
Esophagus
Other tumors
Lymphoma


Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Lymphoma[TI] esophagus[TI]
- Lymphomas comprise a diverse group of clonal (malignant) lymphoproliferative disorders, classified by WHO based on lymphocytic origin (lymphoma)
- Hodgkin lymphomas arise from precursor B cells (Reed-Sternberg cells)
- Classic Hodgkin lymphoma - 95%
- Nodular lymphocyte predominant Hodgkin lymphoma (NLPHL) - 5%
- Non-Hodgkin lymphomas arise from monoclonal expansion of malignant B or T cells
- B cell lymphomas
- B cell acute lymphoblastic lymphoma (ALL)
- Chronic lymphocytic lymphoma / small lymphocytic leukemia (CLL / SLL)
- Mantle cell lymphoma
- Follicular lymphoma
- Marginal zone B cell lymphoma
- Extranodal MALT type
- Hairy cell leukemia
- Plasmacytoma / plasma cell myeloma
- Diffuse large B cell lymphoma (DLBCL)
- Burkitt lymphoma
- T / NK cell lymphomas
- T cell acute lymphoblastic lymphoma (ALL)
- T cell CLL
- Mycosis fungoides / Sézary syndrome
- Peripheral T cell lymphoma
- Angioimmunoblastic T cell lymphoma
- Enteropathy associated intestinal T cell lymphoma
- Hepatosplenic T cell lymphoma
- Anaplastic large cell lymphoma (ALCL)
- Extranodal NK / T cell lymphoma, nasal type
- B cell lymphomas
- Hodgkin lymphomas arise from precursor B cells (Reed-Sternberg cells)
- Primary esophageal lymphoma
- Arises de novo in esophageal mucosa associated lymphoid tissue (MALT)
- Secondary esophageal lymphoma
- Spreads to esophagus by either direct extension or metastasis
- GI tract is most common site of extranodal non-Hodgkin lymphoma (4 - 20%)
- Esophagus is least common site of GI involvement
- < 0.2% of all extranodal non-Hodgkin lymphoma
- Esophagus is least common site of GI involvement
- Lymphomas comprise < 1% of all esophageal cancers
- Secondary lymphoma (contiguous spread from mediastinal or cervical lymph nodes) >> primary esophageal disease
- Most originate from mature B cells
- Non-Hodgkin lymphoma >> Hodgkin lymphoma
- Mostly DLBCL and extranodal marginal zone B cell lymphoma, MALT type
- Males > females
- Wide age range: 17 - 86 years but usually middle age to older adults
- Younger age of onset in HIV+ patients (40 vs. 60 years)
- Primary lymphoma:
- Arises in submucosal lymphoid patches
- Secondary lymphoma
- Proximal esophageal involvement may result from adjacent cervical lymphadenopathy
- Middle esophageal involvement may be due to mediastinal lymphadenopathy
- Distal esophageal involvement often secondary to gastric disease
- Chronic immune suppression or dysregulation
- HIV infection
- Chronic hepatitis C infection
- Features of primary lymphoma (Dawson criteria):
- No palpable superficial lymphadenopathy
- Normal chest radiograph with no evidence of lymphadenopathy
- Normal peripheral white blood cell count
- Primary esophageal lesion with only regional adenopathy
- No liver or spleen involvement
- Insidious onset
- Dysphagia (most common)
- Odynophagia
- Chest / abdominal pain
- Weight loss
- Complications (Ann Otol Rhinol Laryngol 1994;103:843)
- Hemorrhage
- Vocal cord paralysis / hoarseness
- Stricture / obstruction
- Perforation with esophagomediastinal or esophagotracheobronchial fistula or mediastinitis
- Vocal cord paralysis
- Relatively poor prognosis
- Biopsy with ancillary studies (immunohistochemistry, flow cytometry) to confirm histologic type
- Complete blood count may show:
- Leukocytosis ± blasts (leukemic spread)
- Pancytopenia (bone marrow infiltration)
- Nonspecific radiographic features
- Local extension of gastric lymphoma may cause distal esophageal stricture
- Barium swallow / CT: stricture, polypoid or intramural mass
- PET useful for staging
Images hosted on other servers:
Strictures:

Marked 3 cm narrowing

Irregular outline and multiple filling defects

Luminal narrowing
Esophageal thickening ± mass lesions:
4 x 4 cm esophageal mass

Thickening of the esophageal wall

Thickening the aortic arch to the gastrointestinal junction
Endoscopic ultrasound:

Transmural thickening of the esophageal wall

Hypoechoic thickening
Primary esophageal Hodgkin lymphoma:

Submucosal nodules

Circumferential thickening

Aneurysmal dilatation

Nodular thickening of esophageal wall

Fistula to lobectomy
- Stage at diagnosis
- Feasibility of surgery or chemotherapy
- Successful management depends on accurate diagnosis and appropriate subsequent treatment
- Histologic type: MALT lymphoma and Hodgkin lymphoma have better prognoses than DLBCL or T cell lymphomas
- HIV / AIDS associated with worse outcomes
- Median survival: 4 - 6 months
- 3 year old boy with anaplastic large cell lymphoma of esophagus (Pediatr Radiol 2012;42:627)
- 53 year old man with multiple lymphomatous polyposis with widespread involvement of GI tract (Arch Pathol Lab Med 2003;127:1028)
- 53 year old man with primary MALT lymphyoma of esophagus, manifesting as a submucosal tumor (Korean J Gastroenterol 2013;62:117)
- 56 year old man with primary esophageal lymphoma (Ann Thorac Surg 1998;66:1418)
- 58 year old man with primary extramedullary plasmacytoma of esophagus (Ann Diagn Pathol 2003;7:174)
- 59 year old man with MALT lymphoma of esophagus (Int J Clin Oncol 2012;17:174)
- 60 year old woman with dysphagia (Endoscopy 2012;44:E167)
- 61 year old men with Hodgkin lymphoma of esophagus (Am J Clin Pathol 1997;108:593, AJR Am J Roentgenol 2003;180:1335)
- 62 year old woman with MALT lymphoma arising in esophagus, stomach and lung (Gen Thorac Cardiovasc Surg 2011;59:826)
- 63 year old man with T cell lymphoma presenting as esophageal obstruction and bronchoesophageal fistula (Med Sci Monit 2011;17:CS66)
- 65 year old man with MALT lymphoma of esophagus coexistent with bronchus associated lymphoid tissue lymphoma of lung (Yonsei Med J 2005;46:562)
- 67 year old man with multiple polyposis of esophagus (Clin Gastroenterol Hepatol 2012;10:e65)
- 70 year old man with esophageal MALT lymphoma (Dis Esophagus 2013;26:349)
- 70 year old man with CD8+ mycosis fungoides with esophageal involvement (Oncol Lett 2013;5:73)
- 77 year old man with primary isolated non-Hodgkin lymphoma of esophagus (World J Gastroenterol 2009;15:1901)
- 80 year old woman with esophageal perforation and MALT lymphoma (University of Pittsburgh: Esophageal Perforation with an Unusual Etiology [Accessed 31 January 2018])
- 6 cases of primary esophageal lymphoma (Dig Dis Sci 2006;51:77)
- Indolent T cell lymphoproliferative disease of GI tract (Blood 2013;122:3599)
- Esophageal leukemic infiltration in children (J Pediatr Gastroenterol Nutr 2011;52:781)
- Two immunocompetent patients with primary esophageal lymphoma (World J Radiol 2010;2:334)
- Primary esophageal lymphoma: local and systemic therapy
- Radiotherapy, chemotherapy
- Non-Hodgkin lymphoma: CHOP (cyclophosphamide, vincristine, prednisone, doxorubicin), rituximab (anti-CD20 monoclonal antibody)
- Hodgkin lymphoma: ABVD (doxorubicin, bleomycin, vinblastine, dacarbazine) or Stanford V (doxorubicin, vinblastine, mechlorethamine, vincristine, bleomycin, etoposide, prednisone)
- Surgical resection: diagnostic, curative or palliative
- Endoscopic resection for early lesions (Dig Endosc 2014;26:478)
- Radiotherapy, chemotherapy
- Secondary esophageal lymphoma: chemotherapy
Images hosted on other servers:
Endoscopy:

Multiple solid, firm nodular lesions

Ulcerated tumor

Large, rounded mass

Solid, firm nodular lesions

Multiple lymphomatous polyposis
- Submucosal mass with variable ulceration or exophytic growth
Images hosted on other servers:

Ulcerated burgeoning masses

MALT: esophagus /
proximal stomach
are unremarkable
- DLBCL: large centrocytes, centroblasts, immunoblasts and anaplastic large B cells
- Surface Ig+, CD20+, BCL6±, CD10±, CD43±, PAX5+
- Marginal zone B cell lymphoma, MALT type: small lymphocytes, marginal zone B cells, plasma cells, reactive follicles, lymphoepithelial lesions
- Surface and cytoplasmic Ig+ (IgM > IgG or IgA), CD20+, CD5-, CD10-, BCL6-, BCL2+, CD43±, cyclin D1-
- Mantle cell lymphoma: small to medium sized, slightly irregular cells with scant cytoplasm
- Surface IgMD+, CD20+, CD5+, CD10-, CD43+, cyclin D1+
- Burkitt lymphoma: medium sized atypical lymphoid cells with round nuclei, basophilic cytoplasm and tingible body macrophages (starry sky appearance)
- Cytoplasmic lipid droplets are Oil red O+
- Surface IgM+, CD20+, CD10+, BCL6+, BCL2-, Ki67 ~100%
- Follicular lymphoma: mixtures of centrocytes and centroblasts, follicular dendritic cells
- Surface Ig+, CD20+, CD10+, BCL6+, BCL2+, CD5-, CD43-, cyclin D1-
- Classic Hodgkin lymphoma: Reed-Sternberg cells and variants in a reactive background
- R-S cells: CD30+, CD15±, PAX5+, ALK-, CD45-, CD3-
- Nodular lymphocyte predominant Hodgkin lymphoma: vague nodules of small B cells and interspersed large tumor cells (LP cells) with thin nuclear membranes, fine chromatin and variable nucleoli
- LP cells: CD45+, CD20+, CD15-, CD30-
Images hosted on other servers:

Diffuse large B cell lymphoma
Mantle cell lymphoma

Mantle cell lymphoma



Mycosis fungoides
MALT lymphoma:
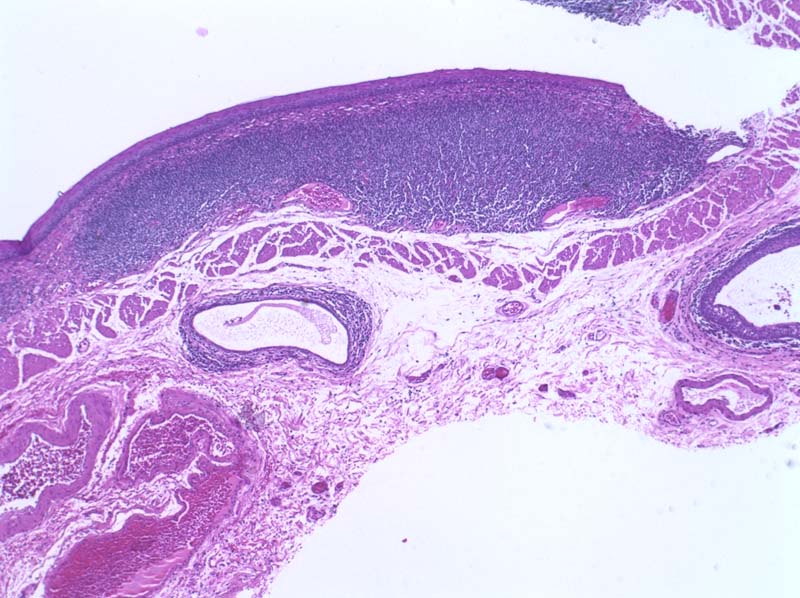

Dense submucosal lymphocytic infiltrate
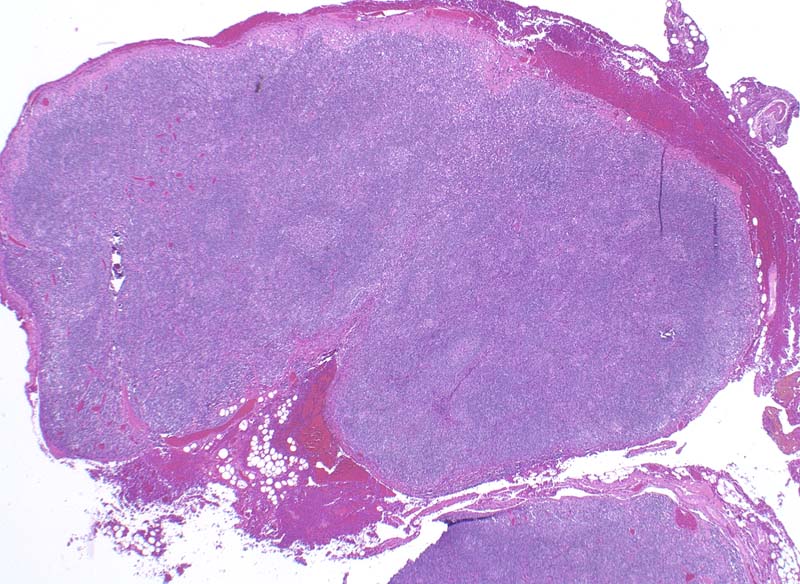
Vaguely nodular growth pattern
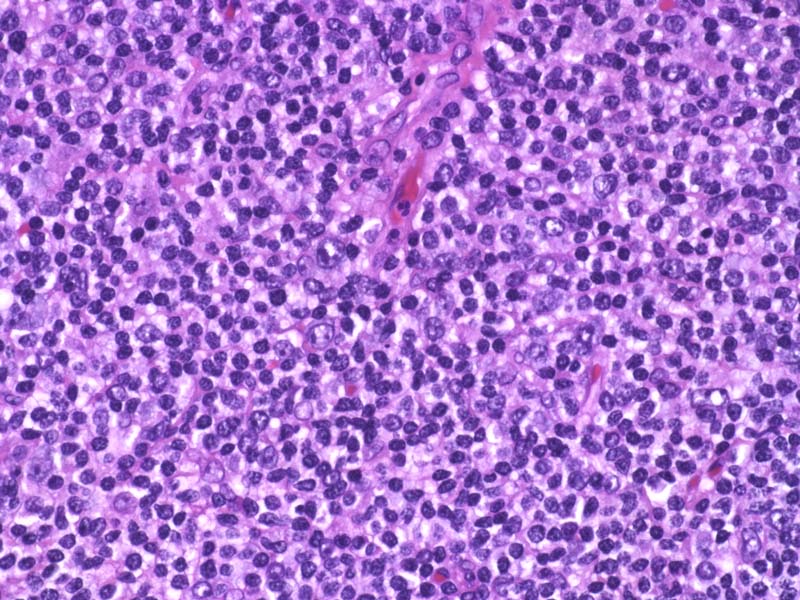
Monocytoid appearance

Germinal centers
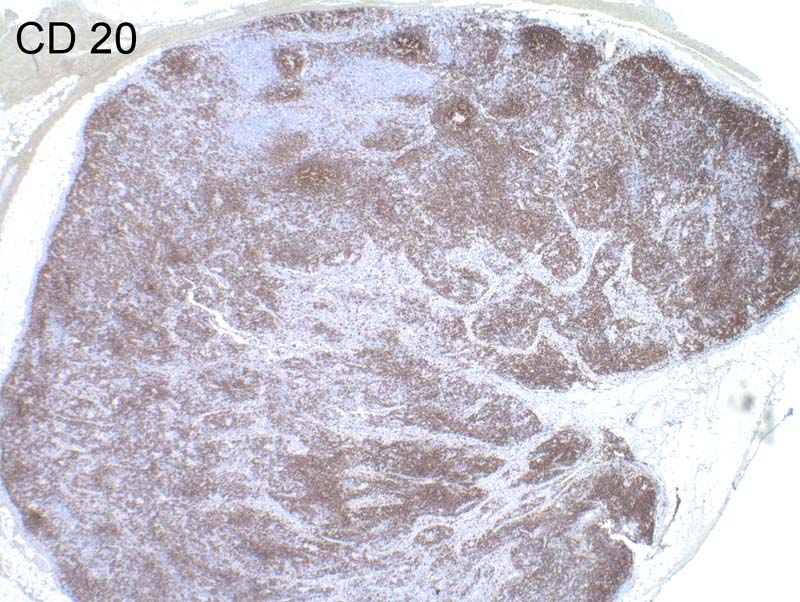
CD20+
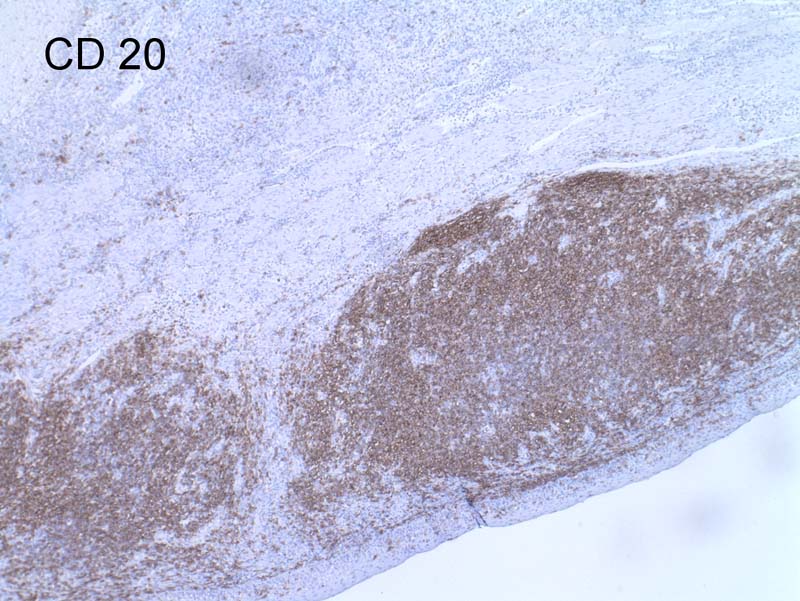
CD20+
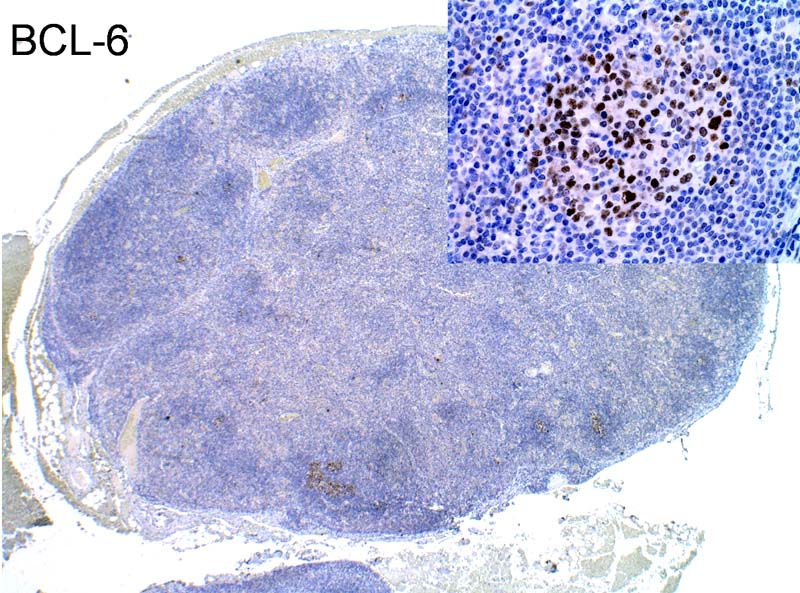
BCL6+ in germinal centers
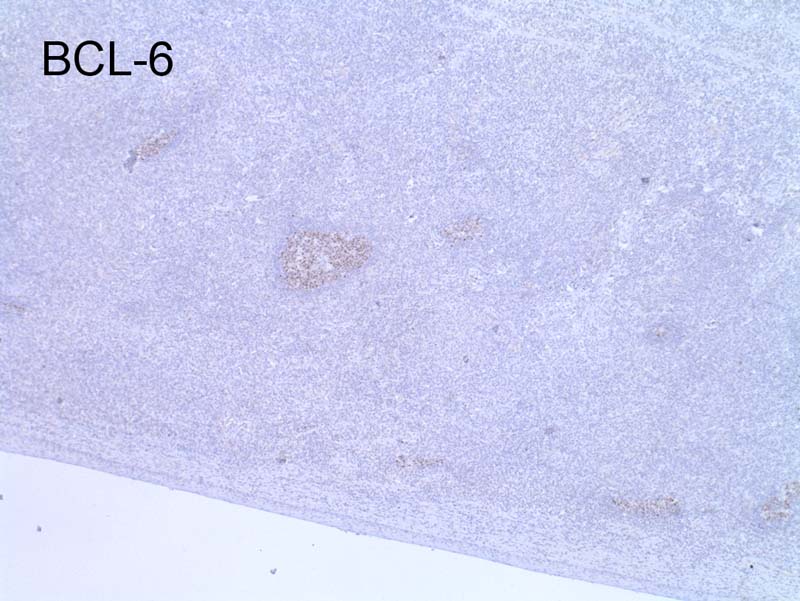
BCL6+
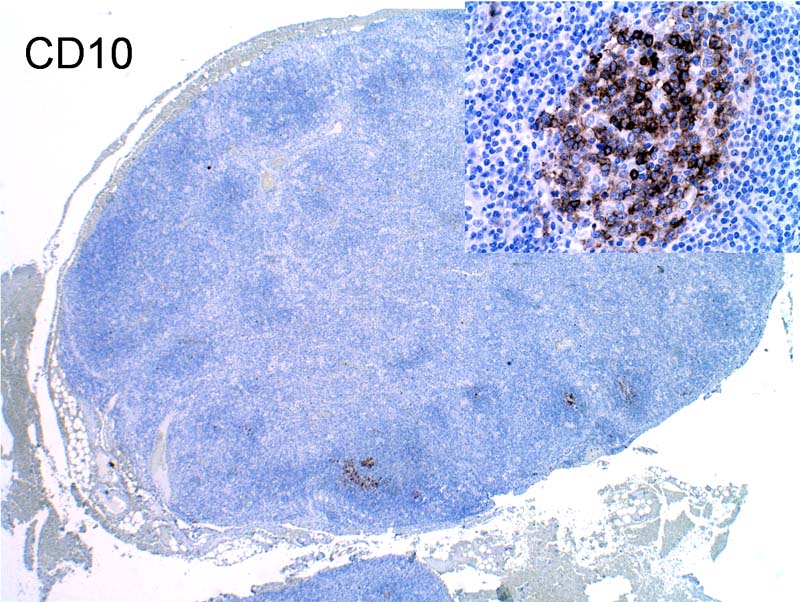
CD10

Ki67
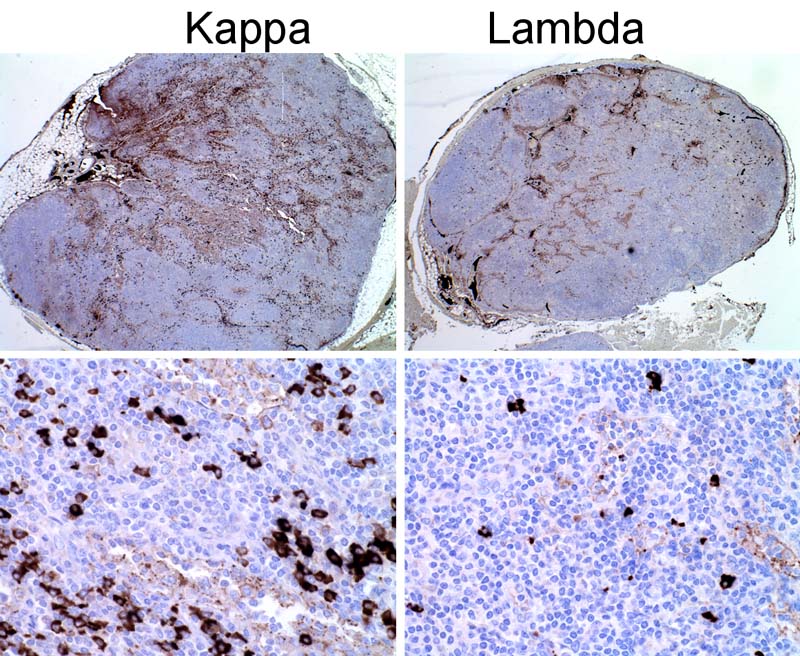
Kappa / lambda
- Discohesive, single abnormal lymphoid cells
Images hosted on other servers:

DLBCL

Burkitt lymphoma

MALT lymphoma
- Peripheral blasts if leukemic spread
- CD45 (leucocyte common antigen): most hematopoietic neoplasms
- Notable exceptions: ALCL, classic Hodgkin lymphoma, plasma cell myeloma
- CD2, CD3, CD4: most T cell neoplasms
- CD5: CLL / SLL, mantle cell lymphoma
- CD10: follicular lymphoma, Burkitt lymphoma, some DLBCL
- CD19, CD20, CD79a: most B cell neoplasms
- CD23: SLL / CLL
- CD30: ALCL, classic Hodgkin lymphoma
- Cyclin D1: mantle cell lymphoma
- EBV: classic Hodgkin lymphoma
- EMA: ALCL, plasmacytoma, LP cells in NLPHL, some T cell lymphomas
- MUM1: classic Hodgkin lymphoma, plasmablastic lymphoma
- PAX5: B cell marker, classic Hodgkin lymphoma
- Most cytokeratins
- Melanocytic markers (S100, HMB45, MelanA, MITF)
- Smooth muscle markers (desmin, caldesmon, smooth muscle actin)
- Neuroendocrine markers (chromogranin, synaptophysin, NSE)
- Useful to determine surface and cytoplasmic CD markers
- Common genetic features of mature B cell lymphomas
- Marginal zone B cell lymphoma, MALT type
- IGH clonally rearranged
- t(11;18)
- DLBCL
- IGH clonally rearranged
- t(8;14) c-myc-IGH
- t(14;18) IGH-BCL2
- Burkitt lymphoma
- IGH clonally rearranged
- t(8;14)
- t(2;8)
- t(8;22)
- Mantle cell lymphoma
- IGH clonally rearranged
- t(11;14) BCL1-IGH
- Marginal zone B cell lymphoma, MALT type
- Reactive lymphoid hyperplasia: polyclonal by IHC / flow cytometry
