Colon
Neuroendocrine tumors
Poorly differentiated neuroendocrine carcinoma
Author: Raul S. Gonzalez, M.D.

Last author update: 2 February 2021
Last staff update: 15 January 2025
Copyright: 2019-2025, PathologyOutlines.com, Inc.
PubMed Search: Neuroendocrine carcinoma colon
Table of Contents
Definition / general | Essential features | Terminology | Sites | Epidemiology | Clinical features | Prognostic factors | Case reports | Radiology images | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Electron microscopy description | Sample pathology report | Differential diagnosis | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2 | Practice question #3 | Practice answer #3Cite this page: Gonzalez RS. Poorly differentiated neuroendocrine carcinoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/colontumorneuroendocrinecarcinoma.html. Accessed August 26th, 2025.
Definition / general
- Poorly differentiated neuroendocrine malignancy, including large cell and small cell neuroendocrine carcinoma (Am J Surg Pathol 2008;32:719, Am J Clin Pathol 1991;95:315)
- Excludes well differentiated neuroendocrine tumors (also known as carcinoid tumors)
Essential features
- Large cell or small cell neuroendocrine carcinoma
- Rare and aggressive (distant metastases common, with poor survival rate)
- Histology similar to neuroendocrine carcinomas elsewhere
Terminology
- Full proper term is poorly differentiated neuroendocrine carcinoma
- 2 subtypes, based on morphology: large cell neuroendocrine carcinoma and small cell carcinoma
Sites
- Usually in cecum or right colon but can arise anywhere
Epidemiology
- Disease typically presents at advanced stage
Clinical features
- Presents earlier than conventional colorectal adenocarcinoma (mean age ~ 60 years) (Dis Colon Rectum 2004;47:163)
Prognostic factors
- Good prognostic factors include peritumoral lymphocytes, microsatellite instability and pure large cell features; poor prognostic factors include CD117 positivity and vascular invasion (Am J Surg Pathol 2012;36:601)
- Slightly improved prognosis if disease is not metastatic or patient responds to chemotherapy (Ann Surg Oncol 2014;21:2956)
Case reports
- 44 year old woman with overlying tubulovillous adenoma of the colon and liver (Arch Pathol Lab Med 2005;129:412)
- 70 year old man with small cell undifferentiated carcinoma of the ascending colon (Tohoku J Exp Med 2006;209:361)
- 76 year old man with primary small cell carcinoma of the cecum (Ann Diagn Pathol 2006;10:162)
- 76 year old man with small cell carcinoma of the large intestine (Arch Pathol Lab Med 2001;125:1251)
- 85 year old woman with a remote history of right sided colon cancer underwent a transverse colon resection for a newly diagnosed colon cancer (Case of the month #531)
- Primary small cell undifferentiated carcinoma of the rectum associated with ulcerative colitis (South Med J 1996;89:921)
Radiology images
Images hosted on other servers:

Rectal mass

Noncontrast CT scans of abdomen
Gross images
Contributed by Raul S. Gonzalez, M.D.

Nodular hemorrhagic lesion
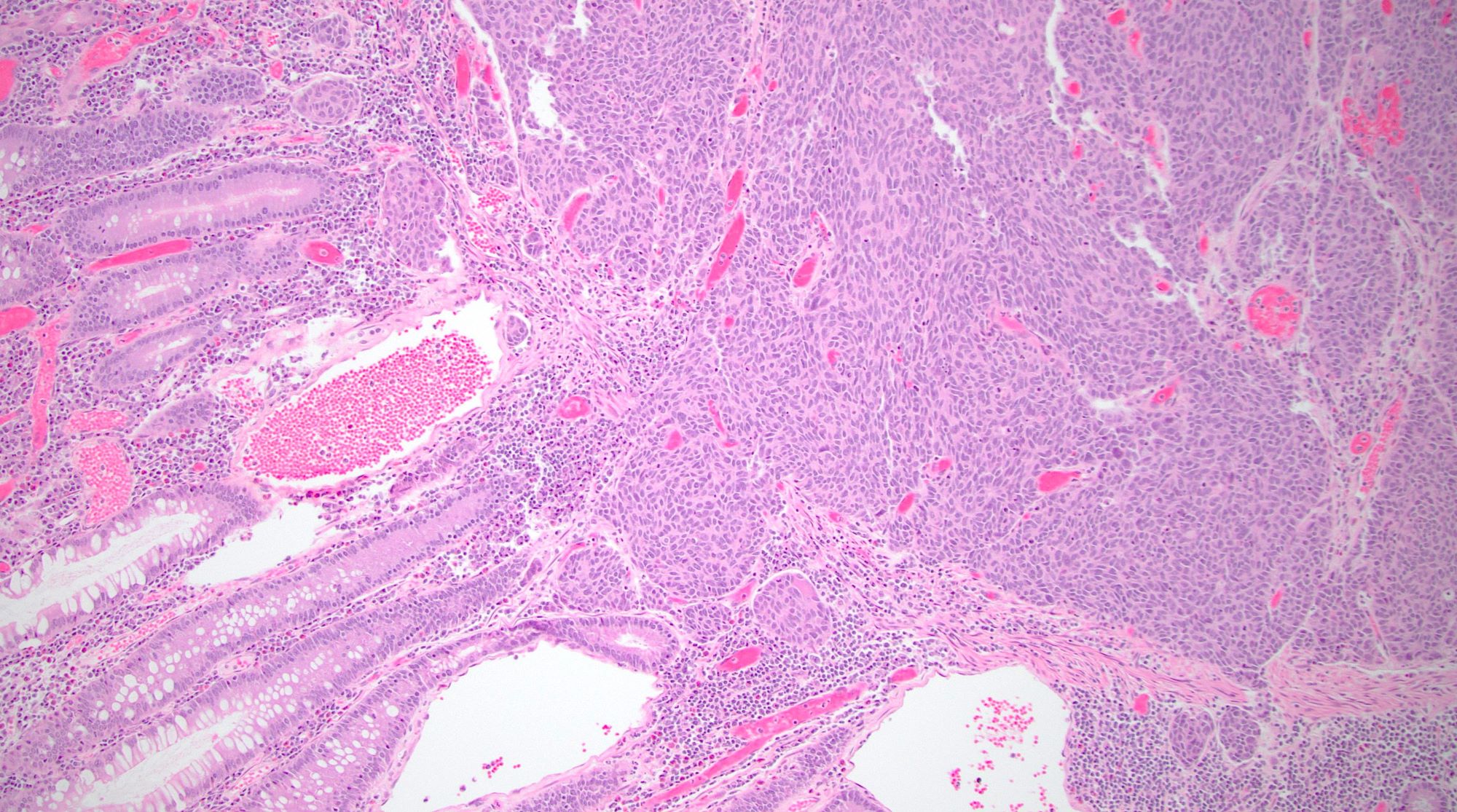
Microscopic (histologic) description
- Large cell
- Organoid arrangement of cells larger than those in small cell carcinoma, with nuclear pleomorphism and hyperchromasia, prominent nucleoli, numerous mitoses and tumor necrosis
- Small cell
- Resembles pulmonary small cell carcinoma, with sheets and nests of small ovoid cells with minimal cytoplasm, hyperchromatic nuclei with stippled chromatin, nuclear molding with peripheral palisading, brisk mitotic activity, apoptotic cells, necrosis and vascular invasion
- No prominent nucleoli or pleomorphism
- May have Azzopardi effect (encrustation of nuclear material around blood vessels)
Microscopic (histologic) images
Contributed by Raul S. Gonzalez, M.D., Aaron Huber, D.O. and Diana Agostini-Vulaj, D.O. (Case #531)
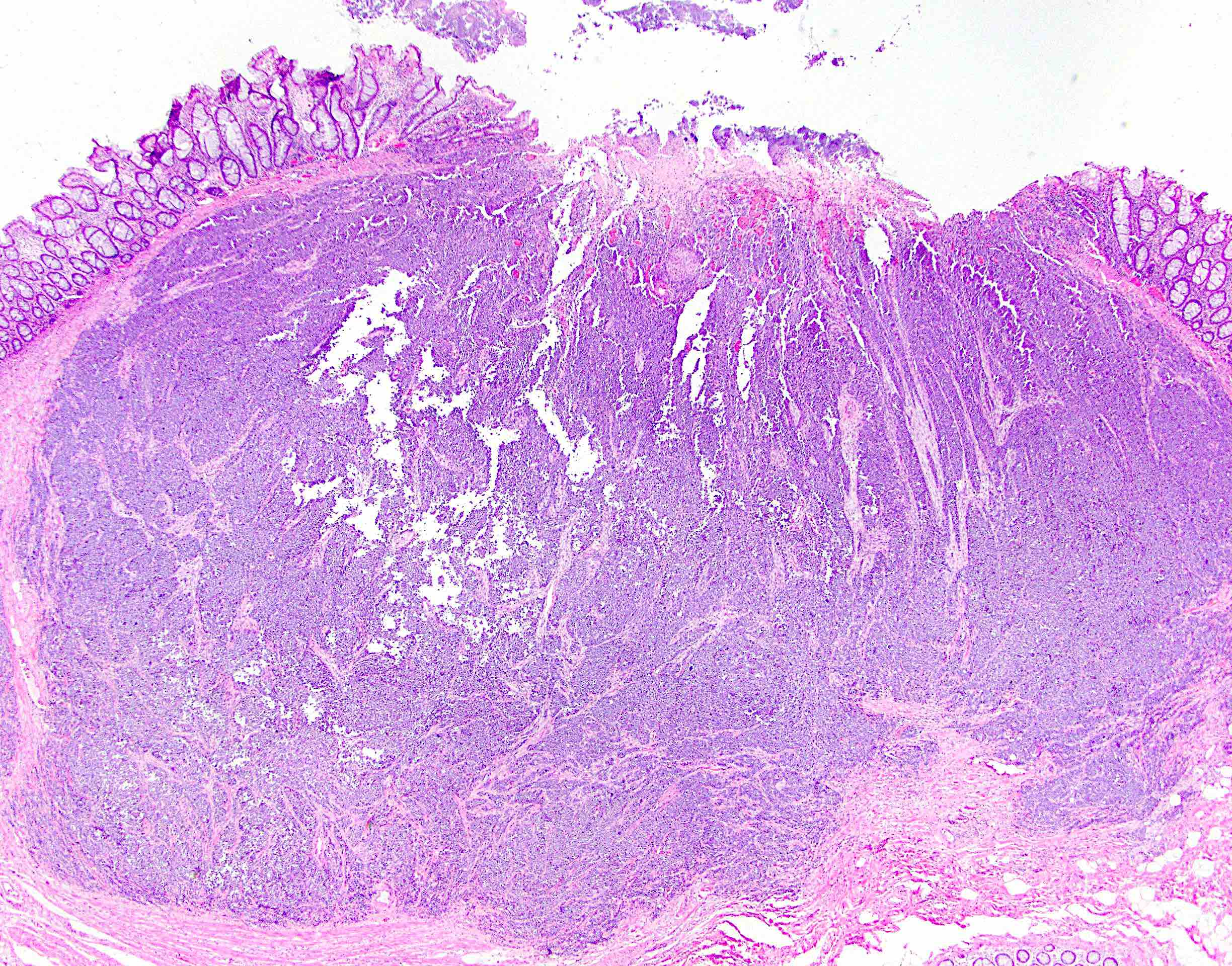
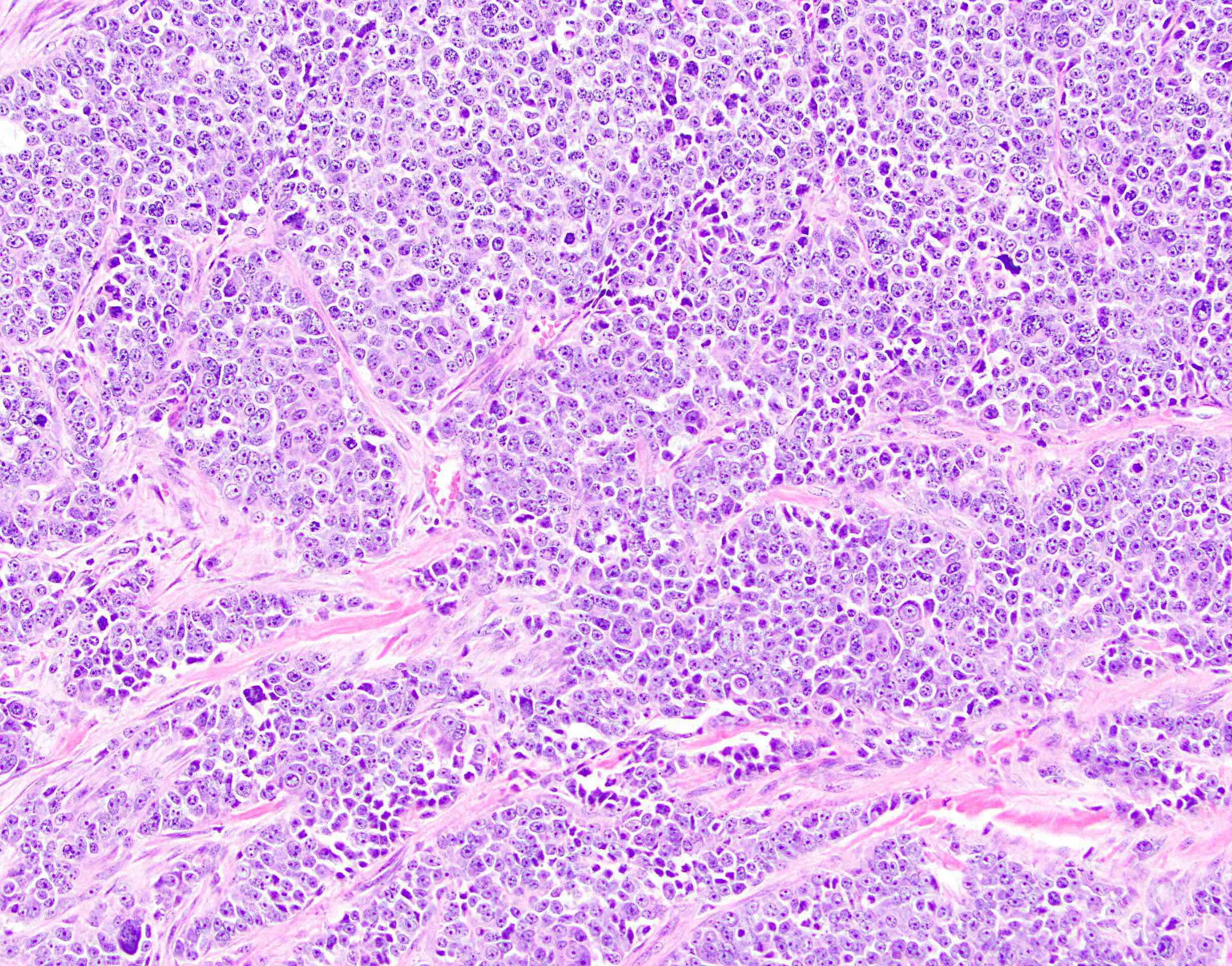
Large cell neuroendocrine carcinoma



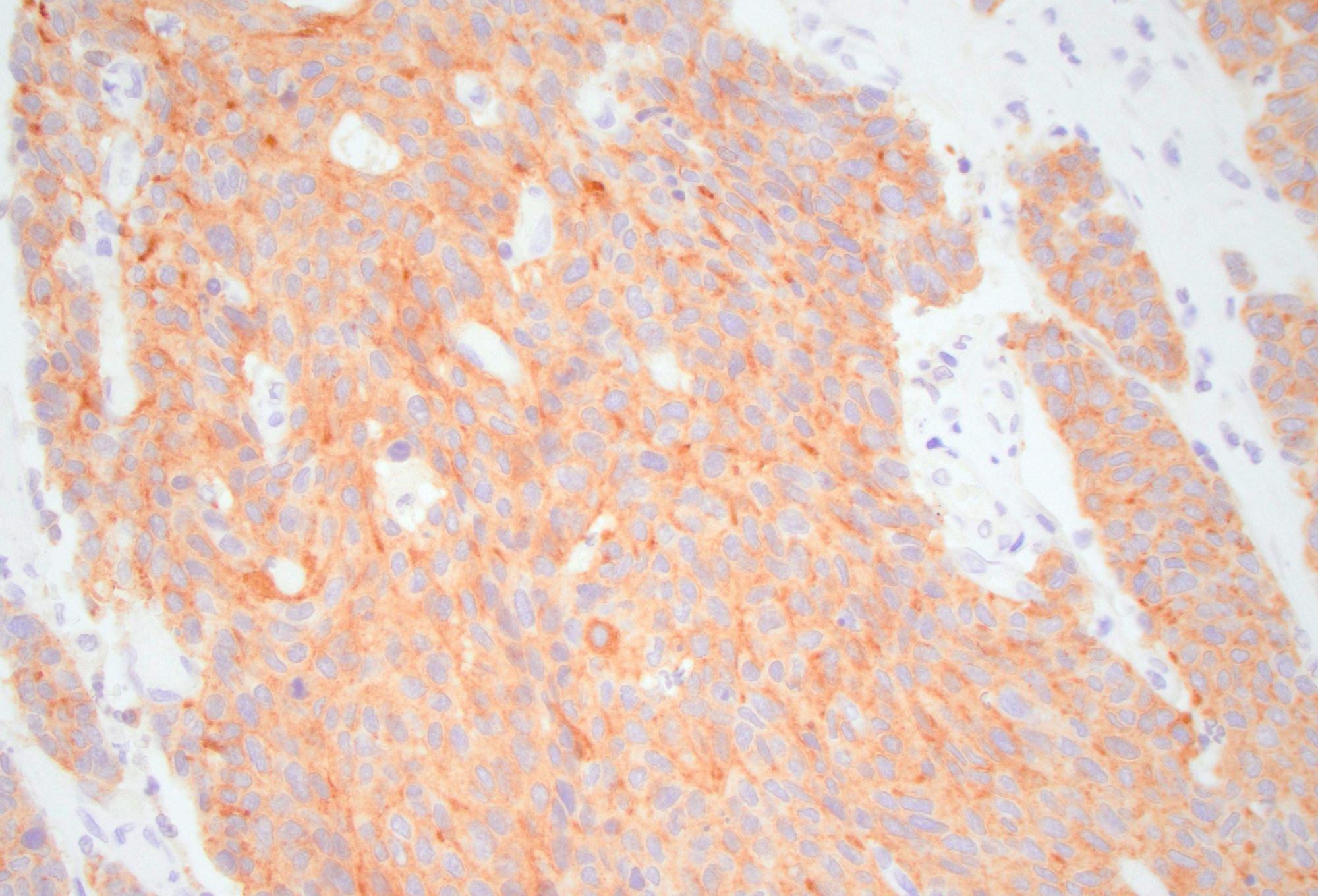
Synaptophysin

Chromogranin

INSM1
Positive stains
- Cytokeratin, synaptophysin, chromogranin; high Ki67 index (so Ki67 stain may not be necessary)
- CDX2 variable; EGFR in 70% (Diagn Pathol 2007;2:35)
- CD117 in 23%, though not associated with activating mutations (Am J Surg Pathol 2003;27:1551)
Electron microscopy description
- Dense core secretory granules
Sample pathology report
- Sigmoid colon, resection:
- Poorly differentiated neuroendocrine carcinoma (see synoptic report and comment)
- Comment: The tumor demonstrates large cell neuroendocrine carcinoma morphology. Immunostains show the tumor is positive for synaptophysin and chromogranin, with a Ki67 index of 85%. By definition, neuroendocrine carcinomas are WHO grade 3.
Differential diagnosis
- Metastatic pulmonary small cell carcinoma:
- No overlying adenoma
- More likely to be TTF1 positive (J Clin Pathol 2010;63:620)
- Mixed adenoneuroendocrine carcinoma (MANEC):
- Tumors with neuroendocrine and adenocarcinoma components of at least 30% each (Cancers (Basel) 2012;4:11)
- Adenocarcinoma with scattered neuroendocrine cells:
- Common
- Histology resembles traditional colorectal adenocarcinoma (Arch Pathol Lab Med 1998;122:912)
Practice question #1
- Which of the following is true about neuroendocrine carcinomas of the colorectum?
- Large cell and small cell subtypes have differences in prognosis and clinical management
- They are positive for synaptophysin but negative for chromogranin
- They can be any WHO grade
- They present at a younger average age than colorectal adenocarcinoma
Practice answer #1
D. They present at a younger average age than colorectal adenocarcinoma
Comment Here
Reference: Neuroendocrine carcinoma
Comment Here
Reference: Neuroendocrine carcinoma
Practice question #2
- A colorectal tumor is resected and appears to be a poorly differentiated adenocarcinoma, with focal but convincing gland formation. A synaptophysin immunostain is performed and shows patchy scattered positive staining in about 5% of cells. How should this tumor be diagnosed?
- Mixed neuroendocrine nonneuroendocrine neoplasm
- Poorly differentiated adenocarcinoma
- Poorly differentiated neuroendocrine carcinoma (large cell neuroendocrine carcinoma)
- Poorly differentiated neuroendocrine carcinoma (small cell carcinoma)
Practice answer #2
Practice question #3
- Which of the following is true of poorly differentiated neuroendocrine carcinoma, large cell type in the colon?
- INSM1 expression is a sensitive and specific immunohistochemical marker for neuroendocrine differentiation
- Mixed neuroendocrine nonneuroendocrine neoplasm may be diagnosed if the poorly differentiated neuroendocrine carcinoma comprises only 5% of the total tumor volume
- This tumor has an overall good prognosis
- This tumor is a common morphologic subtype of colorectal cancer
Practice answer #3
A. INSM1 (insulinoma associated protein 1) is a sensitive and specific marker of neuroendocrine differentiation in neuroendocrine neoplasms. Answer B is incorrect because the WHO criteria for mixed neuroendocrine nonneuroendocrine neoplasm requires at least 30% of each component. Answers C and D are incorrect because LCNEC of the colon is a rare highly aggressive subtype of colorectal cancer with a poor prognosis. See Case #531 for more information.
Comment Here
Reference: Neuroendocrine carcinoma
Comment Here
Reference: Neuroendocrine carcinoma
