
Liver & intrahepatic bile ducts
Noninfectious hepatitis
Neonatal hepatitis
Author: Anthony W.H. Chan, M.B.Ch.B.

Last author update: 1 July 2015
Last staff update: 23 April 2024 (update in progress)
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Neonatal hepatitis
Table of Contents
Definition / general | Terminology | Epidemiology | Etiology | Clinical features | Diagnosis | Case reports | Microscopic (histologic) description | Microscopic (histologic) images | Negative stains | Differential diagnosisCite this page: Chan A. Neonatal hepatitis. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/liverneonatalhep.html. Accessed April 24th, 2024.
Definition / general
- Neonatal cholestasis is prolonged jaundice beyond 2 weeks of age; it can be simply classified into extrahepatic and intrahepatic causes (Clin Res Hepatol Gastroenterol 2014;38:263)
- Extrahepatic biliary atresia is the most common cause of extrahepatic cholestasis
- Neonatal hepatitis is a nonspecific collective term for intrahepatic cholestasis due to all various etiologies
Terminology
- Also known as neonatal giant cell hepatitis because of frequent syncytial giant cell formation
Epidemiology
- Neonatal cholestasis happens in about 1 in 2,500 - 5,000 term infants (Clin Res Hepatol Gastroenterol 2014;38:263)
Etiology
- Intrahepatic neonatal cholestasis accounts for 60 - 70% of all neonatal cholestasis
- Usual causes include (Front Pediatr 2015;3:43):
- 9 - 17%: metabolic disorders - alpha-1-antrypsin deficiency, cystic fibrosis and hypopituitarism are common (Am J Surg Pathol 2010;34:1498)
- 10%: progressive familial intrahepatic cholestasis (PFIC) (J Clin Exp Hepatol 2014;4:25)
- 10%: preterm (increased incidence of 100 - 200x in infants born before 28 weeks of gestation compared to term infants)
- 1 - 9%: congenital / neonatal infection - cytomegalovirus, enterovirus, hepatitis B, herpes simplex, human herpesvirus 6, rubella, sepsis, syphilis, toxoplasmosis, varicella
- 2 - 6%: Alagille syndrome
- 2%: chromosomal abnormalities - trisomy 18 and Down syndrome (incidence 100x normal term infants)
- 13 - 30%: idiopathic neonatal hepatitis
Clinical features
- Prolonged jaundice beyond 2 weeks of age
- Other clinical features depend on underlying etiology
Diagnosis
- Based on clinical, laboratory, radiological and histological features
Case reports
- Newborn boy with idiopathic neonatal giant cell hepatitis presenting with acute hepatic failure (J Perinatol 2002;22:249)
- 7 week old girl with fatal spontaneous subdural bleeding due to neonatal giant cell hepatitis (Forensic Sci Med Pathol 2011;7:294)
Microscopic (histologic) description
- General nonspecific changes:
- Lobular changes: giant cell transformation (hepatocytes containing 4 - 10 nuclei), variable lobular inflammatory infiltrate and necrosis (spotty, confluent to bridging), canalicular ± hepatocellular bilirubinostasis, extramedullary hematopoiesis
- Portal tract changes: variable portal mononuclear inflammatory infiltrate
- Specific changes depend on underlying etiology
Microscopic (histologic) images
Contributed by Anthony W.H. Chan, M.B.Ch.B.
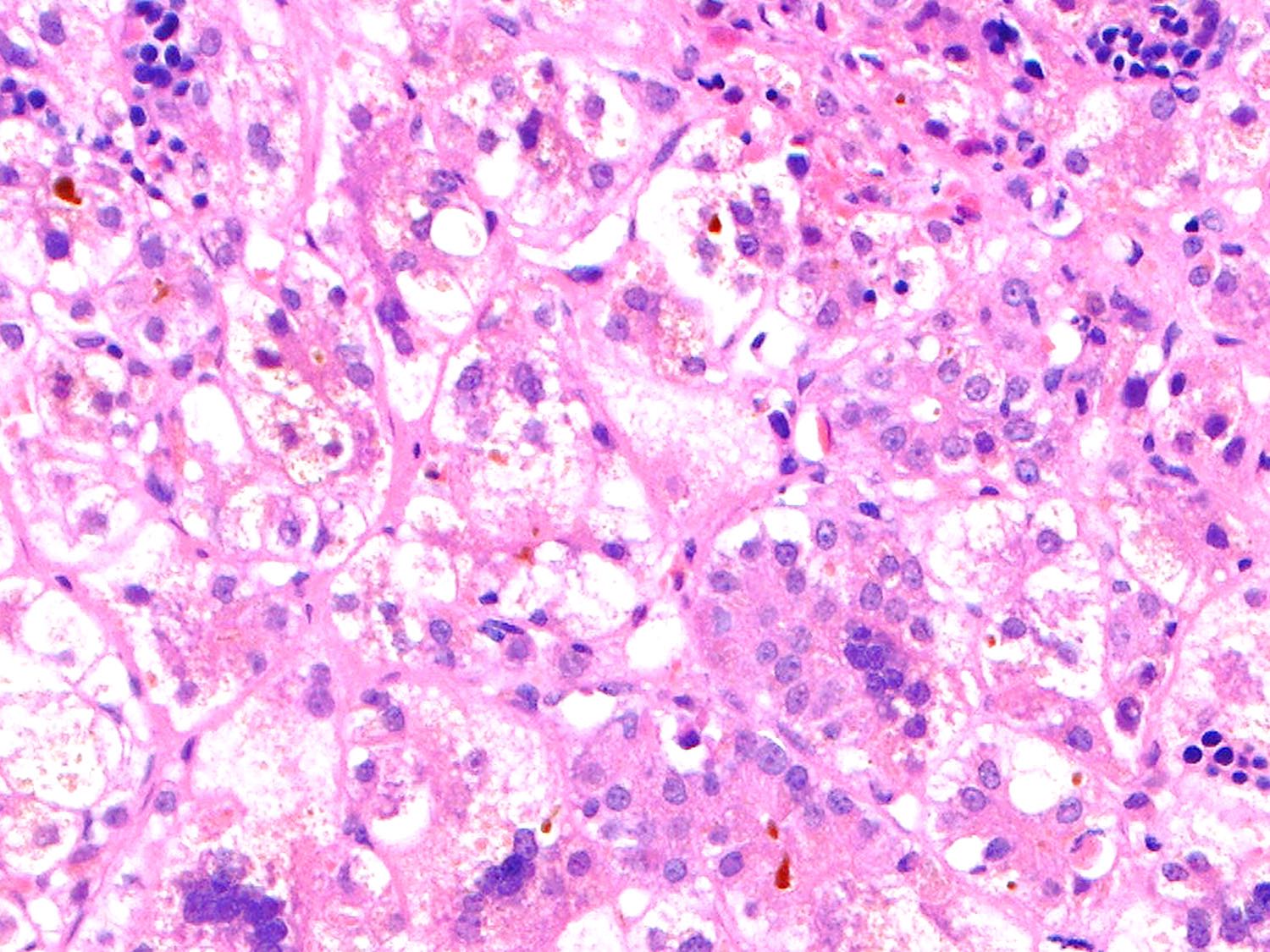
Neonatal hepatitis
Negative stains
Differential diagnosis
- Extrahepatic biliary atresia:
- Diagnostic accuracy of different methods distinguishing extrahepatic biliary atresia from idiopathic neonatal hepatitis: liver biopsy (97.1%), magnetic resonance cholangiography (MRCP; 70.0%), hepatobiliary scintigraphy (66.7%), ultrasound (65.2%) (Clin Imaging 2009;33:439)
- Ductular reaction and portal fibrosis are essential discriminatory histological features suggestive of extrahepatic biliary atresia (Eur J Gastroenterol Hepatol 2014;26:1300)
- Presence of CD56 / NCAM+ bile duct and ductules favor extrahepatic biliary atresia (Am J Surg Pathol 2003;27:1454)
