

Kidney nontumor / medical renal
Glomerular disease
Infectious glomerulonephritis
Bacterial infection related GN
Editorial Board Members: Jonathan E. Zuckerman, M.D., Ph.D., Nicole K. Andeen, M.D.


Last author update: 15 September 2021
Last staff update: 15 September 2021
Copyright: 2021, PathologyOutlines.com, Inc.
PubMed Search: Bacterial infection related glomerulonephritis "last 5 years"[DP]
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Laboratory | Prognostic factors | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Immunofluorescence description | Immunofluorescence images | Electron microscopy description | Electron microscopy images | Genetics | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Lu Z, Kung VL. Bacterial infection related GN. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/kidneybacterialinfectionGN.html. Accessed April 18th, 2024.
Definition / general
- Most common bacterial infection related glomerulonephritides in countries with higher human development indices are IgA dominant infection related glomerulonephritis and infectious endocarditis associated glomerulonephritis
- Biopsy findings are variable
- Subepithelial hump shaped deposits in mesangial waist regions are a characteristic ultrastructural finding of IgA dominant infection related glomerulonephritis
Essential features
- In contrast to acute poststreptoccocal glomerulonephritis, which develops after resolution of infection and is most common in children, both IgA dominant infection related glomerulonephritis and infectious endocarditis associated glomerulonephritis are associated with ongoing infection in adults
- Staphylococcus aureus is the most common infectious trigger of both IgA dominant infection related glomerulonephritis and infectious endocarditis associated glomerulonephritis
- A subset of patients develop positive antineutrophil cytoplasmic antibody (ANCA) serologies
- Treatment of underlying infection is required
- Diabetes and advanced age portend a worse prognosis
Terminology
- Staphylococcus infection associated glomerulonephritis
- Infection related glomerulonephritis with IgA deposits
- IgA dominant postinfectious glomerulonephritis
ICD coding
Epidemiology
- IgA dominant infection related glomerulonephritis (Nat Rev Nephrol 2020;16:32, Diagn Pathol 2020;15:62, Hum Pathol 2003;34:1235, Am J Nephrol 2015;41:98):
- Male predominance
- Older adults with underlying comorbidities, such as diabetes mellitus, alcoholism and hypertension and active bacterial infection
- Most common infectious agent is Staphylococcus aureus
- Infection may be apparent (e.g. skin or soft tissue infections) or occult (e.g. abscess, endocarditis or osteomyelitis)
- Infectious endocarditis associated glomerulonephritis (Kidney Int 2015;87:1241):
- M:F = 3.5:1
- Mean age of 48 years
- Intravenous drug abuse, valvular heart disease, prosthetic heart valves, immunosuppression, malignancy
- Most common infectious agent is Staphyloccocus aureus, followed by Streptococcus species; there are also case reports of Bacillus cereus, Gemella morbillorum, Bartonella species, Cardiobacterium hominis and Coxiella burnetii
- Shunt nephritis (Clin Nephrol 1983;19:48):
- Complication of ventriculoatrial shunts used as palliative therapy for hydrocephalus, hardware infection
- Common pathogens include Staphylococcus epidermidis, Proprionibacterium acnes and Staphylococcus aureus
- As use of ventriculoperitoneal shunts is now favored, shunt nephritis has become very rare
Sites
- Kidneys
- Sometimes skin rash, due to ANCA vasculitis or leukocytoclastic vasculitis with IgA staining
Pathophysiology
- Immune reaction to bacterial proteins, including bacterial superantigens, such as staphylococcal enterotoxins, ultimately result in immune complex deposition in glomeruli, inflammation, complement activation and glomerular injury
- Proposed mechanisms of immune complex deposition in glomeruli:
- Bacterial antigens may be present in glomeruli (Kidney Int 2004;66:121)
- Bacterial antigen specific antibodies may cross react with glomerular antigens
- Neutrophil activation and formation of autoantibodies to neutrophil proteins
Clinical features
- Most patients present with acute kidney injury and nephritic or nephrotic syndrome
- Sites of infection include the upper respiratory tract, skin, lung, heart, urinary tract, teeth / oral mucosa, bone and deep seated abscesses (Kidney Int 2013;83:792)
- Most common bacterial infections are Staphyloccocus aureus and Streptococcus species; many other bacteria also reported (Kidney Int 2013;83:792)
- Infection may not be clinically apparent and is only discovered at the time of glomerulonephritis diagnosis in 16 - 45% of cases (J Am Soc Nephrol 2011;22:187)
- Positive bacterial cultures in 41 - 58% of cases (Medicine (Baltimore) 2008;87:21, Medicine (Baltimore) 1995;74:63)
Diagnosis
- Clinical history
- Bacterial culture
- Serum complement levels
- Serologic workup for nephritic and nephrotic syndromes
- Kidney biopsy
Laboratory
- IgA dominant infection related glomerulonephritis (Nat Rev Nephrol 2020;16:32, Diagn Pathol 2020;15:62, Hum Pathol 2003;34:1235, Am J Nephrol 2015;41:98):
- Acute kidney injury (majority with rise in serum creatinine levels to > 3 mg/dL), hematuria and proteinuria (often nephrotic range) common
- Hypocomplementemia reported in up to 60% of cases
- May have circulating cryoglobulins (Clin J Am Soc Nephrol 2006;1:1179, Kidney Int Rep 2018;3:1128)
- Infectious endocarditis associated glomerulonephritis (Kidney Int 2015;87:1241):
- Acute kidney injury and a nephritic urine sediment common
- Nephrotic range proteinuria uncommon
- Hypocomplementemia common: low C3 levels present in 53% of patients, low C4 levels in 19% of patients
- Serologic testing for ANCA positive in 28% of patients
Prognostic factors
- Diabetes and advanced age portend a worse prognosis (Medicine (Baltimore) 2016;95:e3386)
- IgA dominant infection related glomerulonephritis:
- Progression to end stage renal disease in 20 - 80% of patients (Am J Nephrol 2015;41:98, Hum Pathol 2003;34:1235)
- Infectious endocarditis associated glomerulonephritis:
- Complete recovery in 32% of patients, persistent renal dysfunction in 37%, end stage renal disease in 10% and death in 21% (Kidney Int 2015;87:1241)
Case reports
- 33 - 75 year old men and women with Staphylococcus auerus and IgA dominant deposits and cryoglobulinemic features on biopsy (Kidney Int Rep 2018;3:1128)
- 56 - 80 year old men and women with Staphylococcus auerus infection, biopsied for acute renal failure with heavy proteinuria and hematuria (Clin J Am Soc Nephrol 2006;1:1179)
- 64 year old man with Staphylococcus auerus infection, presenting with leukocytoclastic vasculitis, oliguric acute kidney injury, microscopic hematuria and nephrotic range proteinuria (Can J Kidney Health Dis 2018;5:2054358118776325)
Treatment
- Primary treatment is antibiotic therapy targeting underlying infection
- Some treat with immunosuppression in addition to antibiotic therapy in cases with ANCA positivity and crescentic glomerulonephritis (Medicine (Baltimore) 2020;99:e21358)
Microscopic (histologic) description
- IgA dominant infection related glomerulonephritis:
- Most cases with some amount of endocapillary hypercellularity with neutrophils
- May be diffuse and global (acute exudative glomerulonephritis) or focal and segmental
- Focal crescents can be seen
- Rarely may have focal cryoglobulin-like features, including scattered subendothelial wire loop deposits and intracapillary hyaline pseudothrombi (Clin J Am Soc Nephrol 2006;1:1179, Kidney Int Rep 2018;3:1128)
- Infectious endocarditis associated glomerulonephritis:
- Findings variable
- A crescentic glomerulonephritis is often found
- With or without endocapillary or mesangial hypercellularity
- With or without membranoproliferative features
Microscopic (histologic) images
Contributed by Vanderlene Liu Kung, M.D., Ph.D.
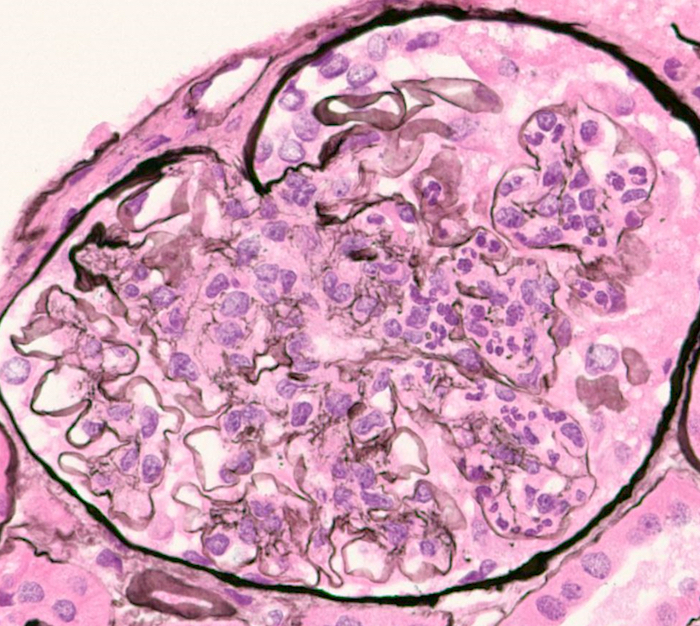
Glomerular capillary luminal neutrophils
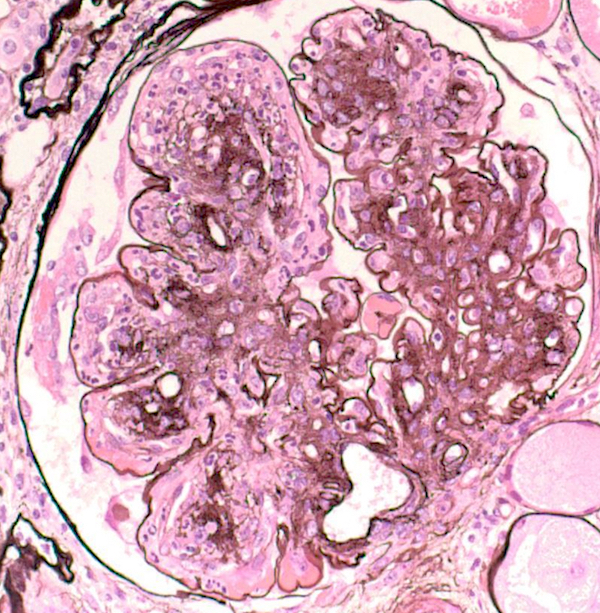
Diabetic
glomerulosclerosis
with exudative GN
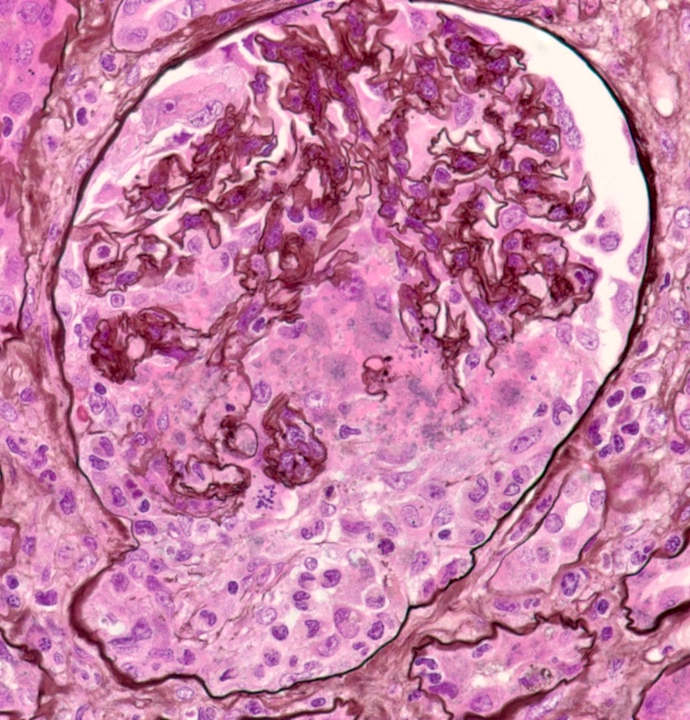
Cellular crescent
Immunofluorescence description
- IgA dominant infection related glomerulonephritis:
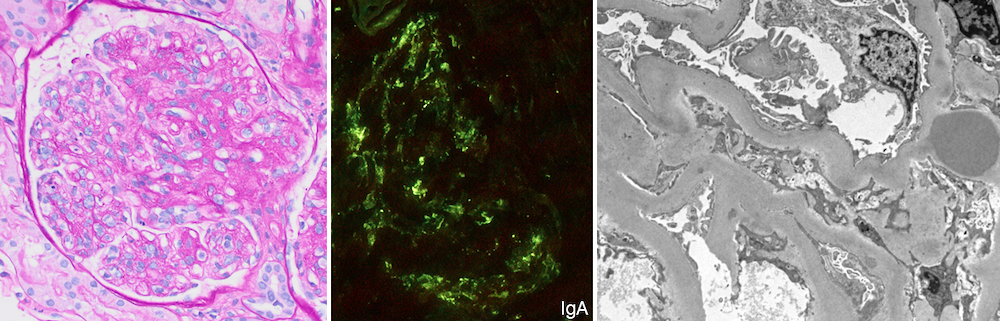
- Granular predominantly mesangial and some capillary wall staining for C3 and IgA
- IgA is sole, dominant or codominant immunoglobulin
- Infectious endocarditis associated glomerulonephritis:
- Usually dominant staining for C3 and IgM, followed by IgG and IgA
- May be pauci-immune (< 2+ intensity staining)
Immunofluorescence images
Contributed by Vanderlene Liu Kung, M.D., Ph.D.
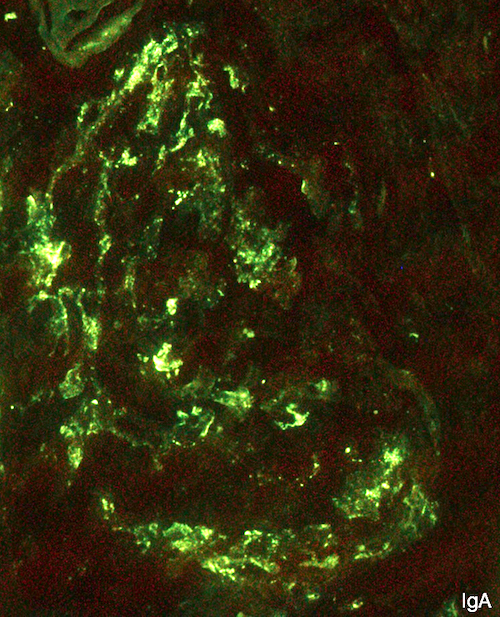
Granular mesangial IgA
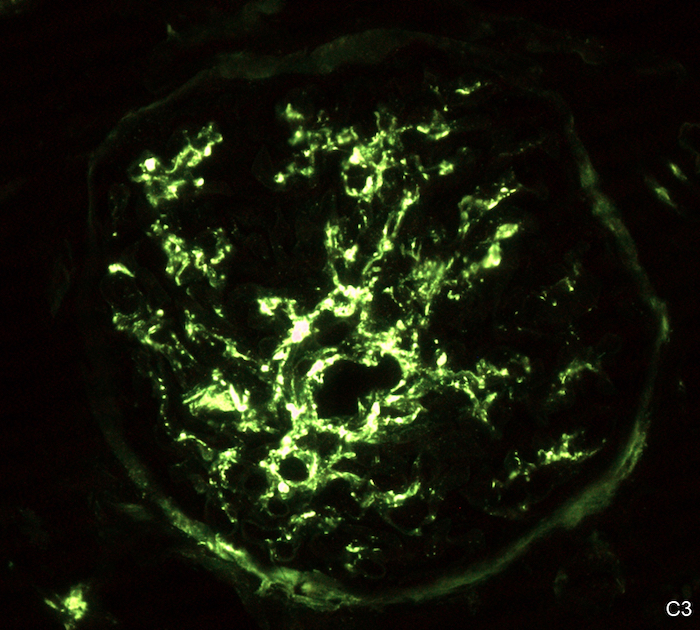
Granular mesangial C3
Electron microscopy description
- IgA dominant infection related glomerulonephritis:
- Scattered mesangial deposits
- Subepithelial hump shaped deposits particularly at mesangial waist (reported in 31 - 100% of cases) (Hum Pathol 2008;39:1309)
- In rare cases with cryoglobulin-like features, large subendothelial and intraluminal deposits seen
- Infectious endocarditis associated glomerulonephritis:
- Small mesangial and capillary wall deposits
- Subepithelial hump shaped deposits uncommon
Electron microscopy images
Contributed by Vanderlene Liu Kung, M.D., Ph.D.
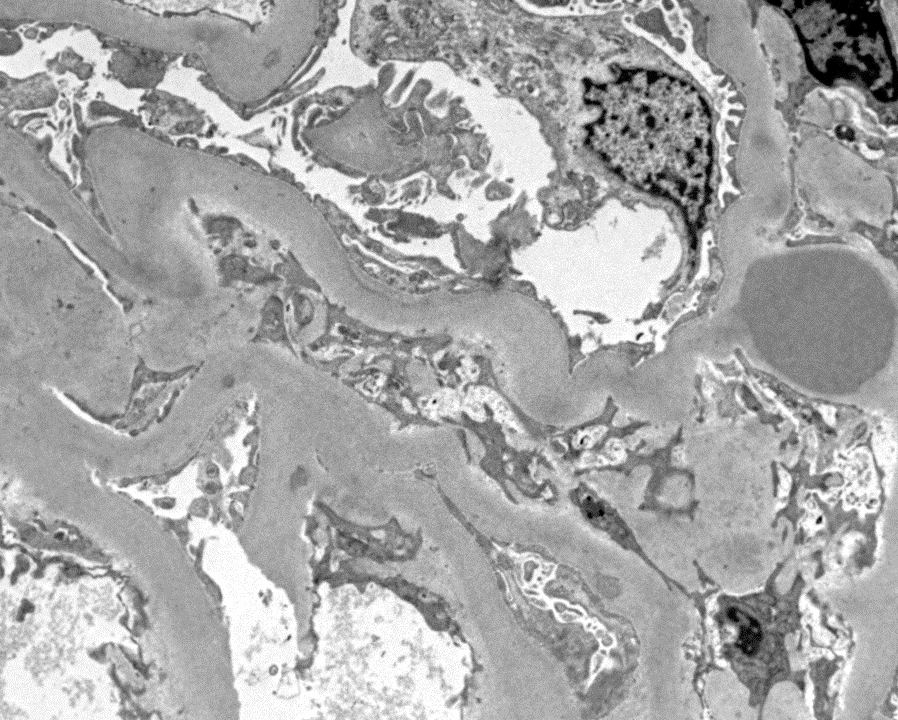
Intramembranous / subepithelial deposits
Genetics
- Genome wide association study of individuals of European ancestry identified polymorphisms in genes encoding the MHC class II antigens HLA-DRA and HLA-DRB1 to be associated with susceptibility to Staphylococcus aureus infection (J Infect Dis 2016;213:816)
- Genetic contributions to why only a subset of individuals with bacterial infections develop renal pathology have yet to be determined
Sample pathology report
- Native kidney, biopsy:
- IgA dominant infection related glomerulonephritis
Differential diagnosis
- IgA nephropathy:
- Chronic disease
- Serum C3 level usually normal
- Light microscopy: exudative glomerulonephritis uncommon
- Immunofluorescence: IgA staining usually stronger than C3
- Electron microscopy: mesangial deposits common, humps absent
- IgA vasculitis:
- Not associated with older age or diabetes
- Light microscopy: exudative glomerulonephritis uncommon
- Immunofluorescence: IgA staining usually stronger than C3
- Electron microscopy: mesangial and subendothelial deposits can be seen, humps absent
- ANCA vasculitis:
- Light microscopy: crescents without mesangial or endocapillary hypercellularity
- Immunofluorescence: pauci-immune
- Electron microscopy: few to absent deposits
Additional references
Board review style question #1
What is the most appropriate primary diagnosis on this biopsy from an 80 year old woman with poorly controlled hypertension and diabetes and untreated cellulitis, who presents with new onset hematuria and proteinuria and is found to have low serum C3?
- Acute postinfectious glomerulonephritis
- Diabetic glomerulosclerosis
- IgA dominant infection related glomerulonephritis
- New onset IgA nephropathy
Board review style answer #1
C. IgA dominant infection related glomerulonephritis
Comment here
Reference: Bacterial infection related glomerulonephritis
Comment here
Reference: Bacterial infection related glomerulonephritis
Board review style question #2
Which of the following clinical scenarios is most compatible with an endocarditis associated glomerulonephritis?
- 10 year old boy with acute nephritic syndrome 2 weeks following streptococcal pharyngitis
- 30 year old man with history of intravenous drug abuse, who presents with rash, acute kidney injury, hematuria and heavy proteinuria and is found to have positive MPO and PR3 ANCA serologies
- 40 year old woman with systemic lupus erythematosus, who presents with nephrotic syndrome
- 60 year old man with longstanding, poorly controlled diabetes, who presents with slowly progressive worsening renal function and proteinuria
Board review style answer #2
B. 30 year old man with history of intravenous drug abuse, who presents with rash, acute kidney injury, hematuria and heavy proteinuria and is found to have positive MPO and PR3 ANCA serologies
Comment here
Reference: Bacterial infection related glomerulonephritis
Comment here
Reference: Bacterial infection related glomerulonephritis
