

Skin nontumor
Infectious disorders
Cysticercosis
Last author update: 1 January 2016
Last staff update: 6 September 2022
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Cysticercosis [title] skin


Table of Contents
Definition / general | Epidemiology | Sites | Diagrams / tables | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Additional referencesCite this page: Soni A, Slominski A. Cysticercosis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/skinnontumorcysticercosis.html. Accessed April 20th, 2024.
Definition / general
- Tissue infection caused by ingestion of larval cysts of the cestode Taenia solium (cysticercus cellulose) (CDC: Cysticercosis [Accessed 27 August 2018])
- Acquired by swallowing food, water or feces contaminated by T. solium eggs
- In cystecicercosis, the human represents an intermediate host and the parasite develops cysticerci in various organs
- Taeniasis: infection caused by the adult tapeworm in the human intestine, which occurs from ingestion of larvae in undercooked pork
- Cysticerci: larval forms of tapeworms found within a fluid filled cyst
Epidemiology
- 50 - 100 million people infected worldwide (eMedicine: Cysticercosis [Accessed 27 August 2018])
- Endemic areas include: Central and South America, India, China Southeast Asia, Africa and Eastern Europe
- In the United States, infection is most common in rural areas and among Latin American immigrants
Sites
- Cysticerci develop in the nervous system, heart, skeletal muscle, eyes and subcutaneous tissue
- Cases in breast are rare; 8 cases were identified by FNAC over a 15 year period in India (Acta Cytol 1996;40:653)
Diagrams / tables
Images hosted on other servers:

Life cycle

Cysticercus
Etiology
- Accidental ingestion of eggs or gravid proglottids of Taenia solium by human host via infected food, water or feces
Clinical features
- Cysticercosis of the skin is rare
- It presents as a palpable, subcutaneous nodule
- In the breast, may present as a freely mobile cystic mass
Diagnosis
- Thorough history, skin biopsy, serology (serum or CSF) and imaging can aid in the proper diagnosis
Radiology description
- CT scan can reveal hyperdense lesions in subcutaneous tissue with or without calcification
- Ultrasound can reveal cystic lesions
Radiology images
Images hosted on other servers:

Computed tomography

Cysts

Mammogram, tubular structure
Case reports
- 14 year old boy presented with an arm swelling for 2 months (Case #458)
- 15 year old girl with solitary breast cysticercosis (Med Trop (Mars) 2007;67:179)
- 19 year old woman with disseminated cutaneous cysticercosis and neurocysticercosis (Indian Dermatol Online J 2012;3:135)
- 19 year old woman with subcutaneous cysticercosis (Rev Chilena Infectol 2013;30:323)
- 31 year old man with disseminated cysticercosis and taeniasis (Am J Trop Med Hyg 2013;89:58)
- 32 year old woman with cysticercus of the breast which mimicked a fibroadenoma (J Clin Diagn Res 2012;6:1555)
- 35 year old woman with an incidental case associated with fibroadenoma (Indian J Pathol Microbiol 2001;44:59)
- 38 year old woman with cystic lesion in left breast containing larval fragment of cysticercus (Trop Parasitol 2013;3:148)
- 45 year old patient with subcutaneous and cerebral cysticercosis (J Am Acad Dermatol 2004;50:S14)
- 56 year old woman with gigantic solitary cysticercosis pseudotumour of the neck (J Surg Case Rep 2010;2010:5)
- 63 year old woman with calcifications detected by mammography caused by cysticercus (Am J Trop Med Hyg 2008;79:864)
Treatment
- Praziquantel and albendazole are effective
- Surgery is appropriate for large, solitary lesions which would otherwise require prolonged antiparasitic therapy
Clinical images
Images hosted on other servers:

Gigantic cysticercosis pseudo tumour

Swelling over neck

Swellings over back
Gross description
- Circumscribed, white to tan, cystic nodules containing a clear fluid
- Viable cysts are translucent, through which a single scolex may be visible (2 - 3 mm nodule)
- As the cyst begins to degenerate, the fluid becomes dense and opaque
- In the later stages, only a calcified nodule may be present
- Cyst sizes vary; commonly 1 mm - 2 cm
- Larval forms identified within the cyst cavity
Gross images
AFIP images

Breast cyst
Images hosted on other servers:

Cysticercosis pseudotumor

Well circumscribed nodule

Specimen from trunk

Breast: tubular, worm-like structure
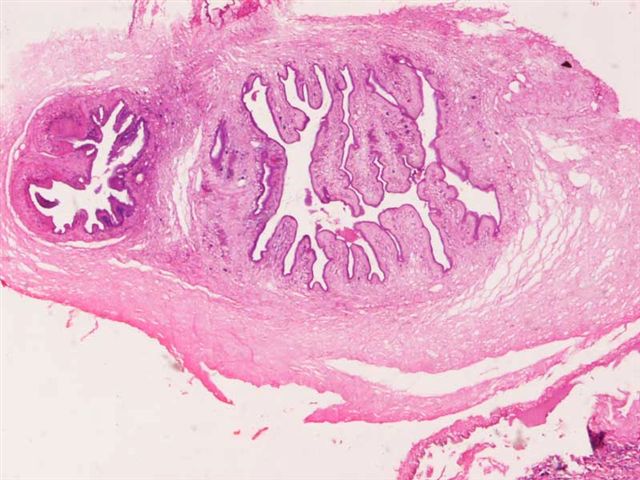
Microscopic (histologic) description
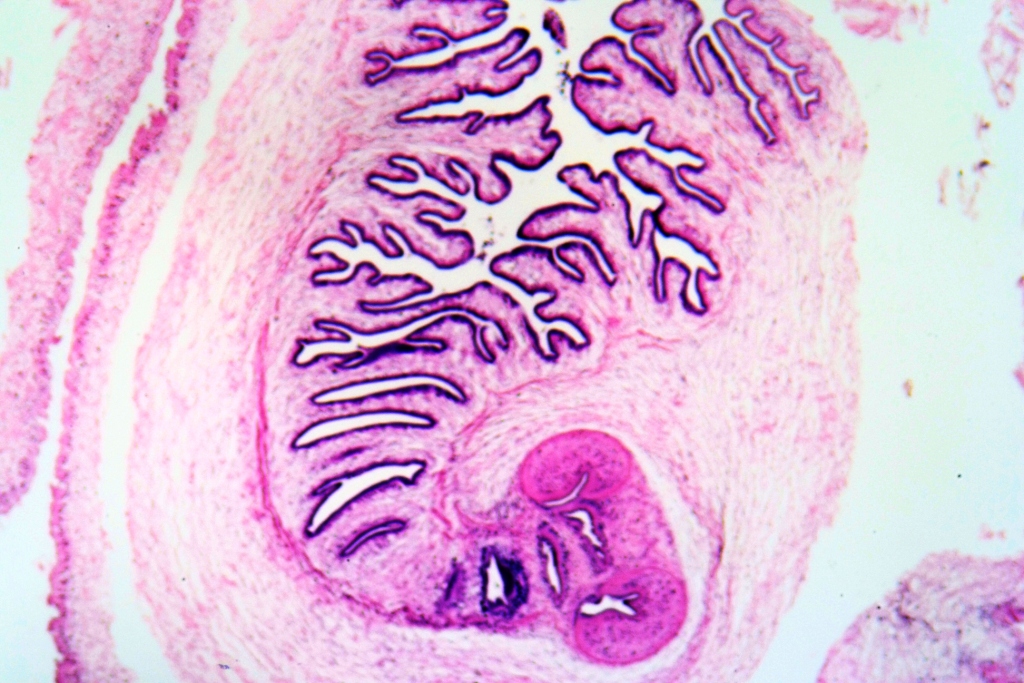
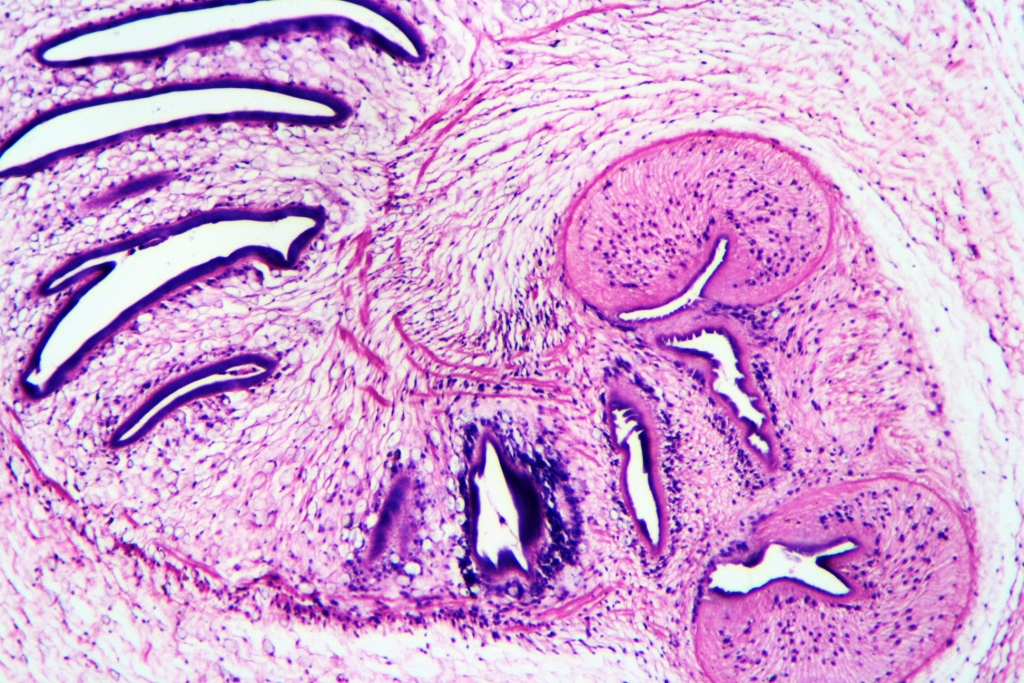
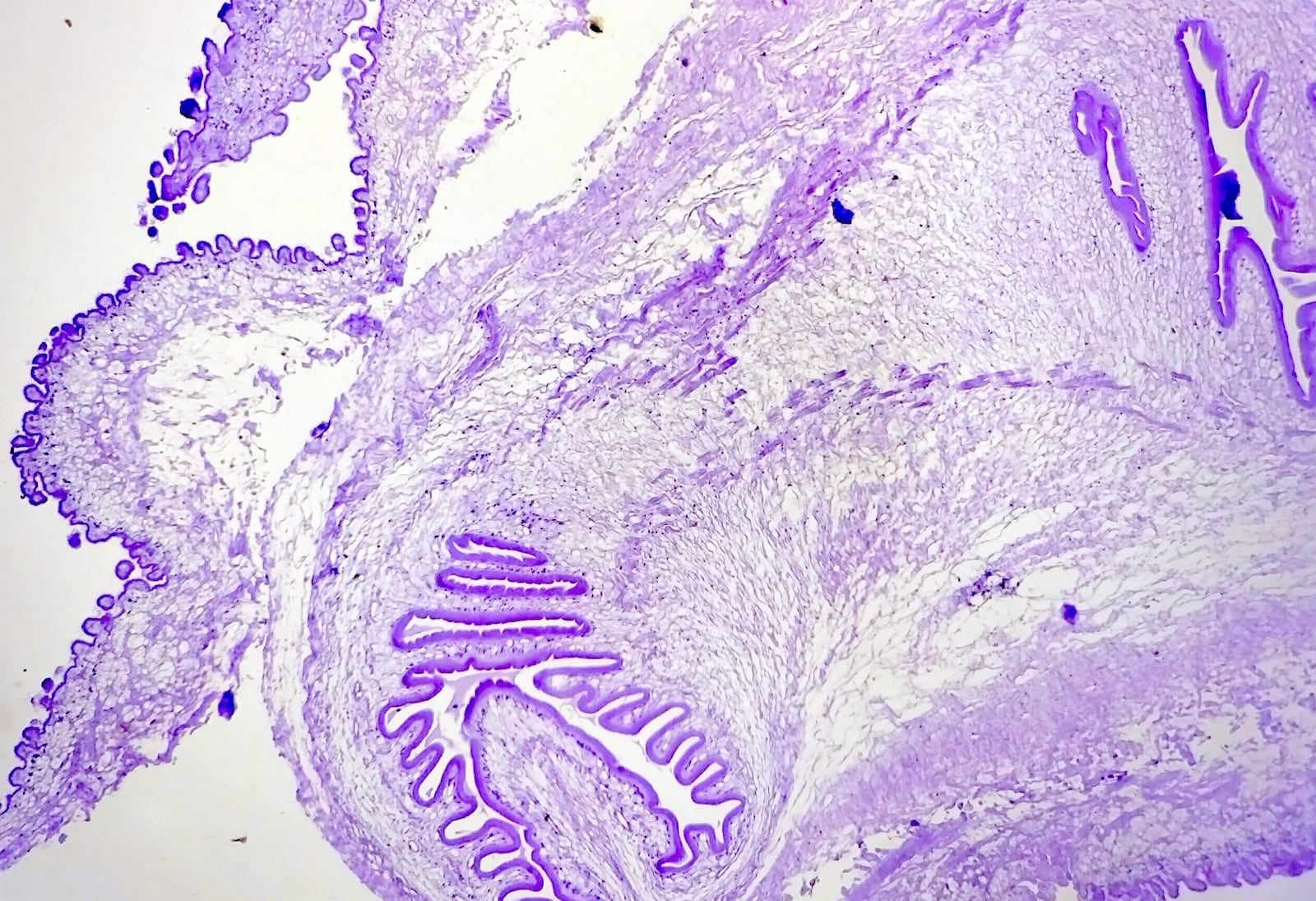
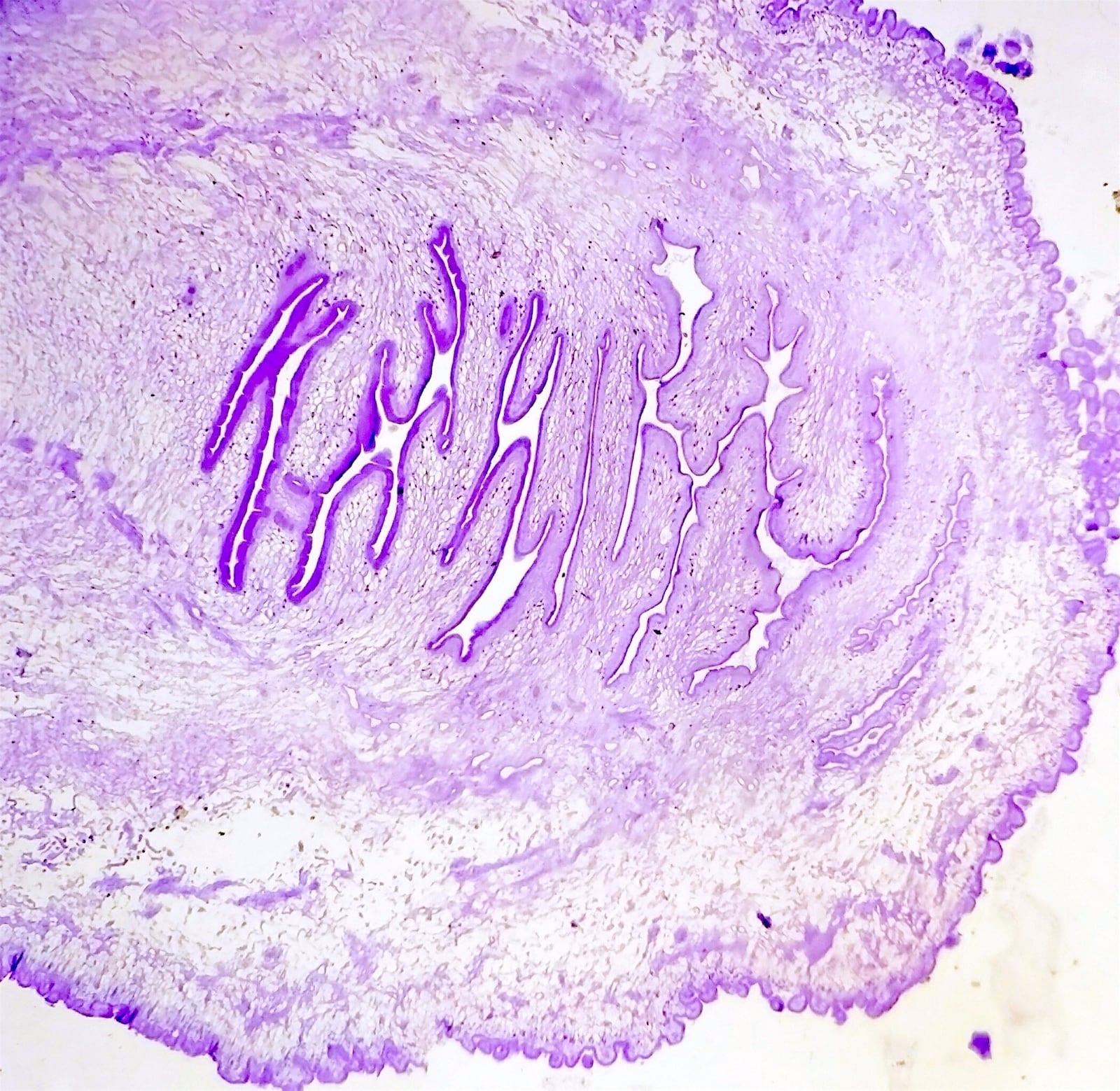
- Cystic cavity contains the the larval form: scolex with hooklets and 2 pairs of suckers
- The larval form, composed of duct-like invaginations, is lined by a double layered, eosinophilic membrane
- Scolex is single and invaginated; contains a rostellum, 4 suckers and 22 - 23 bifrefringent hooklets (may persist for a long time)
- Body wall exhibits a myxoid matrix and calcareous bodies (calcified concretions)
- Cysticerci may remain viable for years
- Colloidal stage: first stage of involution of cysticerci; transparent vesicular fluid is replaced by a turbid, viscous fluid and the scolex shows signs of hyaline degeneration
- Granular stage: cysticercus is no longer viable; cyst wall thickens and the scolex is transformed into coarse mineralized granules
- Host inflammatory reaction is usually not present if the larva is viable
- Finally, a granulomatous reaction develops characterized by histiocytes, epitheloid cells and foreign body giant cells, leading to fibrosis of the supporting stroma and calcification of the parasitic debris
Microscopic (histologic) images
Contributed by Thiriveni Balajji, M.D., M. Kavitha, M.D., Case #458 and Case #115

Subcutaneous cysticercosis with neurocysticercosis



CNS

Eyelid
Cytology description
- Fibrillary stroma with interspersed nuclei and a honeycomb pattern
- Parts of parasite may be identifiable (Acta Cytol 1996;40:653)
- Background usually consists of a mixed inflammatory infiltrate (Acta Cytol 1989;33:659)
- Granulomas may be seen
Cytology images
Images hosted on other servers:

Breast: larval fragment


Bladder: wall of cysticercus

Wall of cysticercus

Epithelioid cell granulomas

Wall of cysticercosis cellulosae

Inflammatory infiltrate


Fibrillary stroma
Positive stains
- Hooklets of cysticerci can be acid fast
