

Kidney nontumor / medical renal
Infection
HIV associated renal disease
Editorial Board Members: Jonathan E. Zuckerman, M.D., Ph.D., Nicole K. Andeen, M.D.


Last author update: 22 May 2023
Last staff update: 22 May 2023
Copyright: 2021-2024, PathologyOutlines.com, Inc.
PubMed Search: HIV associated renal disease
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Diagrams / tables | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Immunofluorescence description | Immunofluorescence images | Positive stains | Negative stains | Electron microscopy description | Electron microscopy images | Genetics | Sample pathology report | Differential diagnosis | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Cazzaniga G, L'Imperio V. HIV associated renal disease. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/kidneyHIVassociatedrenaldisease.html. Accessed April 25th, 2024.
Definition / general
- HIV associated renal disease refers to the group of kidney conditions that develop in patients with HIV infection
- The term includes cases with HIV associated nephropathy (HIVAN), HIV associated immune complex kidney disease (HIVICK) and kidney injury resulting from prolonged exposure to antiretroviral therapy or from opportunistic infections (Kidney Int 2018;93:545)
- Lack of certainty of HIV causality in presentation other than HIVAN
Essential features
- HIVAN: nephrotic range proteinuria with collapsing glomerulopathy (less frequently focal segmental glomerulosclerosis [NOS], minimal change disease, thrombotic microangiopathy), eventually associated with microcystic tubular dilatation and active tubulointerstitial nephritis (Am J Kidney Dis 2016;68:e13)
- HIVICK: lupus-like lesions in HIV infected patients without serologic evidence of lupus; other immune complex diseases (e.g., IgA nephropathy and postinfectious glomerulonephritis) should be better diagnosed as those specific entities (Am J Kidney Dis 2016;68:e9)
Terminology
- HIV associated nephropathy (HIVAN)
- HIV associated immune complex kidney disease (HIVICK)
ICD coding
Epidemiology
- Average age at presentation: 41 years (Expert Rev Anti Infect Ther 2008;6:365)
- Marked reduction with antiretroviral therapies (peak incidence of 4 - 10% of end stage renal disease in U.S., now 0.97% with 800 - 900 cases) (Drugs 2008;68:963, J Nephrol 2001;14:377)
- Strongest association with African American ethnicity compared to other causes of renal failure except sickle cell anemia (J Nephrol 2001;14:377)
- HIVAN accounted for 76% in 1987 and only 14% in 2018 of biopsy diagnoses in HIV infected patients, largely due to highly active antiretroviral therapy (HAART) (Kidney Int 2020;97:1006)
- Non-HIV related immune complex glomerulonephritis (17%) and diabetic nephropathy (16%) most frequent diagnosis in HIV patients (Kidney Int 2020;97:1006)
Sites
- Glomeruli are most often involved in the form of podocytopathy, less frequently with immune complex disease; tubulointerstitial compartment can show microcystic tubular dilatation and active tubulointerstitial nephritis
Pathophysiology
- Infectious agent (HIV)
- Direct HIV1 infection of renal tubular epithelial cells (RTEc), podocytes and parietal epithelial cells (J Am Soc Nephrol 2017;28:719)
- Use of other receptors than the canonical CD4 receptor mediated entry mechanism (J Am Soc Nephrol 2017;28:719)
- Viral replication is not necessary for the HIVAN phenotype (Front Med (Lausanne) 2018;5:177)
- Stimulation of cytokines, including interferon γ (IFNγ)
- Cell cycle dysregulation and aberrant podocyte cell cycle reentry are involved in glomerular injury
- Increase of profibrotic factors and cytokine expression are involved in tubular microcyst and interstitial fibrosis
- Genetic factors
- Mechanism of APOL1 mediated kidney disease is currently unknown but HIV infection seems to act as a second hit for disease expression (J Am Soc Nephrol 2015;26:2882)
Etiology
- Direct HIV infection of the renal parenchyma, hyperproduction of IFNγ, cell cycle dysregulation (J Am Soc Nephrol 2017;28:719)
- APOL1 polymorphisms predispose to HIVAN in African Americans (J Am Soc Nephrol 2015;26:2882)
Diagrams / tables
Images hosted on other servers:

Mechanisms of HIV associated renal disease
Clinical features
- HIVAN
- Nephrotic syndrome, increased serum creatinine, rapid progression, about half reaching end stage renal disease after 3 years (Am J Kidney Dis 2016;68:e13)
- Most cases with classic HIVAN have advanced HIV disease / AIDS with CD4 counts < 200 cells/mm3 (Front Med (Lausanne) 2018;5:177)
- HIVICK
- Varying kidney manifestation: proteinuria, may be nephrotic, hematuria, reduced glomerular filtration rate (GFR) and low levels of complement are common (Am J Kidney Dis 2016;68:e9)
Diagnosis
- HIVAN suspected when typical clinical symptoms (nephrotic syndrome with acute kidney injury) are associated with renal enlargement at imaging in HIV infected patients (Nephrol Dial Transplant 2012;27:3969)
- Final diagnosis is based on histology
Laboratory
- Low estimated glomerular filtration rate (eGFR) (< 30 mL/min / 1.73 m) (Nephrol Dial Transplant 2012;27:2349)
- High proteinuria (Nephrol Dial Transplant 2012;27:1114)
- High HIV load (Nephrol Dial Transplant 2012;27:1114)
- Low CD4+ count (< 200/mL) (Nephrol Dial Transplant 2012;27:2349)
- A nonnegligible proportion of patients do not present with these typical features
Radiology description
- Normal sized or enlarged kidneys, increased cortical echogenicity, renal pelvicalyceal thickening and loss of the renal sinus fat appearance (Radiographics 2008;28:1339)
Radiology images
Images hosted on other servers:

Ultrasound features of HIVAN
Prognostic factors
- Prognosis is poor in patients with HIVAN, even among those treated with HAART (Nephrol Dial Transplant 2012;27:1114)
- Prognosis of HIVICK appears better than for HIVAN (Am J Kidney Dis 2016;68:e9)
Case reports
- 13 year old boy with noncollapsing HIVAN (Pediatr Nephrol 2011;26:973)
- 25 year old woman with relapse of HIVICK with lupus-like features after transplantation (Am J Kidney Dis 2013;62:335)
- 41 year old man with HIVAN before seroconversion (Am J Kidney Dis 2001;37:E39)
Treatment
- HAART: in patients diagnosed with HIVAN who are not already receiving HAART
- Angiotensin converting enzyme (ACE) inhibitor or angiotensin II receptor blockers (ARB) in proteinuric or hypertensive patients with HIVAN (Kidney Int 2018;93:545)
Microscopic (histologic) description
- Glomerular injury:
- HIVAN
- Segmental or global glomerular tuft collapse with overlying visceral epithelial hyperplasia and hypertrophy, frequent protein droplets into the podocytes seen in collapsing cases (Kidney Int 2018;93:545)
- Noncollapsing focal segmental glomerulosclerosis, NOS is more commonly encountered at biopsy in antiretroviral therapy (ART) treated HIV infected patients (Kidney Int 2018;93:545)
- HIVICK
- Variable mesangial and focal or diffuse endocapillary hypercellularity
- Pinpoint hole appearance and spikes of the glomerular basement membrane on silver stain in cases with dominant membranous pattern (Am J Kidney Dis 2016;68:e9)
- HIVAN
- Tubulointerstitial injury:
- HIVAN: tubulointerstitial disease, including tubular microcyst formation, interstitial inflammation and tubular injury
- Proximal tubulopathy due to antiretroviral agent tenofovir disoproxil fumarate
- Prominent CD8 T cell infiltrates in diffuse infiltrative lymphocytosis syndrome (DILS) and immune restoration inflammatory syndrome (IRIS)
- Vascular injury:
- Thrombotic microangiopathy (rare in the HAART era)
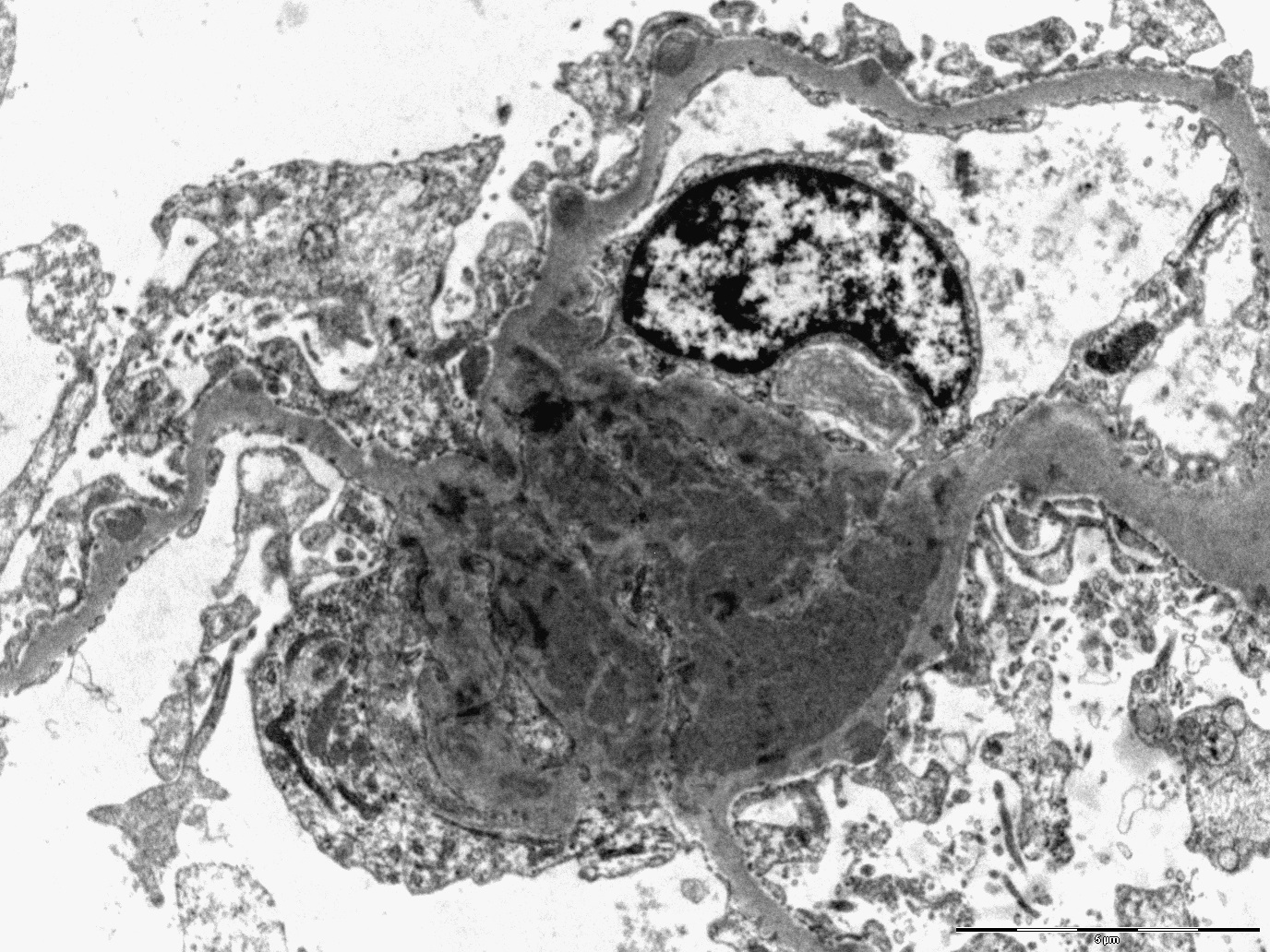
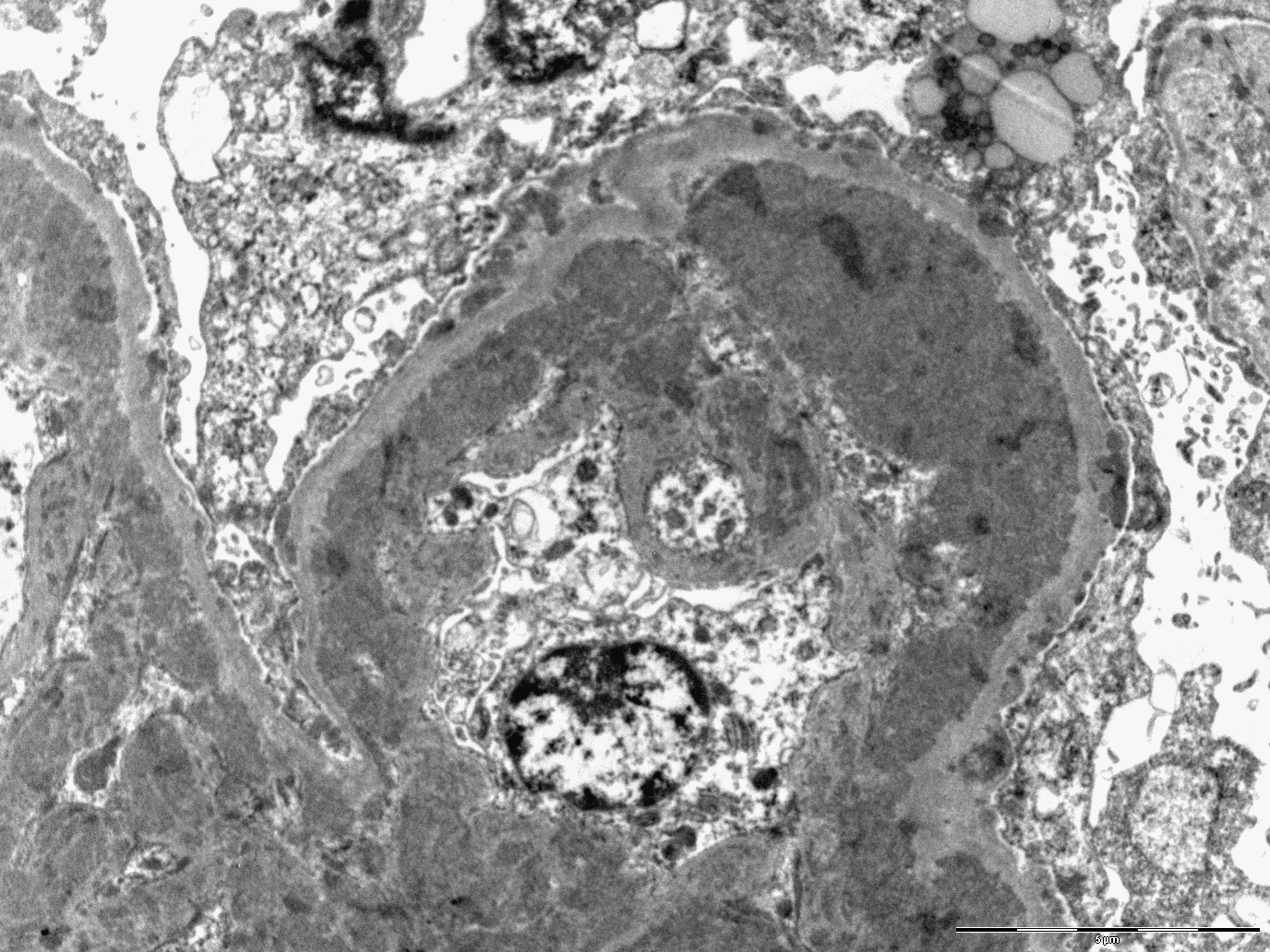
Microscopic (histologic) images
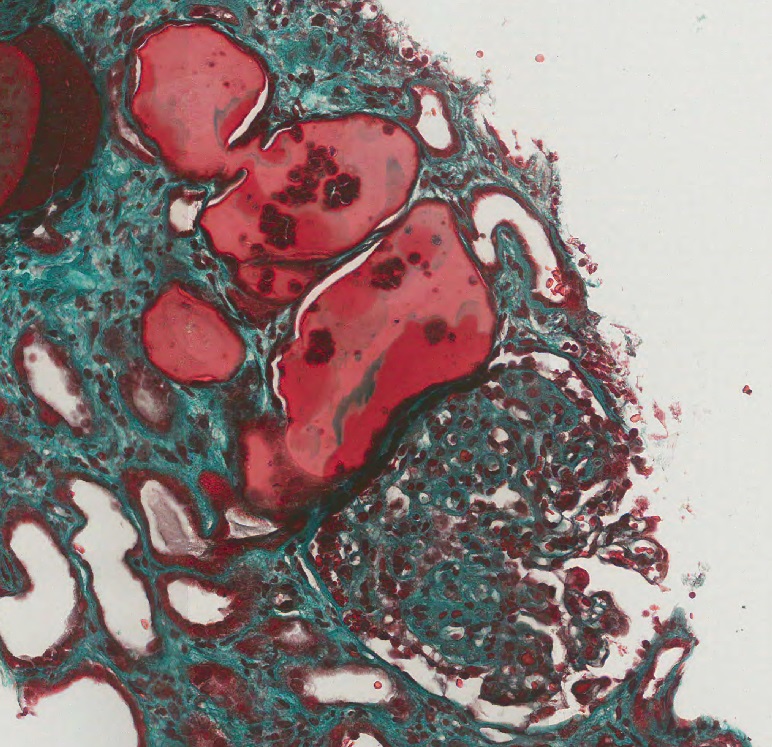
Contributed by Vincenzo L’Imperio, M.D. and Giorgio Cazzaniga, M.D.
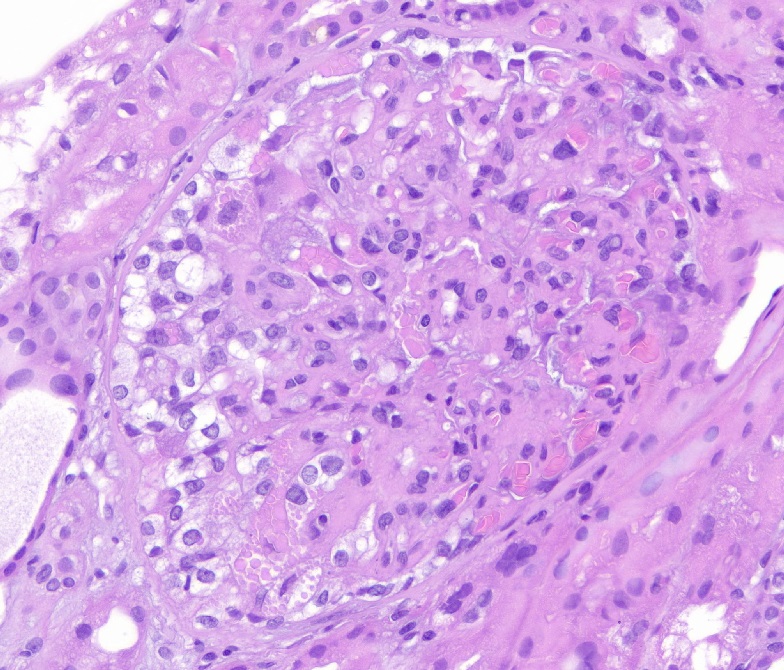
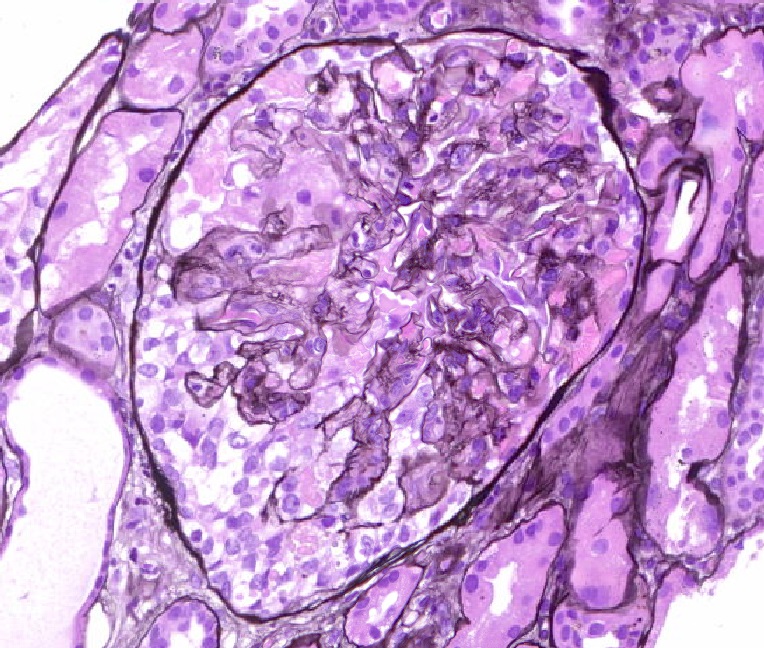
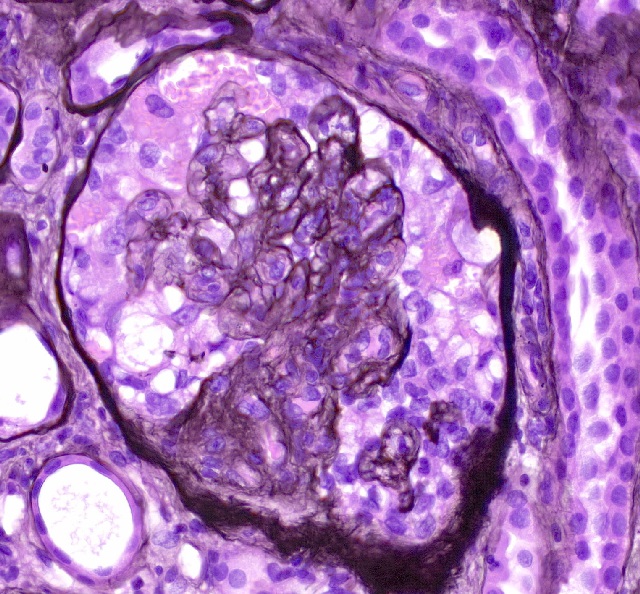
Collapsed glomeruli
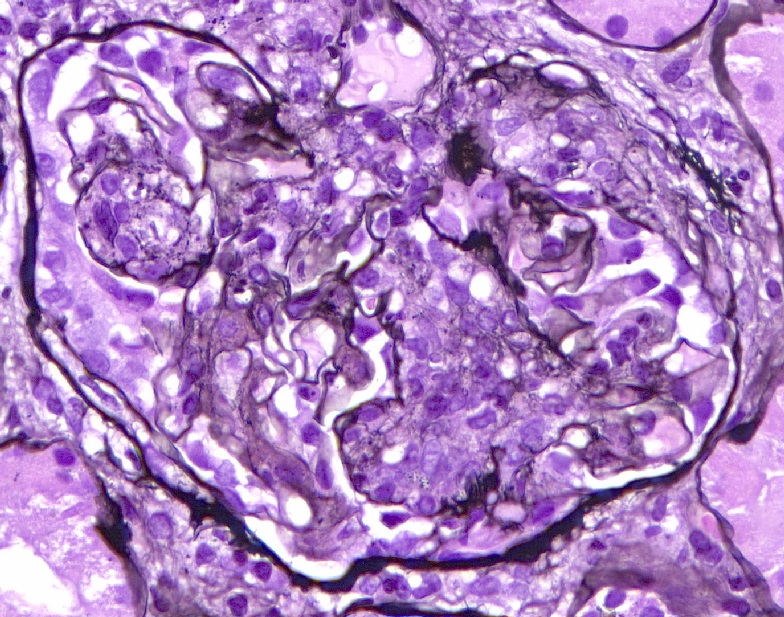
Proliferative
glomerulonephritis
Tubular microcysts with sclerosed glomerulus
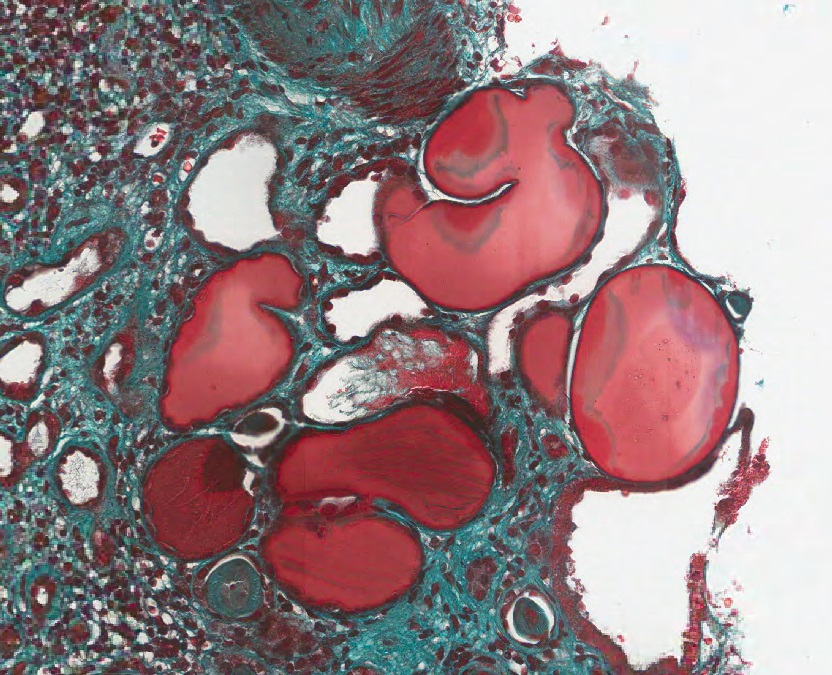
Tubular microcysts
Immunofluorescence description
- Usually negative or nonspecific in HIVAN (Kidney Int 2018;93:545)
- Protein droplets in visceral epithelial cells may stain for immunoglobulins and albumin (Kidney Int 2018;93:545)
- Full house staining with IgG, IgA, IgM, C3 and C1q granular staining in the mesangium and capillary loops in cases of HIVICK (Am J Kidney Dis 2016;68:e9)
- Immunofluorescence for fibrinogen can highlight thrombi in cases of thrombotic microangiopathy
Immunofluorescence images
Contributed by Vincenzo L’Imperio, M.D. and Giorgio Cazzaniga, M.D.
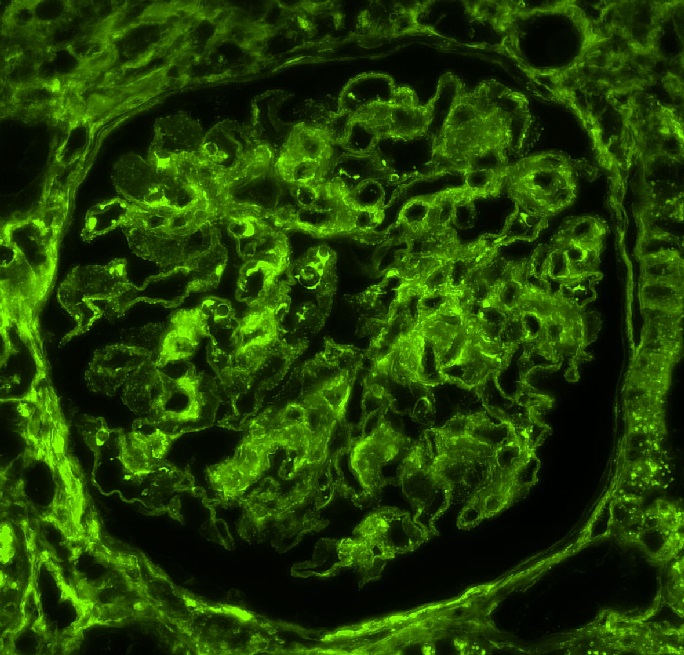
IgG
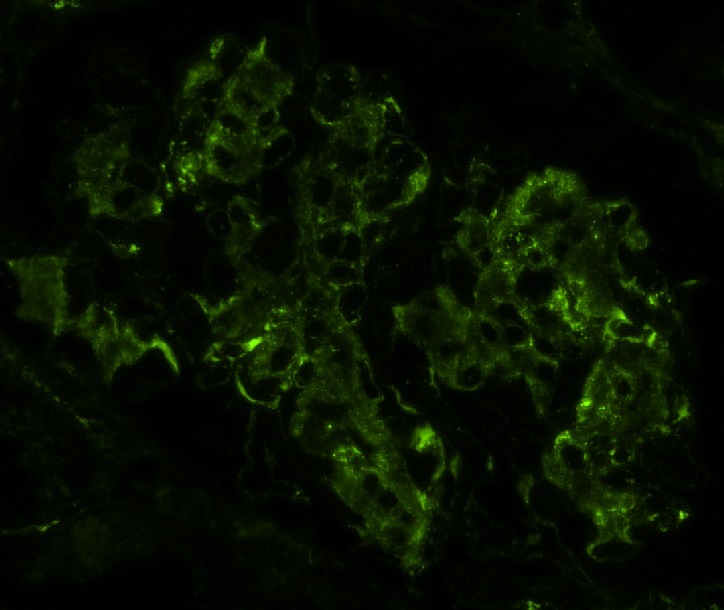
IgA
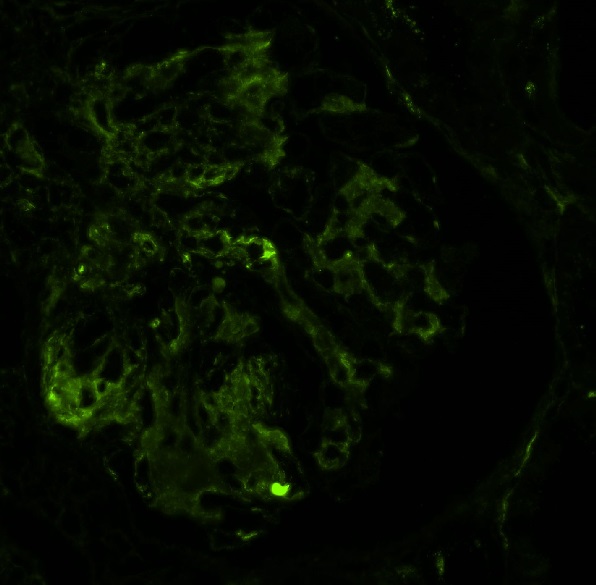
IgM
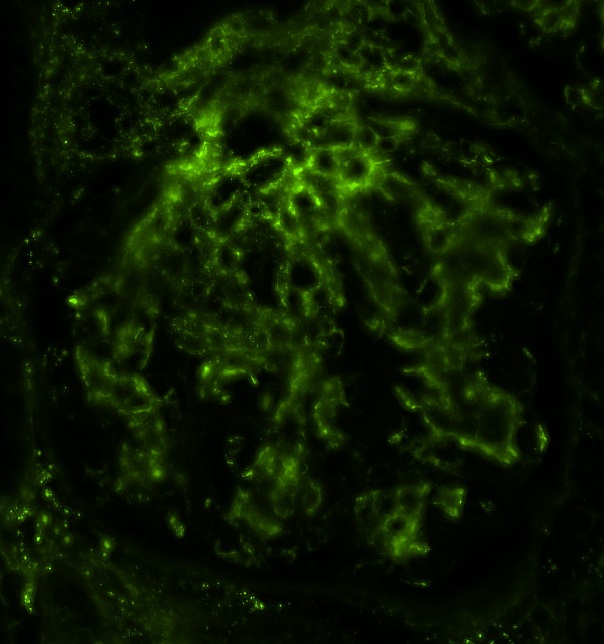
C3
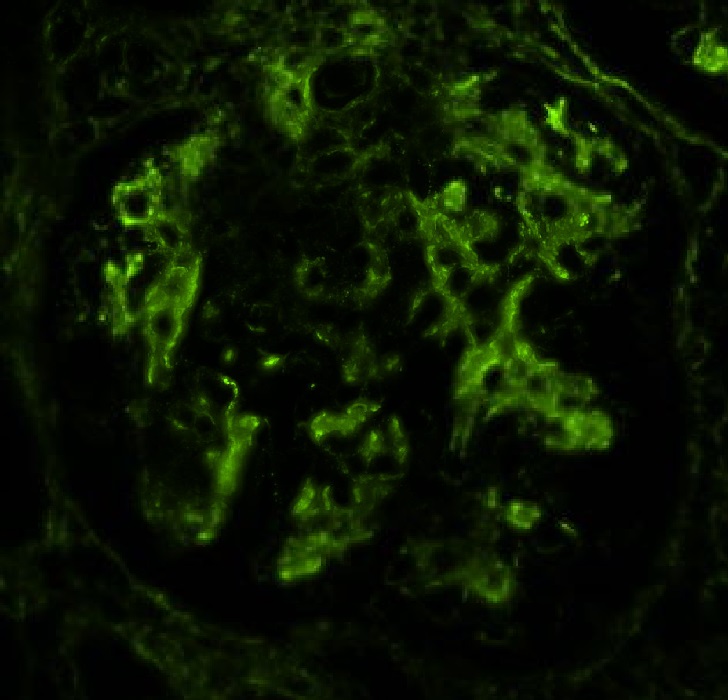
C1q
Positive stains
- Jones methenamine silver (JMS), periodic acid-Schiff (PAS): highlight glomerular architecture with basement membrane collapse in HIVAN
- Further stains not required and often not helpful in differential diagnosis
Negative stains
- HIVAN is accompanied by downregulation of the podocyte maturation markers such as Wilms tumor 1 (WT1), synaptopodin and podocalyxin (J Am Soc Nephrol 2001;12:1677)
Electron microscopy description
- HIVAN (Kidney Int 2018;93:545)
- Extensive foot process effacement
- Hypertrophy and hyperplasia of overlying visceral epithelial cells
- Wrinkled and collapsed glomerular basement membranes
- Tubuloreticular aggregates / inclusions (TRI) in endothelial cells
- Tubuloreticular aggregates may be rare or even absent in patients with low viral loads who are receiving antiretroviral therapy
- HIVICK (Am J Kidney Dis 2016;68:e9)
- Variable deposits are seen, including mesangial, subendothelial and subepithelial deposits
- Tubuloreticular aggregates are present in endothelial cells
- Tubuloreticular aggregates may be decreased or even absent in patients with low viral loads being treated with combination antiretroviral therapy
Electron microscopy images
Contributed by Vincenzo L’Imperio, M.D. and Giorgio Cazzaniga, M.D.
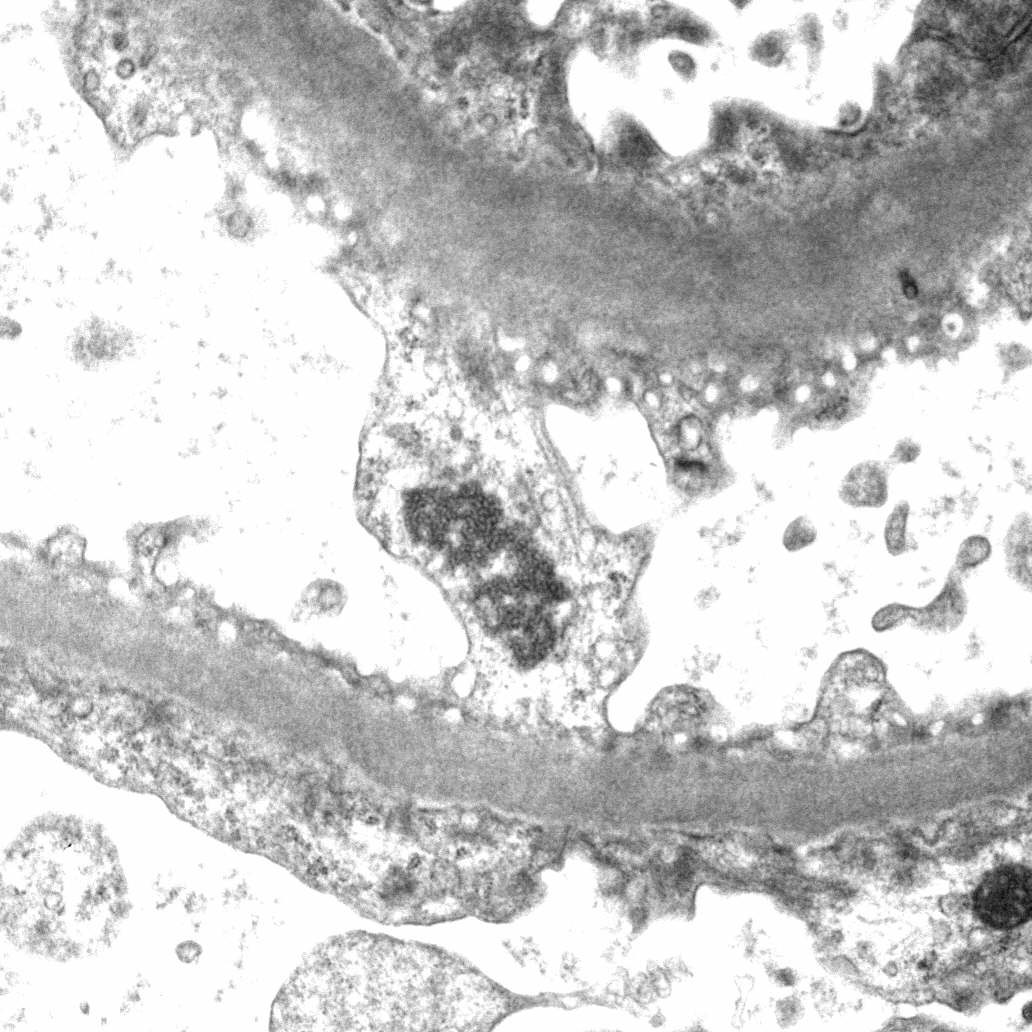
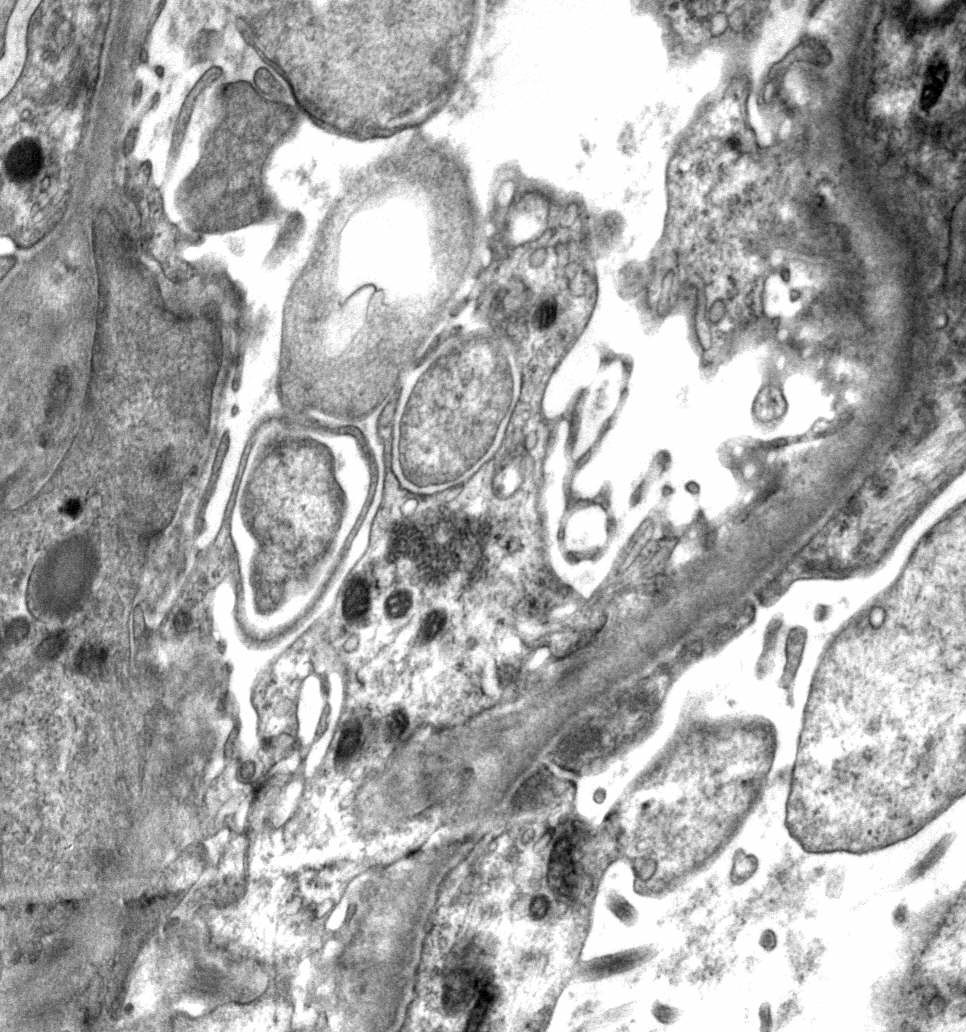
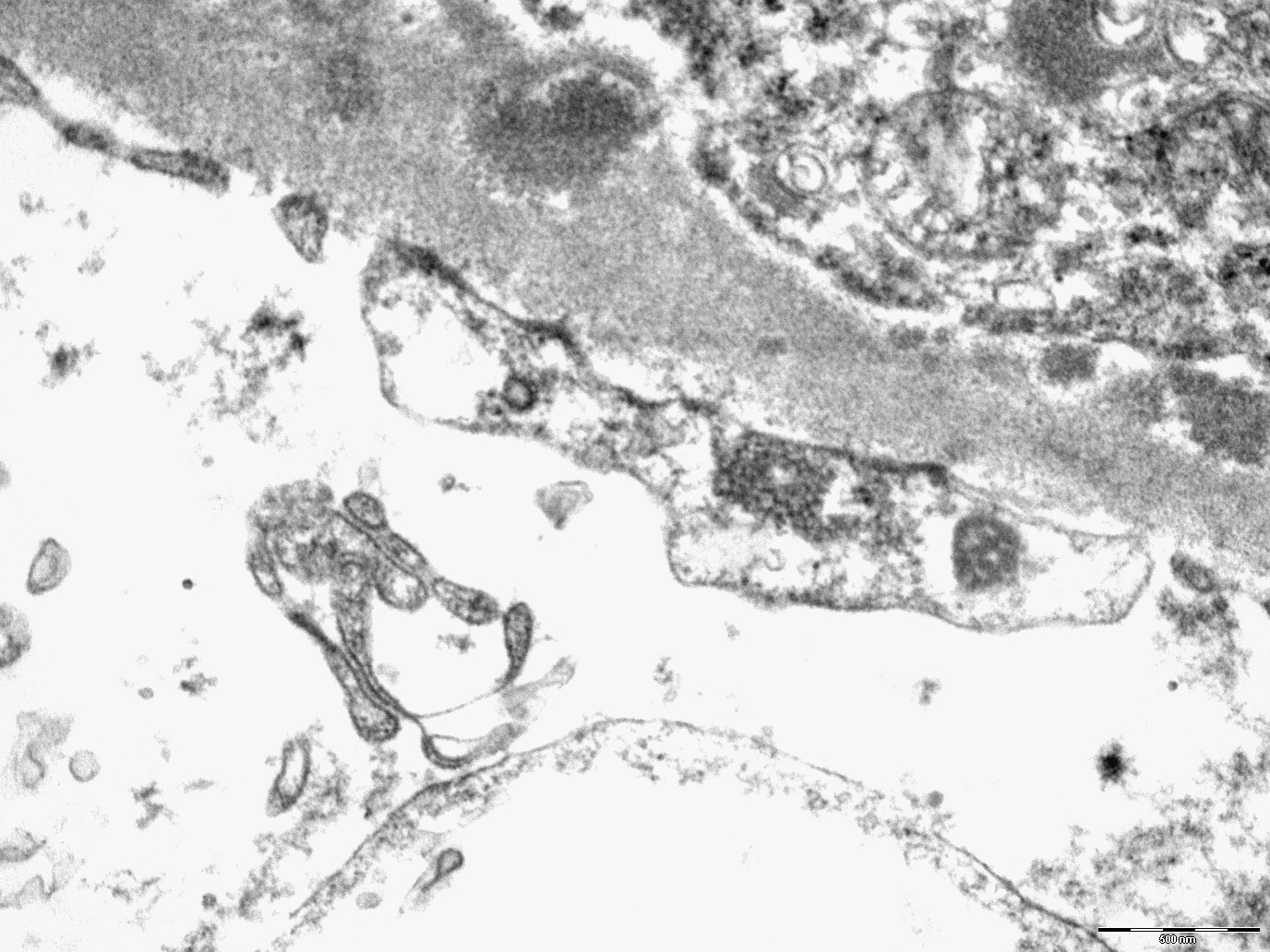
Tubuloreticular inclusion / aggregate (TRI)
Mesangial deposits
Subendothelial deposits
Genetics
- Risk variants in the SRA domain of APOL1 act by a gain of injury or a toxicity mechanism on podocytes or vascular cells (J Am Soc Nephrol 2015;26:2882)
Sample pathology report
- Left kidney, needle core biopsy:
- HIV associated nephropathy (HIVAN) (see comment)
- Comment:
- Microscopic description: Segmental collapse of the capillary loops with occlusion of the lumen and associated podocyte satellite hyperplasia (collapsing lesion). Interstitial fibrosis and tubular atrophy extend to about 20% of the cortex with moderate interstitial lymphocytic infiltrate. Diffuse tubular microcyst formation. No significant changes in the vascular structures.
- Immunofluorescence: No deposits of IgG, IgA, IgM, C3, C1q, kappa or lambda light chains.
- Electron microscopy: Extensive foot process effacement, hypertrophy and hyperplasia of overlying visceral epithelial cells with intracytoplasmic protein droplets, wrinkled and collapsed glomerular basement membranes, tubuloreticular aggregates / inclusions (TRI) in endothelial cells, no deposits.
Differential diagnosis
- Focal segmental glomerulosclerosis collapsing variant, non-HIV related (Kidney Int 2018;93:545):
- Infections (e.g., parvovirus)
- Drugs (e.g., bisphosphonates and calcineurin inhibitors)
- Severe vascular disease (e.g., thrombotic microangiopathy and cocaine use)
- Autoimmune disease (e.g., systemic lupus erythematosus)
- Clinical history of HIV infection and the presence of tubuloreticular aggregates indicate HIVAN as the etiology of the collapsing lesions
- Crescentic glomerulonephritis:
- Antineutrophil cytoplasmic antibody (ANCA) associated glomerulonephritis can show parietal epithelial proliferation but generally does not have protein reabsorption droplets in the epithelial cells
- Crescents are also often accompanied by segmental necrosis and glomerular basement membrane breaks with fibrinous exudates, features that distinguish them from collapsing lesions
- Lupus nephritis (Am J Kidney Dis 2016;68:e9):
- Distinction among lupus nephritis and lupus-like HIVICK must be made on clinical grounds
Board review style question #1
Which gene variant increases the risk of developing collapsing focal segmental glomerulosclerosis in HIV patients?
- ADAMST7
- APOL1
- COL4A5
- PLA2R1
Board review style answer #1
B. APOL1. The risk variants in the SRA domain of APOL1 act by a gain of injury in development of HIV associated nephropathy. ADAMST7 is implicated in pathogenesis of arthritis, the mutation of COL4A5 is responsible for the Alport syndrome and PLA2R1 encodes one of the antibody target proteins in membranous nephropathy.
Comment Here
Reference: HIV associated renal disease
Comment Here
Reference: HIV associated renal disease
Board review style question #2
Which of the following is the name of the electron microscopy feature depicted above in a case of HIV associated collapsing glomerulopathy?
- Clathrin coated vesicles (CCVs)
- Multivesicular body (MVB)
- Podocyte infoldings
- Tubuloreticular inclusion (TRI)
Board review style answer #2
D. Tubuloreticular inclusion (TRI). Tubuloreticular inclusion presence has been shown to be a marker of systemic stimulation by interferons such as in HIV associated renal disease. Podocyte infoldings are translucent microspheres generated by invagination of the podocyte cytoplasm into the basement membranes. Multivesicular bodies are formed by invaginations of endosomes and are intermediates in trafficking for lysosomes. Clathrin coated vesicles are normal subcellular organelles involved in intracellular transport.
Comment Here
Reference: HIV associated renal disease
Comment Here
Reference: HIV associated renal disease
