administered early
- Fulguration with electrocautery during anoscopy
- Posttreatment surveillance is required given the high rate of local recurrence
- Reference: J Anus Rectum Colon 2022;6:92
Clinical images
Contributed by Xiaoyan Liao, M.D., Ph.D.
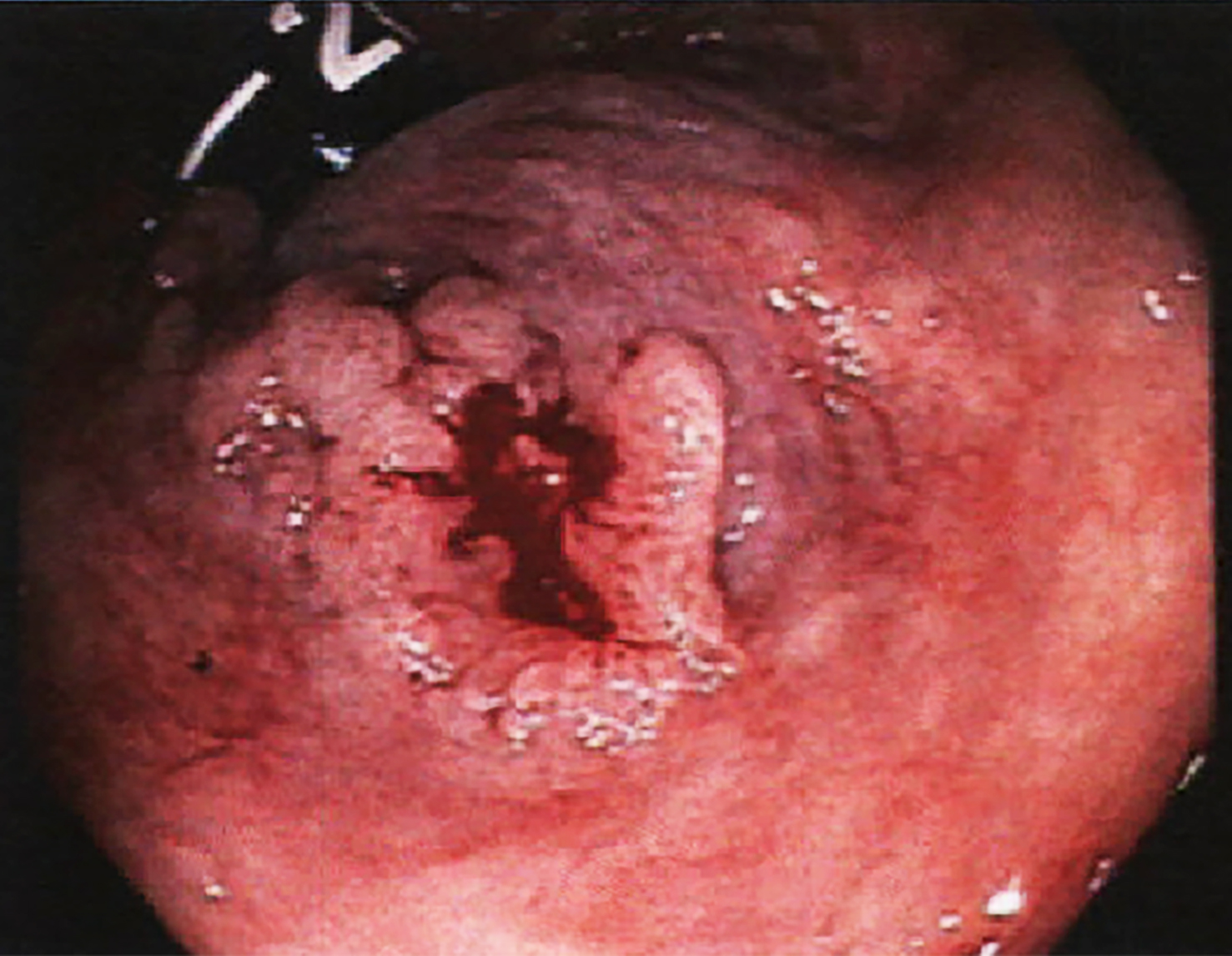
Condyloma acuminatum
Images hosted on other servers:


Anoscopy
Gross description
- May present as papules, plaques or mass lesions
- When present at the anal canal or dentate line, may be mistaken as rectal polyp
Microscopic (histologic) description
- Diagnosis and grading of dysplasia is based on cellular atypia, degree of maturation and mitotic rate (Hum Pathol 2023;132:56)
- Mild dysplasia (AIN1, condyloma acuminatum)
- Cytologic and architectural atypia involving the lower 33% of the epithelial thickness
- Often shows koilocytic changes characterized by perinuclear cavitation and nuclear features of low grade squamous intraepithelial lesion, including nuclear enlargement, coarse chromatin and irregular nuclear membranes (StatPearls: Koilocytosis [Accessed 24 January 2025])
- Pathognomonic but not required for diagnosis
- Often shows koilocytic changes characterized by perinuclear cavitation and nuclear features of low grade squamous intraepithelial lesion, including nuclear enlargement, coarse chromatin and irregular nuclear membranes (StatPearls: Koilocytosis [Accessed 24 January 2025])
- Condyloma acuminatum is exophytic, papillary growth of squamous lesion with parakeratosis and koilocytosis
- Cytologic and architectural atypia involving the lower 33% of the epithelial thickness
- Moderate dysplasia (AIN2): cytologic and architectural atypia involving > 33% but < 66% of the epithelial thickness
- Increased nuclear enlargement and coarse chromatin, compared to AIN1
- Increased mitosis
- Severe dysplasia (AIN3): cytologic and architectural atypia involving > 66% of the epithelial thickness
- Significant nuclear enlargement and atypia, high N:C ratios, increased mitosis often with atypical mitotic figures
- Sometimes interchangeable with carcinoma in situ, which is full thickness squamous dysplasia without any maturation
- Mild dysplasia (AIN1, condyloma acuminatum)
- Diagnostic terms are now unified under the lower anogenital squamous terminology (LAST) standardization project (Arch Pathol Lab Med 2012;136:1266)
- LSIL
- Cytologic and architectural alteration involving < 33% of the epithelium
- Includes lesions that were previously classified as mild dysplasia, anal IEN 1 (AIN1) and condyloma acuminatum
- HSIL
- Cytologic and architectural alteration involving > 33% of the epithelium
- Includes lesions that were previously classified as moderate dysplasia, severe dysplasia, carcinoma in situ, Bowen disease and bowenoid papulosis
- LSIL
Microscopic (histologic) images
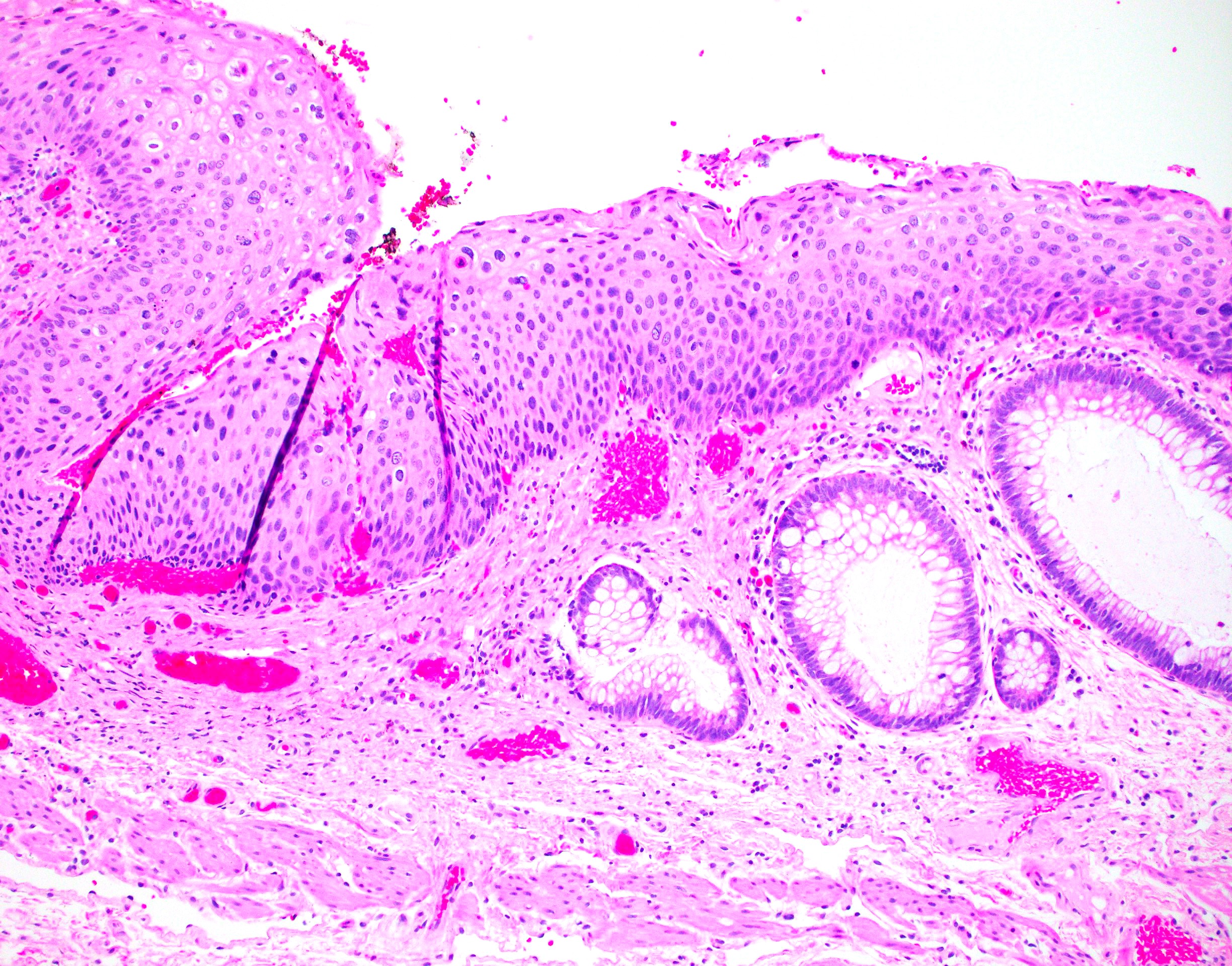
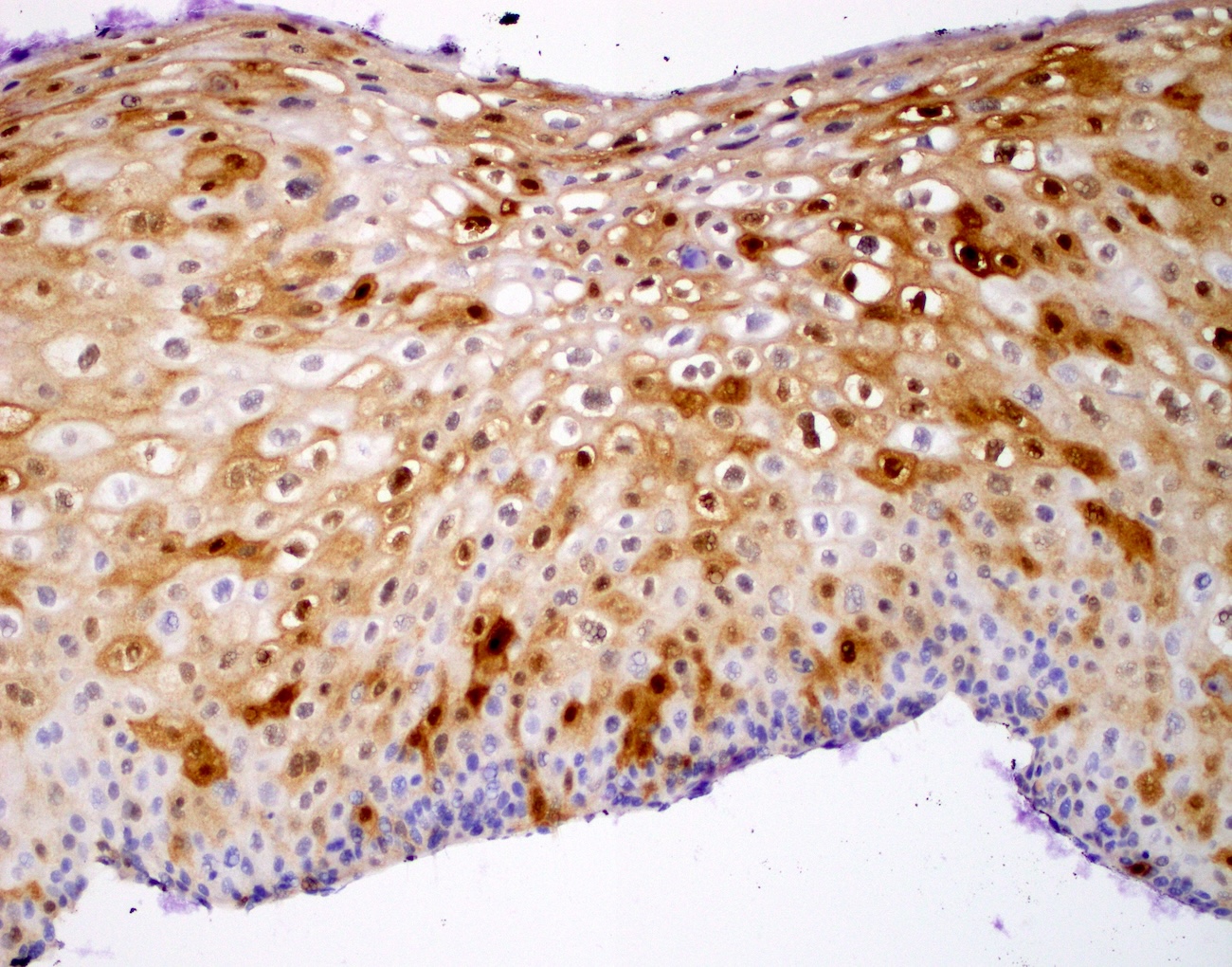
Contributed by Xiaoyan Liao, M.D., Ph.D.
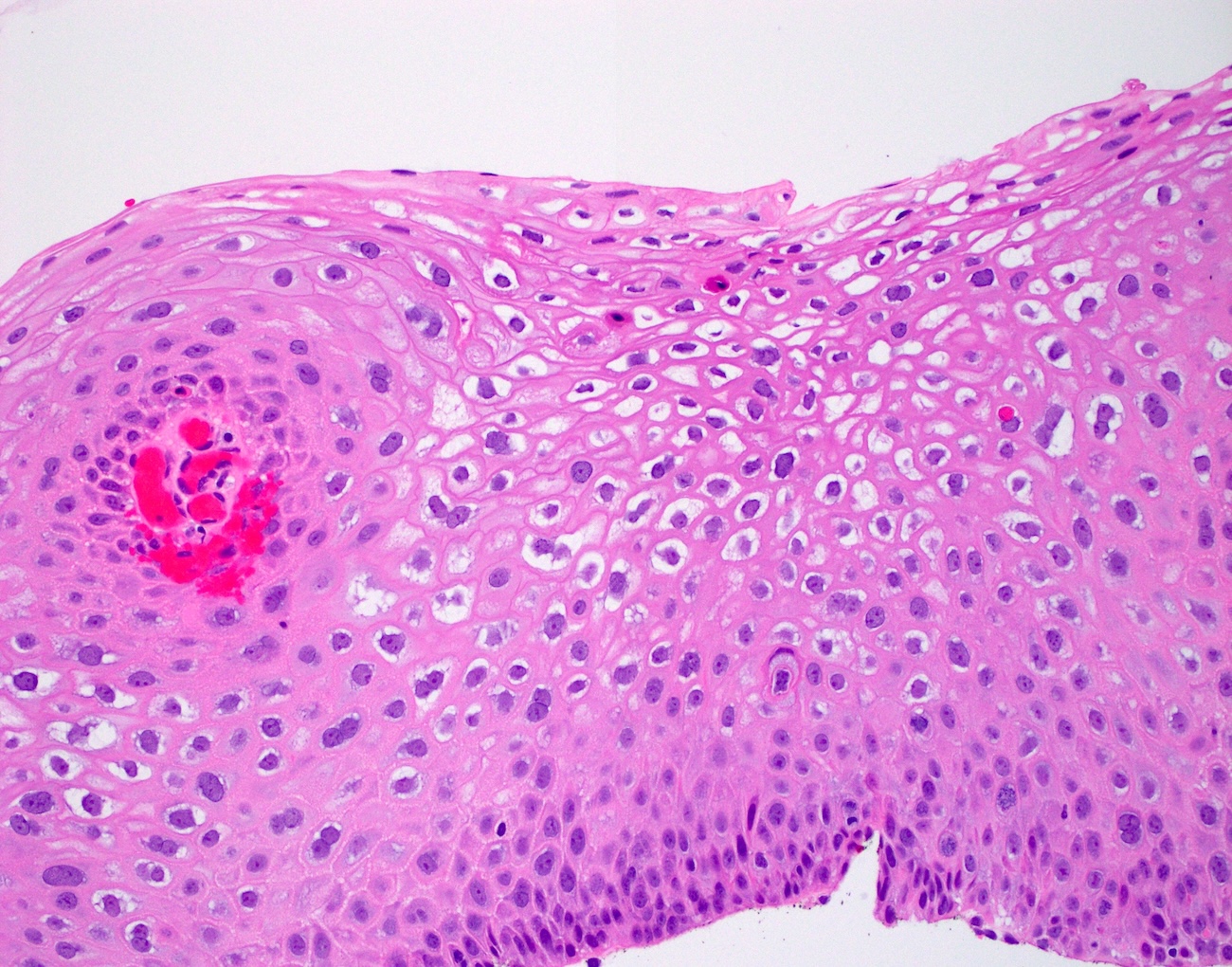
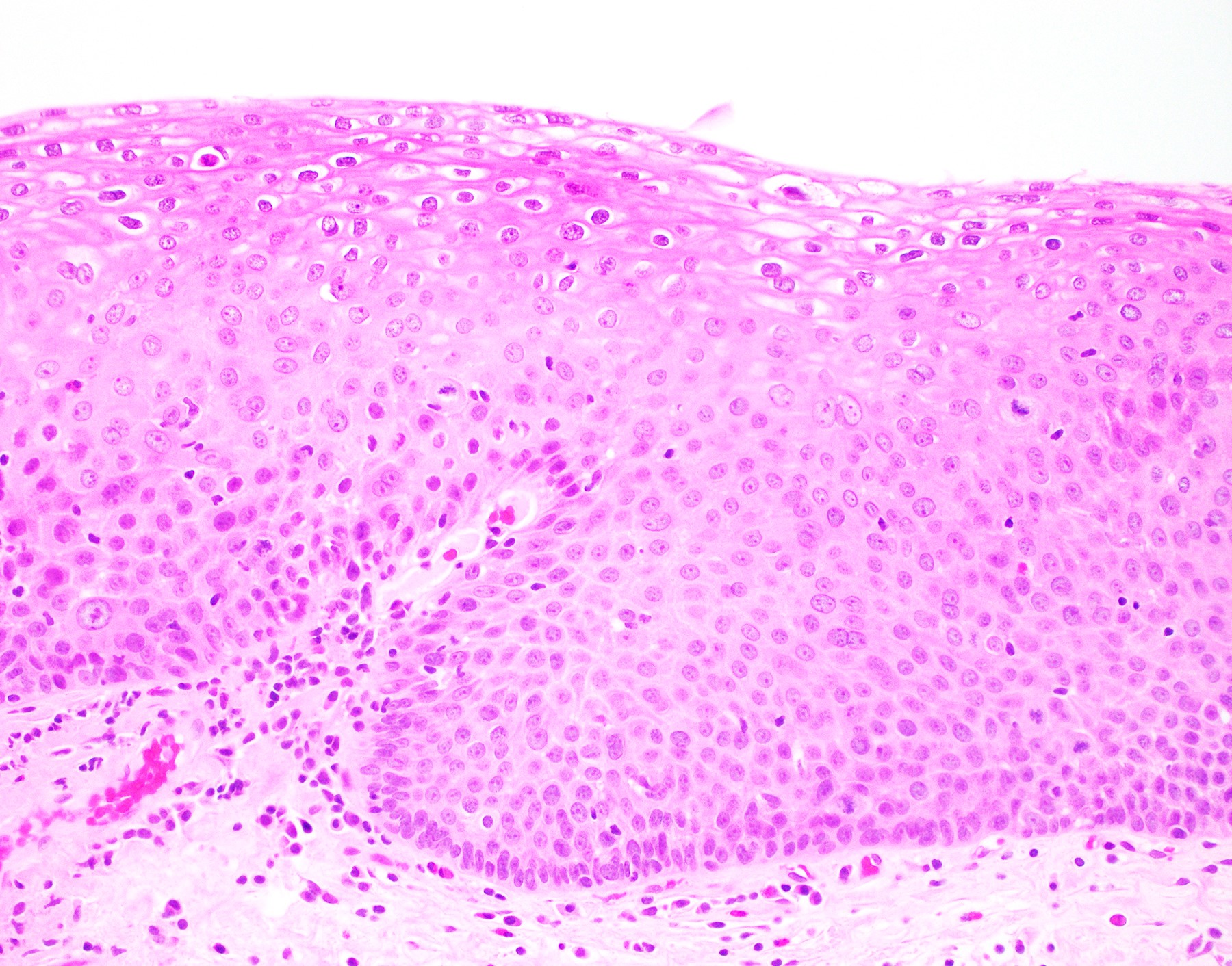
LSIL / AIN1: koilocytic changes and surface maturation
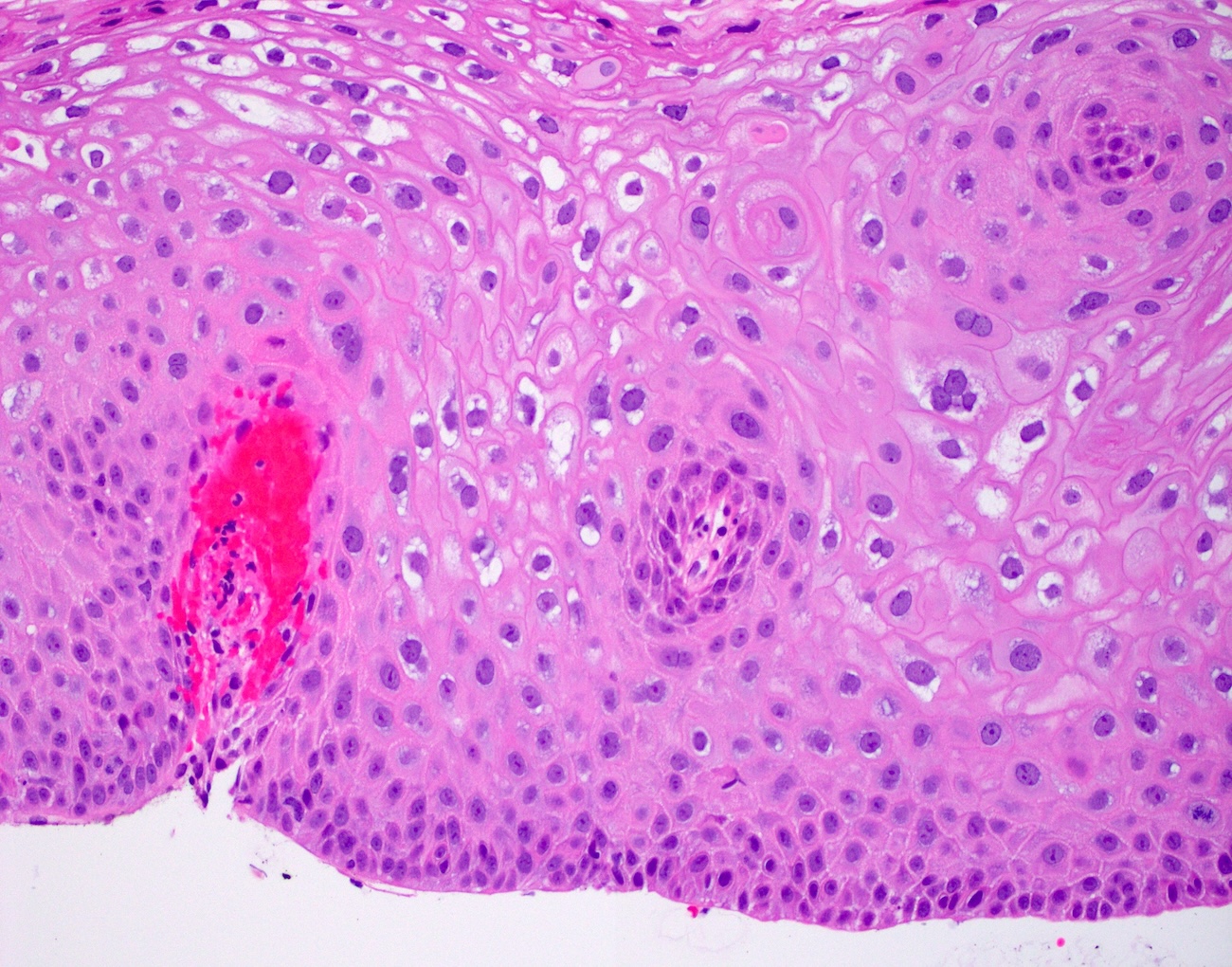
LSIL / AIN1: mild cytologic atypia
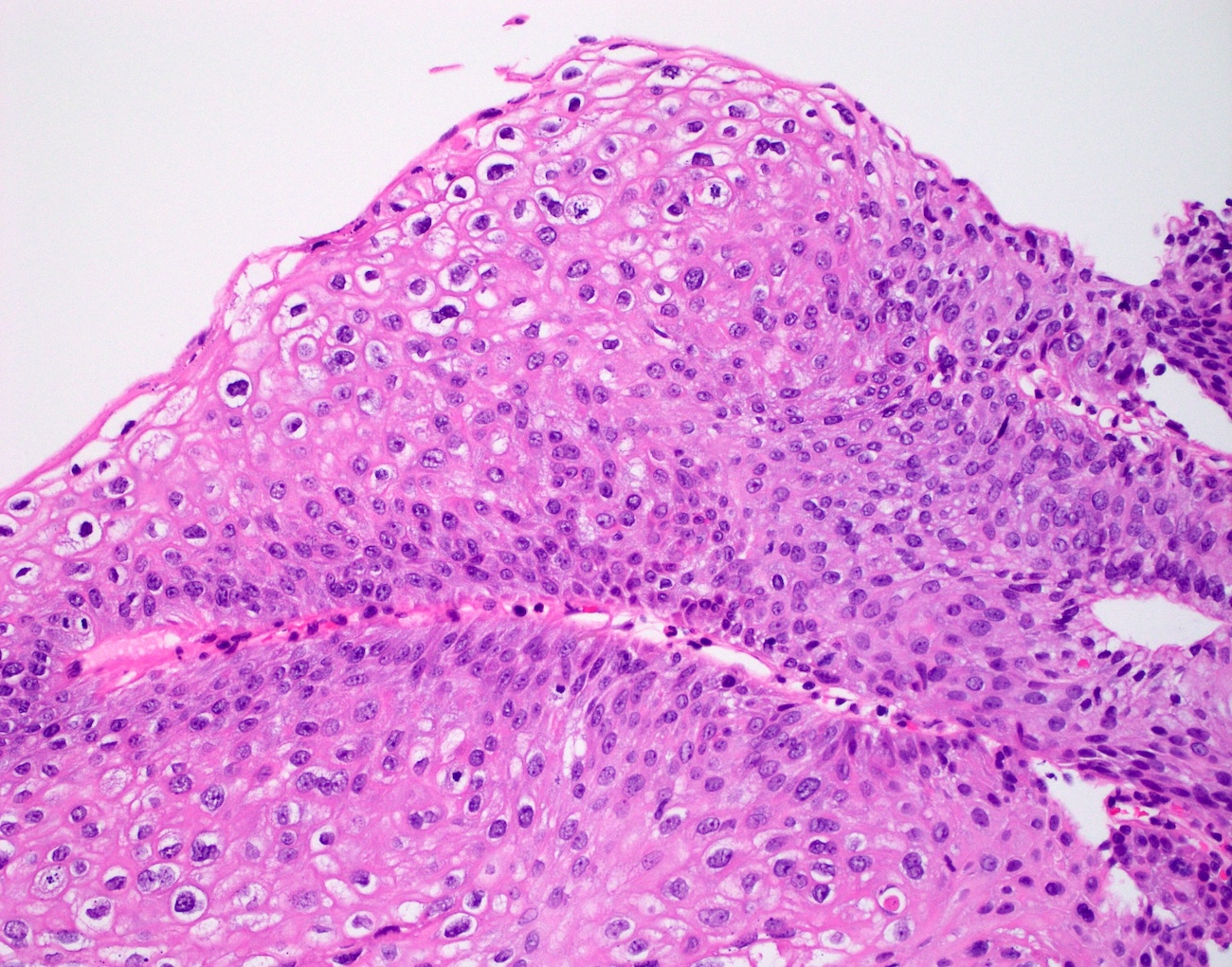
HSIL / AIN2: moderate nuclear atypia and rare abnormal mitoses
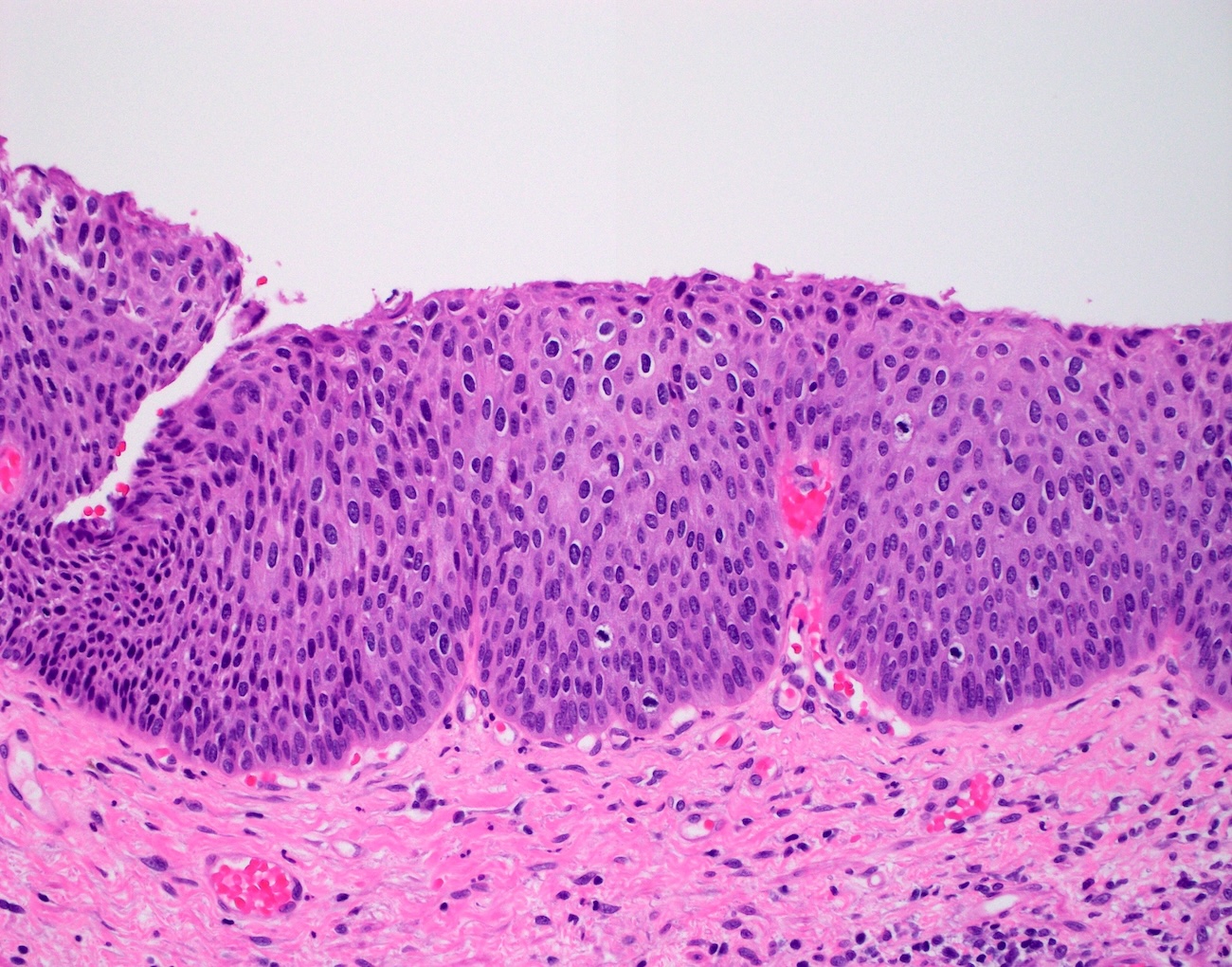
HSIL / AIN3: squamous cells with full thickness cytologic atypia
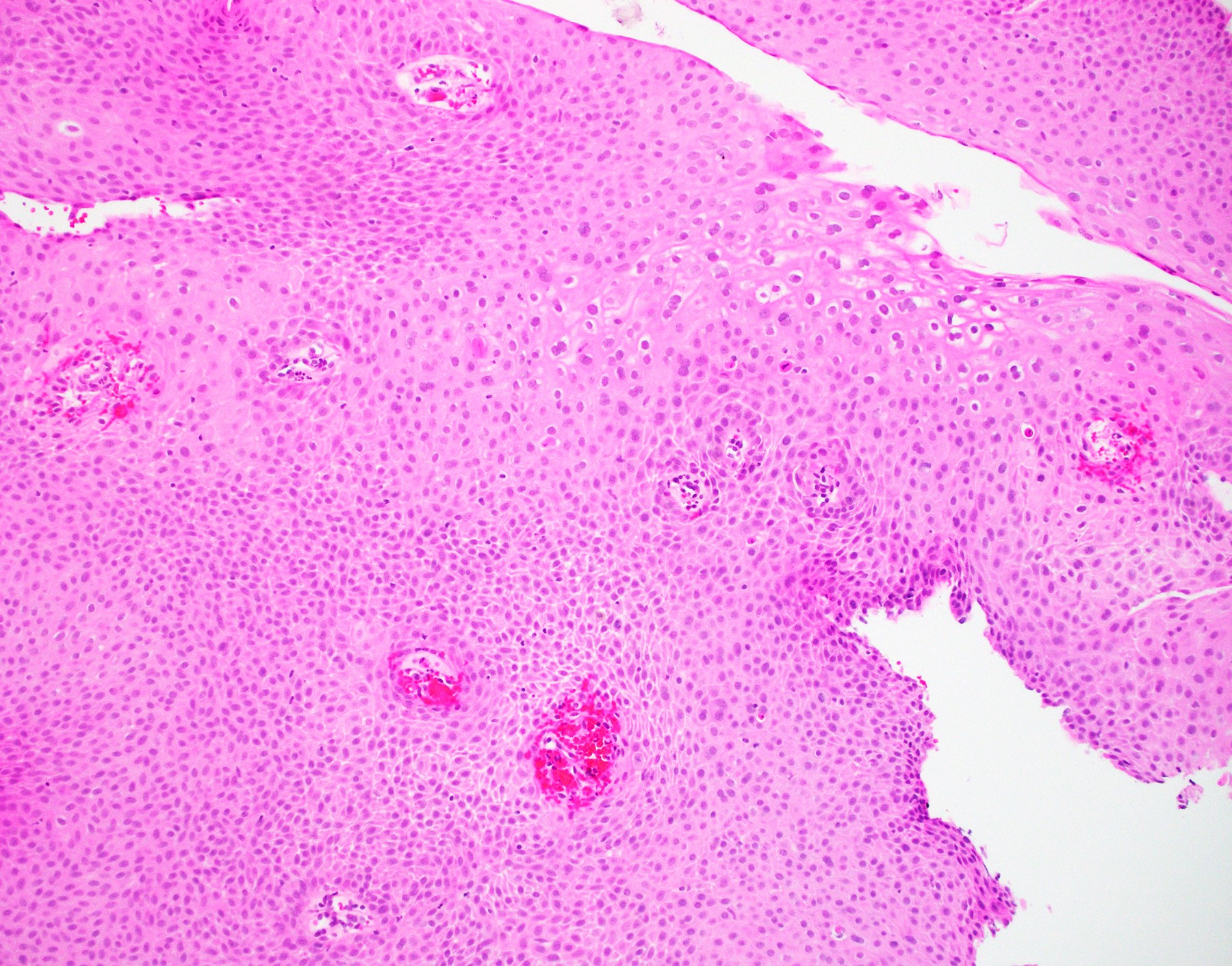
Flat squamous proliferation
Papillary squamous proliferation
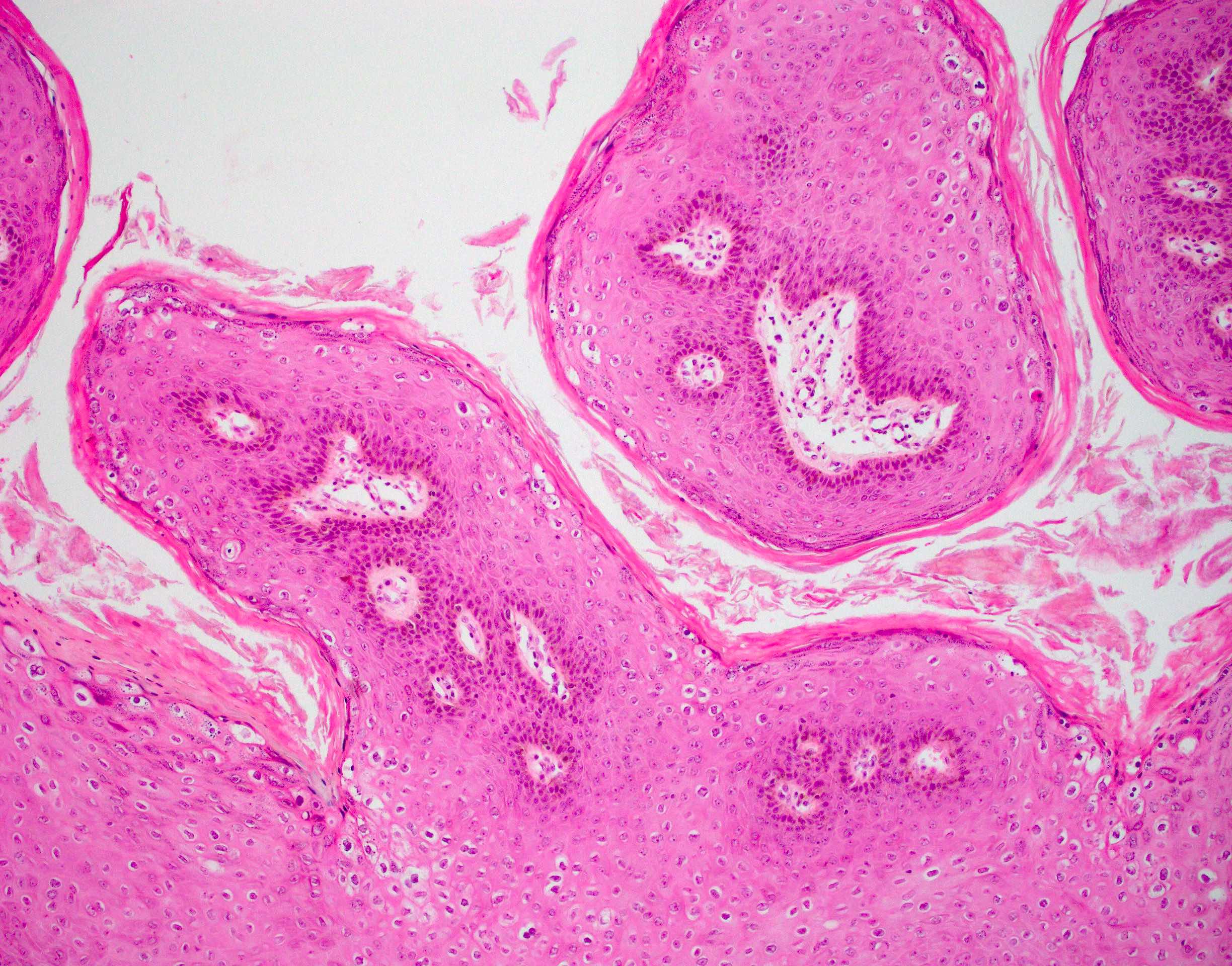

Papillary squamous proliferation, parakeratosis and koilocytosis
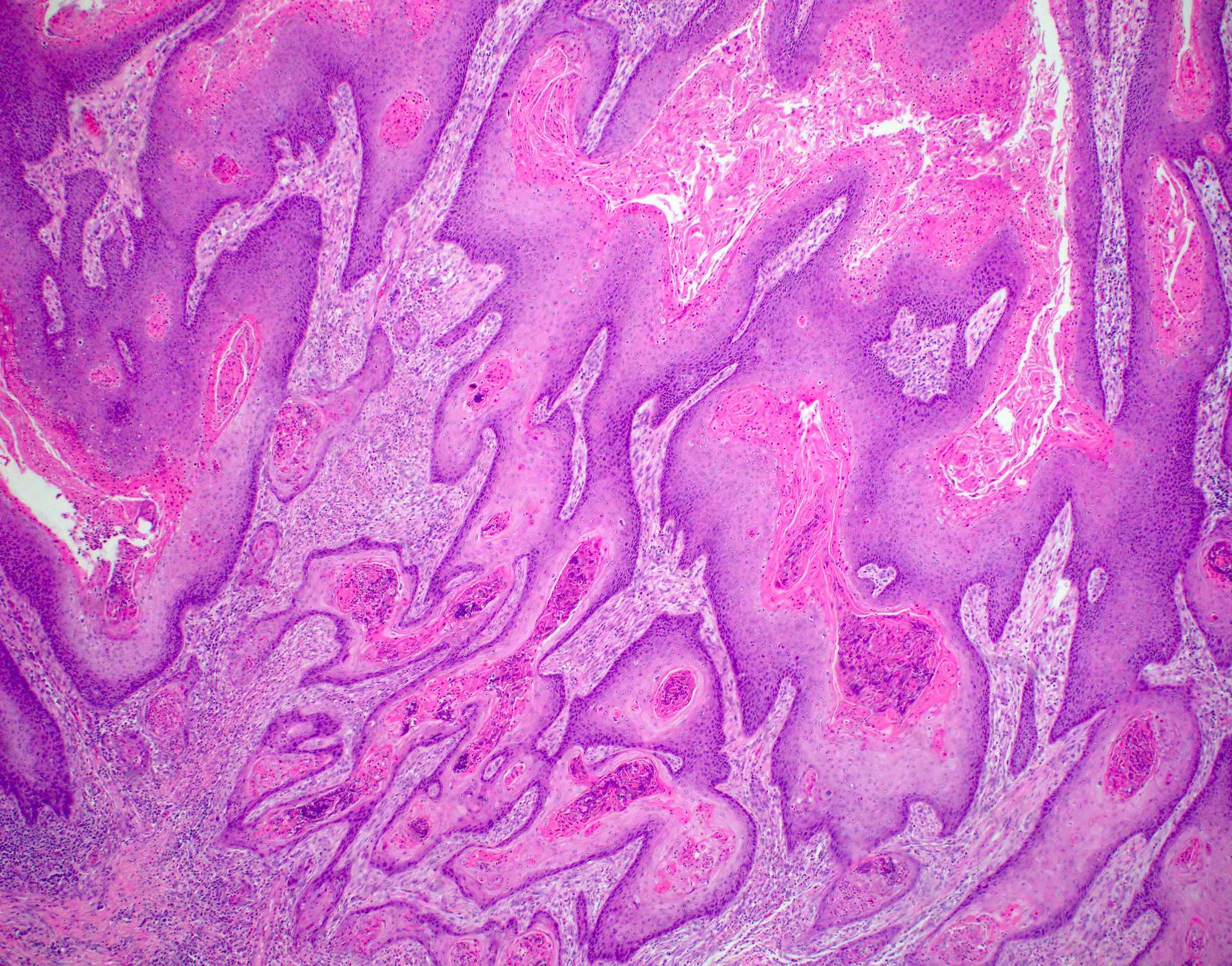
Condyloma with invasion
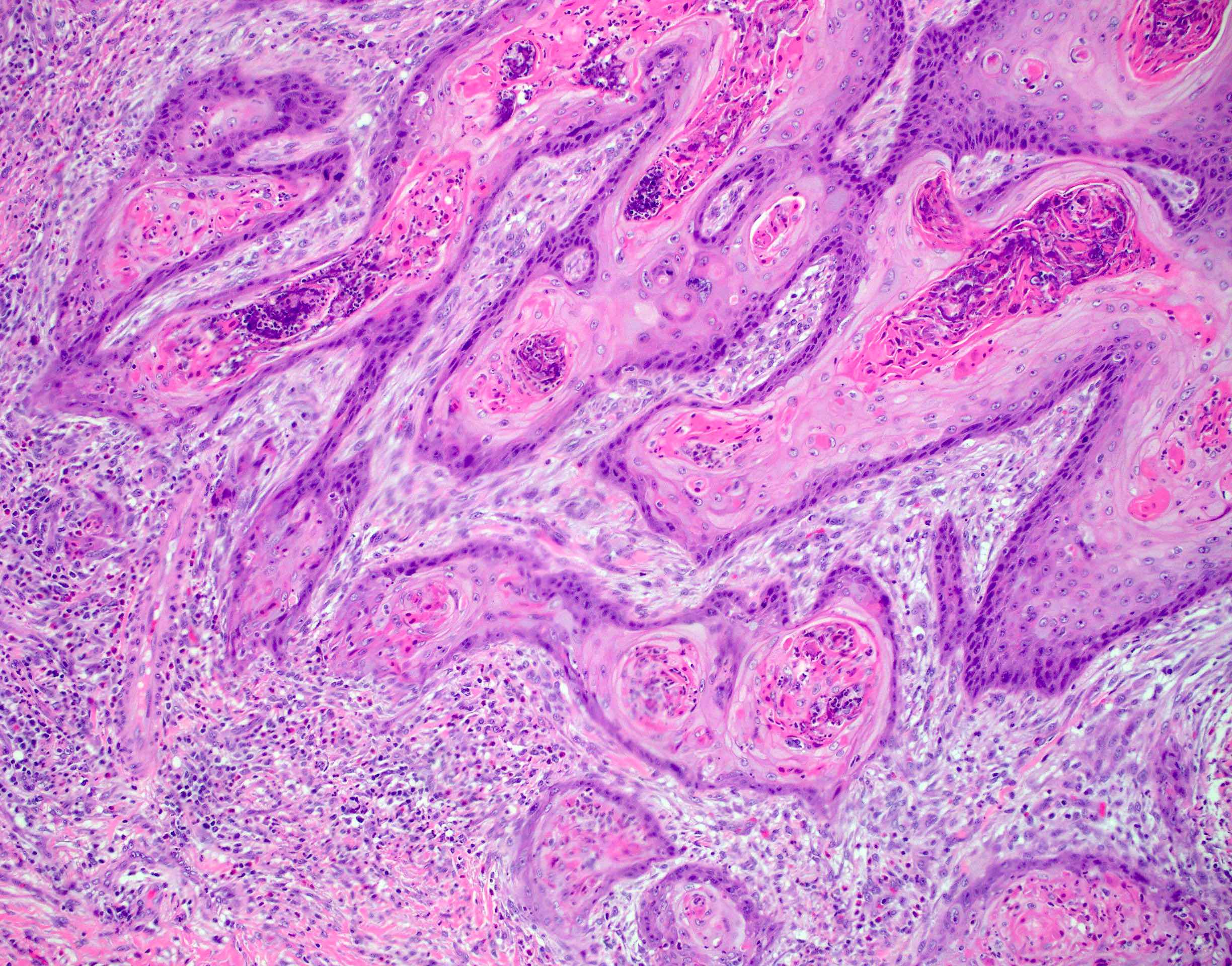
Invasive squamous cell carcinoma arising in condyloma
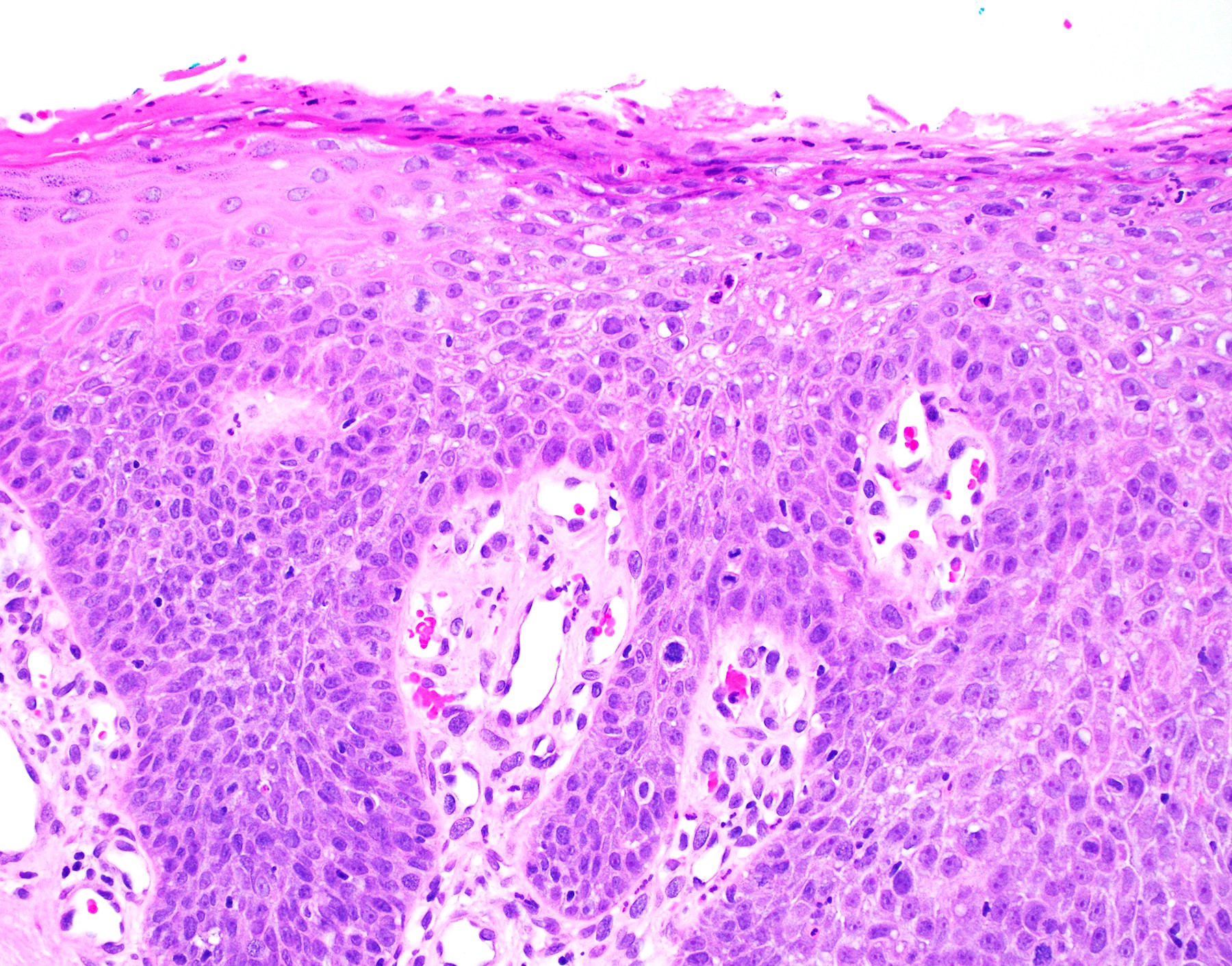
HSIL
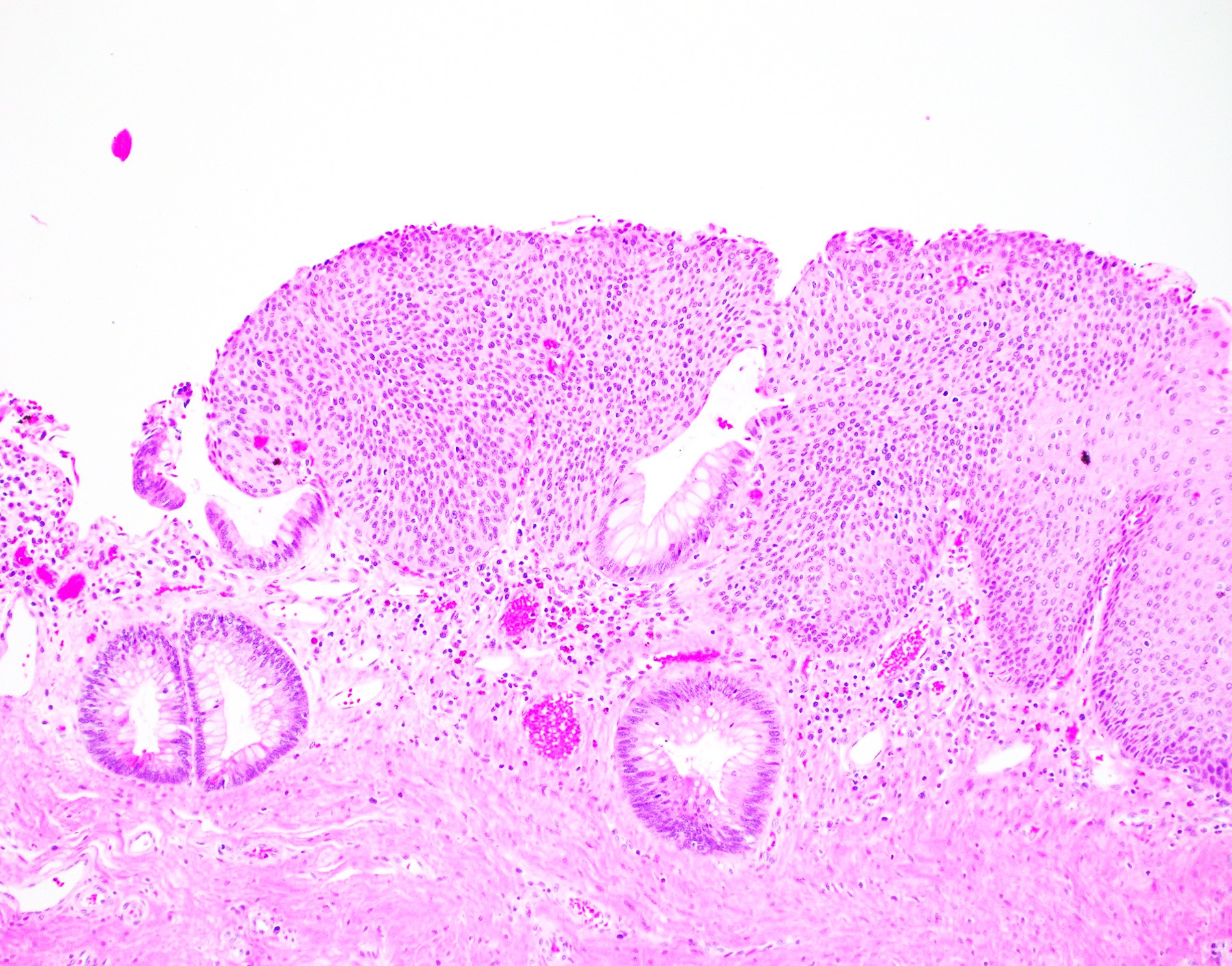
HSIL at the anal transitional zone
Involving a hemorrhoid
LSIL / AIN1: p16 patchy positivity
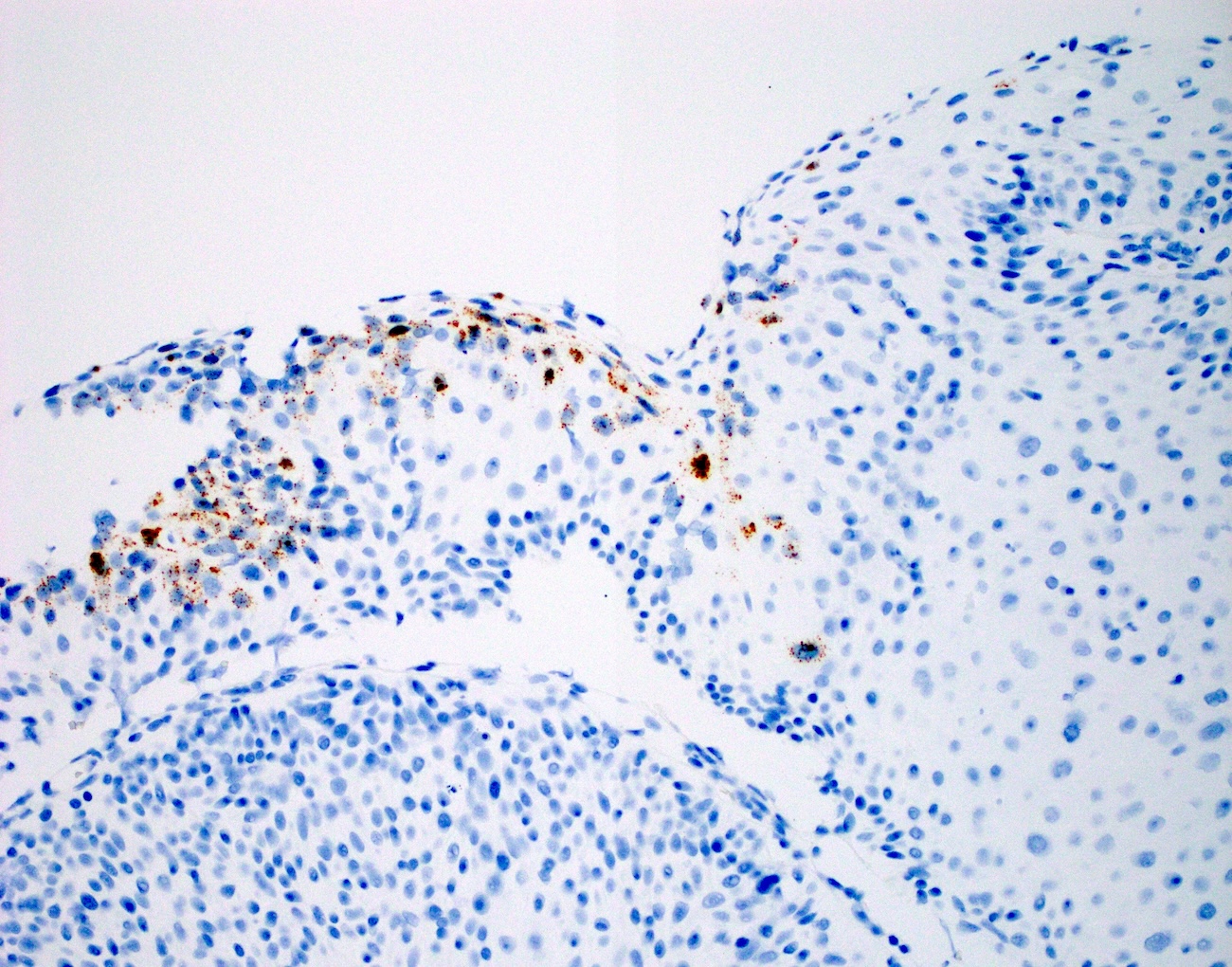
HSIL / AIN2: high risk HPV
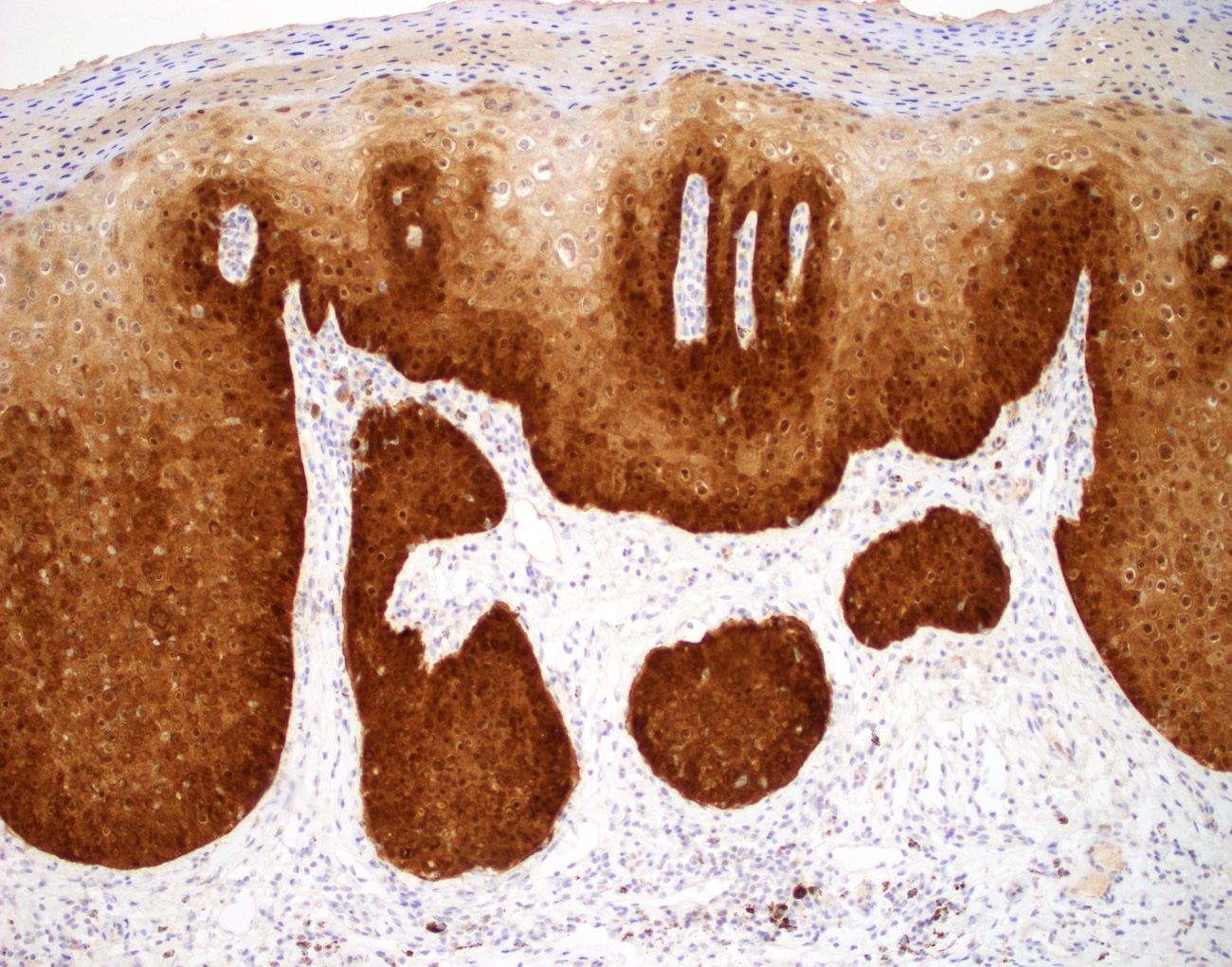
HSIL / AIN2: p16 immunohistochemistry
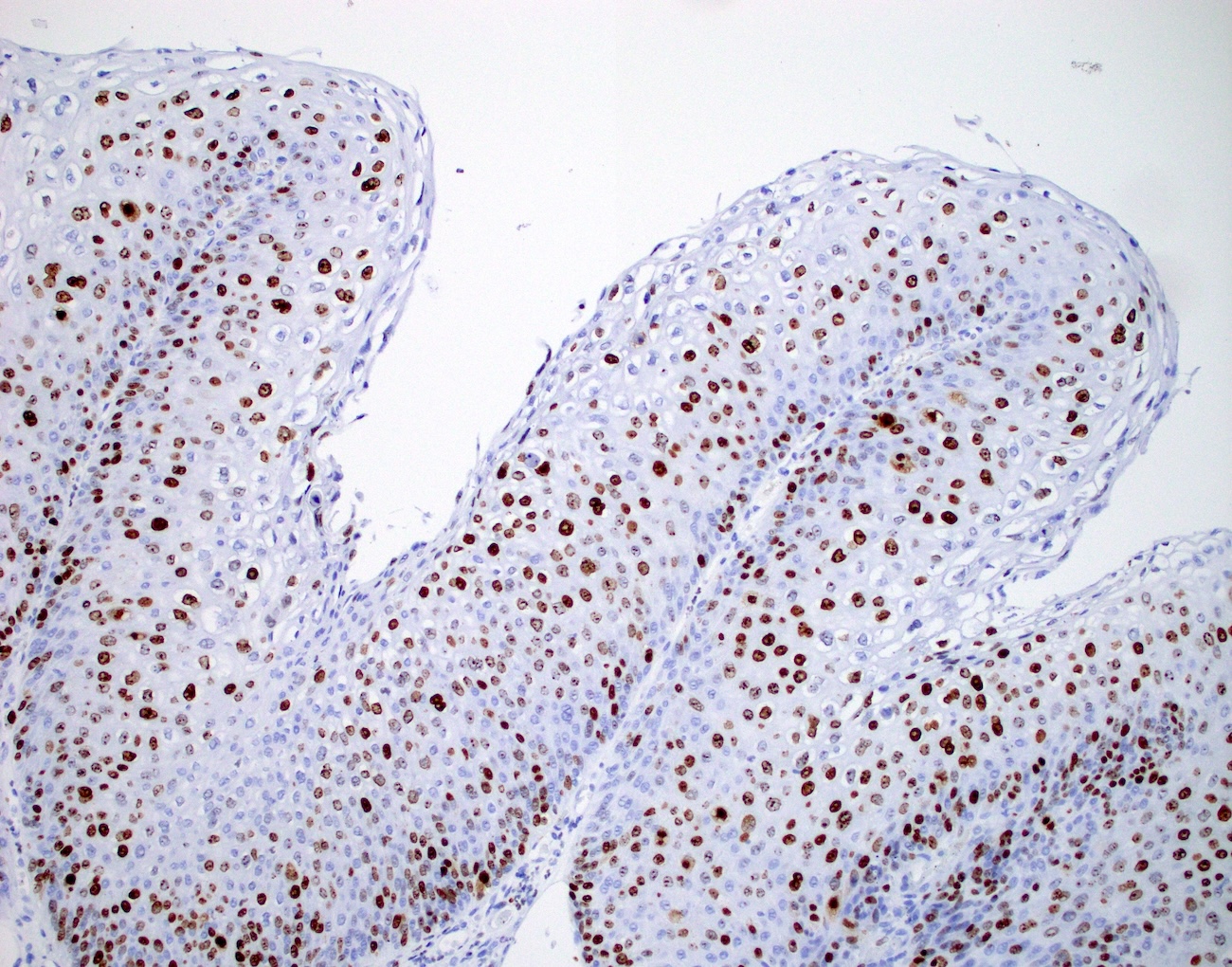
HSIL / AIN2: Ki67
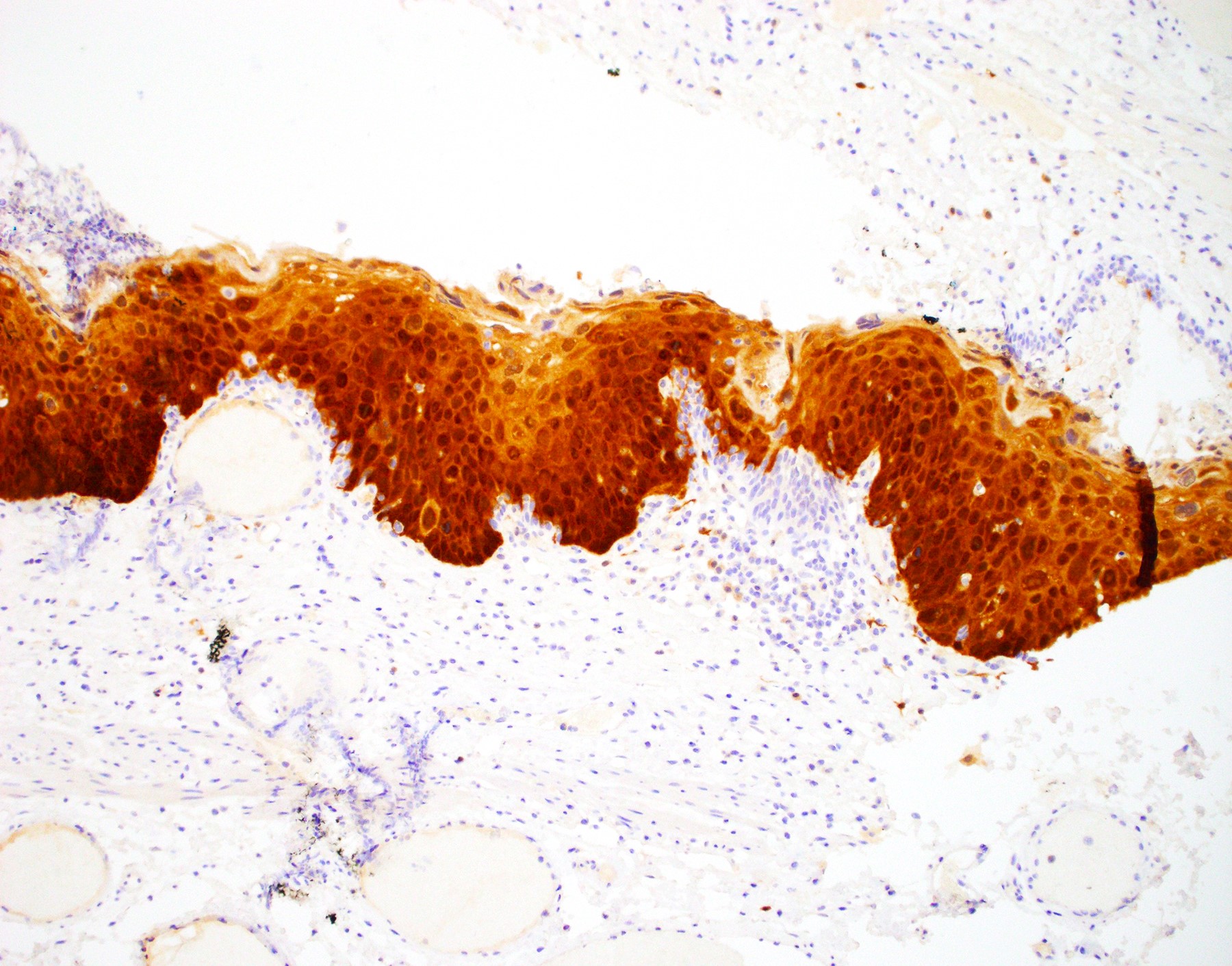
p16 immunohistochemistry
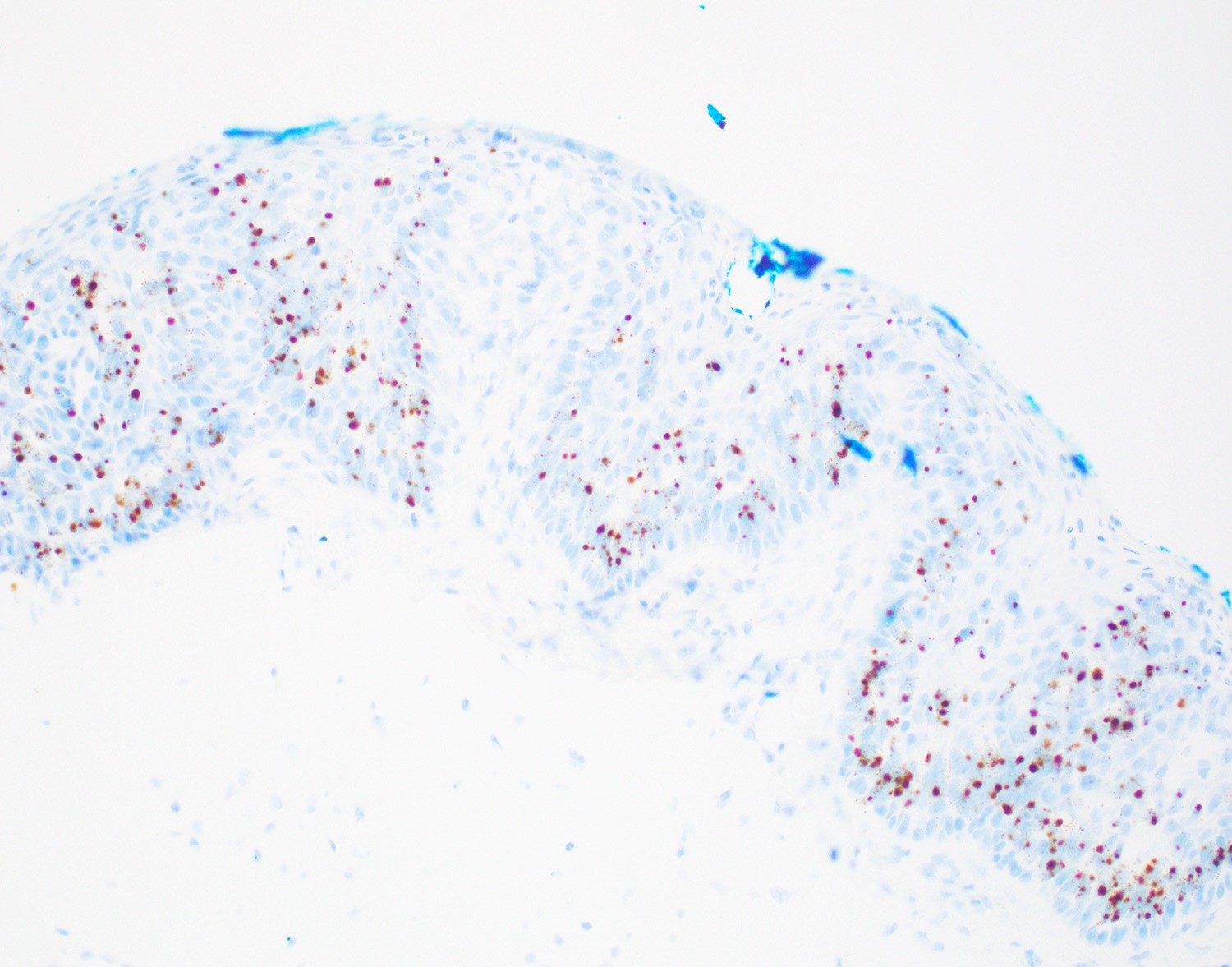
HPV in situ hybridization
Cytology description
- Can be categorized as LSIL, HSIL or atypical squamous cells of uncertain significance (ASCUS)
- LSIL: hyperchromasia, nuclear irregularity, koilocytotic atypia and > 3 fold nuclear enlargement compared to superficial squamous cells
- HSIL: small, immature appearing cells with markedly increased N:C ratio, coarse chromatin and irregular nuclear contour
- ASCUS: typical cells that do not meet the criteria for LSIL or HSIL
- Reference: Diagn Cytopathol 2010;38:538
Cytology images
Contributed by Irene Y. Chen, M.D.
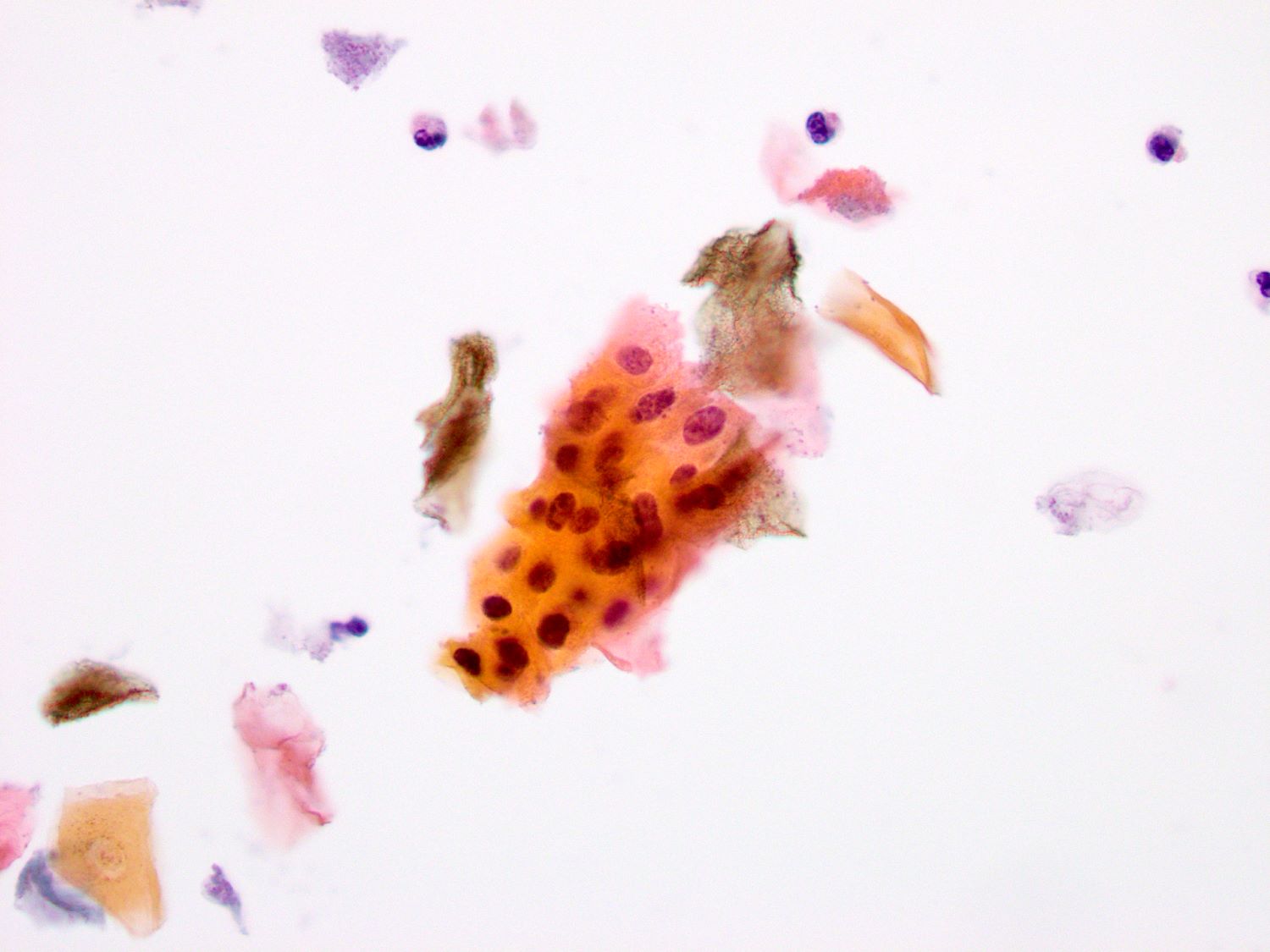
Anal Pap smear
Images hosted on other servers:

LSIL
Positive stains
- p16
- Positive is defined as diffuse, strong, nuclear and cytoplasmic block-like staining
- Surrogate marker for high risk HPV infection
- Distinguishes HSIL from reactive change (91% sensitivity) (Am J Surg Pathol 2021;45:1573)
- Distinguishes AIN2 from AIN1 (89% sensitivity) (Am J Surg Pathol 2021;45:1573)
- Can be positive in LSIL / AIN1 (37%) (Am J Surg Pathol 2021;45:1573)
- Morphology is still the key for diagnosis
- p16 is not recommended when histologic diagnosis is clear cut
- HPV immunostain: positive nuclear staining highlights virally infected cells
- HPV RNA in situ hybridization
- Detects HPV E6 / E7 mRNA transcripts in both transcriptionally active state and when formalin fixed paraffin embedded (FFPE)
- Positive staining with dot-like cytoplasmic and nuclear staining
- High sensitivity and specificity (Am J Surg Pathol 2017;41:607)
- More sensitive than HPV immunostain
- HPV DNA in situ hybridization
- High specificity (89%) but lower sensitivity (83%)
- Ki67: proliferation beyond the basal layer
Negative stains
- p16: negative or weak and patchy in low grade lesions
Molecular / cytogenetics description
- Polymerase chain reaction
- Quantitative reverse transcriptase PCR to detect HPV E6 / E7 mRNA
- Considered the gold standard by the FDA
- Limited utility due to exclusiveness to fresh frozen tissue
- Quantitative PCR to detect HPV DNA
- Cannot distinguish transcriptionally active infection versus passenger
- Quantitative reverse transcriptase PCR to detect HPV E6 / E7 mRNA
- Reference: Infect Agent Cancer 2020;15:46
Sample pathology report
- Anal canal, right lateral, biopsy:
- High grade squamous intraepithelial lesion (moderate dysplasia, AIN2)
Differential diagnosis
- Inflammatory changes / repair:
- Superficial maturation and cellular polarity are maintained
- Round nuclei and may have prominent nucleoli
- No hyperchromasia
- Radiation atypia:
- Cytomegaly and karyomegaly with the maintenance of a low N:C ratio
- Smudgy chromatin with prominent nucleoli
- Squamous cell carcinoma:
- Foci of invasion
- Mass forming
- Adjacent area may show AIN as a precursor lesion
Additional references
Practice question #1
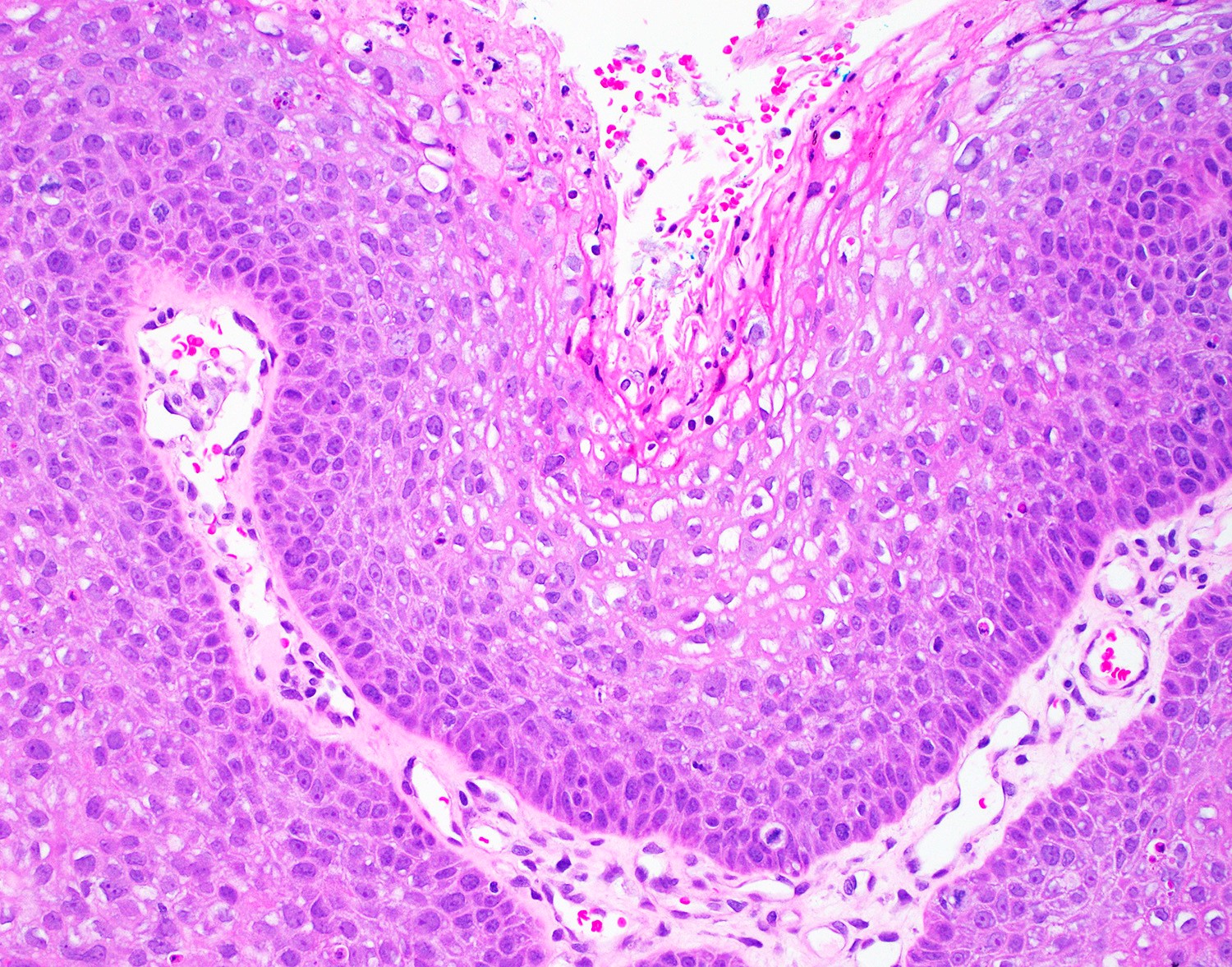
An anal lesion is excised from a 33 year old woman (see image above). No area of invasion is identified on histologic examination. Which of the following statements is true?
- Immunocompromised patients are at increased risk and present at a younger age
- Most cases are incidental findings in asymptomatic patients and do not recur after excision
- Often associated with human papillomavirus genotype 6 and 11
- p16 is often patchy in high grade lesions
Practice answer #1
A. Immunocompromised patients (particularly those HIV+) are at increased risk and present at a younger age. Answer B is incorrect because those lesions often recur after excision. Answer C is incorrect because this is high grade dysplasia and is often associated with HPV 16 and 19. Answer D is incorrect because p16 is often diffuse in high grade lesions.
Comment Here
Reference: Squamous dysplasia
Comment Here
Reference: Squamous dysplasia
Practice question #2
Regarding human papillomavirus (HPV), which of the following is correct?
- Diffuse p16 immunostaining positivity is a surrogate marker for both low and high risk HPV infection
- Low risk HPVs can be associated with high grade lesions
- It is a single stranded RNA virus that does not insert into the human genome
- It only infects the squamous epithelium
Practice answer #2
B. Low risk HPVs can be associated with high grade lesions. While low risk HPVs are generally associated with low grade lesions and high risk HPVs with high grade dysplasia, in recent years there are more and more cases of low risk HPVs giving rise to high grade lesions. Answer A is incorrect because diffuse p16 immunostaining positivity is a surrogate marker for high risk HPV infection. Answer C is incorrect because all HPVs are double stranded DNA viruses and some can insert into the human genome. Answer D is incorrect because the HPV virus can rarely infect glandular epithelium as well.
Comment Here
Reference: Squamous dysplasia
Comment Here
Reference: Squamous dysplasia
