Kidney tumor
Renal cell tumors - benign / indolent
Oncocytoma
Author: Rola Saleeb, M.D., Ph.D.
Editorial Board Member: Maria Tretiakova, M.D., Ph.D.
Editor-in-Chief: Debra L. Zynger, M.D.

Last author update: 21 September 2020
Last staff update: 26 August 2025 (update in progress)
Copyright: 2003-2025, PathologyOutlines.com, Inc.
PubMed Search: Oncocytoma
Table of Contents
Definition / general | Essential features | Epidemiology | Sites | Pathophysiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Cytology images | Positive stains | Negative stains | IHC panels | Electron microscopy description | Electron microscopy images | Molecular / cytogenetics description | Molecular / cytogenetics images | Sample pathology report | Differential diagnosis | Practice question #1 | Practice answer #1 | Practice question #2 | Practice answer #2Cite this page: Saleeb R. Oncocytoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/kidneytumoroncocytoma.html. Accessed September 16th, 2025.
Definition / general
- Benign renal epithelial neoplasms characterized by large round eosinophilic cells packed with mitochondria
Essential features
- Renal oncocytoma are benign renal oncocytic neoplasms
- Cells are packed with mitochondria under electron microscopy
- Essential to differentiate from mimicker oncocytic renal cell carcinoma entities
- Multiple tumors can be associated with syndromic conditions
- Some cases have hybrid morphologies: hybrid oncocytic / chromophobe renal cell carcinoma (HOCT); these are described in syndromic settings but can also be encountered as sporadic cases
Epidemiology
- 5 - 9% of renal tumors
- M:F = 2:1
- Age range is very broad: 24 - 91 years old; mean age is in the 60s (Am J Surg Pathol 1997;21:1, J Kidney Cancer VHL 2017;4:1)
- Rarely associated with renal oncocytosis; these kidneys develop multiple oncocytic lesions, oncocytomas, chromophobe tumors and tumors with hybrid oncocytic / chromophobe morphology (HOCT); these are believed to be associated with Birt-Hogg-Dubé syndrome (Mod Pathol 2019;32:1698)
Sites
- Renal cortex
Pathophysiology
- Benign neoplasms are believed to arise from renal intercalated cells and are packed with respiration defective mitochondria
- Often possess pathogenic mitochondrial mutations; it is suggested that the defective mitochondria activates a metabolic checkpoint leading to autophagy impairment and mitochondrial accumulation and that this acts as tumor suppressive mechanism limiting tumor progression (Cell Rep 2015;13:1895)
- 2 main molecular variant events associated with oncocytomas: rearrangements of CCDN1 (11q13 translocations) or aneuploidy manifested mostly in losses of chromosome Y and 1
- Also suggested that in some oncocytomas (the ones that harbor aneuploidy losses of chromosome 1 and Y), additional p53 mutations may allow for progression to eosinophilic chromophobe renal cell carcinoma (Cell Rep 2015;13:1895)
Clinical features
- Benign
- Usually asymptomatic; detected incidentally on imaging for unrelated reasons
- Rarely presents with hematuria and dysuria
Diagnosis
- Diagnosis is made with the combination tissue histologic morphology and immunohistochemical profile, which should be consistent with indolent clinical behavior and a circumscribed mass lesion
Radiology description
- No specific radiologic findings
- Diagnosis may be suggested by the presence of a central stellate scar on CT, MRI or US; however, this feature is not specific and can be present in any slow growing renal tumor
Radiology images
AFIP images
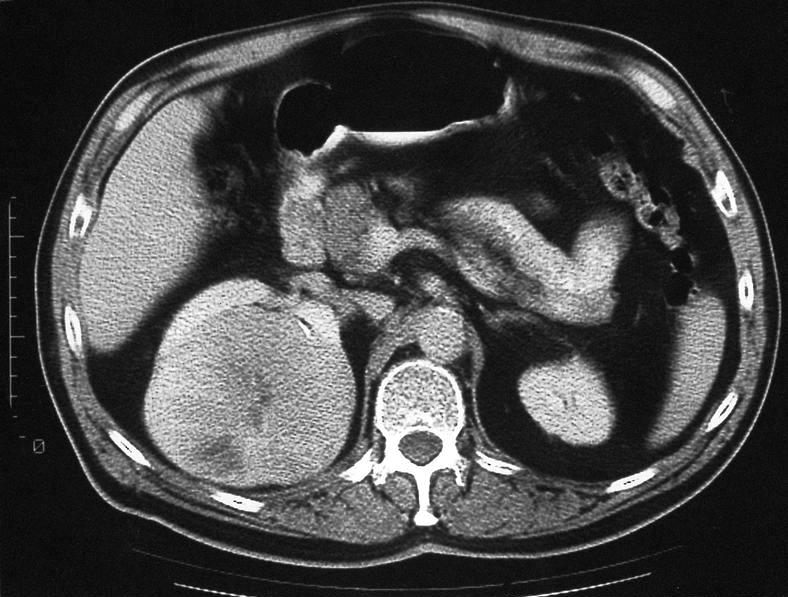
Renal oncocytoma
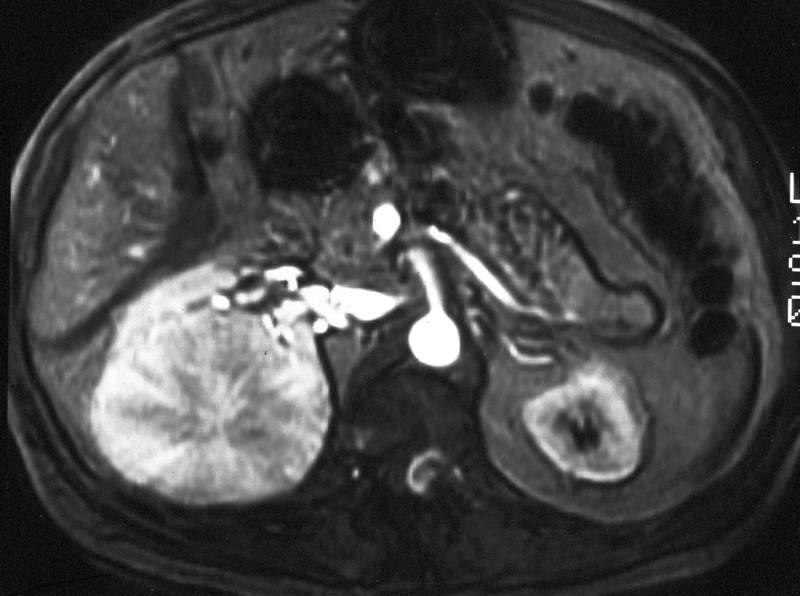
MRI shows same tumor with prominent central scar
Prognostic factors
- Benign tumor
- There are literature suggestions that it can potentially accumulate genetic abnormalities and progress to a chromophobe renal cell carcinoma (Cell Rep 2015;13:1895)
Case reports
- 25 year old woman presenting with a giant renal oncocytoma (J Med Case Rep 2010;4:52)
- 44 year old man presenting with a collision tumor, papillary renal cell carcinoma type 1 and oncocytoma (Pathologica 2019;111:37)
- 48 year old woman presenting with renal hybrid oncococytic / chromophobe tumor and multiple schwanommas (Medicine (Baltimore) 2017;96:e8939)
- 69 year old man with oncocytoma with invasive histopathological features (Klin Onkol 2014;27:138)
Treatment
- Clinical follow up / surveillance or excision / ablation
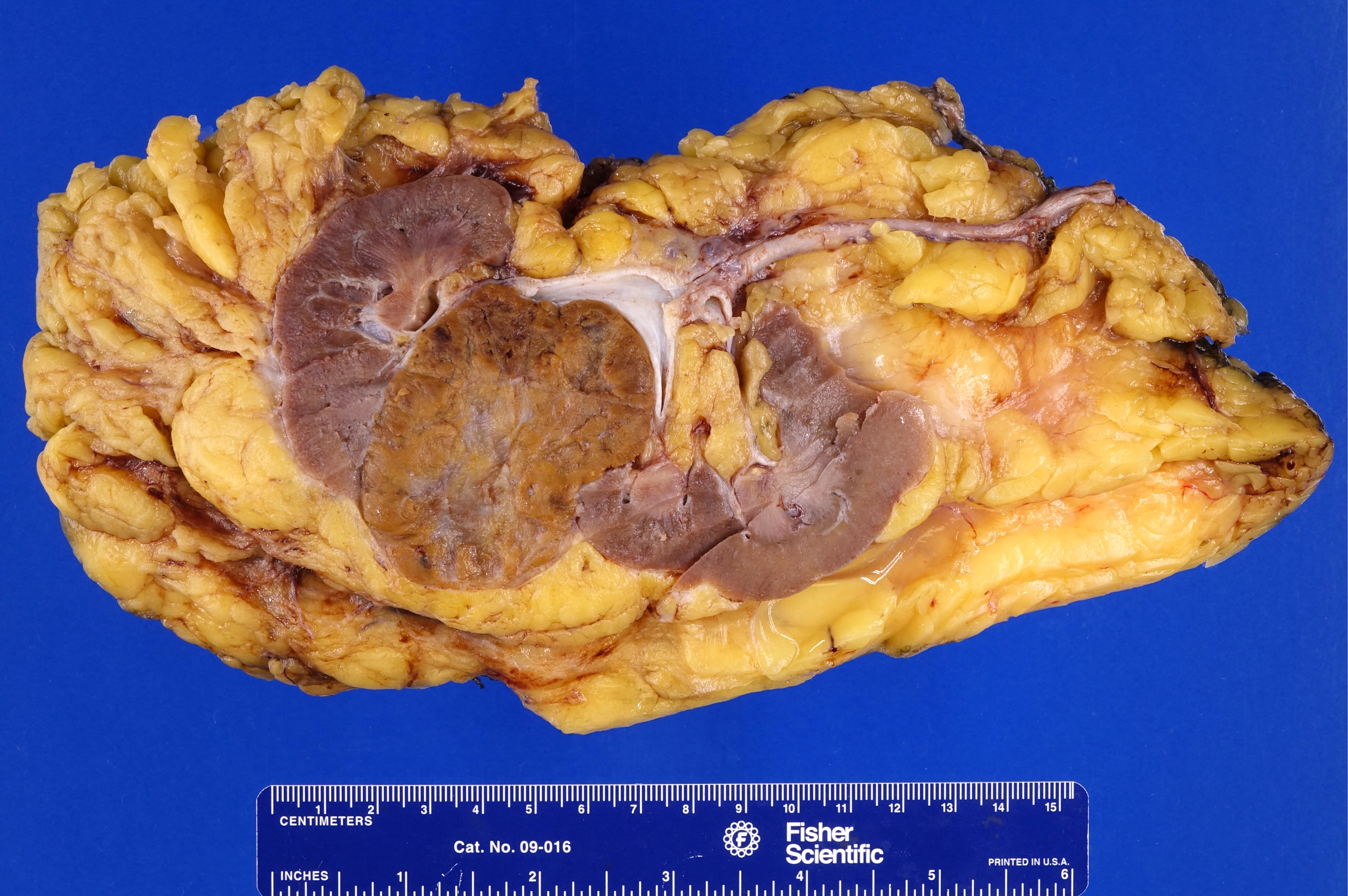
Gross description
- Well circumscribed mass (J Kidney Cancer VHL 2017;4:1, Mod Pathol 2019;32:1698, Am J Surg Pathol 1997;21:1)
- Mass present in the cortex but large masses can extend into and expand the perinephric fat, sinus fat or even the renal vein (Am J Surg Pathol 1997;21:1, Cesk Patol 2001;37:51)
- Mahogany brown cut surface to tan or yellow
- Central stellate scar commonly present; might be in an eccentric location
- Hemorrhage might be present but should not show necrosis
Gross images
Contributed by Debra Zynger, M.D.
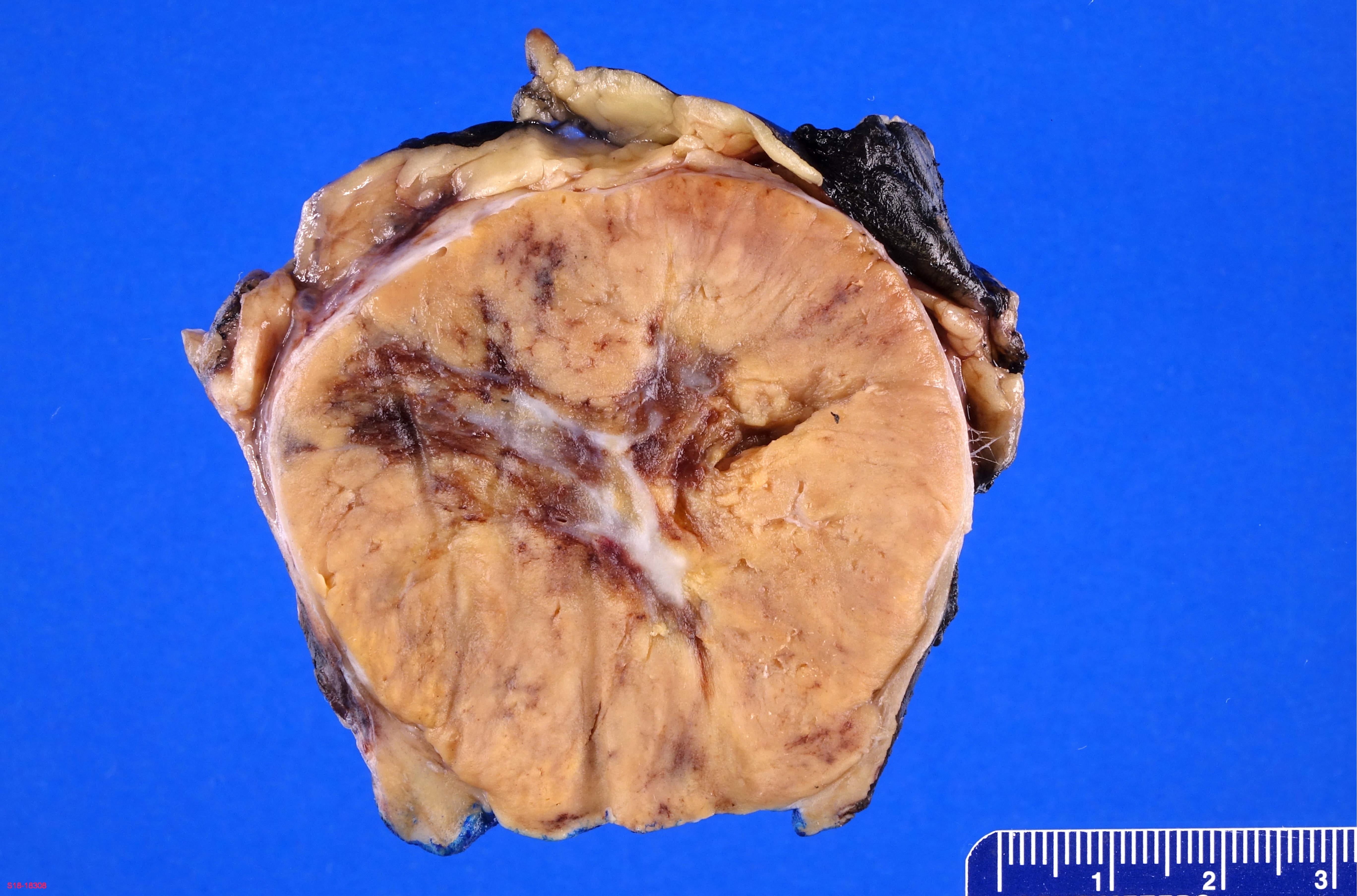
Tan, central scar

Pale brown, central scar
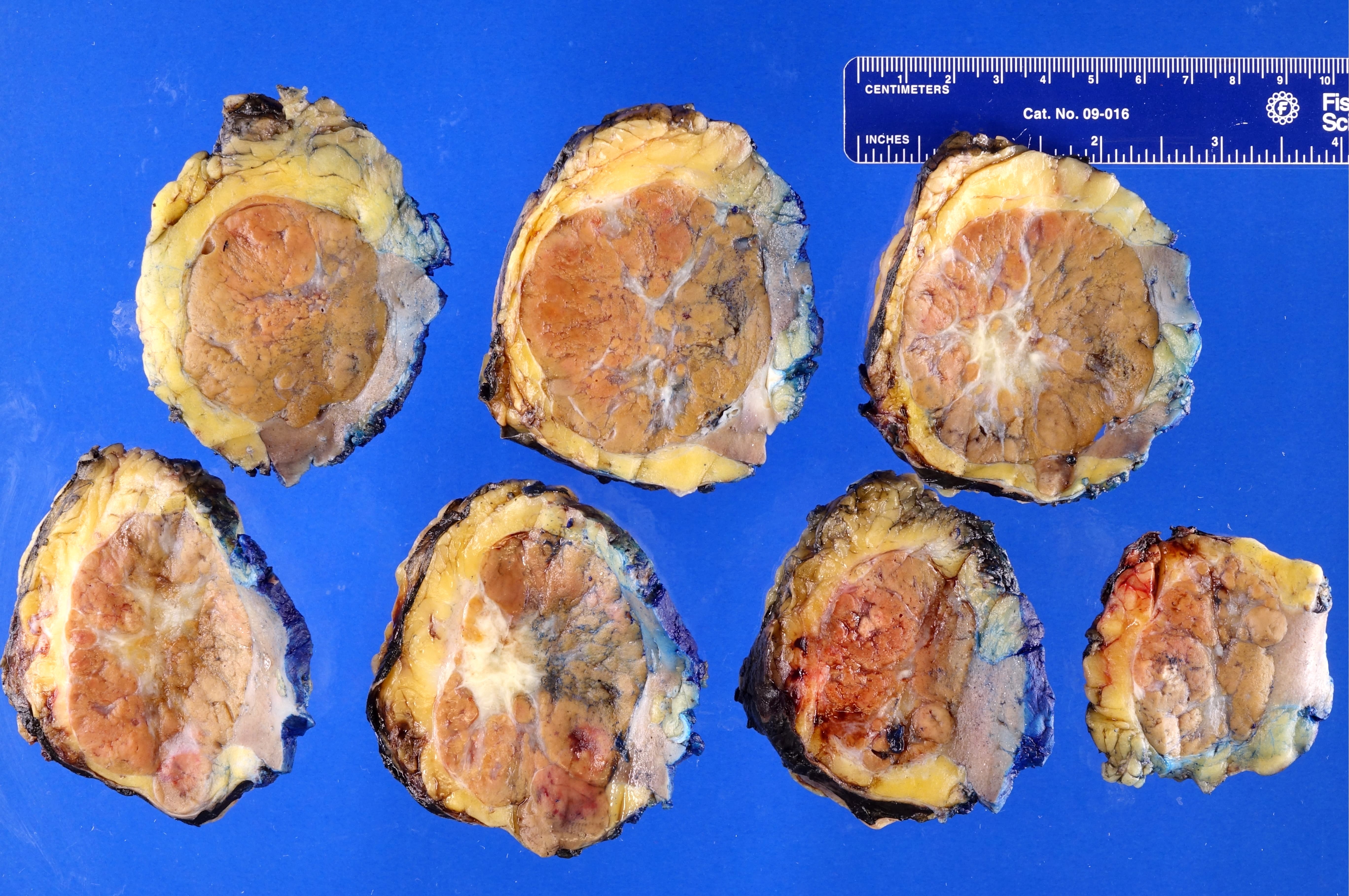
Pale brown, central scar
Mahogany

Congested, dark brown

Hemorrhagic, red
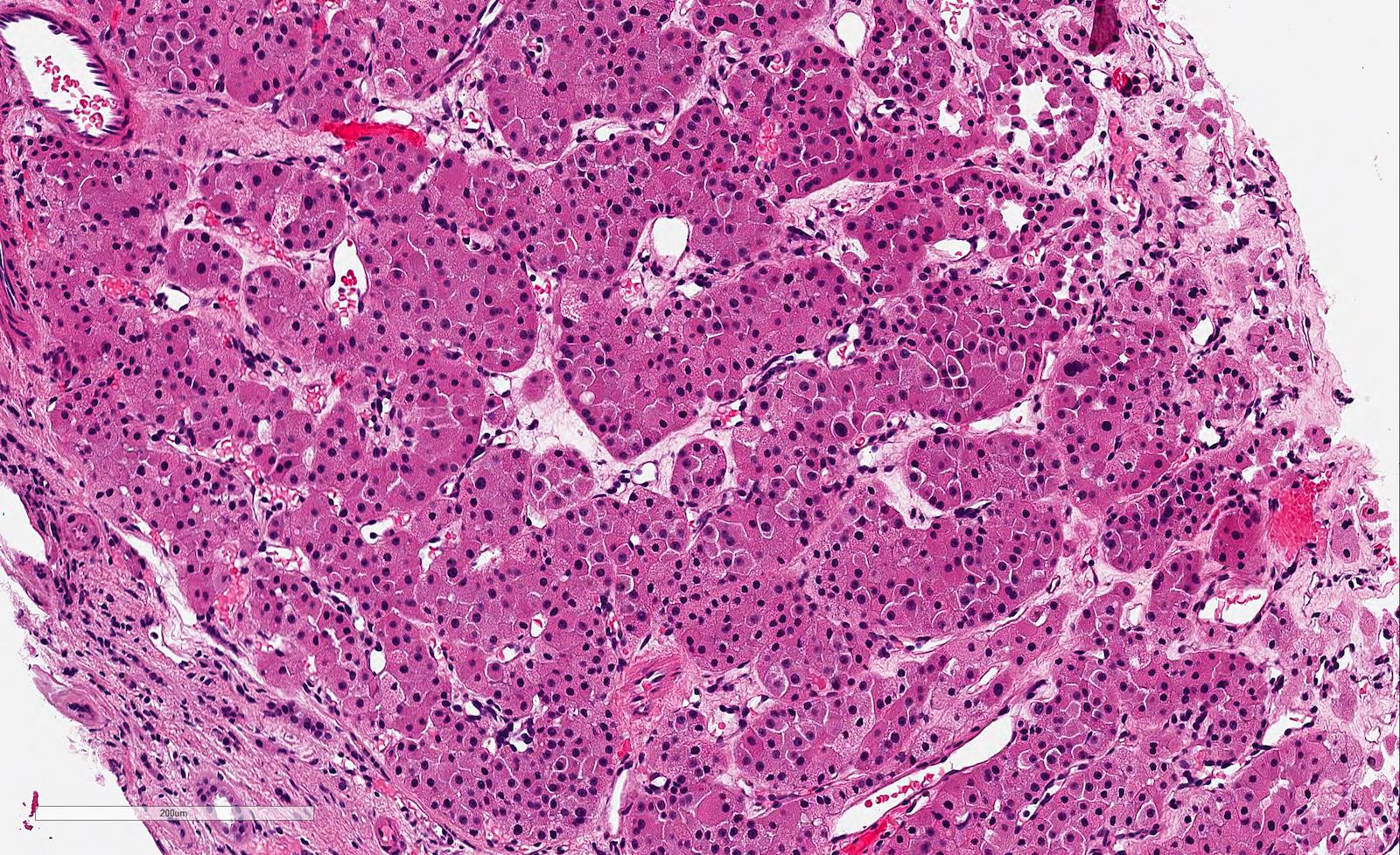
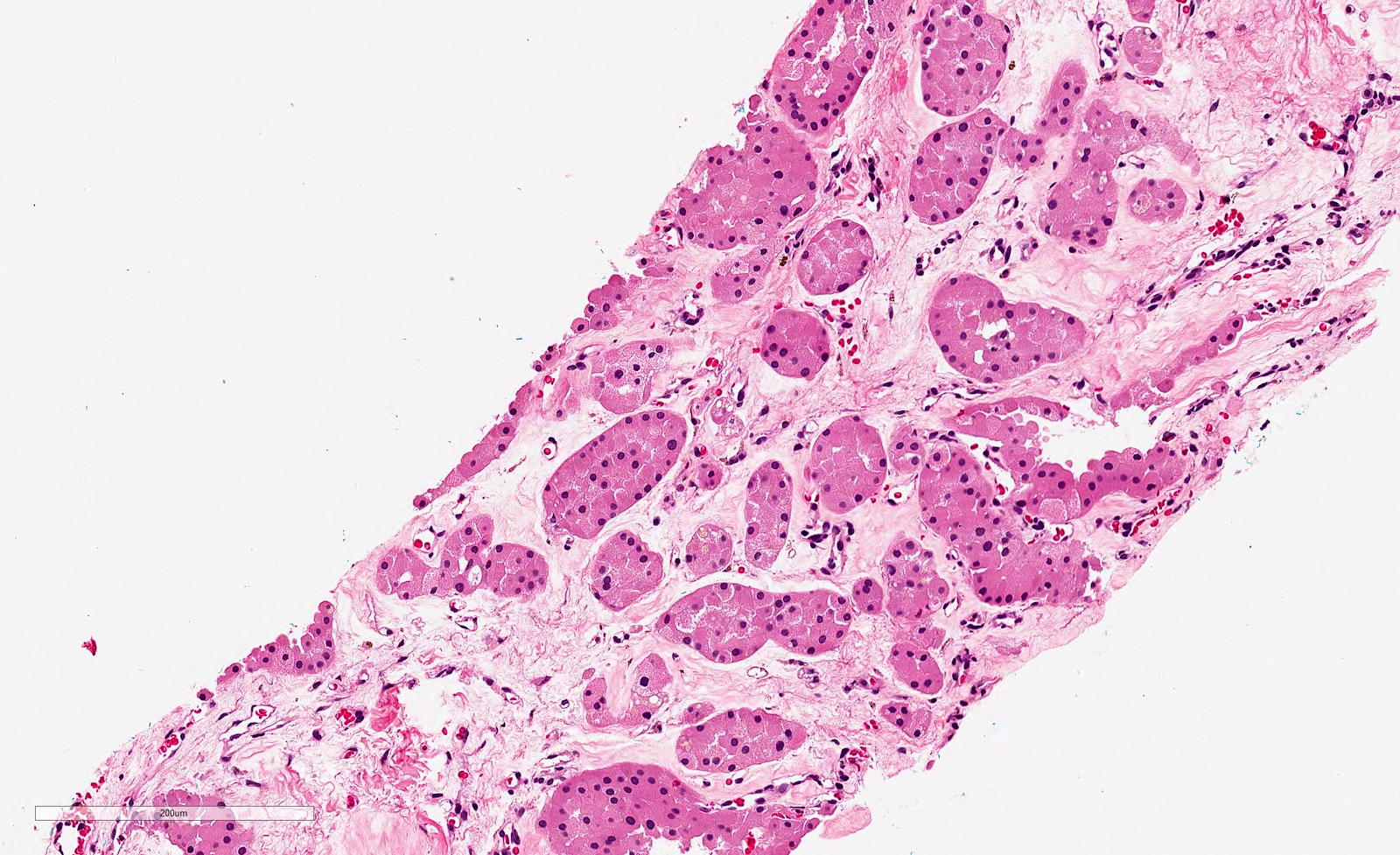
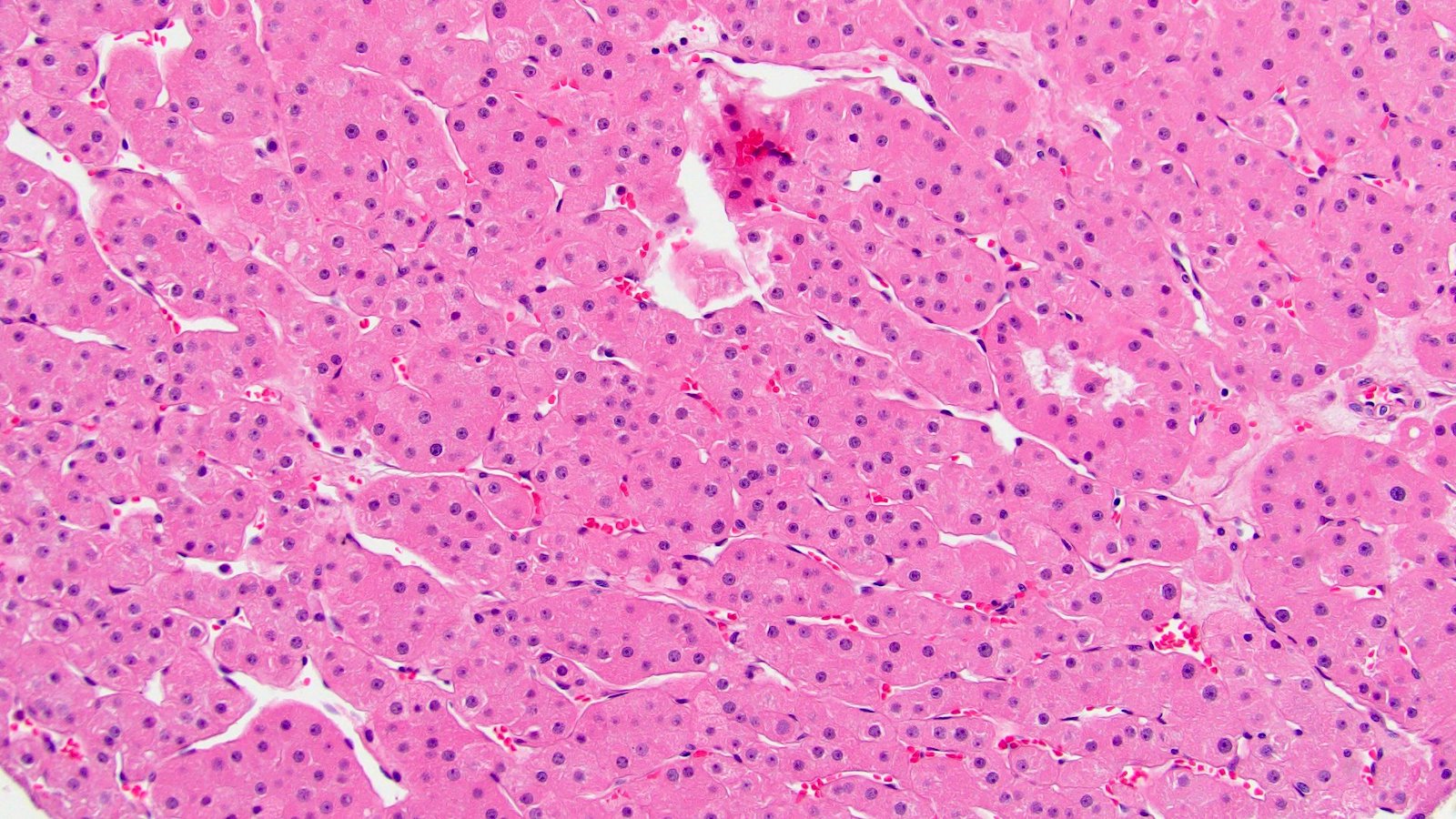
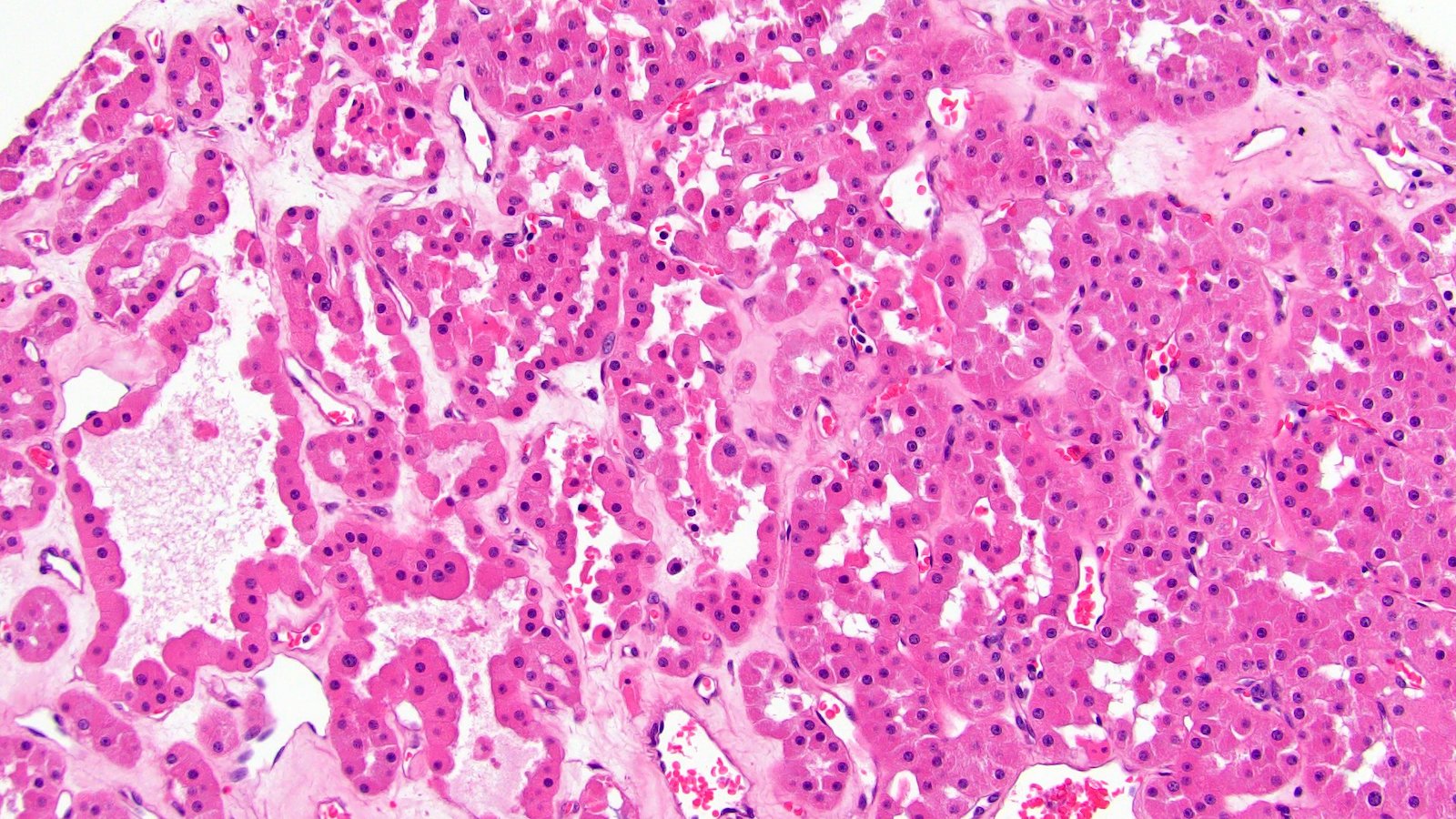
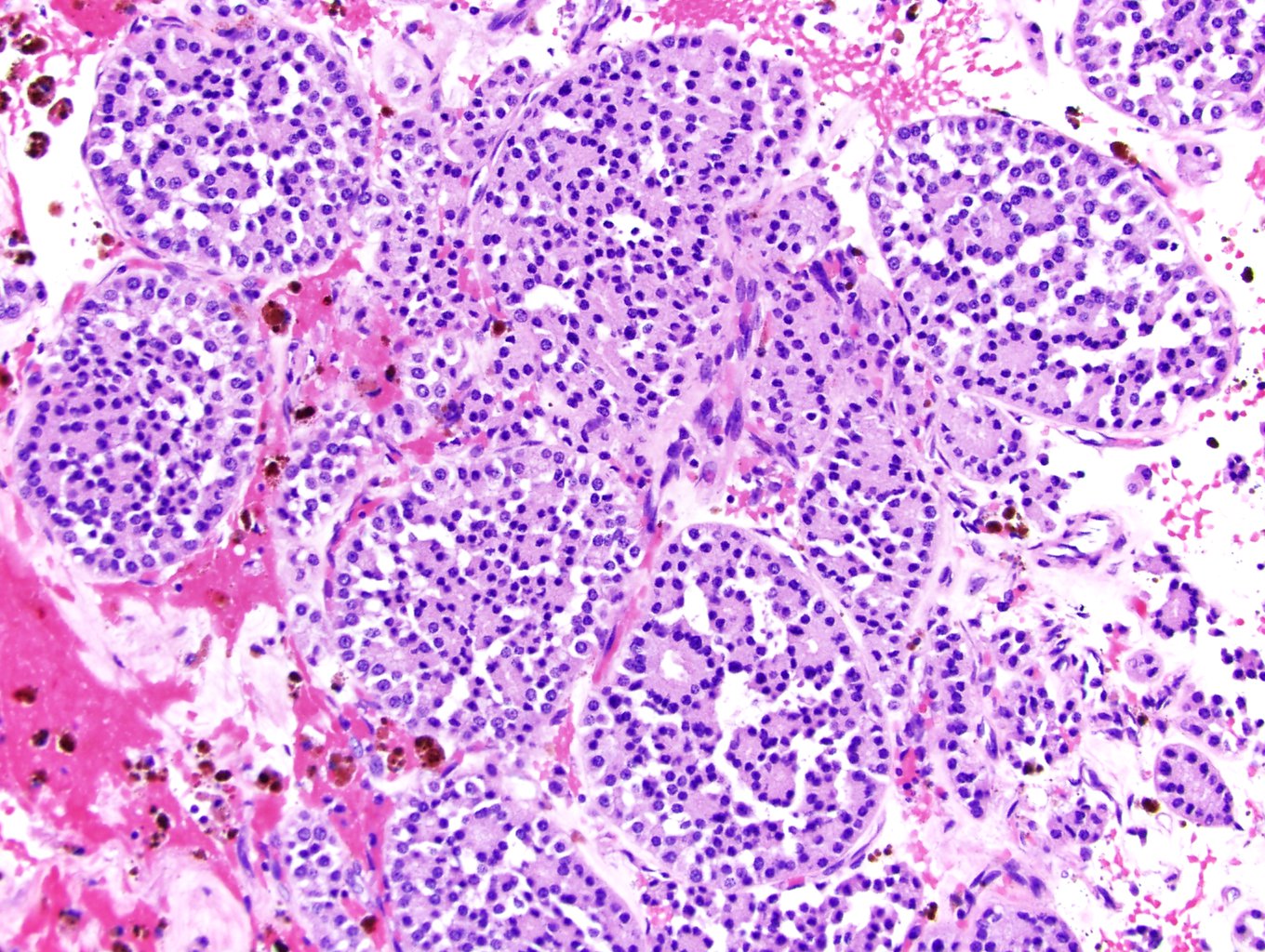
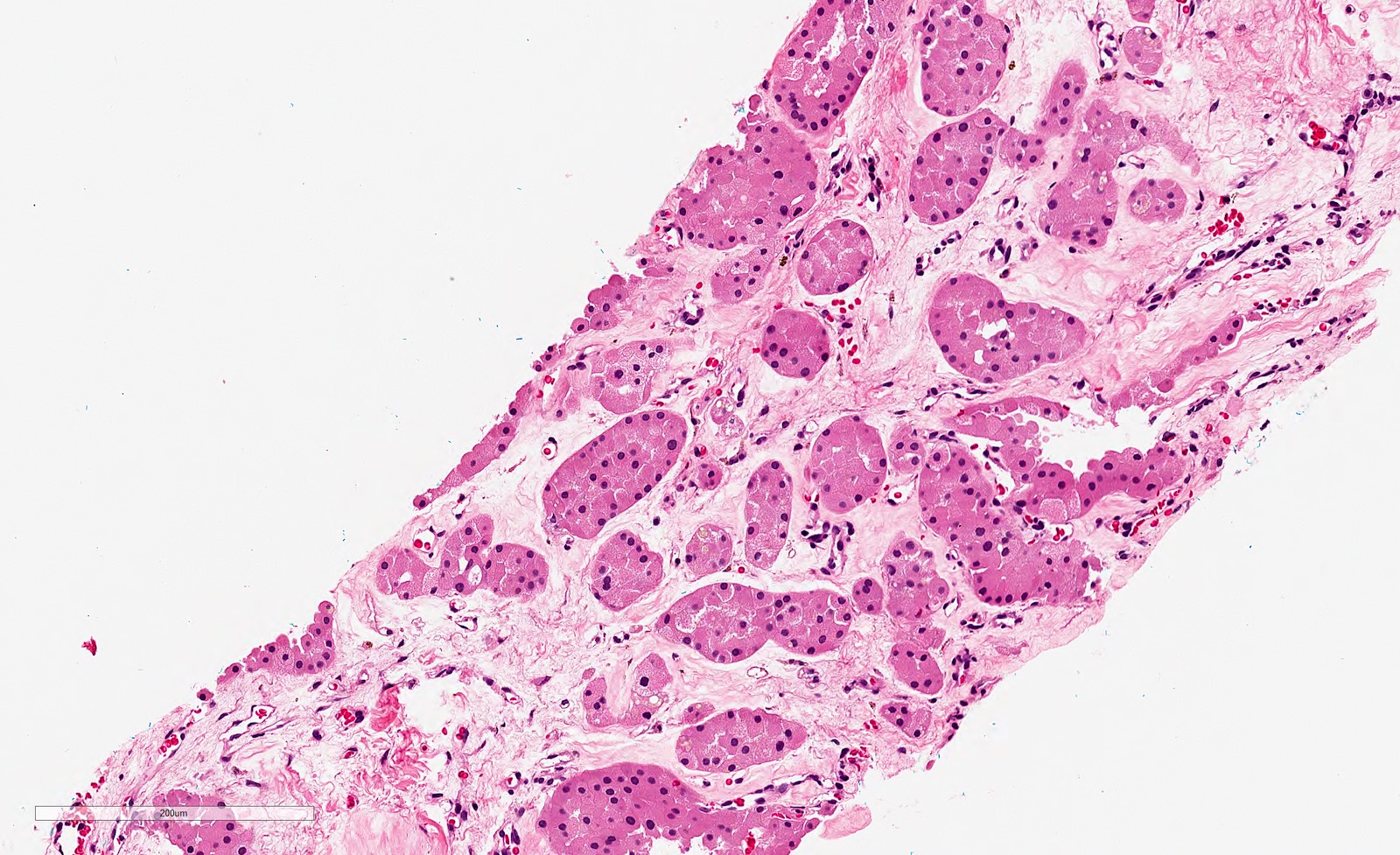
Microscopic (histologic) description
- Well circumscribed lesion; usually no pseudocapsule, tumor directly abuts the renal parenchyma (Am J Surg Pathol 1997;21:1, J Kidney Cancer VHL 2017;4:1)
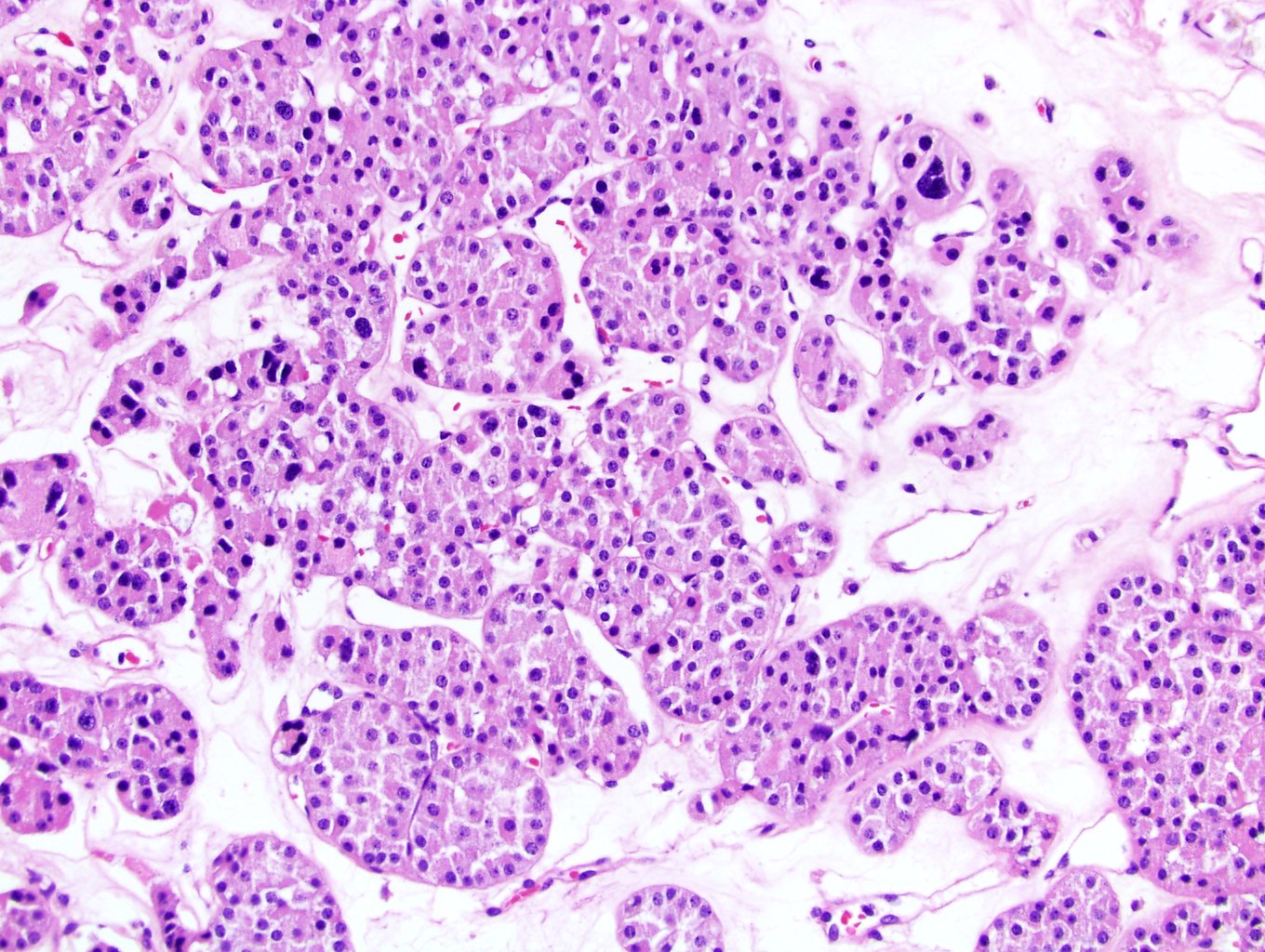
- Architecture is variable: typically small solid nests in a loose connective tissue (edematous looking) stroma
- Other architectures include tubular, micro and macrocystic, packed nests projecting a solid appearance (Am J Surg Pathol 1997;21:1, Cesk Patol 2001;37:51)
- Archipelagenous / trabecular architecture has been described; however, the newly described low grade oncocytic tumor comes in the differential with that pattern (Histopathology 2019;75:174)
- Should not have a papillary architecture; more than focal intracystic papillations is not compatible with the diagnosis of oncocytoma
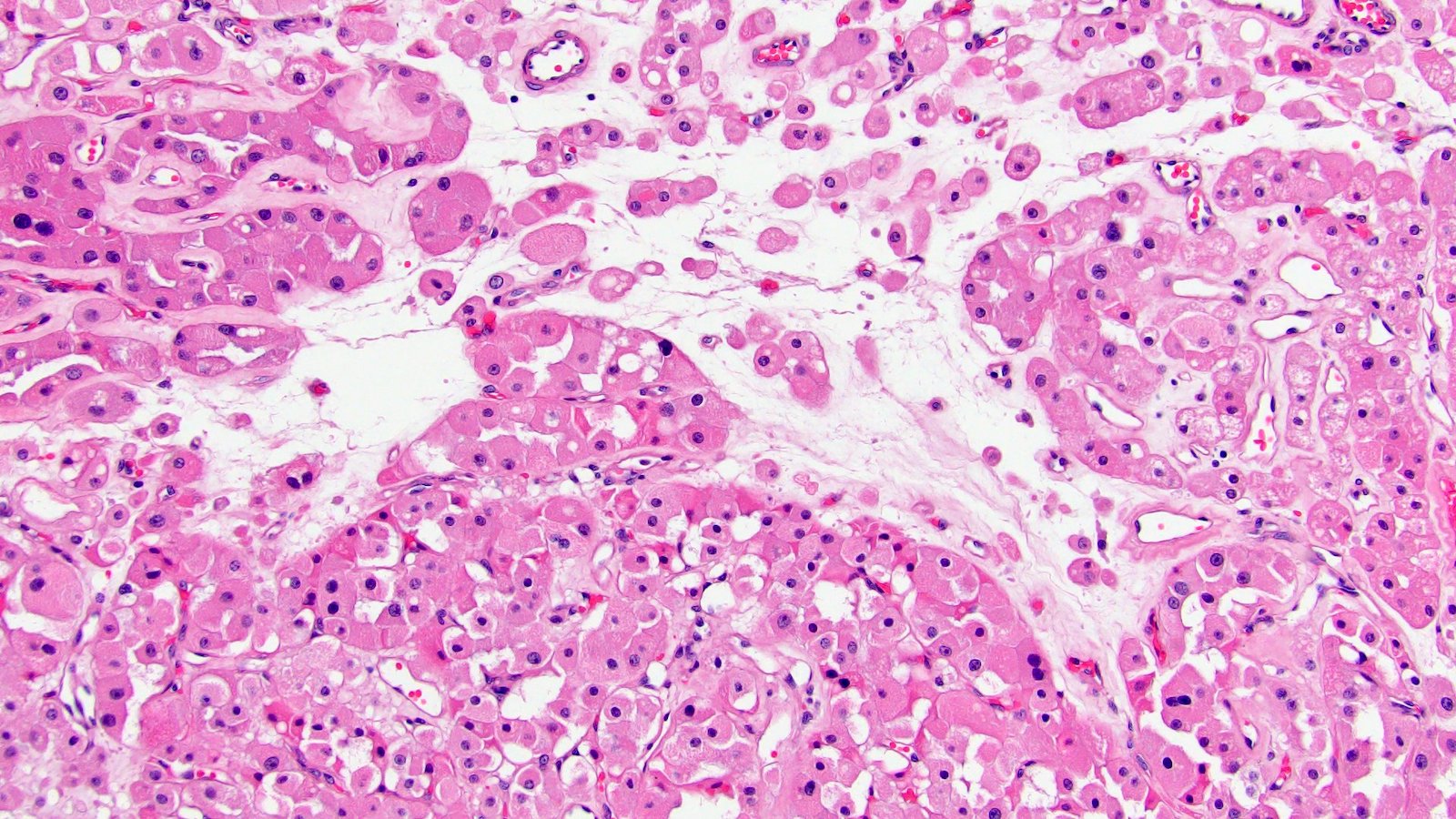
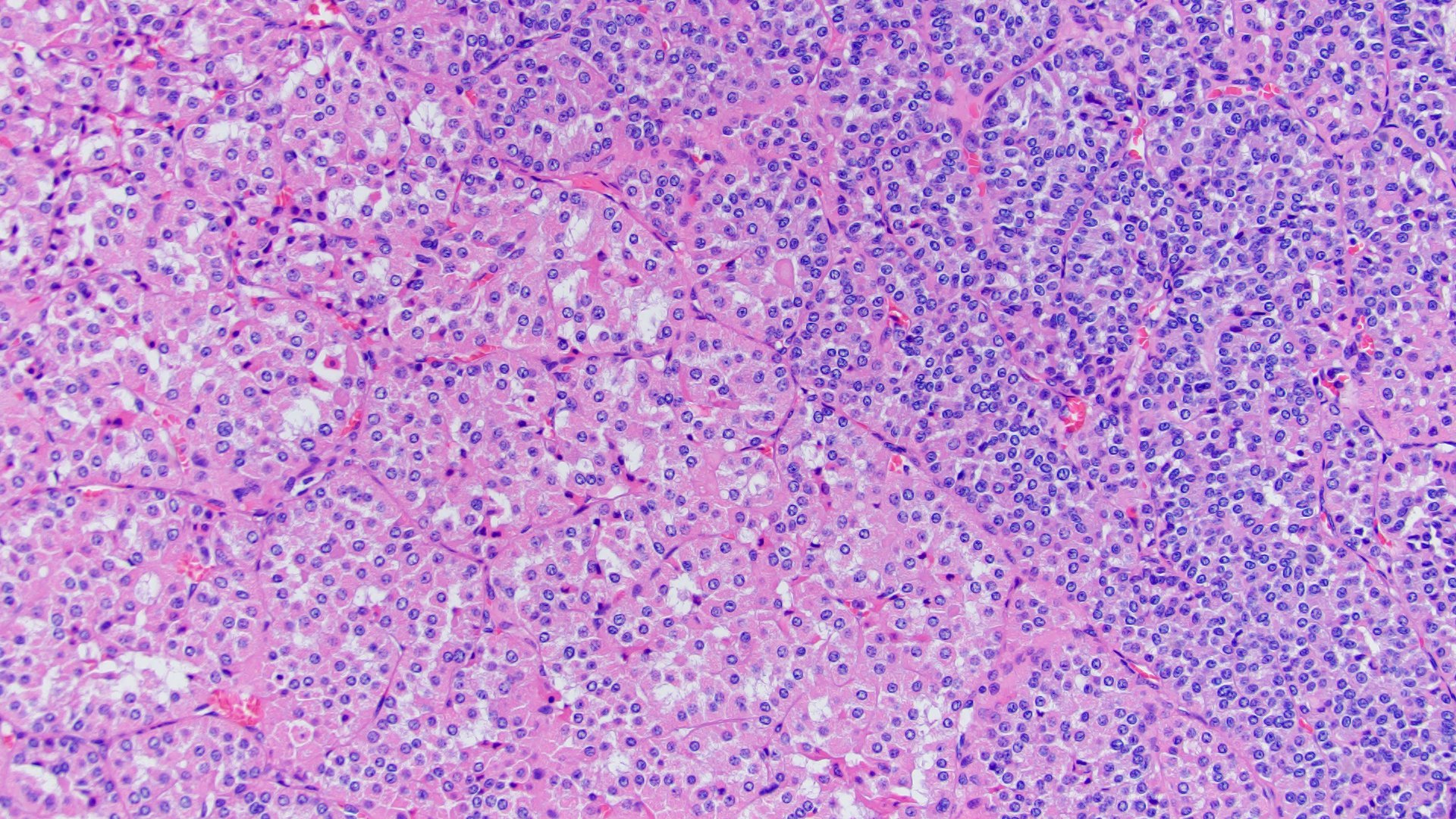
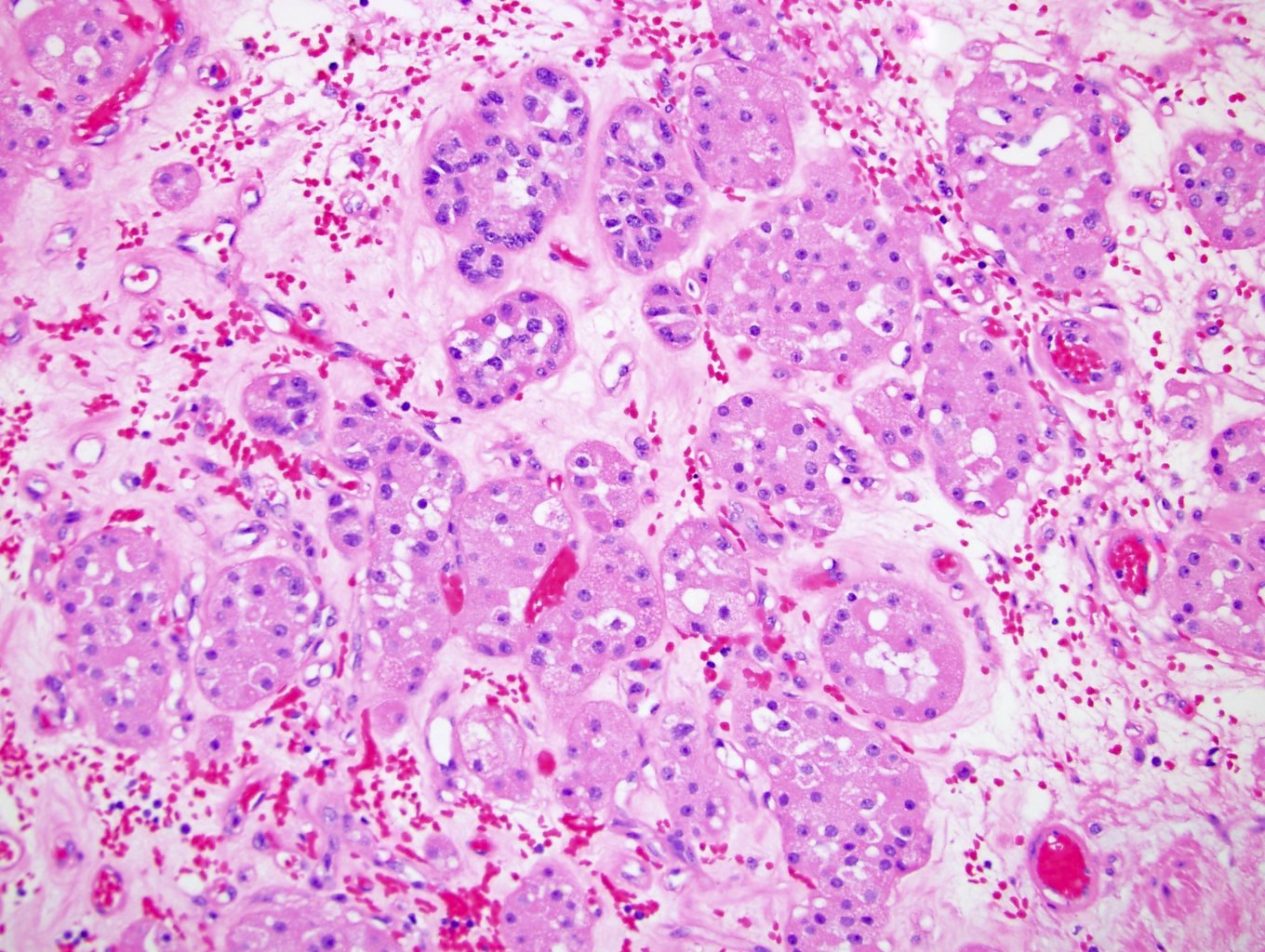
- Composed of large round eosinophilic cells (oncocytes) with dense granular cytoplasm; nuclei are round and regular with even chromatin; small but conspicuous nucleoli are present
- Bizarre pleomorphic hyperchromatic cells are commonly present and are thought to be degenerative in nature
- Population of small cells (oncoblasts) has been occasionally described at the edge of the scar or nests
- Mitotic figures are rare with no atypical mitosis
- Hemorrhage can be present but no coagulative necrosis
- Rarely have foci of dystrophic calcifications
- Cytoplasmic clearing can be identified around scar areas
- Some show perinephric fat or vascular invasion; this does not change the diagnosis of a benign oncocytoma
- Renal oncocytosis
- Rare conditions where kidneys can have numerous oncocytic lesions; the background kidney shows clusters of oncocytic cells lining benign tubules, cysts and can also be present within renal interstitium (Histol Histopathol 2012;27:1407)
- Chromophobe renal cell carcinoma and hybrid oncocytic tumors may also be present in the background of oncocytosis (Histol Histopathol 2003;18:935)
- Believed to be related to Birt-Hogg-Dubé syndrome
Microscopic (histologic) images
Contributed by Rola Saleeb, M.D., Ph.D.

Small nested morphology
Degenerated cells
Loose stroma

c-KIT

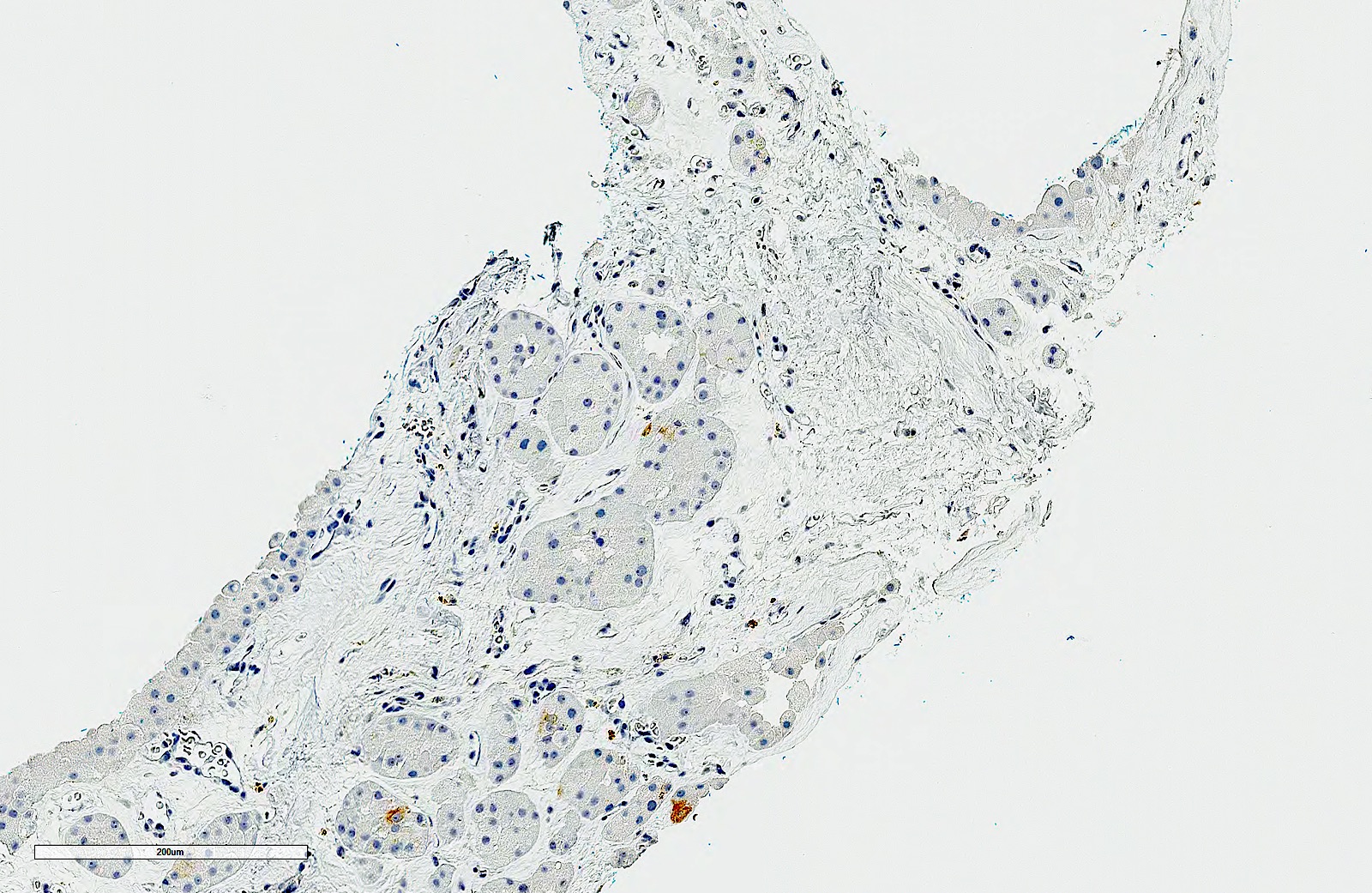
CK7
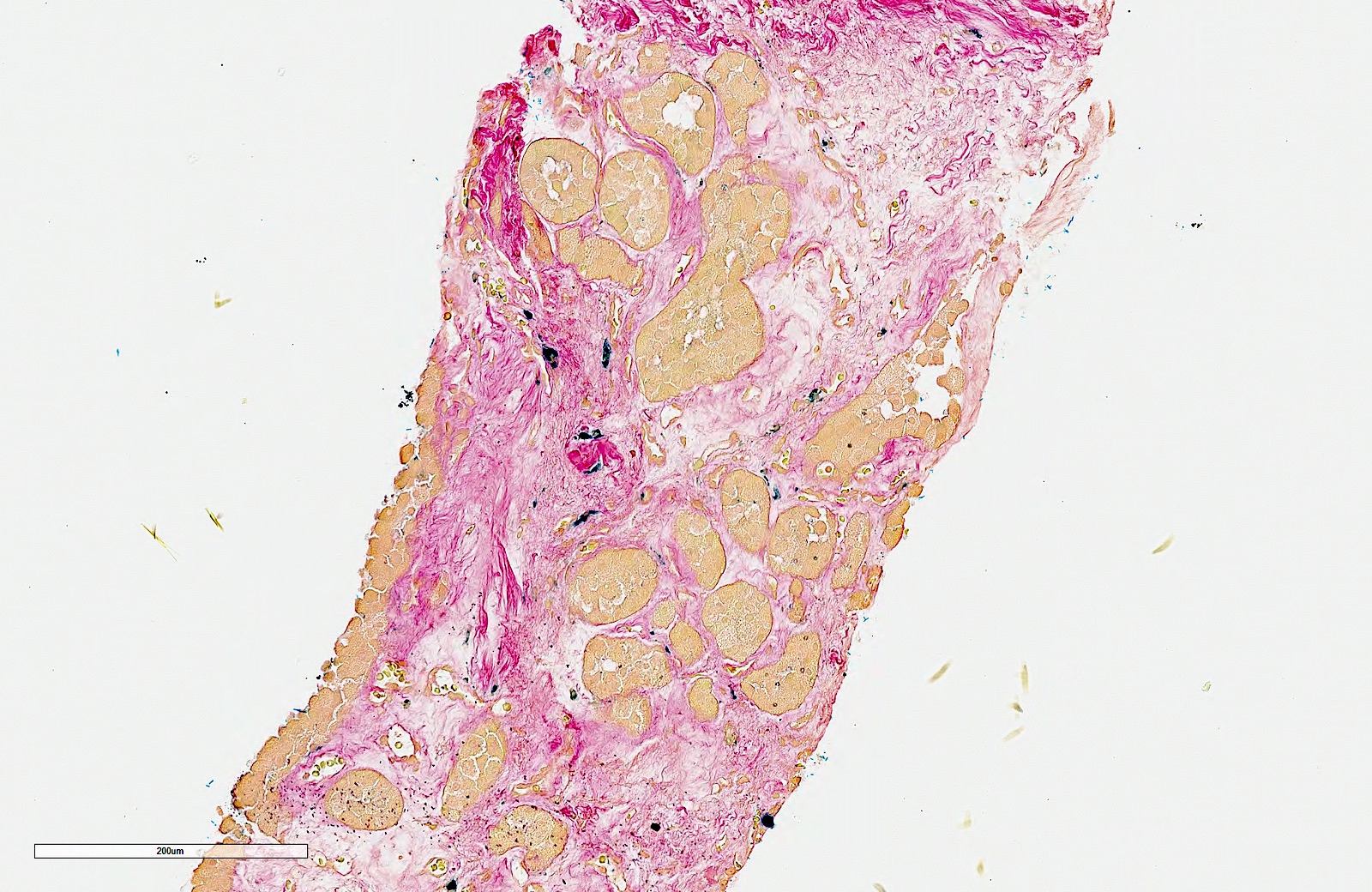
Hale colloidal iron
Contributed by Maria Tretiakova, M.D., Ph.D.
Compact, nested
Central scar
Nested, cystic
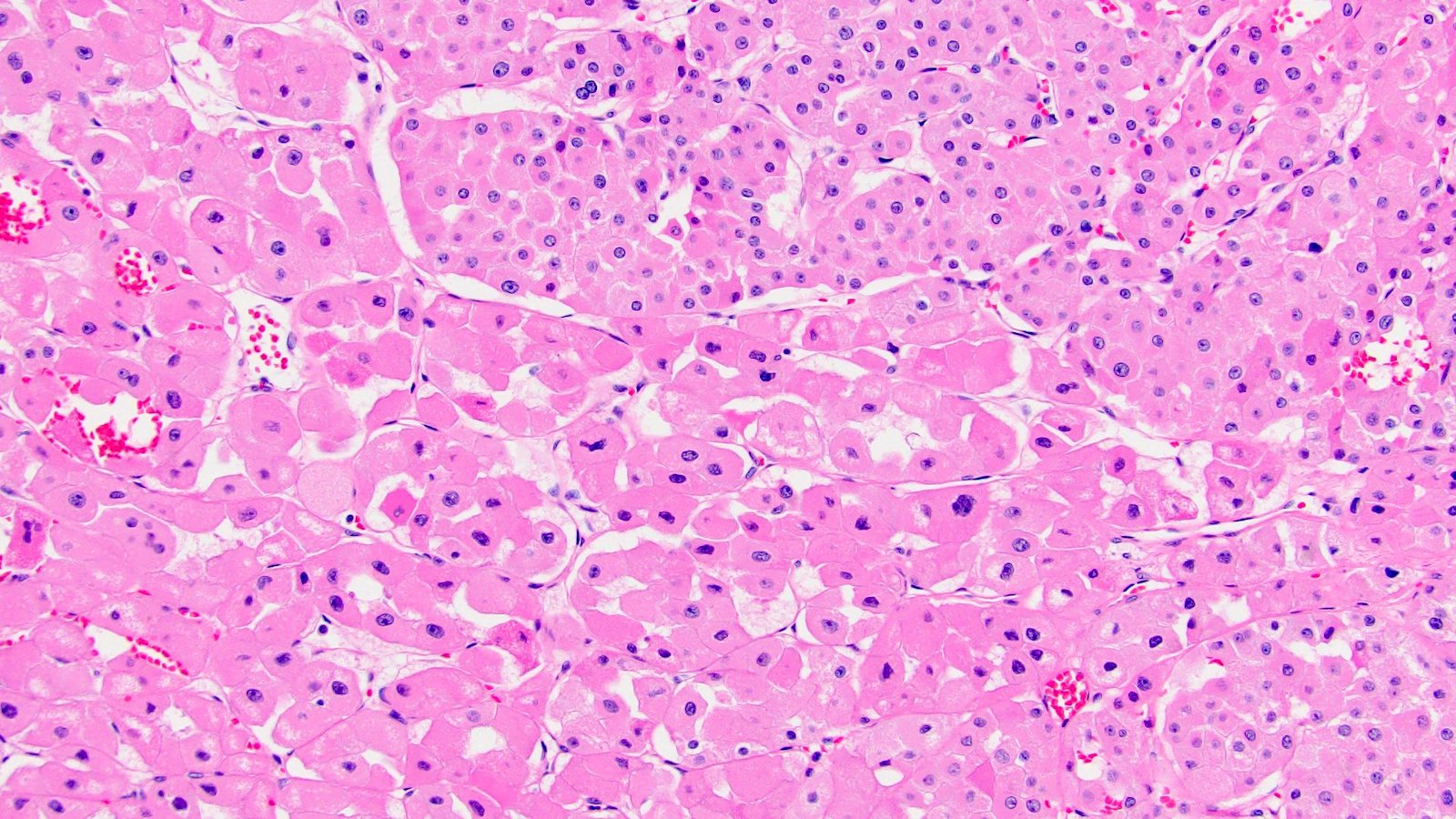
Lack of prominent membranes
Oncoblasts (20x)
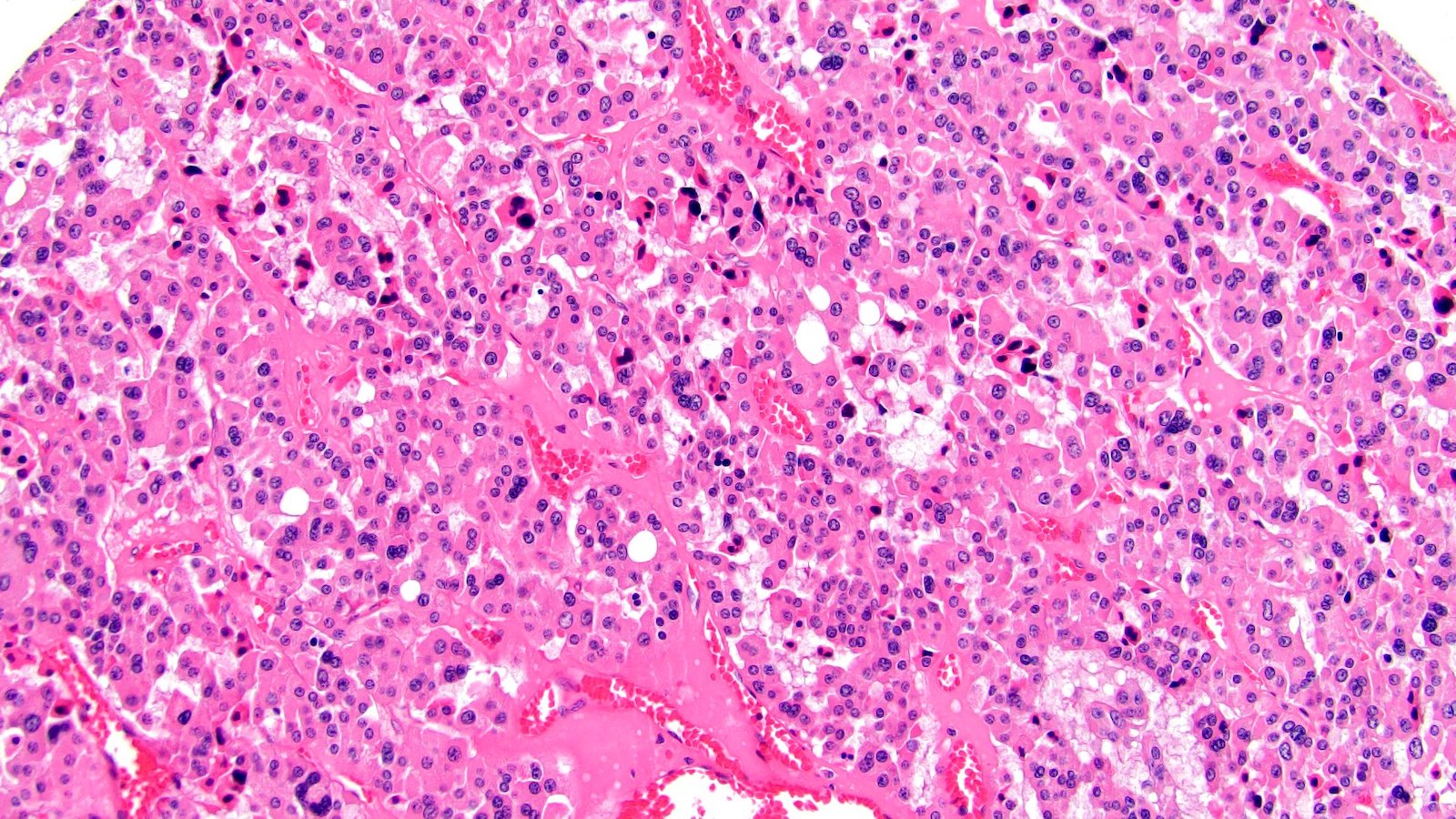
Degenerate atypia
Edematous stroma
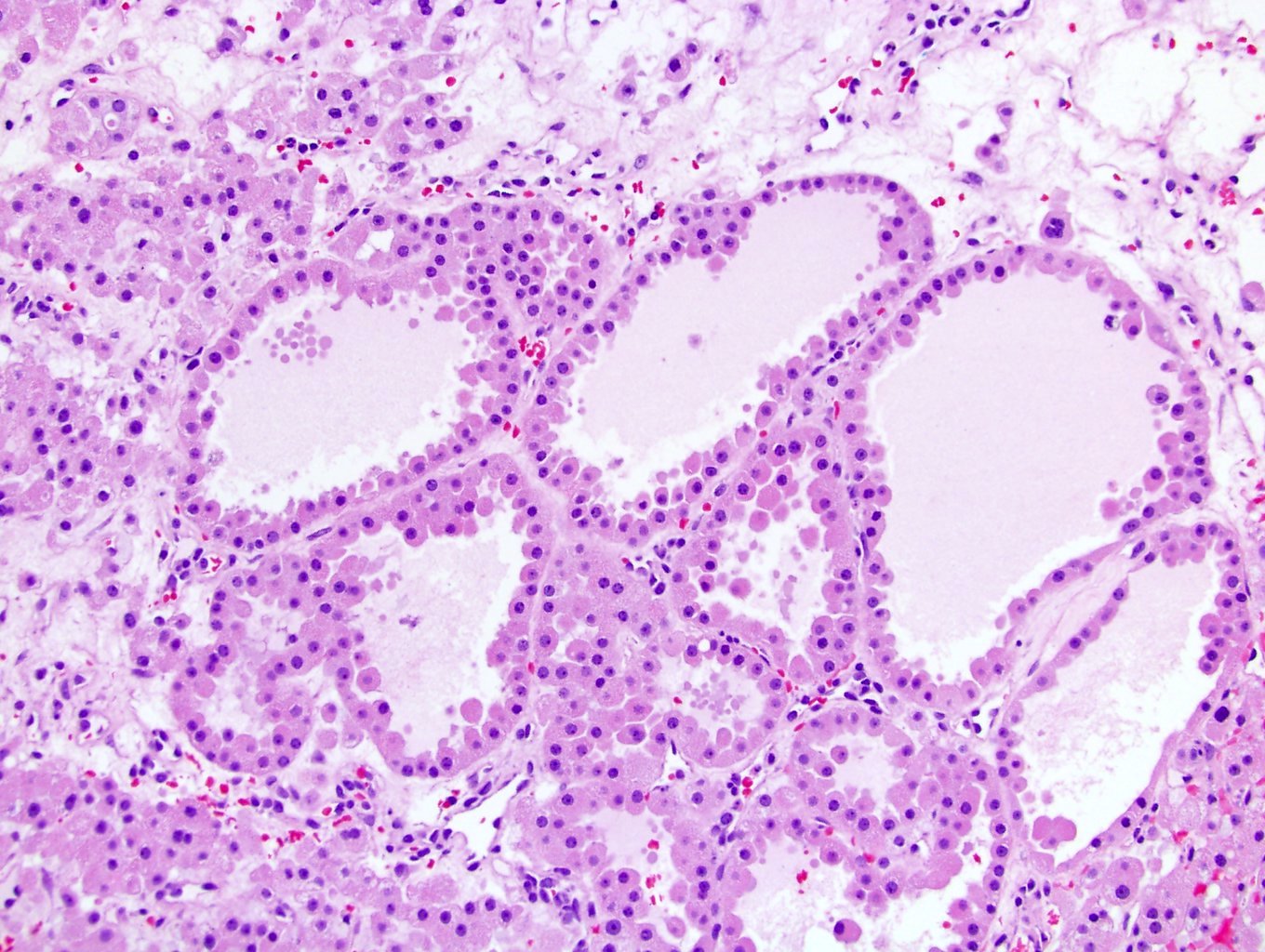
Microcystic, hobnailed
Atypia multinucleation
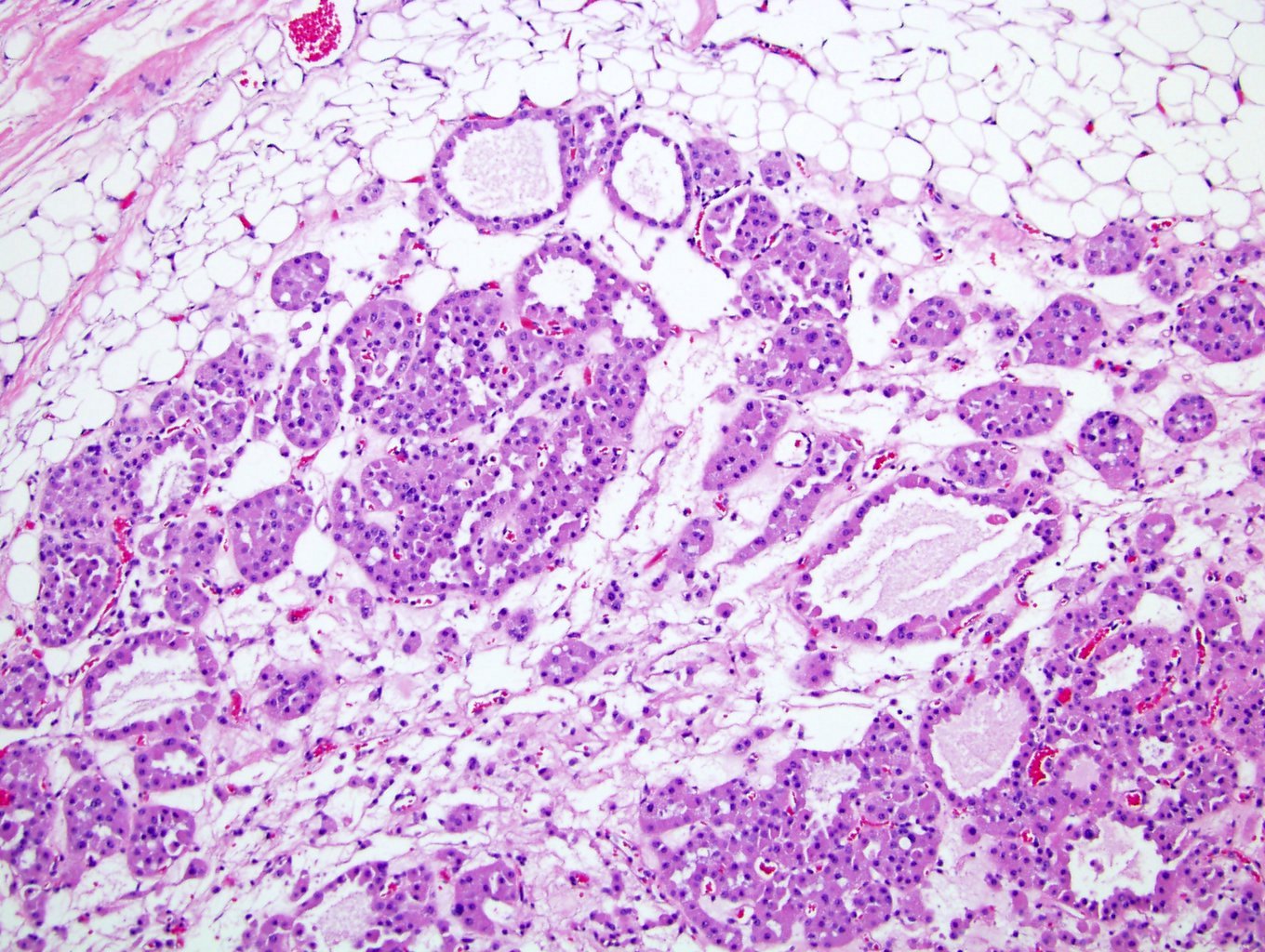
Fat extension
Rosettes

Vascular extension
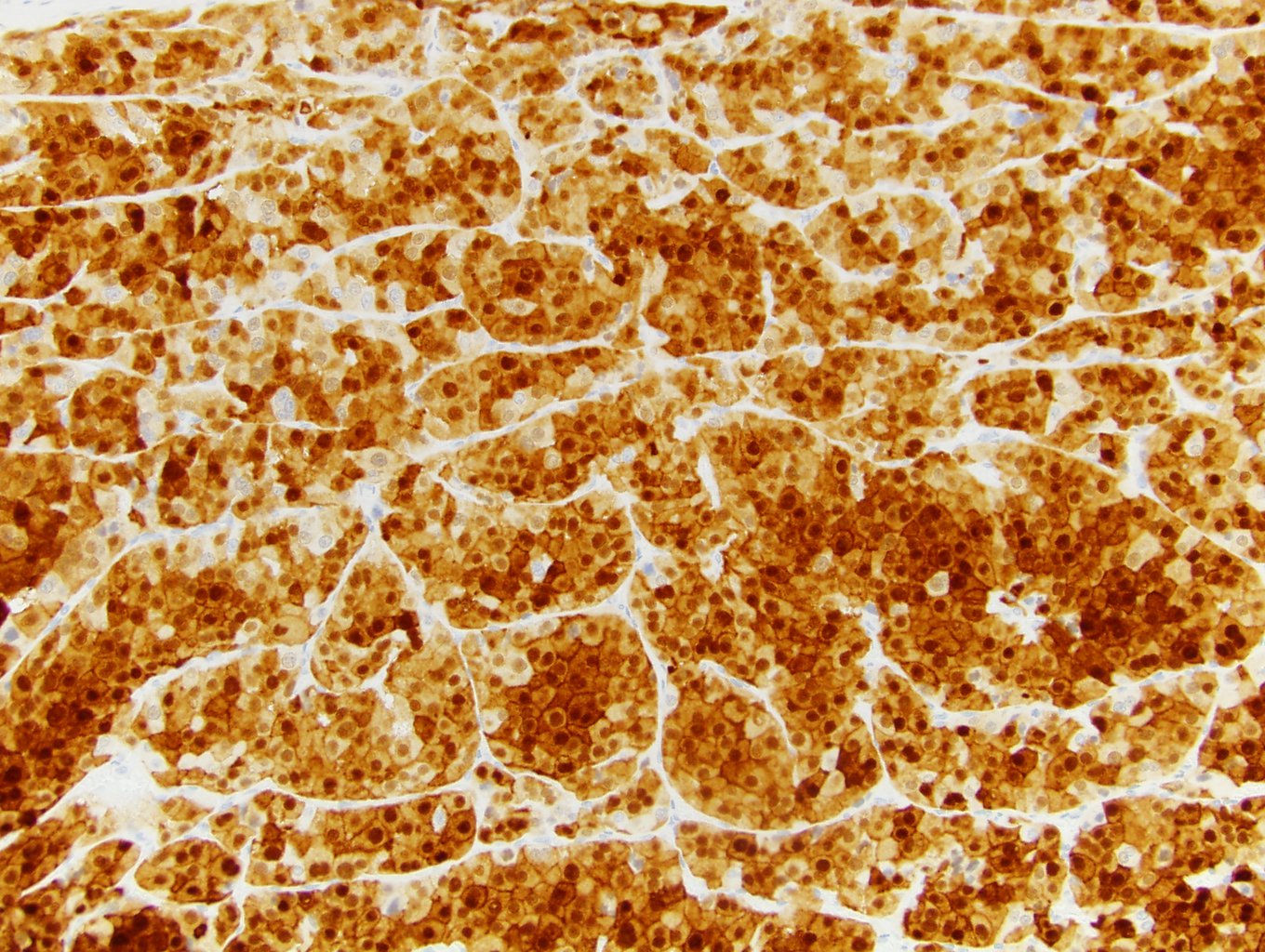
S100A1
CK7
Virtual slides
Images hosted on other servers:

Oncocytoma
Cytology description
- Highly cellular (Br J Urol 1988;61:534, Acta Cytol 1980;24:355, Cancer 2001;93:390)
- Rounded nests (on cell block)
- Cohesive fragments with discohesive cells
- Abundant eosinophilic and uniformly granular cytoplasm
- Round nuclei with medium sized nucleoli (grade 2)
- Mitosis absent and necrosis absent or very infrequent
- Can see occasional hyperchromatic bizarre cells, considered degenerative in nature
Cytology images
AFIP images
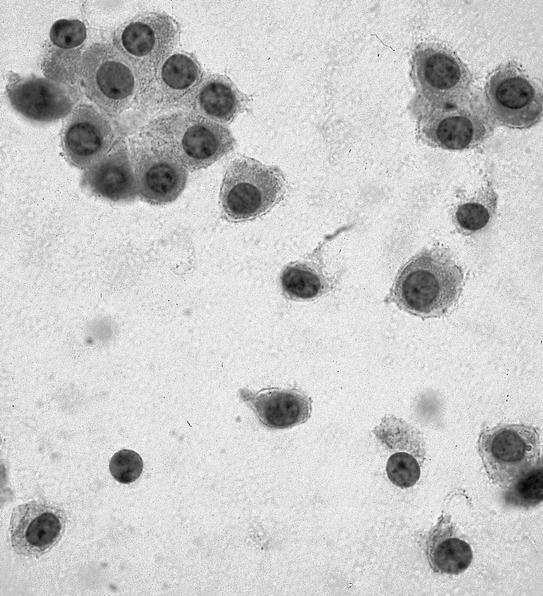
Abundant granular cytoplasm
Images hosted on other servers:

Small clusters and single cells with uniform cytoplasm

Diff-Quik shows
homogeneous granular
cytoplasm and round, regular
nuclei without grooves
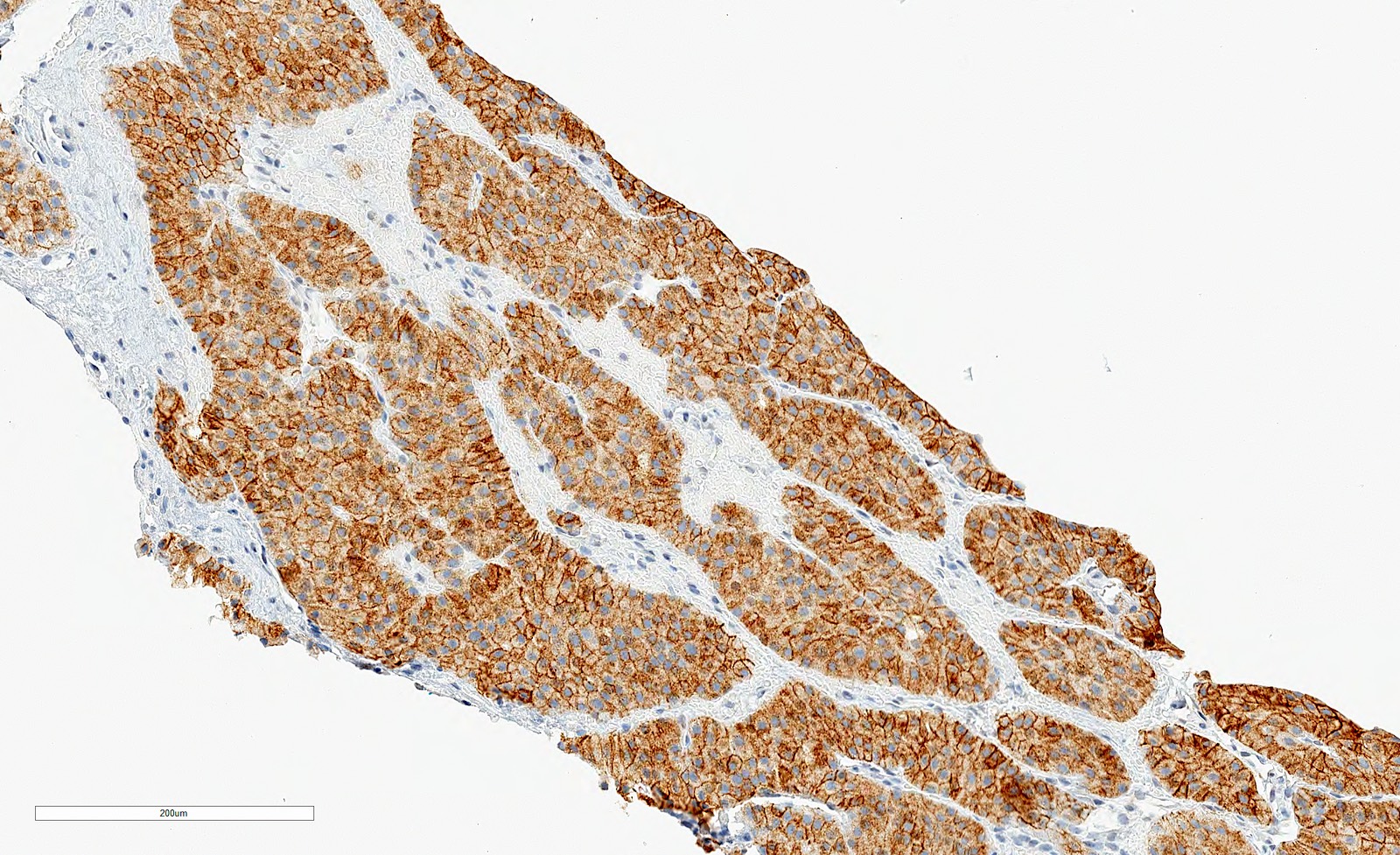
Positive stains
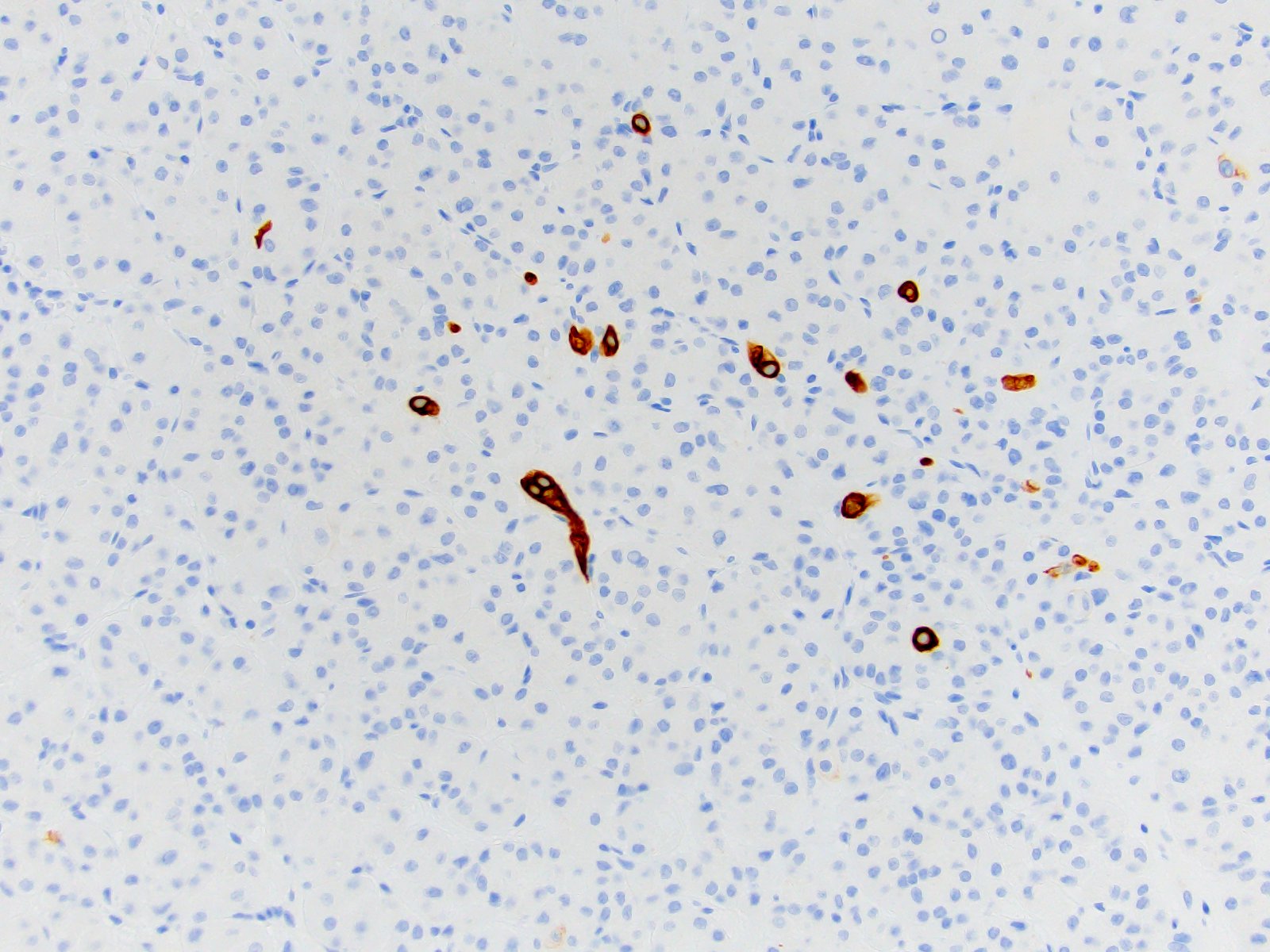
Negative stains
- CK7 negative or scattered rare positive cells
- AMACR
- CAIX
- Vimentin negative but can be positive in cells around central scars or in oncoblasts
- HMB45, melanA
- CK20
- Hale colloidal iron
- References: Semin Diagn Pathol 2005;22:51, Cancers (Basel) 2020;12:168, Am J Surg Pathol 2013;37:1469
IHC panels
Contributed by Maria Tretiakova, M.D., Ph.D.
| Hale | KIT | CK7 | S100A1 | VIM | CAIX | AMACR | SDH | TFE3 | |
| Chromophobe RCC | +++ | +++ | +++ | - | - | - | - | +++ | - |
| Clear cell RCC | - | - | - | - | +++ | +++ | - | +++ | - |
| Oncocytoma | - | +++ | rare | +++ | - | - | - | +++ | - |
| Papillary RCC | - | - | +++ | - | +++ | - | +++ | +++ | - |
| Translocation RCC | - | - | - | - | - | - | ++ | +++ | +++ |
| SDH deficient RCC | - | - | - | - | - | - | - | - | - |
References: Pathol Res Pract 2015;211:303, Ann Diagn Pathol 2020;44:151448, Am J Surg Pathol 2014;38:e6, Arch Pathol Lab Med 2019;143:1455, Transl Androl Urol 2019;8:S123, Hum Pathol 2020 Jul 13 [Epub ahead of print]
Electron microscopy description
- Cytoplasm packed with mitochondria with lamellar cristae (Hum Pathol 1984;15:1054, Histol Histopathol 2003;18:935)
Electron microscopy images
AFIP images
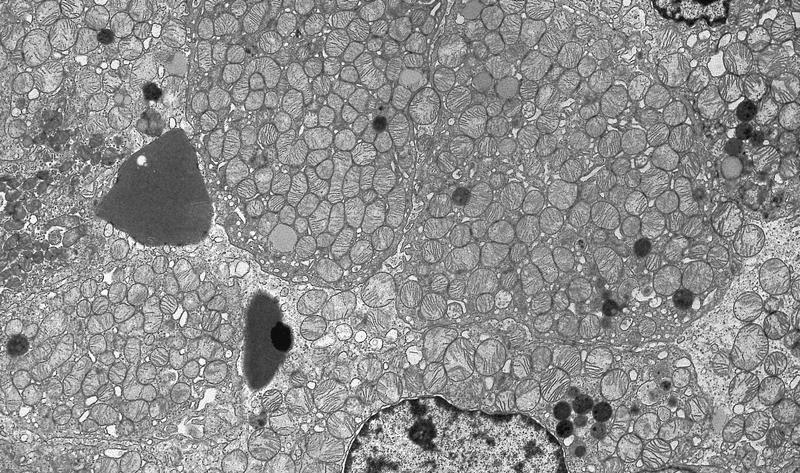
Cytoplasm is packed with large mitochondria
Molecular / cytogenetics description
- Commonly possess mitochondrial mutations
- Commonly harbor losses of chromosome 1 and Y and also chromosome 14
- Some cases show translocation of 11q13 that involve the CCDN1 gene and overexpress cyclin D1 (gene product)
- Has been suggested that tumors with chromosomal losses (aneuploid) have the potential to develop into eosinophilic chromophobe renal cell carcinomas with more additional molecular events as p53 mutations, while the cases that have CCDN1 rearrangements don't tend to progress in that manner (Cell Rep 2015;13:1895)
- Familial cases of Birt-Hogg-Dubé syndrome have mutations in the FLCN gene; it is inherited in an autosomal dominant pattern
Molecular / cytogenetics images
Images hosted on other servers:

FISH: loss of chromosomes 1 and 17
Sample pathology report
- Right kidney, needle core biopsy:
- Oncocytic renal neoplasm, favors oncocytoma (see comment)
- Comment: Tumor shows an oncocytic neoplasm with morphological features and immunoprofile consistent with a renal oncocytoma. The lesion is formed of oncocytic cells arranged in small nests in surrounding loose edematous stroma. Tumor cells have round regular nuclei with intermediate sized prominent nucleoli. No irregular nuclear contours or perinuclear halos identified. Lesional cells are positive for PAX8 and KIT and are negative for CK7. However, taking into account possible tumor heterogeneity, we cannot rule out a hybrid oncocytic tumor or an eosinophilic variant of chromophobe renal cell carcinoma in this limited specimen.
- Right kidney, robotic partial nephrectomy:
- Oncocytoma, 2.6 cm
- Surgical margins negative for tumor
Differential diagnosis
- Eosinophilic variant of chromophobe renal cell carcinoma (Anticancer Res 2019;39:2785):
- Nuclear membrane irregularities (wrinkling) and perinuclear halos
- CK7 positive (however, sometimes patchy in eosinophilic chromophobe)
- S100A1 usually negative
- Hybrid oncocytic / chromophobe tumors (HOCT) (Mod Pathol 2019;32:1698):
- Term usually applied in syndromic settings as the Birt-Hogg-Dubé associated tumors but occasionally sporadic cases can present as such
- Overlapping features morphologically and immunophenotypically between oncocytoma and chromophobe renal cell carcinoma
- Best characterized currently as low grade oncocytic tumors
- SDH deficient renal cell carcinoma (Histopathology 2019;74:31):
- Oncocytic papillary renal cell carcinoma:
- Eosinophilic clear cell renal cell carcinoma:
- Epithelioid angiomyolipoma:
- Nuclear pleomorphism
- May have areas of smooth muscle and adipose tissue
- Negative keratins and negative PAX8
- Positive for melanocytic markers HMB45 and MelanA / MART1; positive for cathepsin K
- MiTF associated renal cell carcinoma (TFEB t6;11 can present with oncocytoma-like features) (Cancers (Basel) 2019;11:1110):
- Morphology can be variable; includes a described biphasic morphology
- Positive for TFE3 or TFEB and cathepsin K
- Negative or focally positive for keratin
- Can be focally positive for HMB45 and MART1
- Low grade oncocytic tumors (LOT) (newly proposed entity) (Histopathology 2019;75:174):
- Eosinophilic, solid and cystic renal cell carcinoma (ESC) (newly proposed entity) (Cancers (Basel) 2020;12:168):
- Described in both sporadic and tuberous sclerosis syndrome setting
- Coarse basophilic cytoplasmic granules
- Positive for CK20
- Preliminary data but seem to exhibit indolent clinical behavior
Practice question #1
A 40 year old man presented with an incidentally discovered renal cortical mass measuring 4.5 cm on imaging. Histological examination revealed an oncocytic lesion. Lesional cells were positive for PAX8, LMWK and CD117 and only rare cells expressed CK7. Which is most likely the correct diagnosis?
- Angiomyolipoma
- Metanephric adenoma
- Oncocytoma
- Papillary adenoma
- Renal cell carcinoma, chromophobe type
Practice answer #1
Practice question #2
A 55 year old man presents with multiple bilateral renal cortical masses on imaging. The patient has a significant family history of kidney cancer; his father died of metastatic chromophobe renal cell carcinoma at age 65. The largest lesions were biopsied bilaterally. Histological morphological examination and thorough immunohistochemical analysis yielded the diagnosis of hybrid oncocytic / chromophobe renal tumors on both lesions. The most likely genetic abnormality this patient has is
- FLCN mutations
- FH gene mutation
- SDH gene mutations
- VHL gene mutations
Practice answer #2
A. FLCN mutations. The syndrome associated with renal oncocytosis and oncocytoma / HOCT / chromophobe tumors is the Birt-Hogg-Dubé syndrome. It is characterized by mutations in the FLCN gene. VHL mutations are the hallmark of clear cell renal cell carcinoma in the VHL syndrome. FH germline mutations are associated with hereditary leiomyomatosis renal cell carcinoma syndrome. SDH complex deficiency syndrome is associated with SDH deficiency renal cell carcinoma, which can also present with an oncocytic morphology. However, SDH deficient RCC can be excluded by proper morphological and immunohistochemical workup.
Comment Here
Reference: Oncocytoma
Comment Here
Reference: Oncocytoma
