
Liver & intrahepatic bile ducts
Viral hepatitis
Hepatitis C virus (HCV)
Author: Komal Arora, M.D.

Last author update: 1 May 2012
Last staff update: 21 February 2024 (update in progress)
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Hepatitis C virus[TI] HCV[TI] liver[TI]
Table of Contents
Definition / general | Causes and complications | Virology | Poor prognostic factors | Treatment | Post liver transplant | Case reports | Microscopic (histologic) description | Microscopic (histologic) images | Additional referencesCite this page: Arora K. Hepatitis C virus (HCV). PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/liverhepC.html. Accessed April 23rd, 2024.
Definition / general
- 0.2% incidence in US, 170 million people infected worldwide
- 90% of non-A, non-B hepatitis cases, 75 - 95% of transfusion associated hepatitis cases are due to hepatitis C
Causes and complications
- 35% IV drug abuse, 15% household contact or heterosexual exposure, 5% blood transfusion, 45% unknown
- 50 - 80% develop chronic liver disease, 20% of these develop cirrhosis
- High risk for hepatocellular carcinoma, particularly with alcoholic cirrhosis (57% at 10 years)
- Acute liver failure is rare
- CD34+ sinusoidal endothelial cells are a risk factor for hepatocellular carcinoma in HCV associated chronic liver disease (Hum Pathol 2001;32:1363)
- In HIV+ patients, cirrhosis more common if CD4 < 200 cells/microL (Hum Pathol 2000;31:69)
- Complications: deterioration of liver status with cirrhosis in 20% and improvement in 10% with chronic hepatitis C; also hepatocellular carcinoma
Virology
- Flavivirus, enveloped RNA virus
Poor prognostic factors
- Necroinflammatory activity is associated with fibrosis progression (Hum Pathol 2001;32:904)
- Also alcohol consumption, advanced age at the time of infection and immunocompromise
Treatment
- Longterm interferon alpha causes regression of cirrhosis in 5 - 10% (Hum Pathol 2004;35:107)
- Interferon used in combination with ribavirin; orthotopic liver transplantation
- 10% have stainable iron; some hepatologists use iron content and location in patient management
- Occasionally may be due to mutation in gene for hereditary hemochromatosis (Arch Pathol Lab Med 2000;124:1632)
Post liver transplant
- Recurrence of hepatitis C (as opposed to reinfection, which is almost universal) associated with more single cell hepatocyte necrosis (acidophil bodies), bile duct damage, lymphoid aggregates, cholestasis, fibrous septum, viral load (HCV RNA) > 1.25 million viral equivalents/ml
- Recurrence may resemble cellular rejection
- Serial biopsies may be necessary (Hum Pathol 2002;33:277, Arch Pathol Lab Med 2000;124:1623, Mod Pathol 2002;15:897)
- HCV RNA levels are highest at time of active hepatocellular destruction (Mod Pathol 1999;12:1043)
Case reports
- 55 year old man with coexisting hepatocellular carcinoma and diffuse large B cell lymphoma (Arch Pathol Lab Med 2000;124:1532)
- With coexisting diffuse large B cell lymphoma (Am J Surg Pathol 1999;23:1124)
Microscopic (histologic) description
- Predominantly sinusoidal lymphocytic infiltrate, often with lymphoid follicles that surround damaged bile ducts, often involvement of portal tracts
- Mallory hyaline, mild and focal macrovesicular steatosis, minimal necrosis
- Usually no / minimal plasma cells or eosinophils; may have irregular acidophil bodies
- Lymphoid aggregates are specific for hepatitis C but only 50% sensitive
Microscopic (histologic) images
Images hosted on other servers:
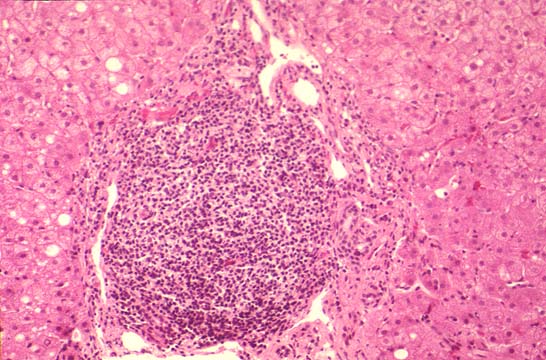
Portal lymphocytosis
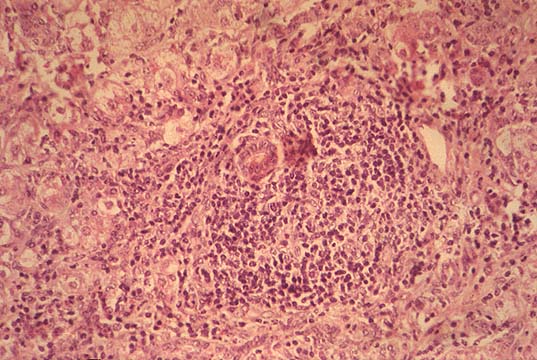
Bile duct involvement
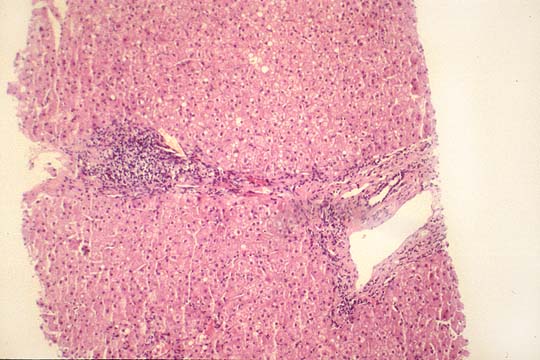
Portal - portal fibrosis
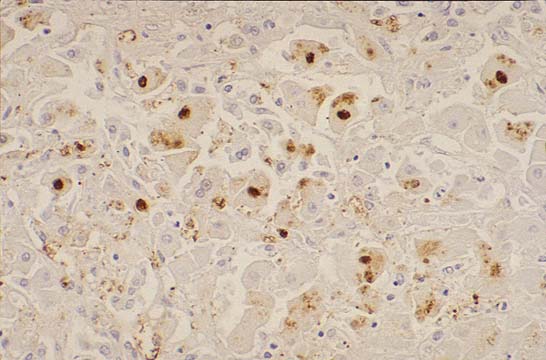
Immunostain
Additional references
