

Heart & vascular pathology
Benign tumors / other nonneoplastic
Papillary fibroelastoma
Authors: Ryan Kendziora, M.D., Melanie C. Bois, M.D.
Resident / Fellow Advisory Board: David B. Chapel, M.D.
Editorial Board Member: Carolyn Glass, M.D., Ph.D.
Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 10 May 2021
Last staff update: 10 May 2021
Copyright: 2007-2024, PathologyOutlines.com, Inc.
PubMed Search: Papillary fibroelastoma [title] review [ptyp]
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Clinical images | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Positive stains | Negative stains | Molecular / cytogenetics description | Videos | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Kendziora R, Bois MC. Papillary fibroelastoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/hearttumorfibroelastoma.html. Accessed April 23rd, 2024.
Definition / general
- Papillary fibroelastoma is a benign papillary growth of endocardium and avascular fibroelastic tissue
- Usually benign and discovered incidentally but can embolize to distal sites
Essential features
- Papillary fibroelastoma is the most common cardiac tumor
- Benign behavior but may result in morbidity / mortality from downstream (thrombo) embolization
- Associated with KRAS mutations in up to 80% of lesions
Terminology
- Fibroelastic papilloma (not recommended)
- Cardiac papilloma (not recommended)
- Giant Lambl excrescence (not recommended)
ICD coding
Epidemiology
- Most common cardiac tumor (J Am Coll Cardiol 2018;72:202)
- Typical patient:
- 60 - 70 years but has been seen in all ages
- M = F
- Risk factors:
- Damaged endothelium (prior radiation therapy, cardiac surgery, structural heart disease resulting in hemodynamic alterations) (Hum Pathol 2002;33:1165, J Am Soc Echocardiogr 2010;23:595)
Sites
- May arise on any endocardial lined surface (e.g. valves, chamber walls)
Etiology
- Debated: reactive versus neoplastic
- Associated with injured endocardium, both iatrogenic and intrinsic, suggesting a reactive phenomenon (Hum Pathol 2002;33:1165, J Am Soc Echocardiogr 2010;23:595)
- KRAS mutations documented in 33 - 80% of lesions, implying a neoplastic origin (J Pathol Clin Res 2017;3:100, Am J Surg Pathol 2020;44:626)
Clinical features
- Considerable variation to clinical presentation
- Most commonly asymptomatic and diagnosed incidentally on routine imaging or at the time of cardiac surgery for an alternate indication
- May present with syncope, myocardial infarction or sudden death
- Stroke / ischemia occurs in 33% diagnosed on imaging (J Am Coll Cardiol 2015;65:2420)
- Embolism thought to be secondary to tumor fragmentation or from thrombi formed on the surface of the lesion
- Higher incidence in individuals with prior cardiac surgery, thoracic radiation or underlying structural heart disease / cardiomyopathy
Diagnosis
- Imaging is the most classic means of diagnosis
- Echocardiography is common due to ubiquitous nature of the modality
- CT also useful as it provides high spatial resolution
Radiology description
- Characteristic appearance on imaging (J Am Coll Cardiol 2018;72:202)
- All modalities:
- Mobile, frond-like lesion on stalk
- Special considerations:
- Echocardiogram: speckled appearance with stippling at tumor edge
- Magnetic resonance: may show some T2 hyperintensity but enhancement is uncommon
Radiology images
Images hosted on other servers:

Echocardiography

Echocardiography and MRI
Prognostic factors
- Excellent prognosis with surgical removal
- 5 year survival significantly worse without resection (J Am Coll Cardiol 2015;65:2420)
Case reports
- 55 year old man with exertional dyspnea and palpitations (Cardiol Res 2019;10:378)
- 58 year old woman with multiple systemic infarcts (Cureus 2019;11:e4798)
- 71 year old woman with stroke (Proc (Bayl Univ Med Cent) 2019;32:247)
Treatment
- Surgical resection is recommended
- Anticoagulation may be considered in patients who are not surgical candidates (Am Heart J 2003;146:404)
Clinical images
Images hosted on other servers:

Tricuspid valve
Gross description
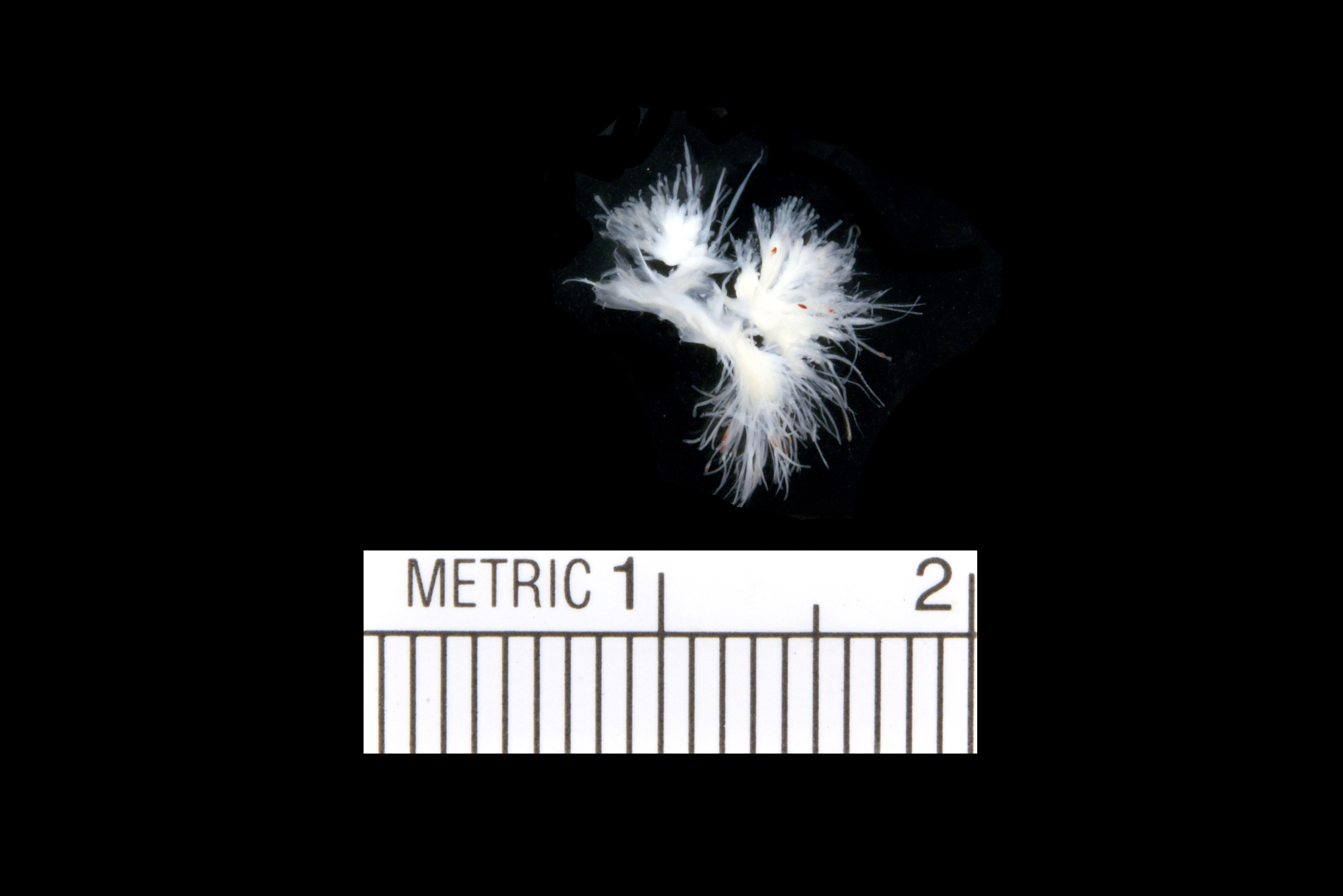
- Arborizing, thin strands of tan-white tissue, usually arising from a common stalk
- Likened to a sea anemone
- Fronds may not be apparent unless tumor is placed in an aqueous medium
Gross images
Contributed by Melanie C. Bois, M.D.
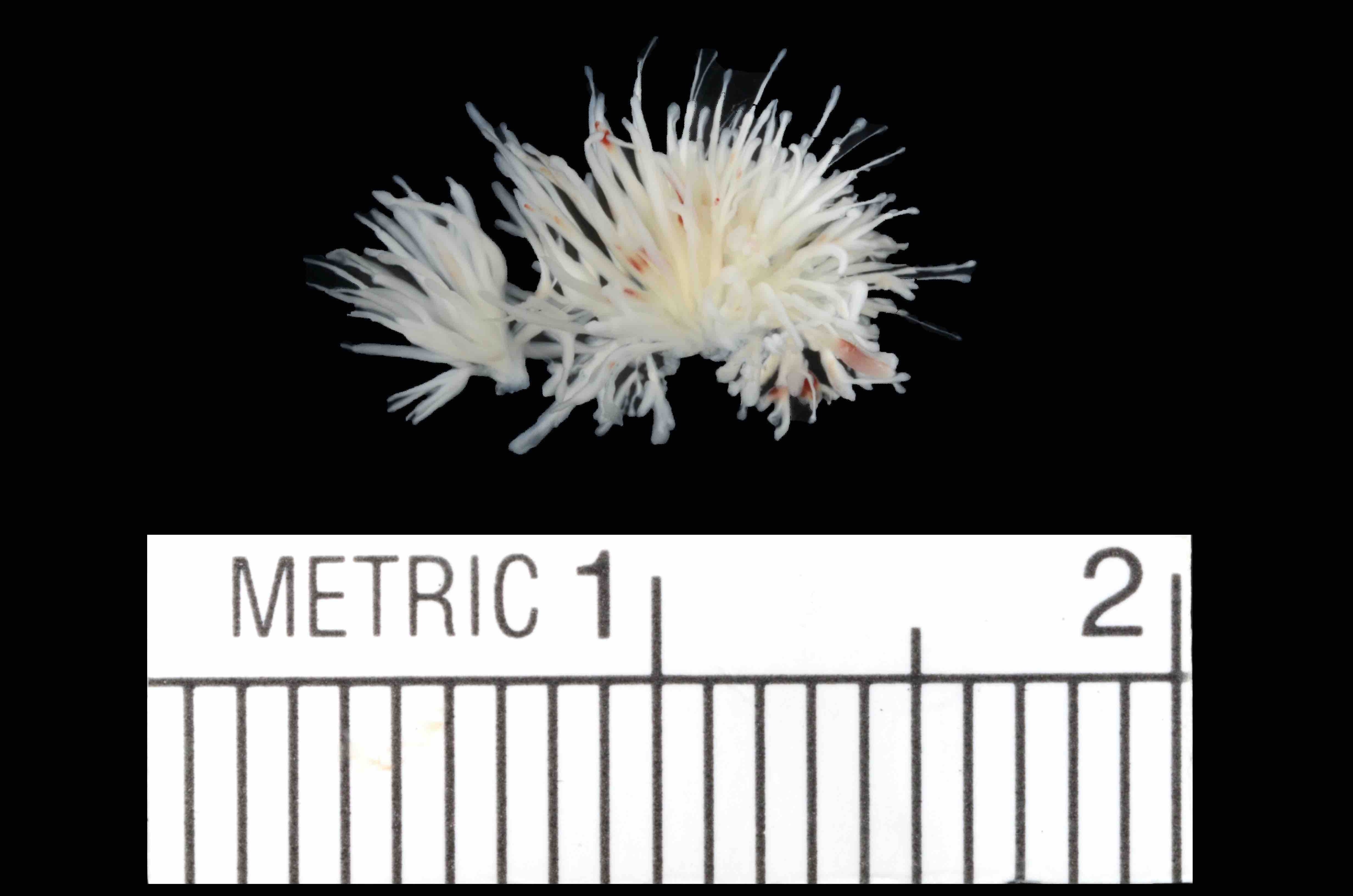
Surgical excision

In nonaqueous medium
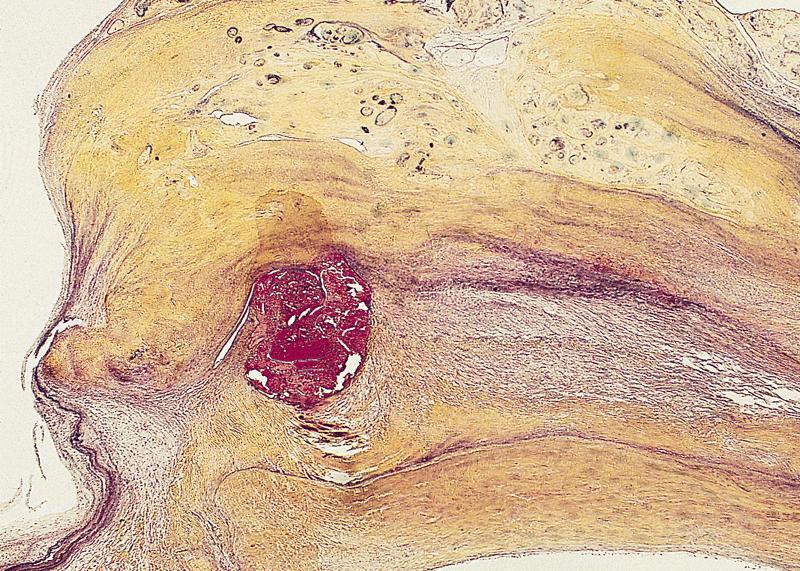
AFIP images

Tumor in noncoronary sinus
Images hosted on other servers:

Multiple small fronds resembling a sea anemone

death due to
occlusion of right
coronary ostium
Microscopic (histologic) description
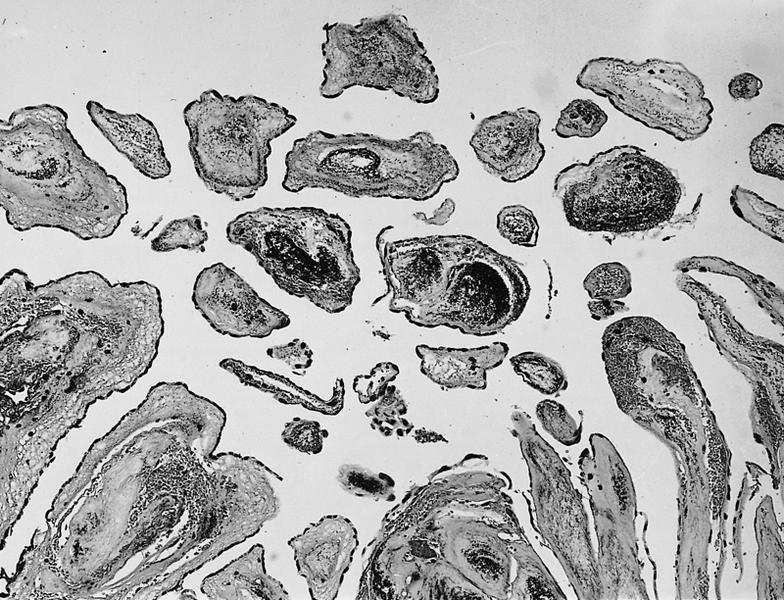
- Multiple, branching fronds of paucicellular, avascular fibroelastic tissue lined by a single layer of endocardium
- Has multiple branching fronds by definition
- Differential diagnosis: Lambl excrescences are microscopically identical but are simple, nonbranching projections of fibroelastic tissue
- May show hydropic change
- Histologic characteristics do not appear to correlate with KRAS mutation status
Microscopic (histologic) images
Contributed by Melanie C. Bois, M.D.
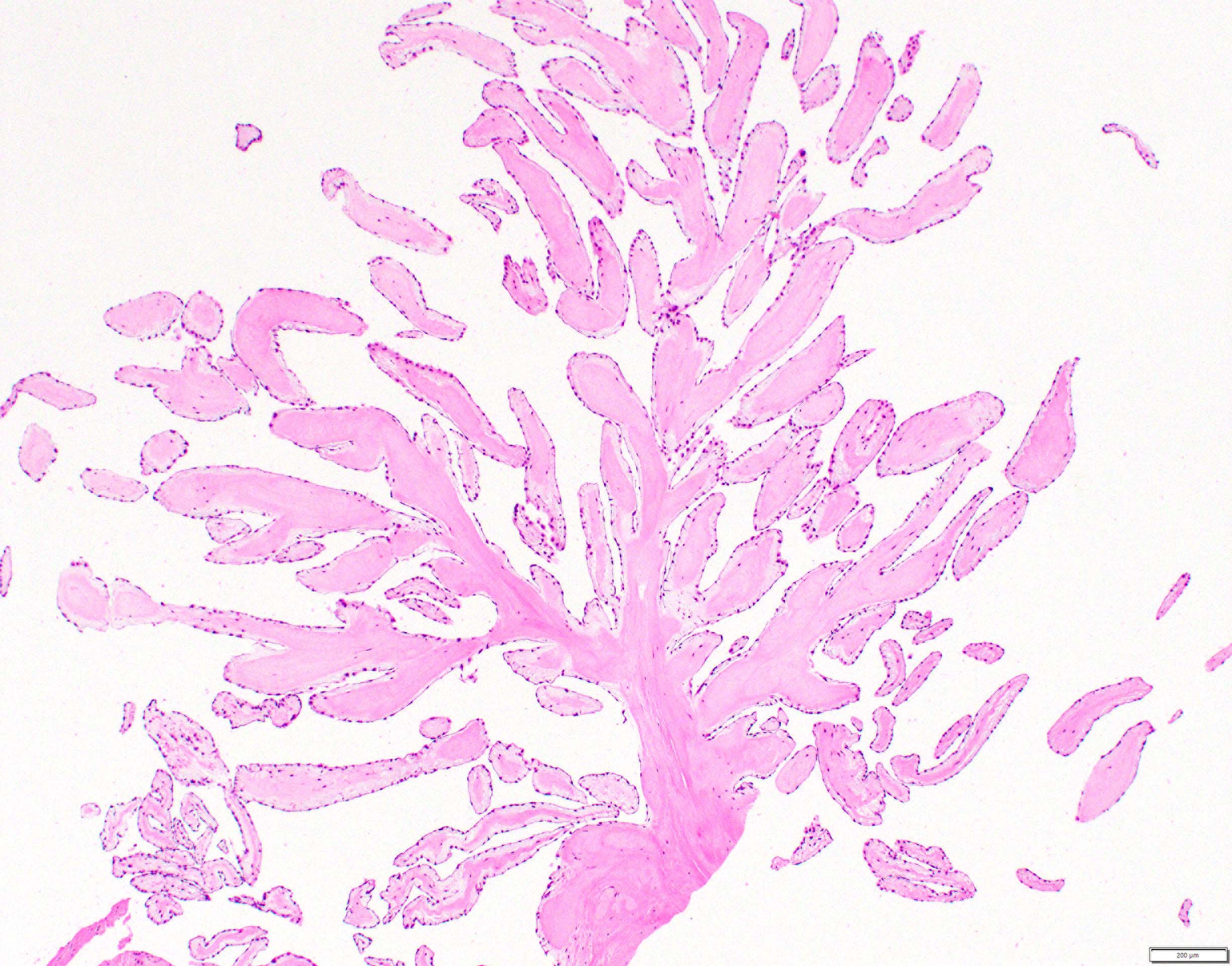
Arborizing fronds
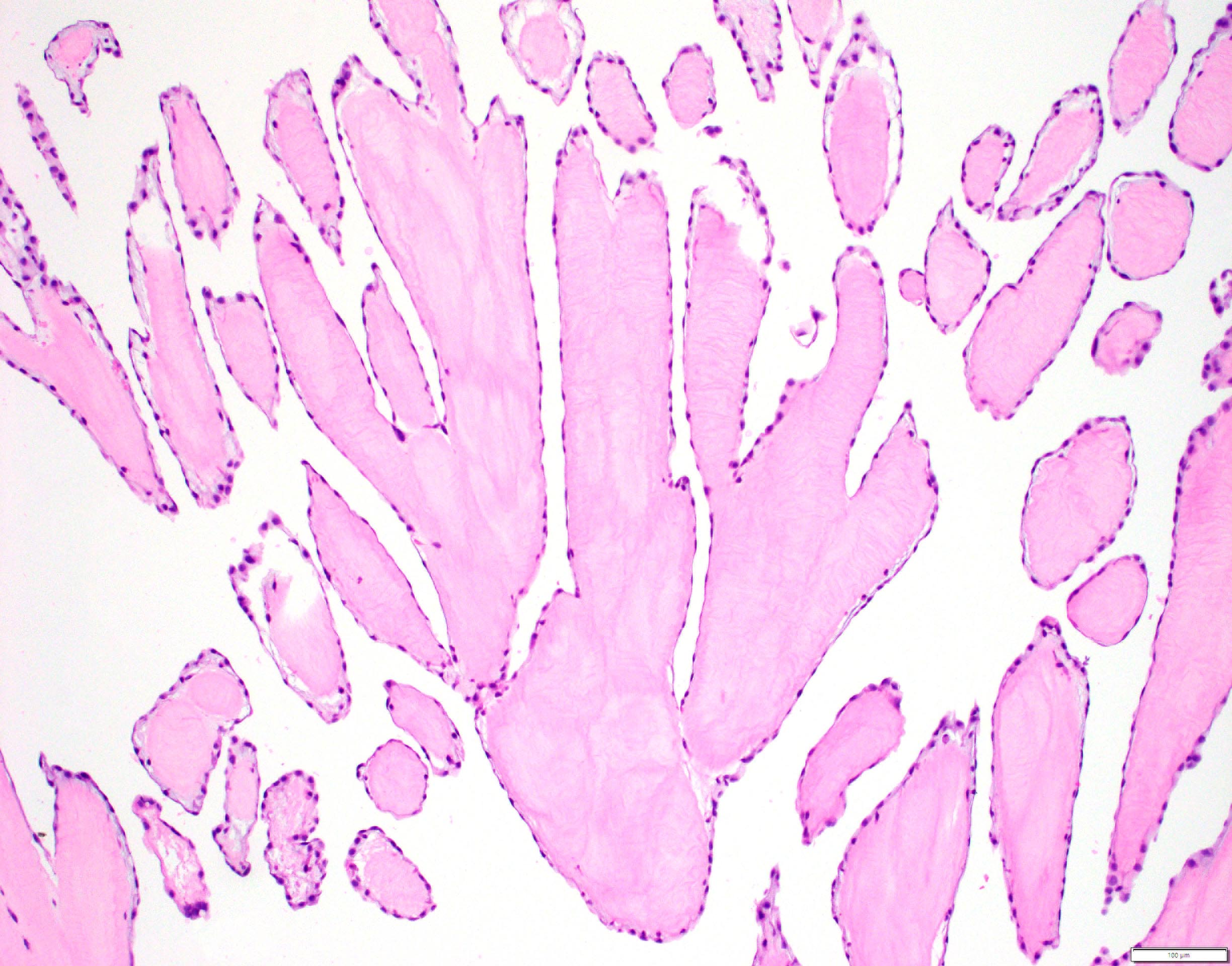
Avascular cores
AFIP images

Arising from aortic valve cusp
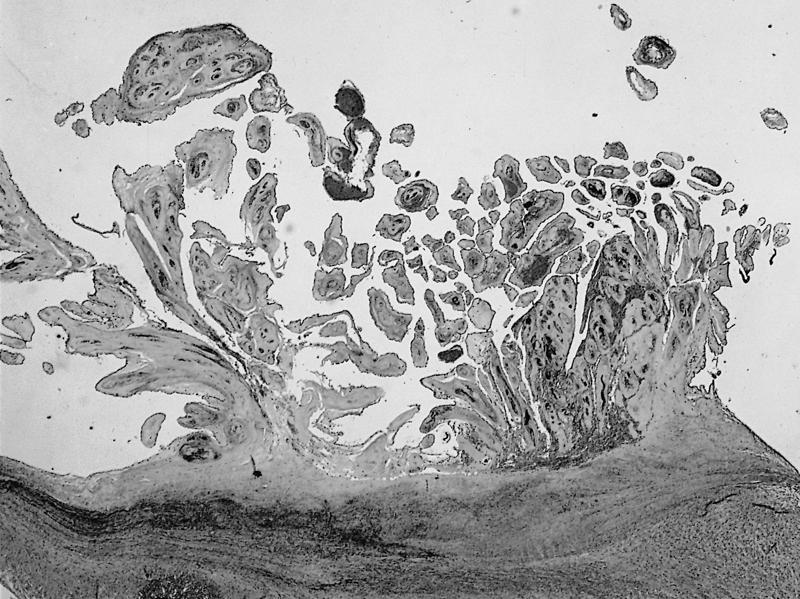
Movat pentachrome stain
Avascular tumor fronds growing into a cardiac chamber
Architecture obscured by scarring
Virtual slides
Images hosted on other servers:

Papillary fibroelastoma
Positive stains
- Elastic fibers: Verhoeff van Gieson (VVG) or other elastic stain highlights elastic core of fronds
Negative stains
Molecular / cytogenetics description
- KRAS mutations identified in up to 80% (J Pathol Clin Res 2017;3:100, Am J Surg Pathol 2020;44:626)
Videos
Resection of large aortic valve papillary fibroelastoma
Sample pathology report
- Heart, aortic valve, excision:
- Papillary fibroelastoma (evaluated with elastic stain)
Differential diagnosis
- Lambl excrescence:
- Similar histology but lacks complex architecture and anastomosing fronds
- Only occurs on the closing edge of valves
- Cardiac myxoma:
- May show similar gross features (particularly when papillary fibroelastoma is collapsed)
- Contains lepidic or myxoma cells that are calretinin positive
- Valvular vegetation:
- May show similar gross features
- Infectious vegetation shows mixed inflammation with or without microorganisms
- Nonbacterial thrombotic endocarditis is a sterile vegetation consisting predominantly of fibrin and blood products
Additional references
Board review style question #1
This tumor was surgically excised from the aortic valve of a 58 year old man. This patient was most likely to have prior exposure to which of the following?
- Cisplatin
- Inferior vena cava (IVC) filter
- Smoking
- Thoracic irradiation
- Vancomycin
Board review style answer #1
D. Thoracic irradiation. Endocardial injury is associated with the development of papillary fibroelastomas. Damage may be from iatrogenic causes (e.g. thoracic irradiation, prior cardiac surgery) or from hemodynamic changes secondary to intrinsic structural heart disease. Chemotherapies and antibiotics have not been associated with papillary fibroelastoma development. IVC filters do not contact the heart.
Comment Here
Reference: Papillary fibroelastoma
Comment Here
Reference: Papillary fibroelastoma
Board review style question #2
A 63 year old woman experienced multiple transient ischemic attacks and was subsequently found to have a large, mobile cardiac mass attached to her aortic valve by a stalk on echocardiography. Why would her cardiologist recommend surgical excision?
- Definitive diagnosis and triage to chemotherapeutic regimen
- Genetic testing for identification of at risk family members
- Potential for malignant transformation
- Risk of thrombus formation with subsequent thromboembolization
Board review style answer #2
D. Risk of thrombus formation with subsequent thromboembolization. Papillary fibroelastomas undergo surgical excision because of their (thrombo) embolic potential. The most common mechanism is thought to be related to thrombus formation with subsequent embolization; however, portions of the tumor may fragment and result in downstream ischemia. They have not been documented to show malignant transformation and surgical resection is considered curative without need for subsequent chemotherapy. They are not thought to be hereditary in origin.
Comment Here
Reference: Papillary fibroelastoma
Comment Here
Reference: Papillary fibroelastoma
