

Cervix
Premalignant / preinvasive lesions - cytology
ASC-H (cytology)
Authors: Joseph Reznicek, M.D., Bonnie Choy, M.D.
Editorial Board Members: David B. Chapel, M.D., Ricardo R. Lastra, M.D.

Last author update: 31 January 2023
Last staff update: 8 December 2023
Copyright: 2022-2024, PathologyOutlines.com, Inc.
PubMed Search: ASC-H
Table of Contents
Definition / general | Essential features | CPT coding | Sites | Diagrams / tables | Clinical features | Laboratory | Management | Cytology description | Cytology images | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Reznicek J, Choy B. ASC-H (cytology). PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/cervixASCH.html. Accessed April 25th, 2024.
Definition / general
- Atypical squamous cells - cannot exclude high grade squamous intraepithelial lesion (ASC-H) refers to cytologic changes that are suggestive of high grade squamous intraepithelial lesion (HSIL) but insufficient for a definitive interpretation
Essential features
- Criteria are based on the 2014 Bethesda System for Reporting Cervical Cytology (Nayar: The Bethesda System for Reporting Cervical Cytology, 3rd Edition, 2015)
- Usually sparse in cellularity
- Cells resemble immature (basal or parabasal) squamous cells with high N:C ratios
- Nuclei are ~1.5 - 2.5x larger than normal intermediate nuclei and show nuclear abnormalities
- Differential diagnosis includes HSIL as well as changes that are not related to human papillomavirus (HPV) infection and neoplasia (e.g., squamous metaplasia, atrophy and intrauterine device [IUD] effect)
CPT coding
- For screening Pap tests (routine and high risk): smear
- For screening Pap tests (routine and high risk): liquid based
- Manual screening only
- ThinPrep imager assisted screening
- FocalPoint (instrument only)
- FocalPoint (with manual screening)
- For diagnostic Pap tests: smear
- For diagnostic Pap tests: liquid based
- Manual screening only
- ThinPrep imager assisted screening
- FocalPoint (instrument only)
- FocalPoint (with manual screening)
Sites
- Cervix, vagina, anus

Clinical features
- Accounts for 0.3% (median) of all Pap test results (Arch Pathol Lab Med 2010;134:331)
- Represents < 10% of all ASC interpretations (Nayar: The Bethesda System for Reporting Cervical Cytology, 3rd Edition, 2015)
Laboratory
- HPV testing may be used as part of screening, triage and surveillance (J Am Soc Cytopathol 2020;9:291)
- Initially endorsed in 2001 as triage test for ASCUS (ASC of undetermined significance) cytologic result
- Approved for:
- Cotesting in 2003
- Postcolposcopic / posttreatment follow up and risk stratification using partial genotype (HPV 16/18) in 2006
- Primary screening option in 2014
- 5 FDA approved HPV testing platforms:
- Qiagen Hybrid Capture
- Hologic Cervista
- Hologic Aptima
- Roche Cobas (FDA approved for primary screening)
- Becton Dickinson Onclarity (FDA approved for primary screening)
- Note: HPV result plays no role in the cytologic examination or grading of SIL
Management
- 2019 American Society of Colposcopy and Cervical Pathology (ASCCP) risk based management consensus guidelines for abnormal cervical cancer screening tests and cancer precursors (J Low Genit Tract Dis 2020;24:102)
- Personalized risk based recommendations based on a patient's risk of cervical intraepithelial neoplasia (CIN) 3+, as determined by a combination of current results and past history (including unknown history)
- Unlike prior versions, the 2019 guidelines do not provide management algorithms for most screening and triage scenarios
- For patients < 25 years old with ASC-H cytology, colposcopy is recommended (refer to the management algorithm in Diagrams / tables)
- For patients ≥ 25 years old with ASC-H cytology:
- Colposcopy is recommended if HPV status is unknown or negative
- Colposcopy / treatment is recommended if HPV positive (untyped or genotyped)
- Use the website or mobile app to calculate risk estimate and determine individualized management recommendation for patients
- 5 year risks for histologic HSIL and cancer for cytology samples interpreted as ASC-H with high risk HPV testing (N Engl J Med 2013;369:2324):
- ASC-H with negative HPV: 12%
- ASC-H with positive HPV: 45%
- Reference: J Low Genit Tract Dis 2020;24:102
Cytology description
- Usually sparse cells
- Common cytologic patterns of ASC-H that are suggestive of HSIL but insufficient for a definitive interpretation (Nayar: The Bethesda System for Reporting Cervical Cytology, 3rd Edition, 2015):
- Small cells with high N:C ratios (atypical immature metaplastic cells)
- Seen in rare single cells or in small groups (< 10 cells)
- Enlarged nuclei (1.5 - 2.5x larger than normal intermediate nuclei)
- Some nuclear abnormalities; features such as coarse chromatin, focal irregular nuclear contour and hyperchromasia favor an interpretation of HSIL
- Crowded sheet pattern:
- Crowded squamous cells with atypical nuclear features, loss of polarity or are difficult to visualize
- Features such as dense cytoplasm, polygonal shape of the cell and sheets with sharp linear edges favor squamous over glandular differentiation (Hum Pathol 1999;30:816)
- Small cells with high N:C ratios (atypical immature metaplastic cells)
Cytology images
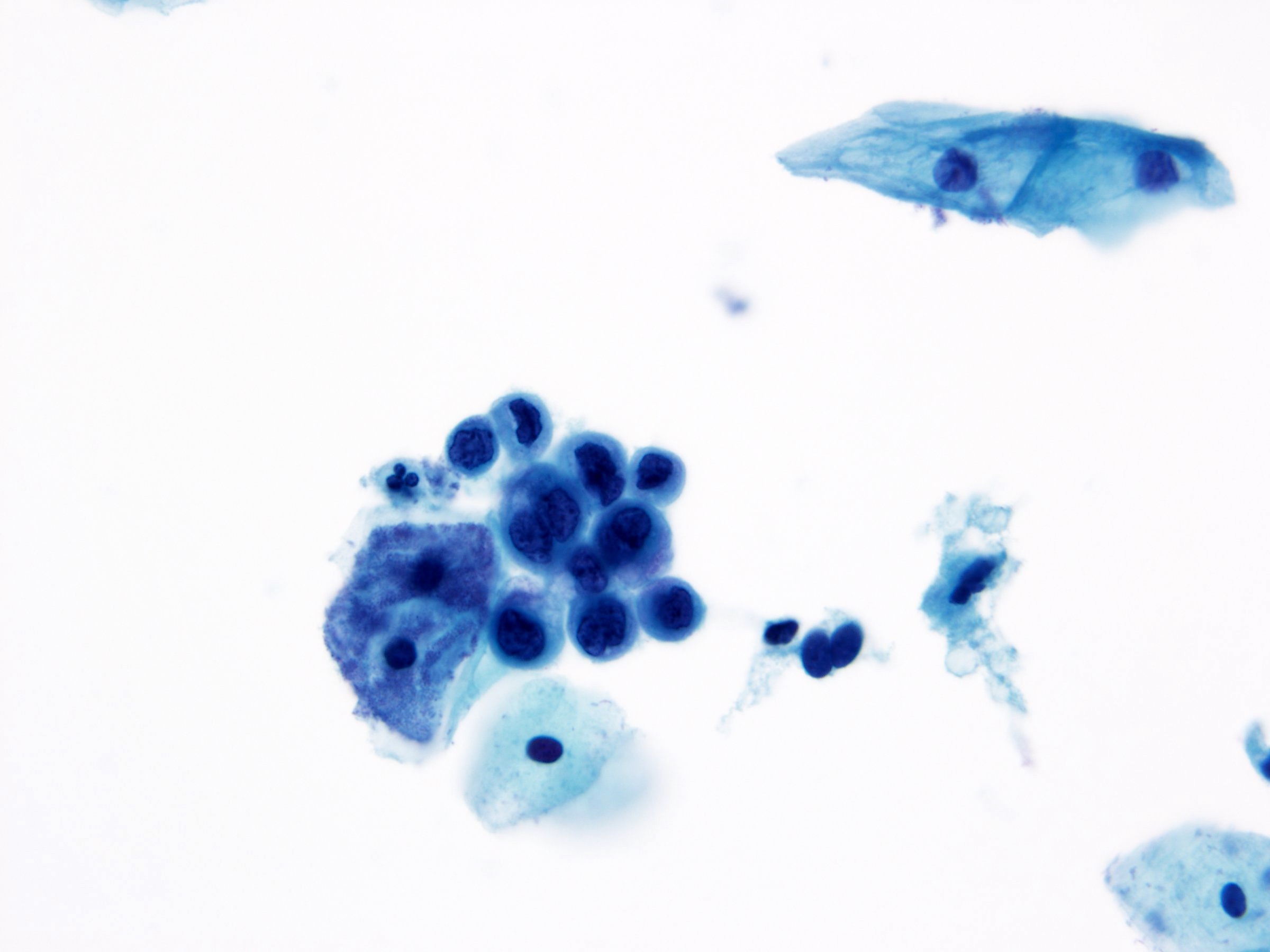
Contributed by Bonnie Choy, M.D.
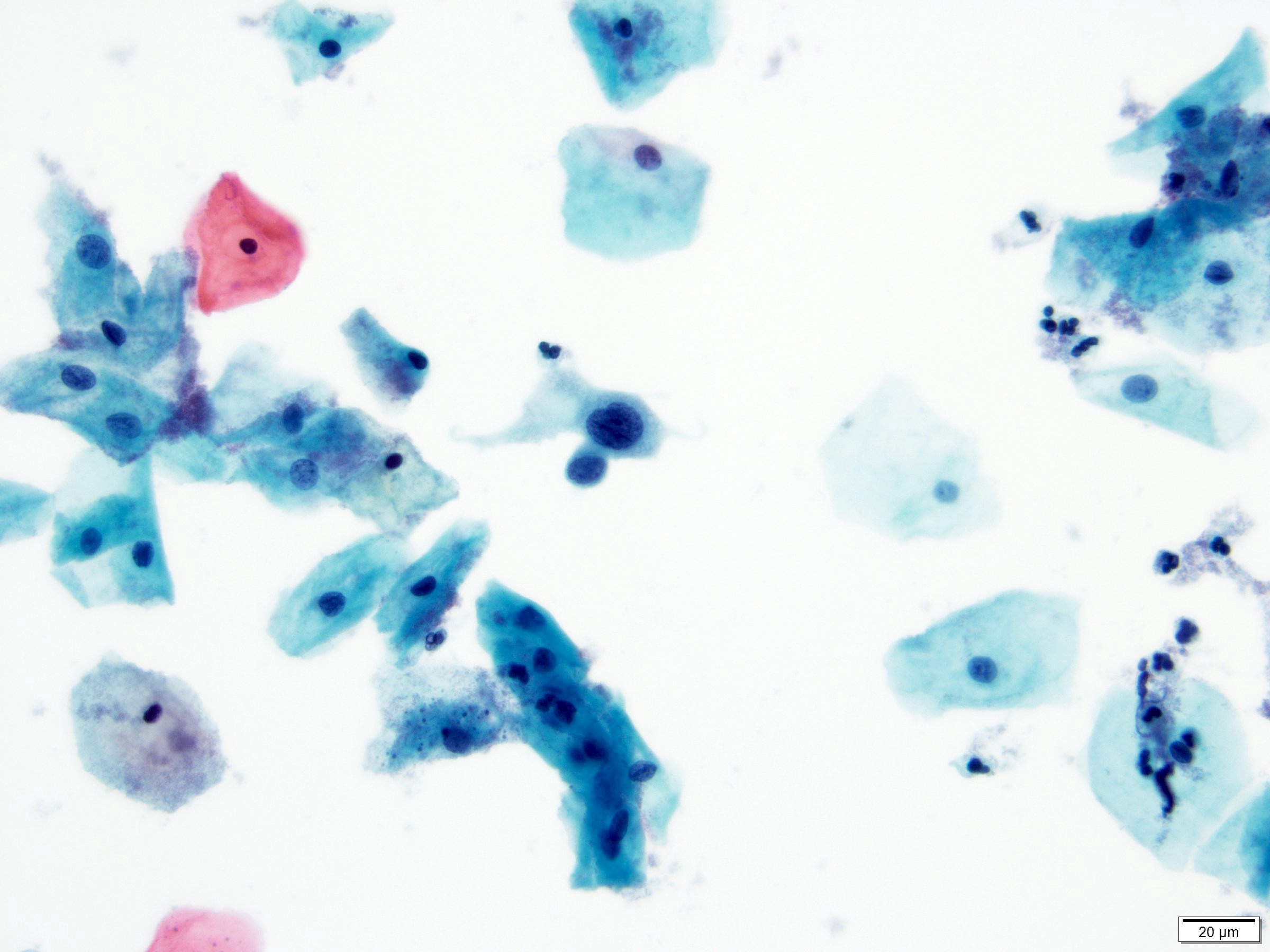
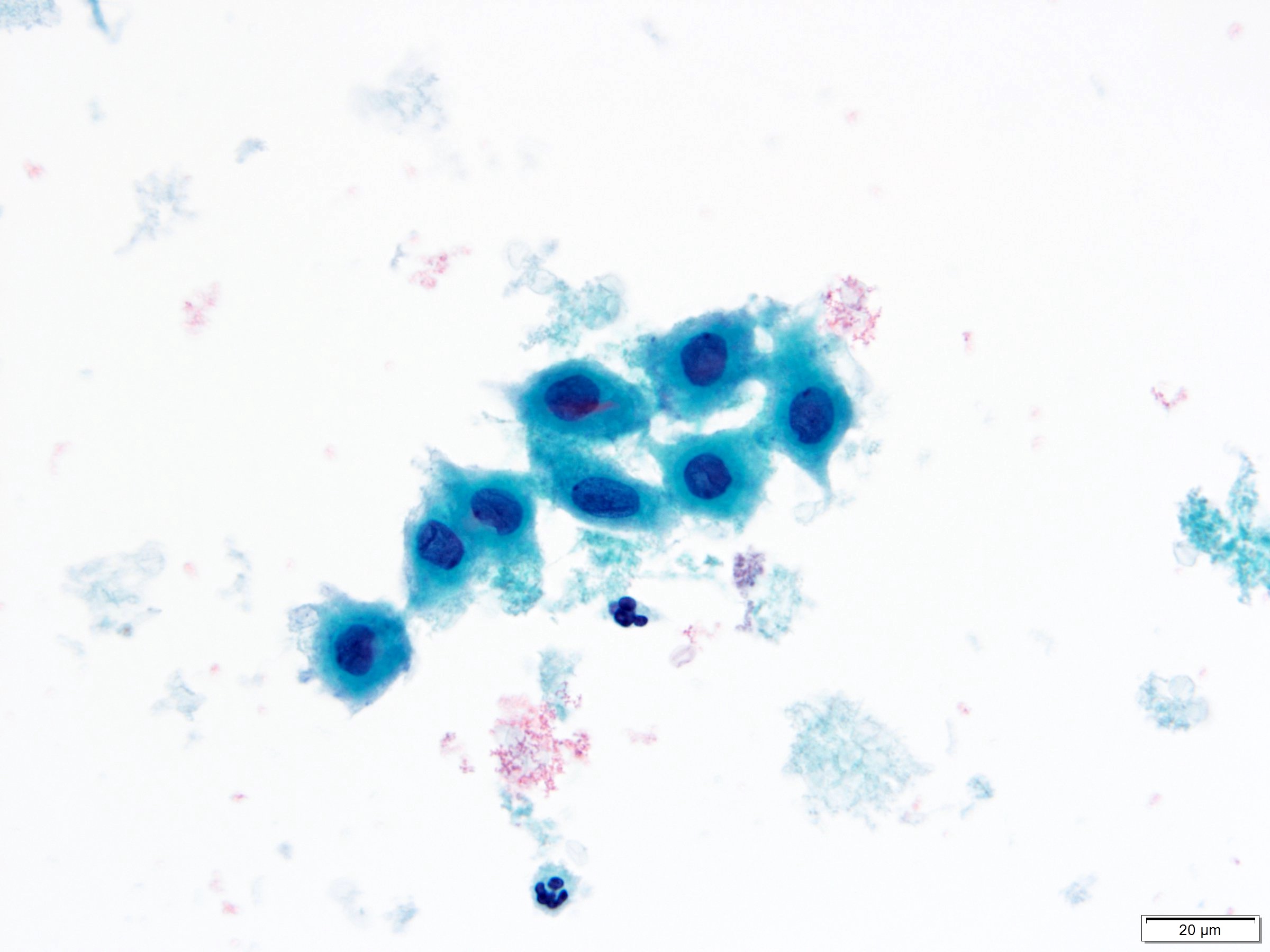
High N:C ratio
Irregular nuclear membranes and hyperchromasia

HSIL
Squamous metaplasia
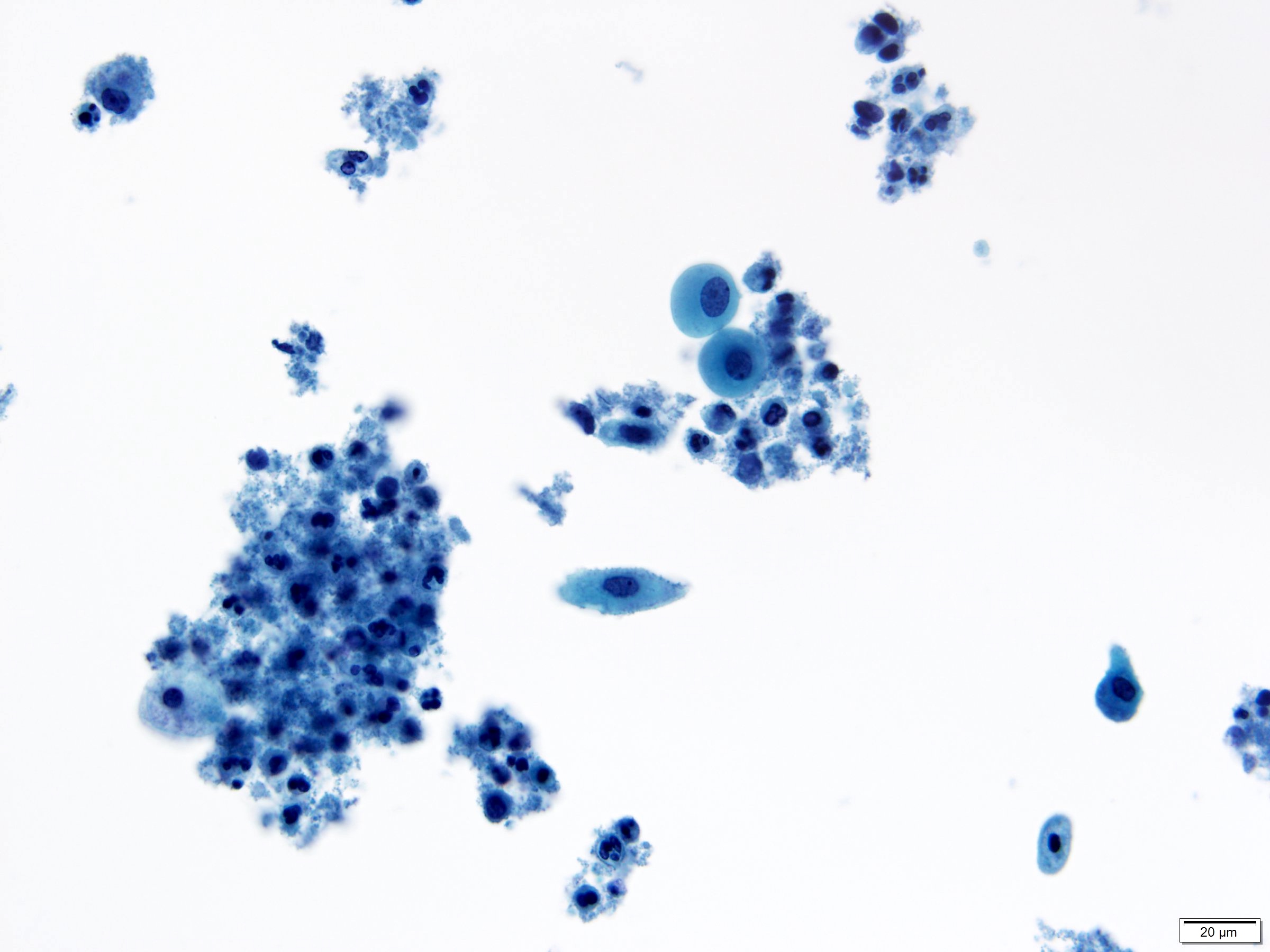
Atrophy with inflammation

Endometrial cells
Images hosted on other servers:

WHO digital atlas
Sample pathology report
- Statement of adequacy:
- Satisfactory for evaluation
- Transformation zone component present
- Final interpretation:
- Epithelial cell abnormality, squamous cell
- Atypical squamous cells - cannot exclude a high grade squamous intraepithelial lesion (ASC-H)
Differential diagnosis
- HSIL:
- Approximately the size of parabasal cells
- Nuclear atypia, including nuclear enlargement, irregular nuclear contours with frequent prominent indentations / grooves, generally hyperchromatic, lack of nucleoli
- High N:C ratio
- Squamous metaplasia:
- Less nuclear enlargement and lower N:C ratio
- Minimal to mild nuclear membrane abnormalities
- If reactive, may have nucleoli
- Atrophy:
- Variable N:C ratio
- Smooth nuclear contours / membranes
- Smudgy or degenerated nuclear chromatin
- No mitoses
- Blood and inflammation may be present but no tumor diathesis
- Isolated endocervical cells:
- Presence of small nucleoli
- Finely granular and evenly distributed chromatin
- Smooth nuclear contours
- Granular or finely vacuolated cytoplasm, occasionally with some elongation
- Exfoliated cells may have rounded up appearance and high N:C ratio
- Retain columnar cytoplasmic configuration with eccentrically placed nuclei
- Exfoliated endometrial cells:
- Small cells with dark nuclei and scant cytoplasm
- Small nucleoli may be seen
- Apoptotic bodies may been present within shedding endometrial groups
- IUD effect:
- May present as isolated cells with high N:C ratio
- Degenerative nuclei with wrinkled chromatin
- Usually more regular nuclear membranes
- Presence of nucleoli
- Histiocytes:
- Small to medium sized, oval kidney bean nuclei
- Sometimes prominent longitudinal groove
- Finely textured, normochromatic
- Abundant foamy vacuolated cytoplasm
Board review style question #1
The cervical cytology specimen shown above is from a 35 year old woman. What is the most likely interpretation?
- Atypical glandular cells, NOS
- Atypical squamous cells - cannot exclude HSIL (ASC-H)
- Atypical squamous cells - undetermined significance (ASCUS)
- Low grade squamous intraepithelial lesion (LSIL)
Board review style answer #1
Board review style question #2
A cervical cytology specimen shows very rare cells with nuclear atypia, irregular nuclear contours and high N:C ratios, concerning but not definitive for the diagnosis of high grade squamous intraepithelial lesion. What is the best interpretation?
- Atypical squamous cells - cannot exclude HSIL (ASC-H)
- Atypical squamous cells - undetermined significance (ASCUS)
- High grade squamous intraepithelial lesion (HSIL)
- Low grade squamous intraepithelial lesion (LSIL)
Board review style answer #2
