

Kidney tumor
Other tumors
Metastases
Deputy Editor-in-Chief: Debra L. Zynger, M.D.


Last author update: 24 January 2022
Last staff update: 13 October 2023
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: "kidney metastases"
Table of Contents
Definition / general | Essential features | Epidemiology | Clinical features | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Molecular / cytogenetics description | Differential diagnosis | Board review style question #1 | Board review style answer #1Cite this page: Andeen NK, Tretiakova M. Metastases. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/kidneytumormalignantmetastases.html. Accessed April 20th, 2024.
Definition / general
- Malignant neoplasm metastatic to kidney, not of primary renal or renal pelvis origin
- Most are carcinomas (80.8%)
- Primary site (BJU Int 2016;117:775)
- Usually lung (43.7%)
- Colorectal (10.6%)
- ENT (6%)
- Breast (5.3%)
- Soft tissue (5.3%)
- Thyroid (5.3%)
- Primary site (BJU Int 2016;117:775)
- Also melanoma, pancreas, ovary, testis
Essential features
- In surgical pathology based studies, metastasis to kidney is uncommon; usually recognized after the diagnosis of primary tumor and may not be seen until long after that diagnosis
Epidemiology
- Epidemiology differs depending on type of cohort data analyzed (radiographic, autopsy or surgical pathology)
- Radiology study showed that the kidney was the 8th most common site of metastases from nonrenal primary malignancies (AJR Am J Roentgenol 2011;197:W680)
- Represents a small proportion of resected / biopsied renal masses (< 1% in one series) (Histopathology 2015;66:587)
- Mean age 56 - 61 years, M:F ratio = 1:1 (BJU Int 2016;117:775, Histopathology 2015;66:587)
Clinical features
- Presents with flank pain (30%), hematuria (16%) and weight loss (12%) (BJU Int 2016;117:775)
- Often solitary (77%), although most later develop more sites of metastasis (BJU Int 2016;117:775)
- 88% diagnosed after primary tumor, 9% concurrent with primary; in 2% the metastasis to kidney preceded diagnosis of primary tumor (Histopathology 2015;66:587)
- In 19%, there is a > 10 year interval between time of diagnosis of primary tumor and diagnosis of kidney metastasis (Histopathology 2015;66:587)
- 37% of patients have no other known metastasis at time of diagnosis (Histopathology 2015;66:587)
- Renal cell carcinoma is the most common recipient of tumor to tumor metastasis in malignant tumors (Urology 1987;30:35)
Radiology description
- Compared with renal primaries, more often solid and endophytic; no difference in tumor size, polar predominance or CT enhancement patterns (AJR Am J Roentgenol 2011;197:W680)
Radiology images
Images hosted on other servers:

Metastatic oral squamous cell carcinoma

Metastatic phyllodes tumor
Prognostic factors
- In a series of 151 patients with tumors metastatic to kidney, median overall survival from time of metastatic diagnosis was 1.1 years and median overall survival from primary tumor diagnosis was 3 years (BJU Int 2016;117:775)
Case reports
- 21 year old woman with osteosarcoma (Clin Genitourin Cancer 2008;6:124)
- 42 year old man with oral squamous cell carcinoma metastatic to kidney (J Clin Diagn Res 2015;9:TJ01)
- 53 year old woman with cervical metastasis resembling an abscess (Eur J Cancer Care (Engl) 2007;16:526)
- 53 year old and 75 year old men with lung and pancreatic tumors metastatic to angiomyolipoma (Arch Pathol Lab Med 2008;132:1016)
- 65 year old woman with lung adenocarcinoma metastatic to clear cell renal cell carcinoma (Arch Pathol Lab Med 2005;129:e49)
- Patient with breast adenoid cystic carcinoma metastatic to kidney (Hum Pathol 2007;38:1425)
- Parotid gland malignant mixed tumor with initial presentation as solitary kidney tumor (Am J Surg Pathol 2000;24:1159)
Treatment
- May be treated with ablation or resection
Gross description
- 30% multiple
- 23% bilateral
- 69% located in cortex (Histopathology 2015;66:587)
Gross images
Contributed by Debra Zynger, M.D.

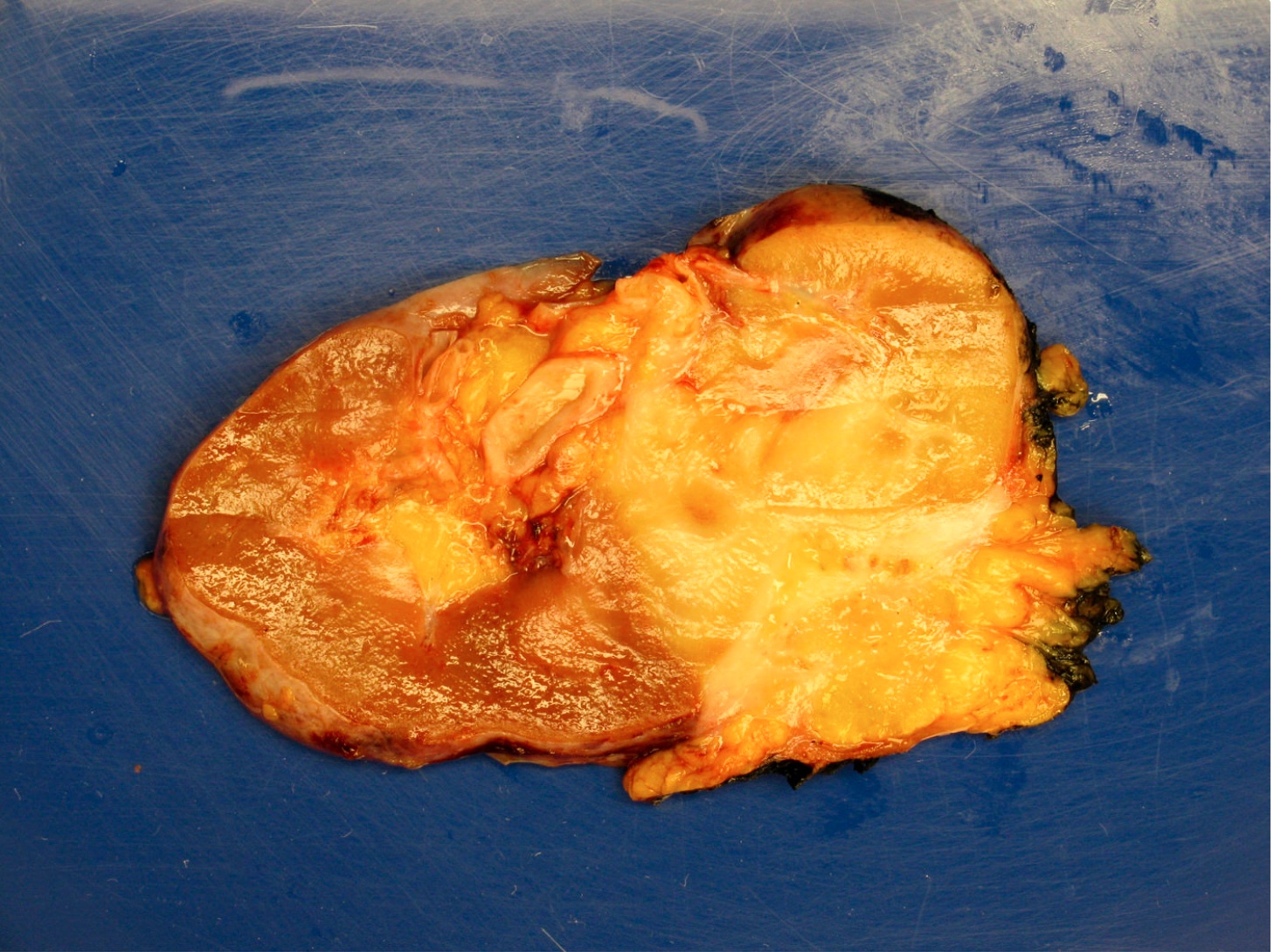
Lung squamous cell carcinoma
Images hosted on other servers:

Myeloma

Small cell lung cancer

Solitary fibrous tumor
Microscopic (histologic) description
- Varies; may mimic urothelial carcinoma with divergent differentiation or unusual primary kidney tumors
Microscopic (histologic) images
Contributed by Maria Tretiakova, M.D., Ph.D., Nicole K. Andeen, M.D.

Breast carcinoma
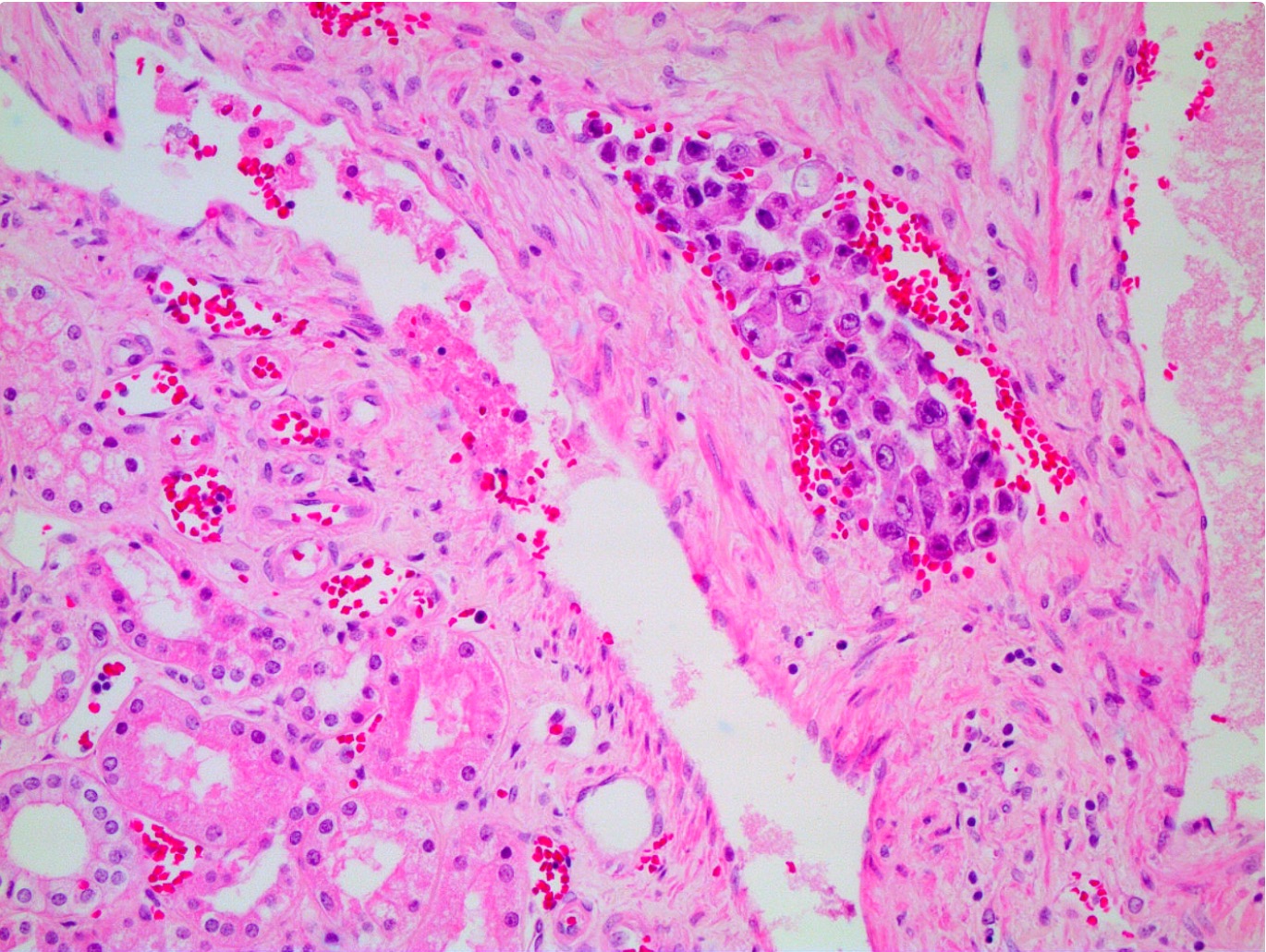
Gastric carcinoma

Well differentiated neuroendocrine tumor
Cytology description
- Uncommon to diagnose kidney metastases via cytology (Anal Quant Cytopathol Histpathol 2014;36:345, Nayar: Cytopathology in Oncology, 2013 )
Positive stains
- Other primaries: TTF1, CDX2, GATA3, ER, SF1, calretinin, inhibin, OCT 3 / 4, SALL4, synaptophysin, chromogranin (Adv Anat Pathol 2010;17:377)
Negative stains
- Renal cell carcinoma markers: PAX8 (83% of renal cell carcinomas are positive), EMA (78% of clear cell renal cell carcinomas are positive), CAIX (87% of clear cell renal cell carcinoma are positive), hKIM-1 (human kidney injury molecule-1) (83% of clear cell renal cell carcinoma are positive), PAX2, renal cell carcinoma (Am J Surg Pathol 2011;35:678)
Molecular / cytogenetics description
- Molecular testing not currently used consistently; diagnosis is based on history, morphology and IHC
Differential diagnosis
- Depends on metastasis type; H&E and clinical history are best discriminators
- Adrenal cortical carcinoma: SF1 (86% adrenal vs. 0% clear cell renal cell carcinoma (RCC) positive), calretinin (89% adrenal vs. 10% clear cell RCC positive), inhibin (86% adrenal vs. 9% clear cell RCC positive), MelanA (86% adrenal vs. 10% RCC positive) (Am J Surg Pathol 2011;35:678)
- Metastatic carcinoid: nested and insular growth pattern, positive for synaptophysin and chromogranin
- Type 1 papillary renal cell carcinoma: has true fibrovascular cores, foamy macrophages, negative for neuroendocrine markers
- Renal cell carcinoma: usually express PAX8 (83% RCC positive) and CAIX (87% clear cell RCC positive) (Am J Surg Pathol 2011;35:678)
- Urothelial carcinoma: based in renal pelvis, positive for p63, uroplakin, CK20 (variable expression in other metastatic diagnostic considerations)
Board review style question #1
Which is the most useful immunohistochemical panel to differentiate adrenal cortical carcinoma from clear cell renal cell carcinoma?
- Inhibin, calretinin, CD10, PAX2
- MelanA, CK7, RCC, PAX2
- SF1, calretinin, CAIX, PAX8
- SF1, CK7, RCC, CD10
Board review style answer #1
