
Esophagus
General
Grossing & features to report
Author: Israh Akhtar, M.D.
Editorial Board Member: Aaron R. Huber, D.O.
Deputy Editor-in-Chief: Catherine E. Hagen, M.D.

Last author update: 5 August 2022
Last staff update: 14 September 2023
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Esophagus gross specimen
Table of Contents
Definition / general | Relevant clinical history for esophageal specimens | Procedure - biopsies | Procedure - esophagectomies | Procedure - endoscopic mucosal resections | Sections to obtain | Tips | Diagrams / tables | Frozen section | Gross description | Gross images | Sample gross description report | Gross differential diagnosis | Features to report - general | Features to report - biopsies | Features to report - endoscopic resection, esophagectomy or esophagogastrectomy | Features to report - optional | Board review style question #1 | Board review style answer #1Cite this page: Akhtar I. Grossing & features to report. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/esophagusgrossing.html. Accessed April 19th, 2024.
Definition / general
- This topic describes how to gross esophageal biopsies, esophagectomy specimens and endoscopic mucosal resection specimens
- Essential clinical history
- Gross differential diagnosis
- Features to report in biopsies, esophagectomies and mucosal resections (Arch Pathol Lab Med 2015;139:1446)
Relevant clinical history for esophageal specimens
- Organ / tissue resected or biopsied
- Indication for the procedure
- Endoscopic appearance of lesion / tissue sampled (e.g., mass, ulcer, stricture)
- Gross appearance of the organ / lesion / tissue sampled
- Location of biopsies:
- Upper (cervical), middle (midthoracic) or lower esophagus (lower thoracic)
- How many centimeters from the incisors on esophagogastroduodenoscopy (EGD)
- Relevant clinical and imaging findings (e.g., history of caustic ingestion)
- Prior surgery / biopsies and results (e.g., history of Barrett esophagus)
- Prior malignancy
- Prior treatment (e.g., neoadjuvant therapy, chemo or radiotherapy)
- Immune status (e.g., history of HIV, transplant)
- References: Pathology Resident Wiki: Gastrointestinal Grossing [Accessed 21 June 2022], Lester: Manual of Surgical Pathology, 3rd Edition, 2010, Gupta: Ace My Path - Gross Dictation Handbook, 1st Edition, 2022, Arch Pathol Lab Med 2015;139:1446
Procedure - biopsies
- Biopsies performed for evaluation of heartburn, dysphagia or surveillance of dysplasia in a patient with history of Barrett esophagus
- Patient identification: patient name, (last, first) label - designated specimen
- Received in formalin / unfixed
- Count the number of tissue fragments and describe their color
- Filter small fragments through tissue paper / biopsy bags
- Record the aggregate measurement or give the range, if multiple pieces
- Submit all tissue for processing in 1 cassette, if < 6 pieces
- Reference: Arch Pathol Lab Med 2015;139:1446
Procedure - esophagectomies
- Esophagectomies are performed with or without proximal stomach for severe dysplasia or for neoplasms; less frequently for strictures
- Patient identification: patient name, (last, first) label - designated specimen
- Received in formalin / unfixed / fresh for intraoperative consultation
- Confirm procedure as esophagectomy or other
- Orientation: identify anatomic structures, only esophagus or esophagus and portion of stomach or other; look for any sutures to identify the margins
- Remove the staple line with scissors, as close to the staples as possible
- Locate the lesion by gently palpating the luminal surface
- Open the specimen longitudinally
- Avoid cutting across any palpable lesions
- Measure the length and diameter or circumference and wall thickness of the esophagus and attached proximal stomach, if present
- Describe the mucosa, look for any areas of ulceration, glandular mucosa (pink or tan, appears different from pale squamous mucosa) strictures and tumors and the narrowing of the lumen caused by these lesions
- Note the dimensions of any lesions and their location, with reference to the proximal / distal / deep margins, the squamocolumnar junction (Z line) and the gastroesophageal (GE) junction
- This should be measured on the fresh specimen due to retraction following fixation
- Z line is the intersection of squamous and glandular mucosa
- GE junction is the junction of the tubular esophagus and saccular stomach, irrespective of the types of mucosa present
- Proximal displacement of the Z line above the GE junction suggests Barrett esophagus
- Describe the external surface and note areas of retraction, induration, perforation by the tumor or any lymph nodes
- Photograph lesions (as appropriate)
- Ink the proximal, distal and deep (adventitial) margins underneath the tumor, pin the specimen on a board and fix in 10% formalin; if the tumor is large, make longitudinal cuts to aid in fixation
- Fix the specimen in formalin overnight
- Describe any lesions including:
- Size
- Color
- Configuration (e.g., exophytic, ulcerated, infiltrative)
- Depth of invasion: after fixation cut through the tumor or ulcer to assess the depth of invasion into the esophageal wall
- Location (including relationship to squamocolumnar junction) (see note)
- Note: tumors that have their epicenter at the gastroesophageal junction and extend no more than 2 cm into the proximal stomach are staged as esophageal, while tumors with an epicenter more than 2 cm into the proximal stomach are staged as primary gastric carcinoma even if the tumor involves the gastroesophageal junction
- Percent of circumference involved
- Luminal diameter at the lesional site
- Degree of proximal dilatation
- Describe uninvolved mucosa:
- Normal squamous esophagus: glistening smooth white mucosa
- Normal glandular stomach: velvety pink / red mucosa with rugal folds
- Barrett (glandular) mucosa: pale pink / salmon, finely granular, may be discontinuous
- Adventitial soft tissue / fat should be thoroughly searched and sectioned for lymph nodes
- Nodes may be very small and close to the esophageal or gastric outer surfaces
- Reference: Arch Pathol Lab Med 2015;139:1446
Procedure - endoscopic mucosal resections
- Indications:
- Barrett esophagus, with or without dysplasia or intramucosal carcinoma
- Lesions that are ≤ 2 cm, well to moderately differentiated and limited to the mucosa or superficial submucosa (Middle East J Dig Dis 2017;9:5, Gastroenterology 2015;149:1599, Endoscopy 2007;39:24)
- Procedure:
- Should arrive in the laboratory in a fresh state, with margins oriented by the endoscopist
- Specimen is usually round or oval
- Ink base and lateral mucosal margins with different colors
- Stretch the specimen gently and fix overnight in 10% formalin on a rigid board, with mucosal surface up
- After fixation the specimens should be serially sectioned at 2 - 3 mm intervals parallel to the long axis (not < 2 mm)
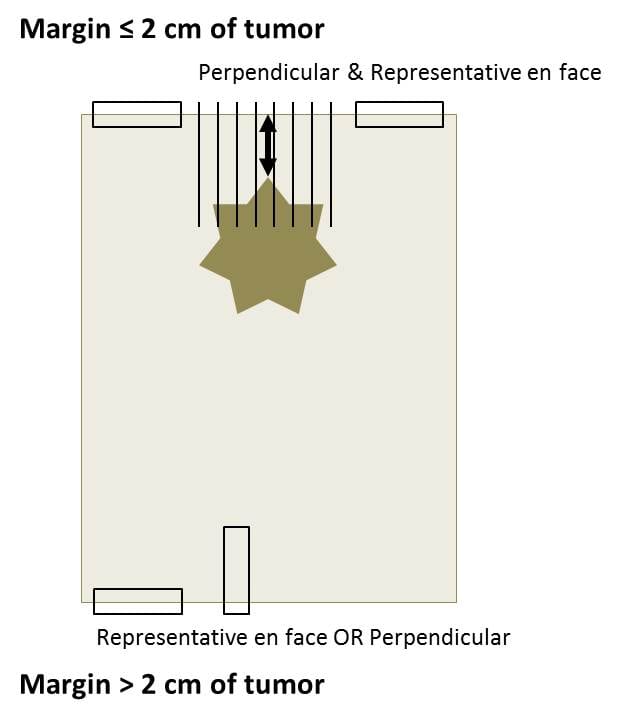
Sections to obtain
- Submit tumor: 1 section per centimeter, including maximal depth of invasion and relation to proximal / distal margins
- Longitudinal sections preferred
- If no gross tumor present (which is often the case after neoadjuvant therapy of the GE junction tumors), then the entire ulcerated / fibrotic area should be blocked off and submitted
- Margins: en face sections of proximal / distal margins unless tumor is < 2 cm from the margin then margin can be best demonstrated in perpendicular sections
- Esophagus and stomach: representative sections of uninvolved areas
- Other gross lesions (including Barrett esophagus): representative sections
- Lymph nodes: submit entirely
- For endoscopic mucosal resection (EMR): entire specimen should be submitted in a sequential manner (World J Gastrointest Endosc 2012;4:489)
Tips
- If no gross tumor present (which is often the case after neoadjuvant therapy of the GE junction tumors), then the entire ulcerated / fibrotic area should be blocked off and submitted
- Examine the specimen for Barrett mucosa, presenting as salmon / pink, granular mucosa (similar to gastric mucosa) above the GE junction, replacing the glistening white squamous mucosa
- Tumors that have their epicenter at the gastroesophageal junction and extend no more than 2 cm into the proximal stomach are staged as esophageal, while tumors with an epicenter more than 2 cm into the proximal stomach are staged as primary gastric carcinoma even if the tumor involves the gastroesophageal junction (Amin: AJCC Cancer Staging Manual, 8th Edition, 2017)
- 15 lymph nodes are recommended for esophageal or GE junction cancer; however, if not found submit entire adventitial tissue for lymph nodes (Ann Surg Oncol 2020;27:1227)
- For EMR, immediate pinning and fixing of the specimen helps preserve the size, shape and orientation of the lesion
Diagrams / tables
Images hosted on other servers:

Sections to obtain from esophagectomy specimen
How to obtain sections from margins
Frozen section
- Assessment of margins
- Assessment of depth of invasion and margin in an EMR (Clin Gastroenterol Hepatol 2006;4:173)
- Confirmation of pathology
- Volume of cancer cells for tumor banking (Methods Mol Biol 2020;2129:83)
Gross description
- Portions of esophagus are usually resected to remove neoplasms and less frequently strictures
- After checking the history, indication for the procedure and most recent endoscopic findings, proceed as below
Gross images
Images hosted on other servers:

Esophagectomy with proximal portion of stomach

Esophagectomy specimen status posttreatment

Esophageal endoscopic mucosal resection
Sample gross description report
- The specimen designated esophagus is received fresh in a container labeled with the patient's name and medical record number and consists of an esophagectomy and partial gastrectomy, including esophagus (20.0 cm length x 3.5 cm circumference) with attached proximal stomach (4.0 cm length x 10.0 cm circumference). There is a tan-pink, firm, fungating mass (2.5 x 2.0 cm), which invades through the muscularis propria into the adjacent soft tissue. The tumor is 15.0 cm from the proximal resection margin, 2.5 cm from the gastroesophageal junction, 6.5 cm from the distal resection margin and 0.2 cm from the deep resection margin (inked in black). The adjacent esophageal mucosa is tan-pink and finely granular from the gastroesophageal junction, up to within 10.0 cm of the proximal margin. The remainder of the mucosal surfaces are unremarkable. The attached soft tissue contains four palpable lymph nodes (range 0.3 - 0.5 cm). Gross photographs are taken. Section code:
- Cassette 1: proximal resection margin, en face
- Cassette 2: distal resection margin, en face
- Cassettes 3 - 4: tumor with deepest extent of invasion and deep margin, longitudinal
- Cassette 5: tumor with adjacent esophageal mucosa, longitudinal, representative
- Cassette 6: tumor with adjacent gastric mucosa, longitudinal
- Cassette 7: abnormal esophageal mucosa, representative
- Cassette 8: normal gastric mucosa, representative
- Cassettes 9 - 10: submit all lymph nodes, entirely
Gross differential diagnosis
- Normal esophageal mucosa white, smooth and glistening
- Adenocarcinoma:
- Close to the GE junction
- Grossly resemble colonic adenocarcinomas
- Tan / pink, polypoid, central ulceration
- May invade the submucosa and undermine proximal / distal normal appearing mucosa
- Barrett mucosa:
- Pale pink / salmon colored
- Finely granular
- Extends proximally from the GE junction
- May be discontinuous
- May be associated with adenocarcinoma
- Squamous cell carcinoma:
- Occurs in upper, middle and lower esophagus
- Exophytic (intraluminal), infiltrative / ulcerating or circumferential thickening
- Preoperative radiation therapy given in most cases
- Residual tumor difficult to detect and may be present as shallow ulceration, erosion, fibrosis or granular mucosa
- Leiomyoma:
- Typically arises from muscularis propria
- Well circumscribed tumor with white-pink, whorled cut surfaces
- Intramural or intraluminal / polypoid
Features to report - general
- Editorial note
- Lymphoma (consider the Hodgkin or non-Hodgkin protocol)
- Gastrointestinal stromal tumor (consider the GIST protocol)
- Non-GIST sarcomas (consider the soft tissue protocol)
- Others (report using separate TNM staging systems or CAP protocols)
Features to report - biopsies
- Specimen type (procedure)
- Site of biopsy (if known)
- Histologic type
- Histologic grade
- Microscopic tumor extension
- Additional findings
- Reference: Arch Pathol Lab Med 2015;139:1446
Features to report - endoscopic resection, esophagectomy or esophagogastrectomy
- Specimen:
- Esophagus
- Proximal stomach
- Other (specify)
- Not specified
- Procedure:
- Endoscopic resection
- Esophagectomy
- Esophagogastrectomy
- Other (specify)
- Not specified
- Tumor site:
- Cervical (proximal) esophagus
- Mid esophagus:
- Upper thoracic esophagus
- Mid thoracic esophagus
- Distal (lower thoracic) esophagus
- Esophagogastric junction (EGJ)
- Proximal stomach and EGJ
- Other (specify)
- Not specified
- Esophagus not otherwise specified
- Relationship of tumor to EGJ:
- Tumor is confined to the tubular esophagus and does not involve the EGJ
- Tumor midpoint is in the distal esophagus and tumor involves the EGJ
- Tumor midpoint is at the EGJ
- Tumor midpoint is in the proximal stomach or cardia and tumor involves the EGJ
- Not specified
- Cannot be assessed
- Distance of tumor center from EGJ (if applicable): __ cm
- Tumor size:
- Greatest dimension: __ cm
- Cannot be determined
- Histologic type:
- Squamous cell carcinoma
- Adenocarcinoma
- Adenosquamous carcinoma
- High grade neuroendocrine carcinoma:
- Large cell neuroendocrine carcinoma
- Small cell neuroendocrine carcinoma
- Adenoid cystic carcinoma
- Mucoepidermoid carcinoma
- Basaloid squamous cell carcinoma
- Spindle cell squamous cell carcinoma
- Verrucous squamous cell carcinoma
- Lymphoepithelioma-like carcinoma
- Mixed squamous cell carcinoma - neuroendocrine carcinoma
- Mixed adenocarcinoma - neuroendocrine carcinoma
- Mixed adenocarcinoma - neuroendocrine tumor
- Undifferentiated carcinoma
- Other (specify)
- Carcinoma, type cannot be determined
- Histologic grade:
- Not applicable
- GX: cannot be assessed
- G1: well differentiated
- G2: moderately differentiated
- G3: poorly differentiated
- G4: undifferentiated
- Microscopic tumor extension:
- Cannot be assessed
- No evidence of primary tumor
- High grade dysplasia (carcinoma in situ)
- Tumor invades lamina propria
- Tumor invades muscularis mucosae
- Tumor invades submucosal
- Tumor invades muscularis propria
- Tumor invades through muscularis propria into periesophageal soft tissue (adventitia)
- Tumor directly invades adjacent structures (specify)
- Margins (Middle East J Dig Dis 2017;9:5):
- If all margins uninvolved by invasive carcinoma, dysplasia and intestinal metaplasia
- Margins examined (proximal, distal, radial, mucosal, deep, others):
- Distance of invasive carcinoma from closest margin: __ cm
- Specify closest margin
- Proximal / distal margin involved by:
- Invasive carcinoma
- Dysplasia:
- Squamous dysplasia: low / high grade
- Intestinal metaplasia (Barrett esophagus) with dysplasia: low grade / high grade
- Intestinal metaplasia (Barrett esophagus) without dysplasia
- Circumferential (adventitial / deep) margin:
- Cannot be assessed
- Uninvolved by invasive carcinoma
- Involved by invasive carcinoma
- Other margins (specify):
- Cannot be assessed
- Uninvolved by invasive carcinoma
- Involved by invasive carcinoma
- For endoscopic resection specimens only:
- Mucosal margin:
- Cannot be assessed
- Involved by invasive carcinoma
- Uninvolved by invasive carcinoma
- Uninvolved by dysplasia
- Involved by:
- Squamous dysplasia: low / high grade
- Intestinal metaplasia (Barrett esophagus) with dysplasia: low grade / high grade
- Mucosal margin:
- Treatment effect (carcinomas treated with neoadjuvant therapy) (Dis Esophagus 2006;19:329):
- No prior treatment
- Present:
- No viable cancer cells (complete response, score 0)
- Single cells or rare small groups of cancer cells (near complete response, score 1)
- Residual cancer with evident tumor regression (partial response, score 2)
- No definite response / absent with extensive residual cancer with no evident tumor regression (poor / no response, score 3)
- Cannot be determined
- Treatment history not known
- Lymphovascular invasion:
- Not identified
- Present
- Indeterminate
- Perineural invasion:
- Not identified
- Present
- Indeterminant
- Regional lymph nodes:
- Lymph node examination required only if lymph nodes present in the specimen
- No nodes submitted or found
- Number of lymph nodes involved
- Number of lymph nodes examined
- Lymph node examination required only if lymph nodes present in the specimen
- Pathologic staging (pTNM):
- TNM descriptors:
- m (multiple primary tumors)
- r (recurrent)
- y (posttreatment)
- Primary tumor (pT)
- Regional lymph nodes (pN)
- Distant metastasis (pM)
- TNM descriptors:
- Additional pathologic findings:
- None
- Intestinal metaplasia (Barrett esophagus)
- Squamous or glandular dysplasia: low grade / high grade
- Esophagitis
- Gastritis
- Other (specify)
- Ancillary studies (specify):
- HER2 neu status: for HER2 reporting, CAP gastric HER2 template should be used
- Clinical history:
- Barrett esophagus
- Other (specify)
- Not known
- References: Edge: AJCC Cancer Staging Manual, 7th Edition, 2009, CAP: Cancer Protocol Templates [Accessed 21 June 2022], CAP: Protocol for the Examination of Specimens from Patients with Carcinoma of the Esophagus [Accessed 21 June 2022], Surg Oncol Clin N Am 2006;15:751
Features to report - optional
- Size of largest tumor involvement in metastatic lymph node (Ann Surg Oncol 2002;9:1010, Ann Thorac Surg 2007;83:1265)
- Extracapsular lymph node involvement (Am J Surg Pathol 2006;30:171)
- Other features (esophagitis, Barrett esophagus, dysplasia, specific types of infection)
Board review style question #1
For esophageal or gastroesophageal junction cancers, what is the number of lymph nodes recommended for pathological evaluation?
- At least 5
- At least 5 - 10
- Not less than 15
- No number is required but entire adventitia should be submitted
Board review style answer #1
C. The current evidence supports the goal of obtaining at least 15 lymph nodes for pathological evaluation in both primary esophagectomy and postinduction therapy cases. Earlier, no number was required for esophageal or gastroesophageal cancer. If no lymph node is found, the entire adventitia should submitted (Ann Surg Oncol 2020;27:1227).
Comment Here
Reference: Esophagus - Grossing & features to report
Comment Here
Reference: Esophagus - Grossing & features to report
