

Bone & joints
Vascular tumors
Angiosarcoma
Author: Nat Pernick, M.D.

Last author update: 1 June 2005
Last staff update: 31 January 2022
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed search: angiosarcoma [title] bone
Table of Contents
Definition / general | Radiology description | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Electron microscopy description | Differential diagnosis | Additional references | Epithelioid angiosarcomaCite this page: Pernick N. Angiosarcoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/boneangiosarcoma.html. Accessed April 20th, 2024.
Definition / general
- Also called hemangioendothelioma in bone, although angiosarcomas have more cytologic atypia
- Rare; may be multicentric
- 1/3 affect long tubular bones but any bone may be affected
- 1/3 are multifocal, usually in one geographic area, such as an entire leg
- After diagnosis, search for multicentricity
- Distant metastases common, often to lungs
- Graded 1 - 3 based on atypia of endothelial cells
- Grade 1 have excellent prognosis versus poor prognosis for grade 3
Radiology description
- Lytic areas of destruction, with minimal / no reactive new bone formation
Gross description
- Red, hemorrhagic
Gross images
Contributed by Mark R. Wick, M.D.

Primary bone multifocal
Microscopic (histologic) description
- Obvious atypia of tumor cells, solid areas alternating with irregular, anastomosing vascular channels
- Necrosis and hemorrhage, brisk mitotic activity
- Variable differentiation often within same tumor; may be epithelioid or histiocytic
- May have benign giant cells, eosinophils, occasionally reactive bone formation
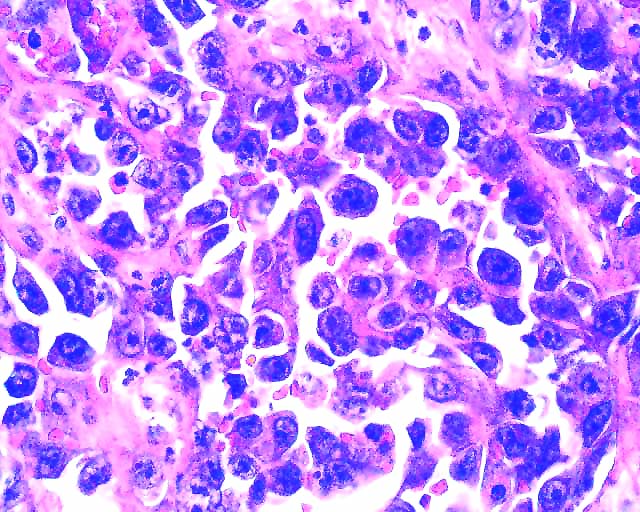
Microscopic (histologic) images
Contributed by Mark R. Wick, M.D. and AFIP images
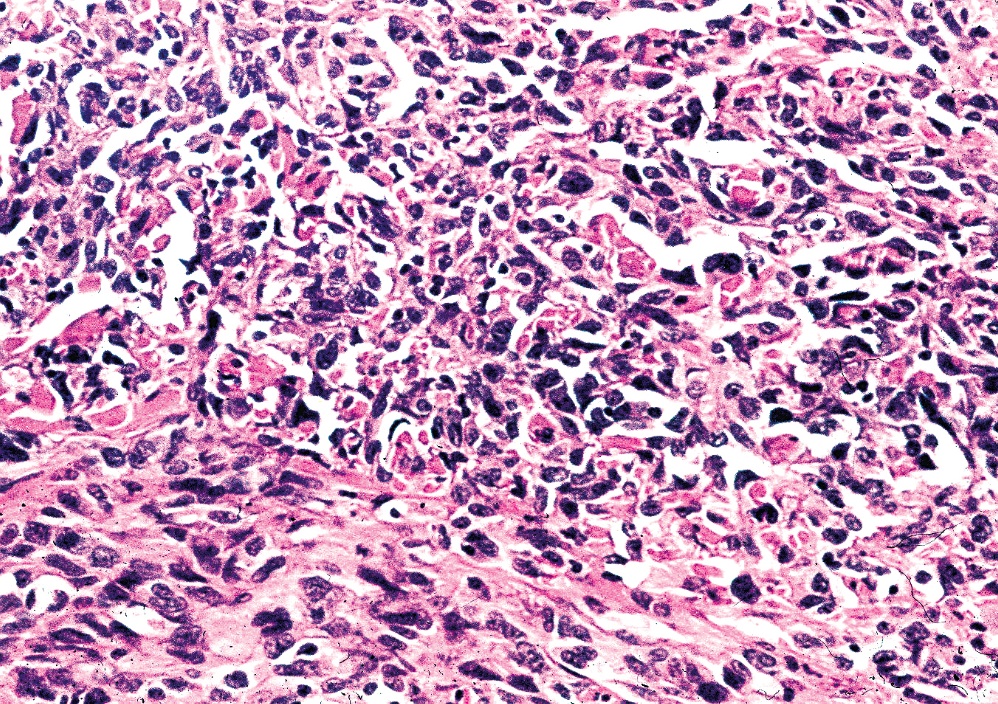
Primary bone
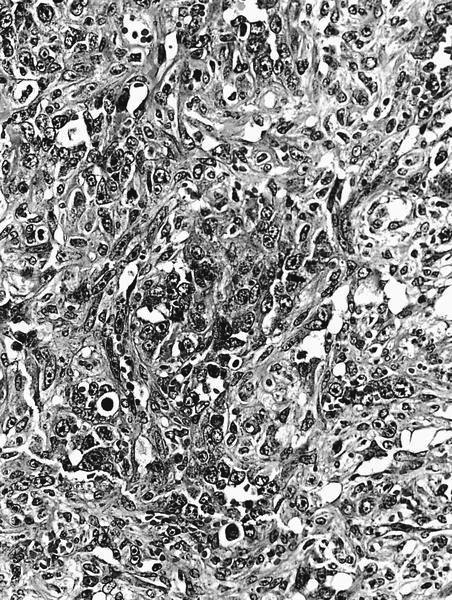
Grade 3
Positive stains
Electron microscopy description
- Endothelial cell features, may have pericytic features
Differential diagnosis
Additional references
Epithelioid angiosarcoma
Definition / general
Radiology images
Contributed by Mark R. Wick, M.D.

Case reports
Gross description
Microscopic (histologic) description
Microscopic (histologic) images
Contributed by Mark R. Wick, M.D.
Positive stains
Negative stains
Electron microscopy description
Differential diagnosis
Additional references
- 80% male, mean age 62 years, range 26 - 83 years
- 60% multifocal
- Aggressive clinical course
- > 90% of tumor cells have epithelioid features
Radiology images
Contributed by Mark R. Wick, M.D.
Primary bone Xray
Case reports
- 48 year old with humerus tumor (Hum Pathol 199;28:985)
Gross description
- Friable, hemorrhagic, destructive tumor, 2 - 12 cm
- Poorly defined, infiltrates medullary canal, frequently erodes cortex and invades adjacent soft tissue
Microscopic (histologic) description
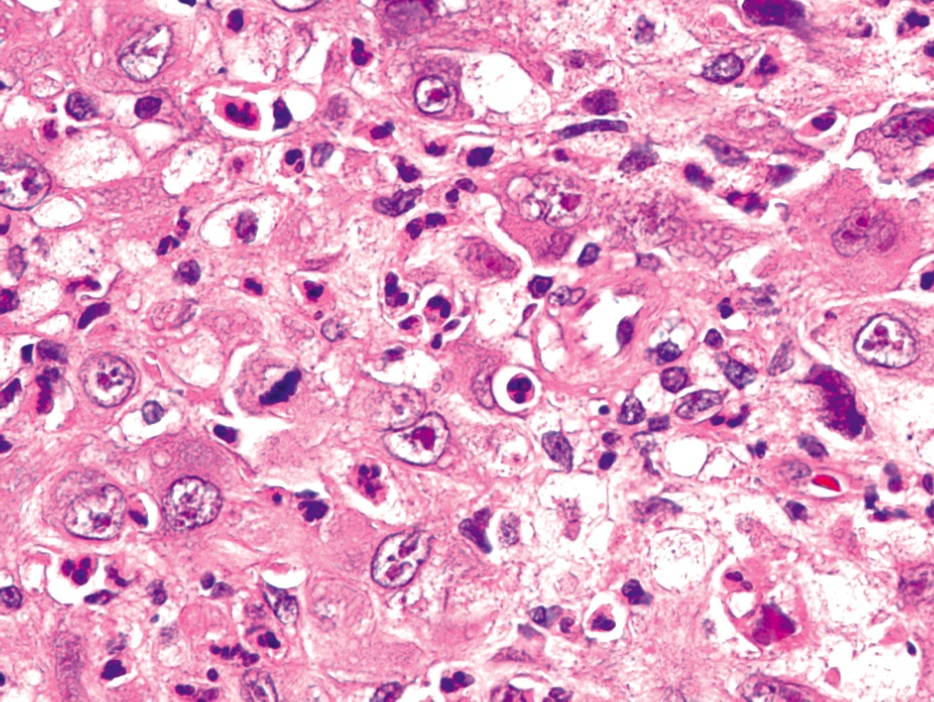
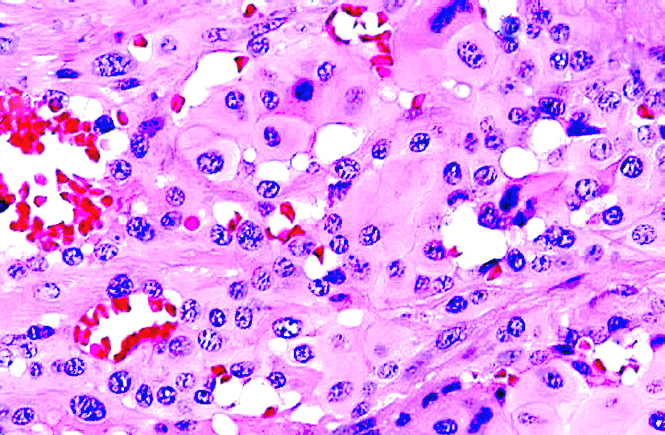
- Solid and infiltrative sheets replacing the marrow and encasing bony trabeculae
- No lobular growth pattern
- Usually with prominent vascular channels or cystically dilated spaces
- Tumor cells are large, polygonal with abundant eosinophilic cytoplasm, large nuclei with open chromatin, prominent eosinophilic nuclei
- Frequent intratumoral hemorrhage, neutrophils, intracytoplasmic lumina
- Frequent mitotic figures and necrosis
- May have rhabdoid or spindled features
Microscopic (histologic) images
Contributed by Mark R. Wick, M.D.
Various images
Primary bone
Positive stains
- CD31, factor VIII related antigen, cytokeratin (often), CD34 (variable)
Negative stains
Electron microscopy description
- Long junctions, intracytoplasmic filaments, mitochondria, rough endoplasmic reticulum
- May contain rare Weibel-Palade bodies
Differential diagnosis
- Metastatic carcinoma: no well formed vascular channels, no neutrophils; negative for factor VIII, CD31 and CD34
- Mucin+ cytoplasmic vacuoles
Additional references
