

Bladder & urothelial tract
Other nonneoplastic
Müllerian lesions
Author: Alcides Chaux, M.D.
Last author update: 1 July 2011
Last staff update: 2 November 2022
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Bladder Müllerian lesions
Table of Contents
Definition / general | Terminology | Epidemiology | Sites | Etiology | Clinical features | Case reports | Treatment | Clinical images | Gross description | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Differential diagnosisCite this page: Chaux A. Müllerian lesions. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/bladderendocervicosis.html. Accessed April 19th, 2024.
Definition / general
Endocervicosis
Endometriosis
Endosalpingiosis
- Rare benign tumor-like lesions characterized by prominent endocervical type glands in muscularis propria
Endometriosis
- Presence of functional endometrial tissue within bladder
- Ureter:
- Rare in ureter but can result in renal failure due to silent obstruction
- Associated with hydroureter / hydronephrosis
- Tendency to involve distal third of left ureter (Hum Pathol 2008;39:954)
- Extrinsic: involving serosal or peritoneal surface (adventitia or connective tissue)
- Intrinsic: involving muscularis propria, lamina propria, lumen
- Rarely malignant transformation or endometrial hyperplasia can be present
Endosalpingiosis
- Involvement of lamina propria and muscularis propria by tubules and cysts with tubal type epithelium (ciliated cells, intercalated cells, peg cells)
Terminology
Endosalpingiosis
- Called Müllerianosis if 2 of 3 related entities (endocervicosis, endometriosis or endosalpingiosis) are present (Mod Pathol 1996;9:731)
Epidemiology
Endocervicosis
Endometriosis
Endosalpingiosis
- Women in reproductive years (mean age 39 years, range 34 - 65 years)
- Also men receiving estrogen for prostate cancer
Endometriosis
- Women between the second and fifth decades
- Uncommon, occurs in < 2% of all patients with endometriosis
- Seen in post menopausal women receiving exogenous estrogen
- Also can occur, very rarely, in men taking estrogens for prostate cancer
Endosalpingiosis
- Very uncommon
- Usually seen in women of childbearing age
Sites
Endocervicosis
Endometriosis
Endosalpingiosis
- Posterior wall or posterior dome preferentially affected
Endometriosis
- Usually posterior wall of bladder above trigone or at dome
Endosalpingiosis
- Posterior wall or posterior dome
Etiology
Endocervicosis
Endometriosis
Endosalpingiosis
- Müllerian origin (Am J Surg Pathol 1992;16:533)
Endometriosis
- Probably due to retrograde menstruation, which seeds surface of bladder serosa or postsurgical
- Not due to metaplasia of Müllerian remnants or extension from anterior uterine adenomyosis (Am J Obstet Gynecol 2002;187:538)
Endosalpingiosis
- Metaplastic (Müllerian metaplasia) or implantative (similar to endometriosis)
Clinical features
Endocervicosis
Endometriosis
Endosalpingiosis
- Benign behavior (Hum Pathol 1996;27:816)
- Associated with endometriosis and cesarean section
Endometriosis
- Bladder is the most common site (70 - 80%) of endometriosis of the urinary tract
- May develop into endocervicosis (mucinous metaplasia), endometrioid adenocarcinoma, clear cell carcinoma, adenosarcoma
- Usually associated with prior surgery or female GU symptoms of urgency, frequency, suprapubic pain, rarely hematuria
- Mass is frequently apparent either by palpation or cystoscopic examination
- Bladder implants typically occur at vesicouterine pouch; may grow through muscularis into submucosa, producing a luminal bulge or rarely a polypoid mucosal mass (Radiographics 2006;26:1847)
- Mucosa may appear blue at cystoscopy
Endosalpingiosis
- Suprapubic pain, urinary frequency, dysuria
- May occur after surgery in some cases
Case reports
Endocervicosis
Endometriosis
Endosalpingiosis
- 36 year old woman with chronic pelvic pain (Arch Pathol Lab Med 2005;129:e109)
- 67 year old woman with solid bladder wall mass (Int J Clin Exp Pathol 2009;2:91)
Endometriosis
- 51 year old woman with endometrioid adenocarcinoma arising in ureteral endometriosis (Scientific World Journal 2010;10:1714)
Endosalpingiosis
- 54 year old woman with pure endosalpingiosis, possibly implanted after surgery (Int J Surg Pathol 2010;18:381)
Treatment
Endocervicosis
Endometriosis
Endosalpingiosis
- Excision
Endometriosis
- Hormones, resection (usually no recurrence after partial cystectomy, Hum Reprod 2010;25:884)
Endosalpingiosis
- Excision; may recur (Urology 2004;64:1031)
Clinical images
Images hosted on other servers:
Endometriosis

Laparoscopic segmental cystectomy
Gross description
Endocervicosis
Endometriosis
Endosalpingiosis
- Mass between bladder and uterus in posterior bladder wall, dome or trigone
- Up to 2.5 to 3.0 cm in size
- Spongy cut surface with mucinous / milky fluid
Endometriosis
- Usually serosal
- Palpable mass in 50%
- Rarely polypoid (Am J Surg Pathol 2004;28:285)
Endosalpingiosis
- May form mass on posterior wall of bladder
Microscopic (histologic) description
Endocervicosis
Endometriosis
Endosalpingiosis
- Irregular proliferation of prominent endocervical type glands in muscularis propria, less frequently in lamina propria or subserosal connective tissue
- Glands are irregular in size and shape and may be cystically dilated, containing mucinous secretions with neutrophils
- Glands are lined by a single layer of tall mucinous columnar cells, less commonly flat or cuboidal cells, rarely ciliated or goblet-like cells
- Focal glandular rupture leads to mucin accumulation within the stroma with a fibroblastic histiocytic response
- Absent or mild nuclear atypia, no mitotic figures
- No desmoplasia, no glandular crowding or back to back architecture
Endometriosis
- Resembles endometriosis elsewhere: endometrium-like glandular epithelium associated with endometrial stroma cells and recent or old hemorrhage
- Rarely, only glands or stroma are found
- Ureter:
- Similar to endometriosis seen elsewhere, diagnosis based on the presence of endometrial glands (usually inactive or proliferative pattern) with endometrial stroma (usually normal appearing), sometimes restricted to a thin zone around the glandular component
- Foamy or hemosiderin laden macrophages
- Sometimes a fibrotic reaction
Endosalpingiosis
- Involvement of lamina propria and muscularis propria by tubules and cysts of Müllerian type epithelium
- May replace urothelium and form polypoid projections into bladder lumen
- Tubules and cysts are round / oval, may have prominent branching
- Glands are lined by tubal type epithelium (ciliated cells, intercalated cells, peg cells)
- No atypia, no mitotic figures, no necrosis
Microscopic (histologic) images
AFIP images
Endosalpingiosis

Ovary: glands lined by ciliated epithelium lie in fibrous stroma
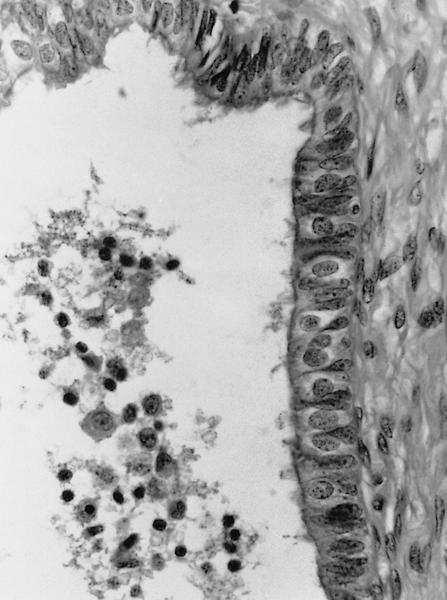
Ovary: ciliated,
secretory and
intercalated cells
line the cystic space
Images hosted on other servers:
Endocervicosis

Prominent
endocervical
glands in
muscularis propria

Complex cystic lesion

Columnar cells with granular mucinous apical cytoplasm
Endometriosis

Endometrial glands and
stroma involving the
peri-ureteral soft tissue
Positive stains
Endocervicosis
Endometriosis
Endometriosis
Differential diagnosis
Endocervicosis
Endosalpingiosis
- Adenocarcinoma:
- Marked atypia, mitotic figures
- Adenoma malignum from uterine cervix:
- Infiltration of bladder serosa, deep cervical involvement
- Glands are variable in shape or size with irregular or claw shaped outlines
Endosalpingiosis
- Adenocarcinoma:
- Marked atypia, invasive borders, usually not ciliated and lacks 3 types of tubal cells
