

Kidney tumor
Benign / borderline adult tumors
Well differentiated neuroendocrine tumor (carcinoid)
Editorial Board Members: Debra L. Zynger, M.D., Nicole K. Andeen, M.D.


Last author update: 28 December 2021
Last staff update: 21 March 2024 (update in progress)
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Well differentiated neuroendocrine kidney tumor
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Negative stains | Electron microscopy description | Electron microscopy images | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Cheng L, Tretiakova M. Well differentiated neuroendocrine tumor (carcinoid). PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/kidneytumormalignantcarcinoid.html. Accessed April 17th, 2024.
Definition / general
- Well differentiated epithelial neoplasm arising from renal parenchyma and showing neuroendocrine differentiation
Essential features
- Rare tumor arising from renal parenchyma; associated with horseshoe kidney and mature teratoma of kidney
- Expresses neuroendocrine markers histologically but most are clinically nonfunctional
- Distant metastasis is common at diagnosis and Dual Tracer PET imaging (DOTATATE scan) can help identify metastases
Terminology
- Carcinoid tumor, atypical carcinoid tumor
ICD coding
Epidemiology
- Rare primary tumor in kidney; 58 cases reported in Surveillance, Epidemiology and End Results (SEER) database (Front Endocrinol (Lausanne) 2021;11:624251)
- Median age = 59; M:F = 52.2%: 48.8% for all renal neuroendocrine neoplasms (Front Endocrinol (Lausanne) 2021;11:624251)
- 20 - 30% of cases are associated with horseshoe kidney (Clin Genitourin Cancer 2020;18:e343)
- Can arise within mature teratoma of the kidney (Diagn Pathol 2007;2:15)
Sites
- Arises from renal parenchyma; can extend into renal pelvis and inferior vena cava (Urology 2020;135:e2)
Pathophysiology
- Indeterminate but may originate from renal stem cells or misplaced neural crest cells since no neuroendocrine cells have been identified in adult renal parenchyma (Arch Pathol Lab Med 2006;130:1693, Front Endocrinol (Lausanne) 2021;11:624251)
Etiology
- Uncertain
Clinical features
- Symptoms including abdominal / back / flank pain, hematuria, palpable mass, etc. (Front Endocrinol (Lausanne) 2021;11:624251)
- 33% of patients are asymptomatic (J Urol 2006;176:2359)
- Metastasis presented at diagnosis in 12/21 (57%) patients (Am J Surg Pathol 2007;31:1539)
- Tumors are usually nonfunctional but rarely show ectopic adrenocorticotropic hormone (ACTH) syndrome (Endocrinol Diabetes Metab Case Rep 2021;2021:20)
Diagnosis
- Imaging study followed by histological examination of biopsy or resection specimen
Laboratory
- May show increased serum chromogranin A and urine 5-HIAA (Front Endocrinol (Lausanne) 2021;11:624251)
Radiology description
- CT: solid hypodense (55%) or hyperdense (29%) mass with calcifications (33%), mimicking renal cell carcinoma (Radiol Case Rep 2015;9:923)
- Gallium 68 DOTATATE PET / CT: hypermetabolic / increased uptake (Perm J 2020;24:19.147, Pathol Oncol Res 2020;26:341)
Radiology images
Images hosted on other servers:

Right renal mass

Enhancing right renal mass

Tumor extending into IVC

Cystic tumor

Slightly hyperdense tumor

Metastases on DOTATATE scan
Prognostic factors
- Unfavorable prognostic factors:
- Age: > 40 years
- Size: > 4 cm
- > 1 mitotic figure/10 high power fields (HPF)
- Metastasis at diagnosis
- Extension throughout renal capsule
- Reference: J Urol 2006;176:2359
Case reports
- Woman in late 40s presented with a 14.9 cm mass arising from horseshoe kidney (Mayo Clin Proc 2021;96:1687)
- 47 year old man presented with a 23.5 cm cystic lesion in the right kidney (Turk Patoloji Derg 2020;36:90)
- 51 year old man presented with left renal mass and ectopic ACTH syndrome (Endocrinol Diabetes Metab Case Rep 2021;2021:20)
- 55 year old man with renal well differentiated neuroendocrine tumor and bilateral multiple clear cell papillary renal cell carcinomas (Case Rep Pathol 2017;2017:9672368)
- 5 cases of primary renal well differentiated neuroendocrine tumor in 1 institution (Pathol Oncol Res 2020;26:341)
Treatment
- Nephrectomy with lymph node dissection
- Somatostatin analogs, tyrosine kinase inhibitors and peptide receptor radionuclide therapy (PRRT) for metastasis (Front Endocrinol (Lausanne) 2021;11:624251)
Gross description
- Well circumscribed, soft, brown-tan mass with focal hemorrhage, necrosis or cystic degeneration
Gross images
Contributed by Jennifer Jeung, M.D. (Case #204)


Tan, soft, well encapsulated mass in lower pole
Images hosted on other servers:

Tumor in horseshoe kidney

Renal mass with hemorrhage

Necrotic renal mass

Tumor involving sinus fat

Cystic renal mass
Microscopic (histologic) description
- Variable architecture: tightly packed cords with minimal stroma (most common, 81%), sheet-like / solid pattern, nests / organoid pattern, trabeculae, ribbons, pseudo glands, etc. (Am J Surg Pathol 2007;31:1539)
- Round to oval / elongated nuclei with stippled / speckled chromatin, inconspicuous nucleoli and moderate eosinophilic / granular cytoplasm
- Occasional calcifications (5/21, 24%) of variable sizes (Am J Surg Pathol 2007;31:1539)
- Usually lack of necrosis and low mitotic activity (< 4/10 HPF)
- Grading of well differentiated neuroendocrine tumor of kidney is not clearly defined in WHO 2016 classification; mitotic counts and the Ki67 index may be good markers (Diagn Pathol 2019;14:12)
Microscopic (histologic) images
Contributed by Maria Tretiakova, M.D., Ph.D. and Sleiman Khalil, M.D.
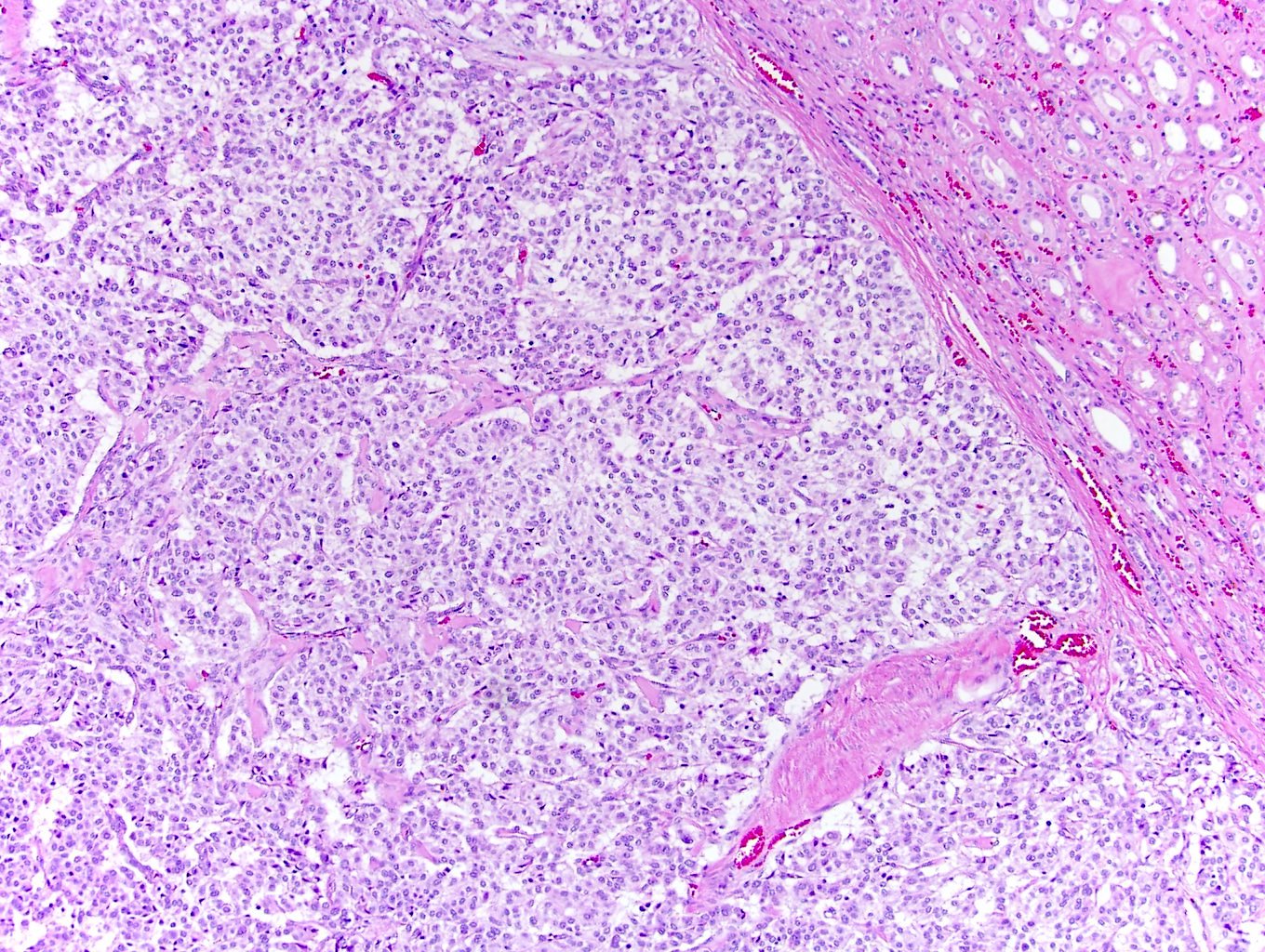
Well demarcated tumor

Nests and pseudoglands
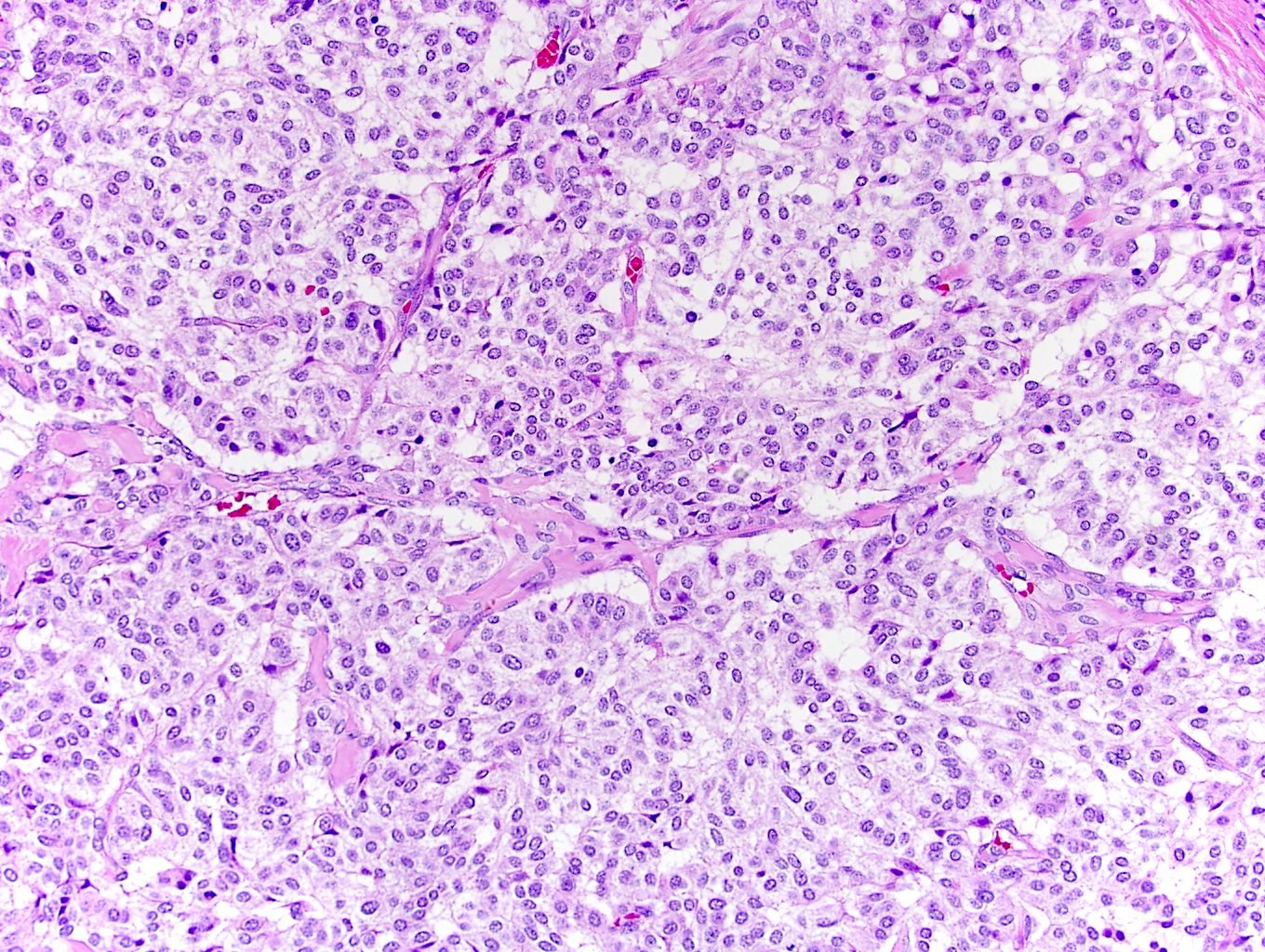
Monotonous tumor cells

Positive synaptophysin
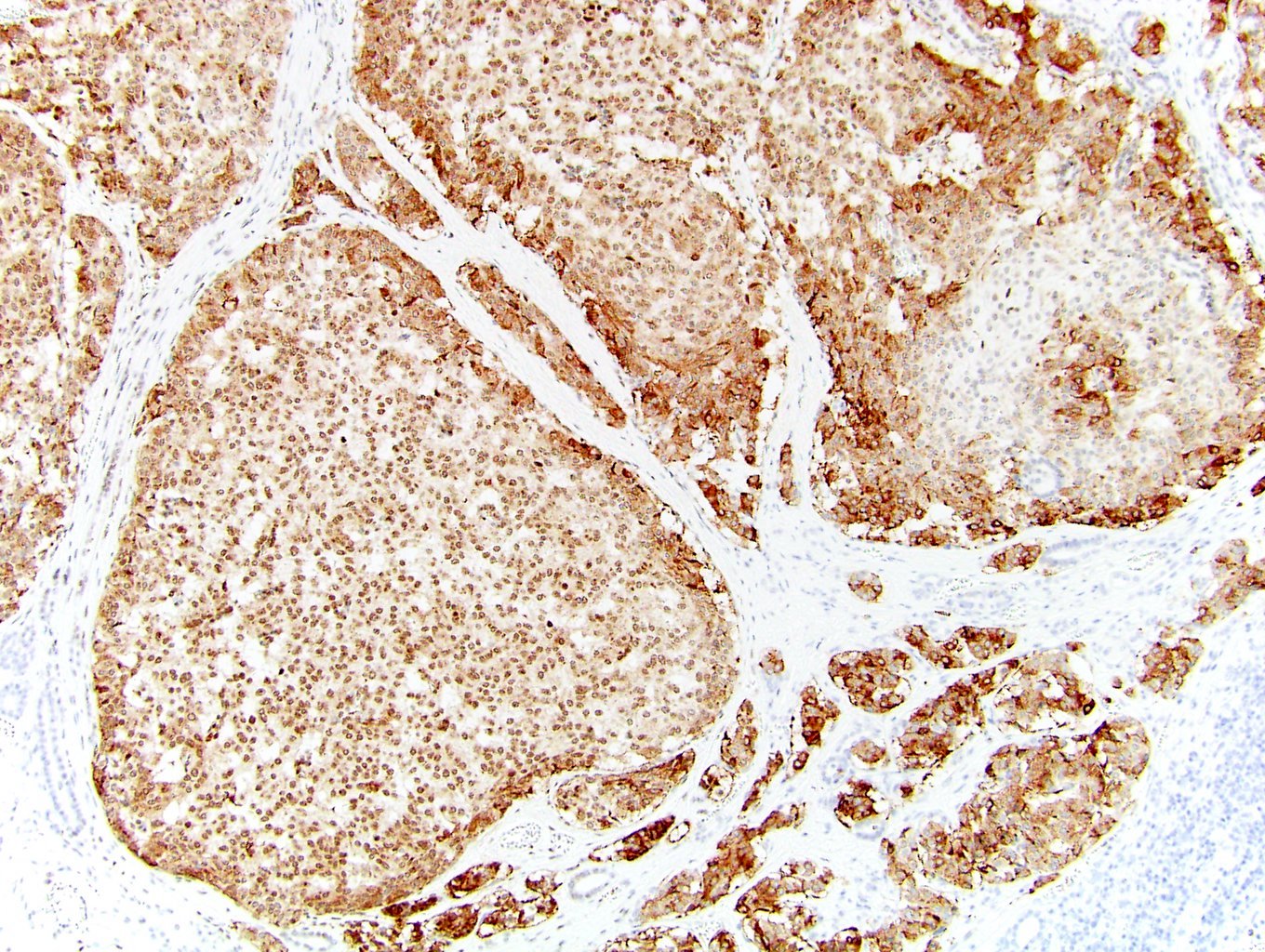
Positive chromogranin

Positive CD99
Contributed by Leandro Freitas, M.D., Ana Grizotto, M.D., Athanase Billis, M.D. and the Genitourinary Pathology Society (Case #521)
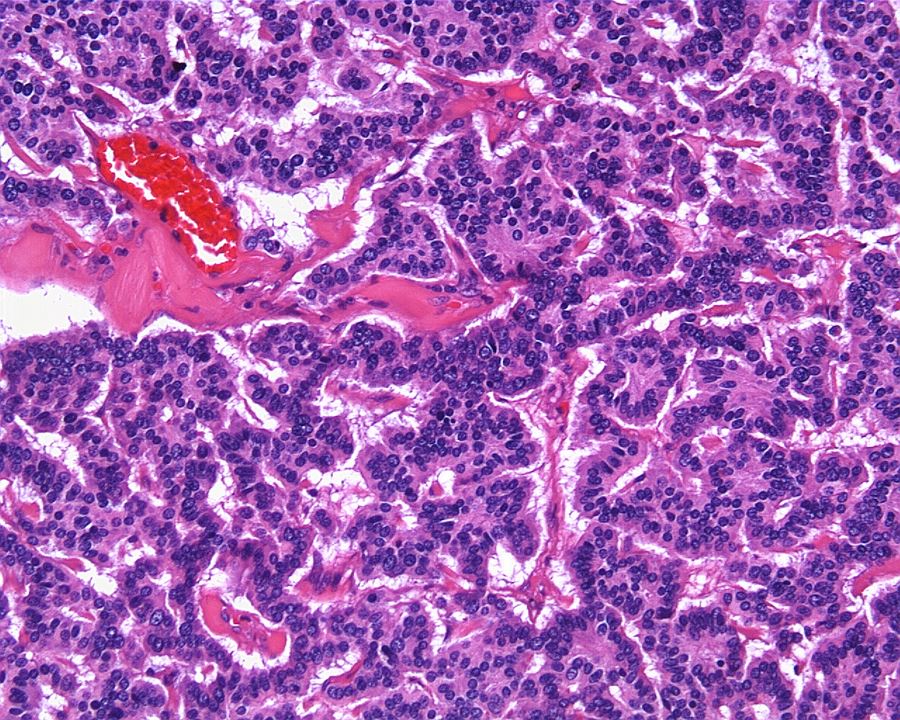
Classic appearance
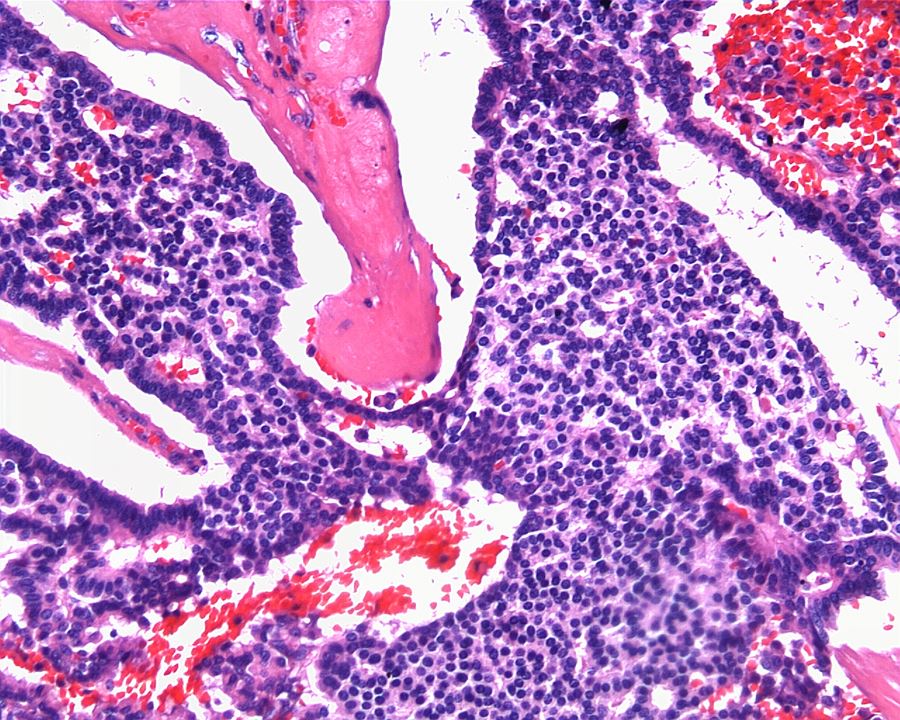
Prominent stroma
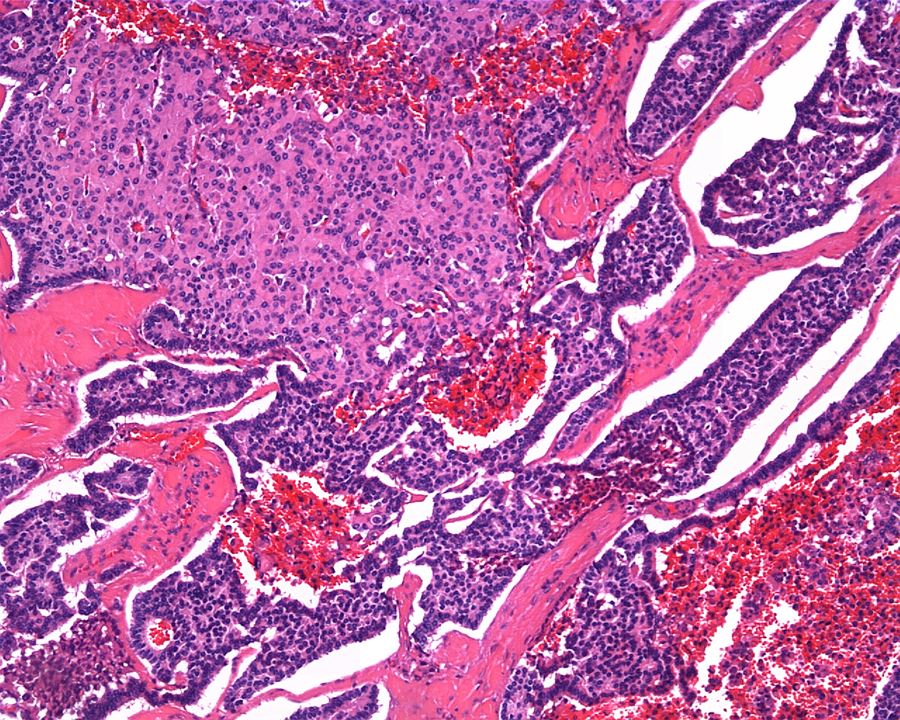
Areas of solid growth
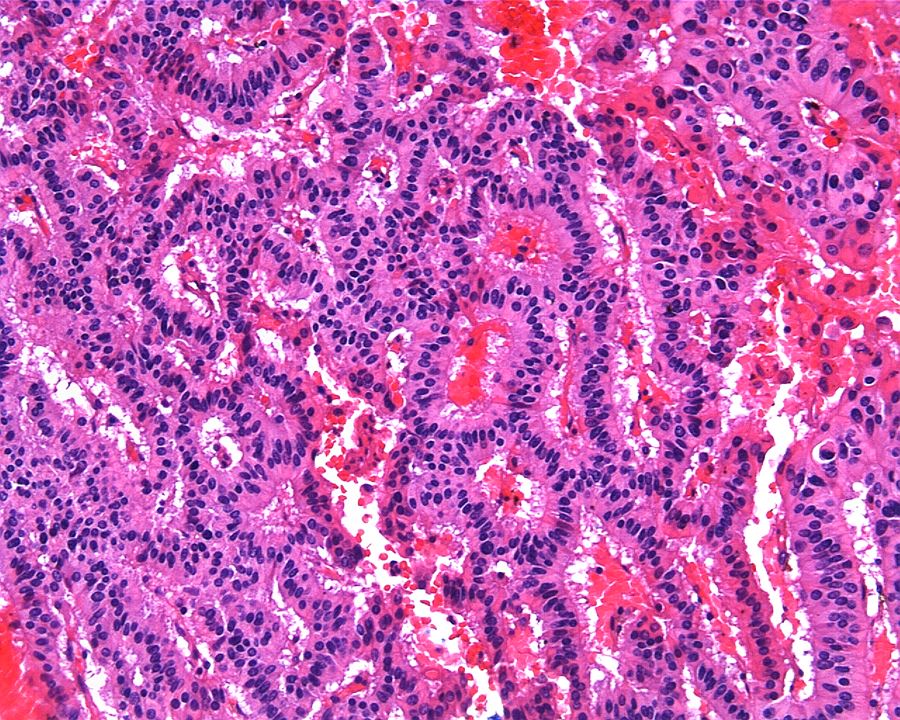
Gland-like lumina
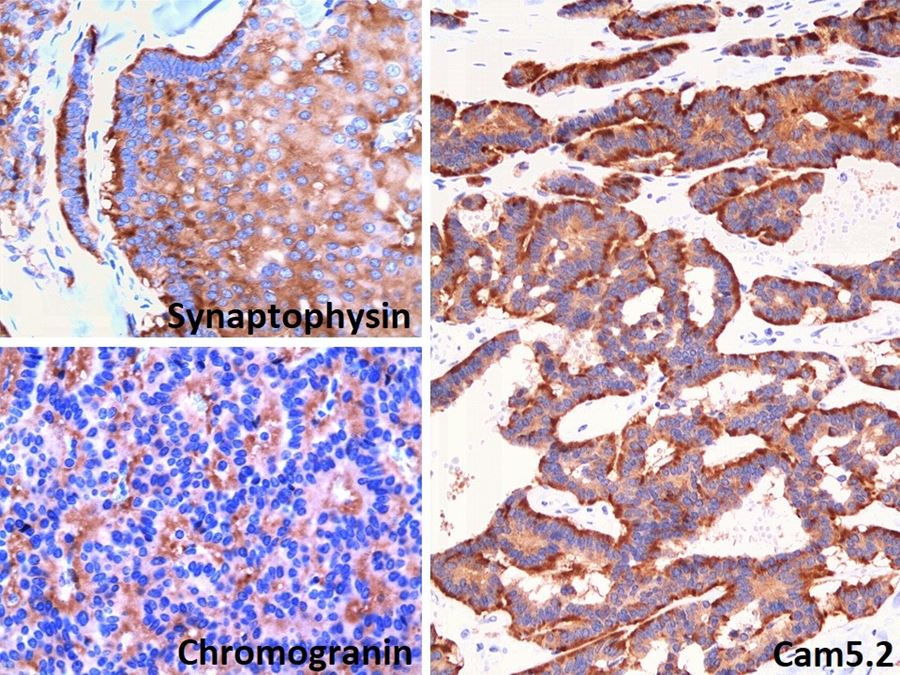
Synaptophysin, chromogranin, CAM5.2
Cytology description
- Tumor cells present singly; in clusters, may show pseudo glandular differentiation
- Monotonous cells with plasmacytoid appearance, oval to round nuclei, fine speckled chromatin (Diagn Cytopathol 2007;35:306, Radiol Case Rep 2015;1:108)
Cytology images
Images hosted on other servers:

Monotonous cells

Positive synaptophysin stain

Granular cytoplasm
Positive stains
- Cytokeratin markers: CK AE1 / AE3, CK8/18
- Neuroendocrine markers: synaptophysin (90%), chromogranin (65%), CD56 (3/6, 50%) (Am J Surg Pathol 2007;31:1539, Diagn Pathol 2019;14:12)
- Strong membranous CD99 immunoreactivity (8/9) (Hum Pathol 2011;42:1554)
Negative stains
- Renal transcription factors: PAX8 (9/9), PAX2 (9/9) (Hum Pathol 2011;42:1554)
- CK7 (17% positive), CK20 (6% positive) (Am J Surg Pathol 2007;31:1539)
- CDX2 (9/9), TTF1 (9/9) (Hum Pathol 2011;42:1554)
- GATA3 (Case Rep Pathol 2017;2017:9672368)
Electron microscopy description
- Presence of dense core neurosecretory granules
Electron microscopy images
Contributed by Jennifer Jeung, M.D. (Case #204)
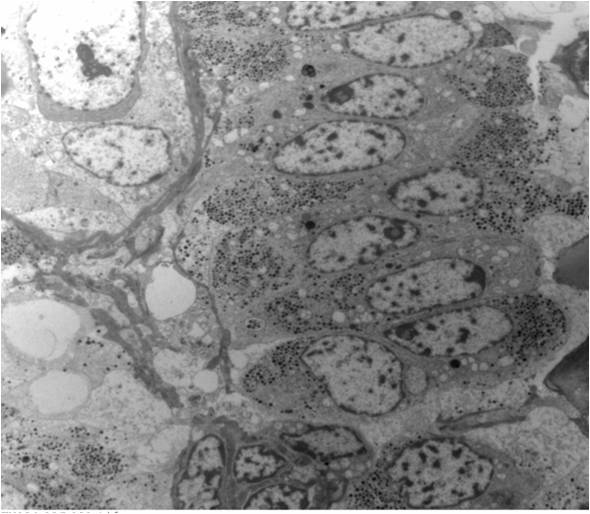
TEM of tumor cells

Prominent neurosecretory granules
Molecular / cytogenetics description
- Genetic alterations are variable and none of them are specific
- Most frequently observed genetic changes are mutations in CDH1 and TET2
- Reference: Histopathology 2019;75:104
Sample pathology report
- Right kidney, core biopsy:
- Well differentiated neuroendocrine tumor, likely renal primary (see comment)
- Comment: The tumor cells show nested growth pattern, with round to oval nuclei, stippled chromatin and eosinophilic granular cytoplasm. No mitosis or necrosis is seen. Immunohistochemistry studies show that the tumor cells are positive for CK AE1 / AE3, synaptophysin and chromogranin and negative for PAX8, TTF1, CDX2 and GATA3. The overall findings are consistent with a well differentiated neuroendocrine tumor. Given the radiographic finding of solitary renal mass and lack of clinical history of neuroendocrine tumors elsewhere, this tumor is most likely a renal primary.
Differential diagnosis
- Metastatic well differentiated neuroendocrine tumor:
- Paraganglioma:
- Zellballen / organoid growth pattern
- Sustentacular cells are positive for S100 and chief cells are positive for neuroendocrine markers
- Negative for cytokeratin and positive for GATA3 (Mod Pathol 2013;26:1365)
- Metanephric adenoma:
- Nested variants of urothelial carcinoma:
- Variable sized anastomosing nests with irregular projection into stroma
- Positive for CK7, CK20, GATA3 and uroplakin II
- High grade neuroendocrine tumor of kidney:
- High grade cytological atypia, necrosis is common; brisk mitotic activity and high Ki67 proliferative index
- Positive for cytokeratin and neuroendocrine markers
- Small cell carcinoma: high N/C ratios, hyperchromatic nuclei, nuclear molding
- Large cell carcinoma: large nuclei, abundant cytoplasm, prominent nucleoli
- Ewing sarcoma:
- Usually in children or young adults < 20 years old
- Small round blue cell tumor, CD99 positive
- Gene rearrangements involving FET and ETS families of genes (most commonly EWSR1-FLI1 gene rearrangement)
Additional references
Board review style question #1
A 45 year old man presented with hematuria. CT showed a well demarcated 3 cm left renal mass in the lower pole. Core biopsy was performed and the H&E slide is above. Immunostains show that the tumor cells are positive for CK8/18, synaptophysin and chromogranin and negative for PAX8, GATA3 and S100. What is the diagnosis of this tumor?
- Metanephric adenoma
- Nested variant of urothelial carcinoma
- Papillary renal cell carcinoma
- Paraganglioma
- Well differentiated neuroendocrine tumor
Board review style answer #1
E. Well differentiated neuroendocrine tumor
Comment Here
Reference: Well differentiated neuroendocrine tumor of kidney (carcinoid)
Comment Here
Reference: Well differentiated neuroendocrine tumor of kidney (carcinoid)
Board review style question #2
Which of the following immunostains is usually negative in well differentiated neuroendocrine tumor but positive in paraganglioma?
- CD56
- CD99
- Chromogranin
- GATA3
- Synaptophysin
Board review style answer #2
