

Cervix
Mesenchymal / mixed epithelial & mesenchymal tumors
Adenomyoma
Author: Leonel Maldonado, M.D.

Last author update: 1 August 2016
Last staff update: 11 April 2024 (update in progress)
Copyright: 2007-2024, PathologyOutlines.com, Inc.
PubMed Search: Adenomyoma of endocervical type
Table of Contents
Definition / general | Essential features | ICD coding | Epidemiology | Sites | Clinical features | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Differential diagnosis | Additional referencesCite this page: Maldonado L. Adenomyoma . PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/cervixadenomyoma.html. Accessed April 19th, 2024.
Definition / general
- Rare and frequently underdiagnosed biphasic tumor composed of benign endocervical glands and smooth muscle typically located in the endocervix, first described in 1996 (Mod Pathol 1996;9:220)
Essential features
- Usually an incidental finding in women of reproductive or postmenopausal age (mean age 40 years)
- Presents as a polyp or mass protruding through the external cervical os, resulting in abnormal bleeding or vaginal discharge, causing concern for malignancy
- Well circumscribed neoplasm composed of irregularly shaped, benign endocervical-type glands, often in a lobular arrangement, admixed with myomatous smooth muscle
- Benign with an excellent prognosis if completely removed
ICD coding
- Suggested ICD-10 Code(s):
- D26.0: other benign neoplasm of cervix uteri
- N84.1: polyp of cervix uteri
- N88.8: other specified noninflammatory disorders of cervix uteri
- N88.9: non-inflammatory disorder of cervix uteri, unspecified
Epidemiology
- Women of reproductive or post-menopausal age (mean age 40 years)
Sites
- Arises from endocervix
- Endometrioid type adenomyomas (not described here) usually originate from the endometrium, but could also arise from the endocervix
Clinical features
- Usually an incidental finding
- May be asymptomatic; usually discovered incidentally during regular gynecologic examination
- May present as a polyp or 'fibroid' protruding through the external cervical os, or may result in abnormal bleeding or vaginal discharge, causing concern for malignancy
- Less commonly, there is cervical enlargement by a mural mass without mucosal involvement
Radiology images
Contributed by Leonel Maldonado, M.D.

MRI of the pelvis
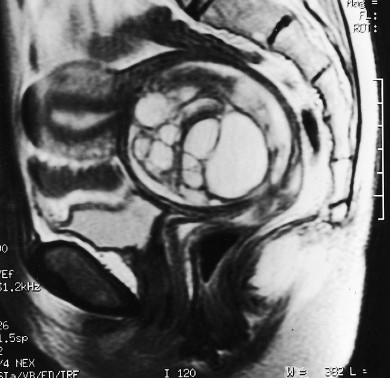
Sagittal T2
Prognostic factors
- Excellent prognosis if completely removed by local excision or simple hysterectomy
Case reports
- 28 and 35 year old women with polypoid adenomyoma of endocervical type (IJBAMR 2015;4:162)
- 44 year old Japanese woman with increasing genital mucinous discharge (Pathol Int 1999;49:1019)
- 44 year old woman with endocervical adenomyoma (APMIS 2001;109:546)
- 53 year old asymptomatic Japanese woman with polypoid adenomyoma of endocervical type (Case Rep Pathol 2014;2014:275421)
- 53 year old woman with reactive atypia and goblet cell differentiation (Obstet Gynecol cases Rev 2015;2:6)
- 55 year old Caucasian woman with intraepithelial mucinous carcinoma arising in an endocervical mucinous adenomyoma (J Reprod Med 2005;50:643)
- 56 year old woman with MR imaging (Radiography 2008;14:162)
- Series of 10 cervical adenomyomas of endocervical type (Histopathology 2015;66:420)
Treatment
- Local excision or simple hysterectomy
Clinical images
Images hosted on other servers:

Bulging tumor from anterior cervix (fig 1)
Gross description
- Usually well circumscribed, unencapsulated and solitary; may be polypoid if submucosal
- White to gray to tan cut surface
- The epithelial component may be seen as mucin filled cysts, while the mesenchymal areas have a firm consistency with a whorled cut surface
Gross images
Contributed by Leonel Maldonado, M.D.
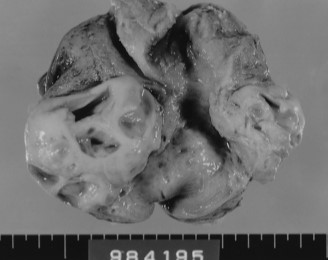
Endocervical mural tumor

Polypoid mass from uterine cervical wall

Polypoid mass with numerous cysts
Microscopic (histologic) description
- Well circumscribed, unencapsulated neoplasm composed of irregularly shaped benign endocervical type glands, often in a lobular arrangement, admixed with myomatous smooth muscle
- Endocervical cells have basal nucleus with abundant pale cytoplasm and may show tubal or tuboendometrioid metaplasia
- The smooth muscle component forms variably sized and shaped fascicles embedded in a collagenous background; cells have bland cytologic features with eosinophilic cytoplasm and spindled cigar shaped nuclei
- Mitotic activity is absent in both epithelial and smooth muscle components
- No desmoplastic response is evident
Microscopic (histologic) images
Contributed by Leonel Maldonado, M.D.
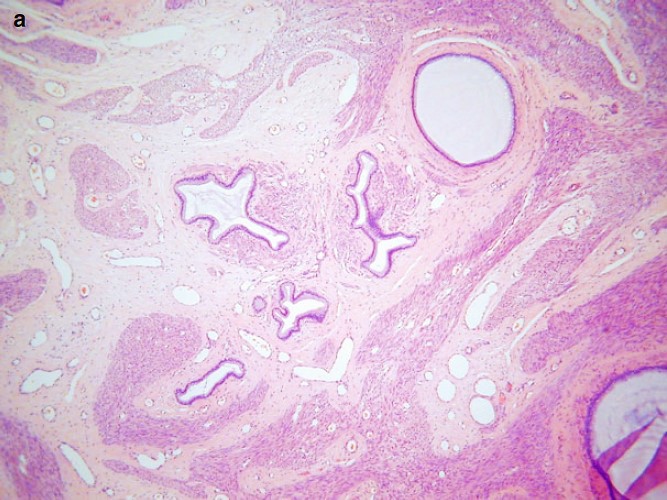
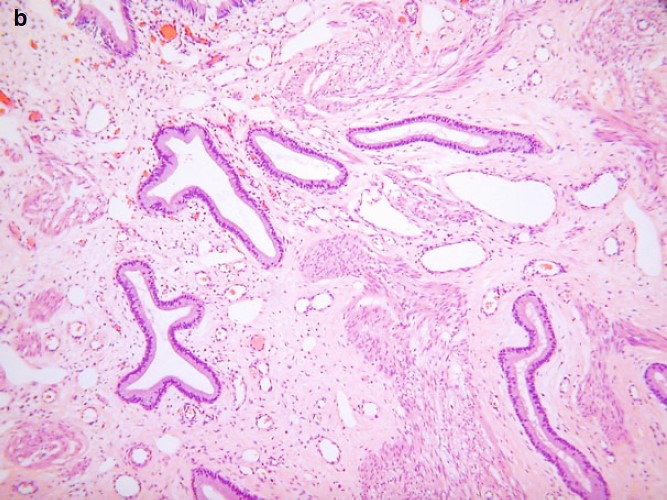
Endocervical type glands surrounded by smooth muscle
Cytology description
- Endocervical polyps in general have no specific cytological pattern, except for the rare finding of a fragment of a polyp in smears which, when present, display smooth borders lined by columnar cells, pale intermediate zones and dark inner cores of numerous small, dark stromal cells
- Otherwise, cervical smears present considerable numbers of benign endocervical cells, shedding in large sheets or forming glands
- Spindled smooth muscle cells present as cohesive fragments with frayed edges revealing spindle cells with bipolar cytoplasmic processes
- Metaplastic and reactive endocervical cells in an inflammatory background can be present as well
Cytology images
Contributed by Leonel Maldonado, M.D.

Fragment of endocervical polyp
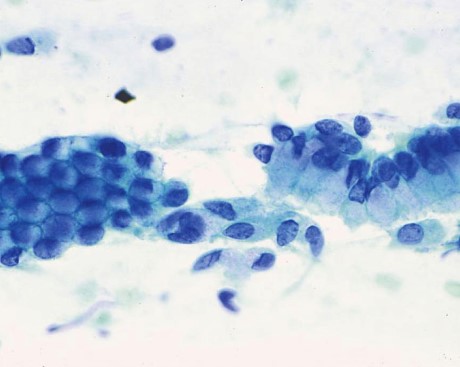
Benign endocervical cells
Positive stains
- Intracytoplasmic mucin: alcian blue / PAS positive
- Endocervical epithelium: PAS, luminal CEA (variable), nuclear ER, nuclear PR (variable), variable Ki67; mucin core proteins, such as MUC5AC, MUC1 and MUC6 are positive (Case Rep Pathol 2014;2014:275421)
- Smooth muscle: smooth muscle actin and nuclear ER
Negative stains
- Glandular epithelium negative for HIK1083 (M-GGMC-1), useful to distinguish from adenoma malignum; lysozyme and chromogranin A negative (APMIS 2001;109:546)
Differential diagnosis
- Adenoma malignum (minimal deviation adenocarcinoma):
- Glands lined by cells with abundant cytoplasm reminiscent of pyloric type epithelium (HIK1083 and cytoplasmic CEA positive), with at least focal malignant cytologic features and rarely identified mitotic figures
- Lymphovascular and perineural invasion
- Lobular endocervical glandular hyperplasia:
- Lobular arrangement of hyperplastic small / medium sized, rounded endocervical glands lined mostly by single layer of columnar, mucin rich epithelium
- Lacks a prominent component of smooth muscle
- Mesonephric adenomyoma:
- Lobular arrangement of dilated gland of nonmucinous type lined by simple cuboidal epithelium with scant cytoplasm and luminal eosinophilic colloid-like material
- Abundant stromal smooth muscle; glands are ER / PR negative and vimentin / CD10 positive (Histopathology 2015;66:420)
- Tunnel clusters:
- Lobular proliferation of often dilated endocervical glands (clefts) with side channels growing out of them
- Benign nuclear features with minimal atypia and no smooth muscle component
Additional references
- Mutter: Pathology of the Female Reproductive Tract, 2014, 3rd ed, Kurman: Blaustein's Pathology of the Female Genital Tract, 2011, 6th ed, McCluggage: Cellular Pathology of Glandular Lesions and Uncommon Neoplasms of the Cervix, 2014, Jiménez-Ayala: Cytopathology of the Glandular Lesions of the Female Genital Tract, 2010, 1st ed, Nayar: The Bethesda System for Reporting Cervical Cytology: Definitions, Criteria, and Explanatory Notes, 2015, 3rd ed
