Liver & intrahepatic bile ducts
General
Anatomy & histology


Copyright: 2002-2025, PathologyOutlines.com, Inc.
PubMed Search: Liver anatomy & histology

- Liver is the largest solid organ and is located in the right upper quadrant of the abdomen
- Functional unit is the hepatic lobule, composed of hepatocyte plates surrounding a central vein with portal tracts at the periphery
- Main cell type is the hepatocyte, which is critical for producing bile and for metabolizing drugs, proteins, fats, carbohydrates and vitamins
- Biliary epithelial cells (cholangiocytes) line bile ducts, which transport and modify bile
- Hepatic stellate cells, located in the space of Disse, store vitamin A and become activated and fibrogenic in response to injury
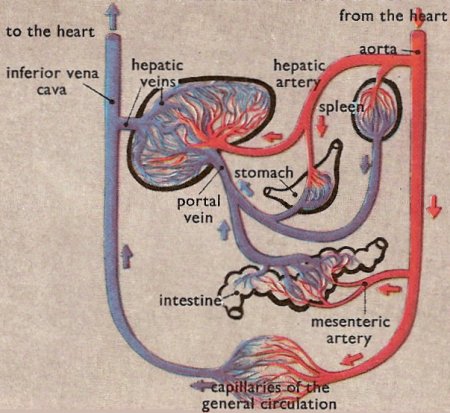
- Dual blood flow from hepatic artery and portal vein passes through sinusoids and exits the liver via hepatic vein branches
- Hepatic: of or relating to the liver
- Arises at embryonic junction (septum transversum): where ectoderm of amnion meets endoderm of yolk sac (externally) and where foregut meets midgut (internally); mesenchymal structure of transverse septum provides support so blood vessels and liver can form in underlying splanchnic mesoderm (UNSW Embryology: Gastrointestinal Tract - Liver Development [Accessed 23 October 2017])
- Hepatic diverticulum buds from ventral foregut at end of third week, grows into primitive septum transversum
- Liver forms from endodermal cells of diverticulum, termed hepatoblasts and mesenchyme
- Blood supply primarily from umbilical vein; also portal vein and hepatic artery
- Placenta clears wastes in bile and absorbs nutrients
- Umbilical vein blood bypasses liver via ductus venosus
- All elements of the biliary tree are recognizable by week 5, although bile duct system is not complete until after birth
- Derived from endoderm (large ducts) and embryonic ductal plate (smaller intrahepatic ducts) (Dig Surg 2010;27:87)
- Hematopoietic cells are present in embryonic / fetal liver but absent at term
- Drug metabolism
- Phase 1 reactions increase polarity and water solubility of compounds via oxidation, reduction and hydrolysis through the cytochrome p450 system
- Phase 2 reactions create fewer toxic byproducts through transferase reactions and conjugations
- Lipid metabolism
- During prolonged fasting states, free fatty acids (FFAs) produced by lipolysis in adipose tissue are transported to the liver
- FFAs are beta-oxidized in liver to release ketone bodies to fuel the brain or formed into triglycerides for storage or transportation
- Carbohydrate metabolism
- In the fed state, carbohydrates are stored as glycogen in the liver
- In the fasting state, glycogen can be broken down for systemic use (glycogenolysis)
- Lactate, amino acids and glycerol can be converted into glucose (gluconeogenesis)
- Protein metabolism
- Ingested proteins are broken down into amino acids to be used throughout the body
- Excess amino acids are oxidized for energy or converted into glucose, ketone bodies or fat
- Nitrogen waste products are converted to urea to be excreted in the urine
- Various proteins are synthesized, including albumin, coagulation factors and fibrinolytic components
- Bile production (Compr Physiol 2013;3:1035)
- Bile salts are produced by hepatocytes from cholesterol and conjugated with glycine or taurine, secreted into canaliculi, modified by cholangiocytes and stored and further concentrated in the gallbladder
- Bile salts returning from the GI tract via the portal vein are actively transported into hepatocytes to be recycled
- Free bilirubin is taken up by hepatocytes, conjugated to glucuronic acid and secreted with bile
- Vitamin metabolism
- Vitamin A storage (hepatic stellate cells)
- Vitamin D 25-hydroxylation
- Vitamins A, D, E and K absorption from intestine, which requires bile salts
- B vitamin uptake, storage and metabolism / conversion
- See also Gross description
- Divided into right and left lobes by Cantlie line projecting between the gallbladder fossa and vena cava and defined by the middle hepatic vein
- Right lobe is divided into anterior and posterior segments by right hepatic vein
- Left lobe is divided into medial and lateral segments by left hepatic vein
- Intrahepatic biliary tree: classified into intrahepatic large bile ducts (grossly visible with fibrous ductal wall and peribiliary glands) and small bile ducts
- Regional lymph nodes: hilar, hepatoduodenal ligament, caval
- May appear clinically as hepatic mass
- Anterior abdominal wall defects are frequently associated with accessory hepatic lobes
- Can present with torsion (Surg Radiol Anat 2011;33:819)
Images hosted on other servers:

Lobule and portal triad

Anatomy and functional segments

Embryonic hepatic bud formation

Anterior and posterior views
Blood supply

Intrahepatic biliary tree

Anatomy of abdomen

Location of liver

Superior view of liver

Inferior view of liver

Impressions of liver

Cells, ducts, blood vessels

Microscopic anatomy

Types of capillaries

Parts of liver

Hilum of liver

Couinaud segments

Liver and veins

Liver, lobule, portal tract

Biliary tract
- Metabolic differences among the zones of hepatic lobules influence hepatocytes’ susceptibility to viral infection, drug injury, nonalcoholic fatty liver disease and other insults (Exp Biol Med (Maywood) 2017;242:1605)
- Aspartate transaminase (AST) and alanine transaminase (ALT) to evaluate potential hepatocyte damage
- Albumin, coagulation factors, prothrombin time (PT) and partial thromboplastin time (PTT) to evaluate synthetic function
- Alkaline phosphatase and bilirubin to evaluate the biliary system and excretion
- Reference: CMAJ 2005;172:367
- Normal weight in adults is 1,400 - 1,600 grams (Am J Surg Pathol 1987;11:709)
- Can be divided into 4 lobes: right, left, caudate and quadrate
- Gallbladder (if present) is located on posterior surface of right lobe
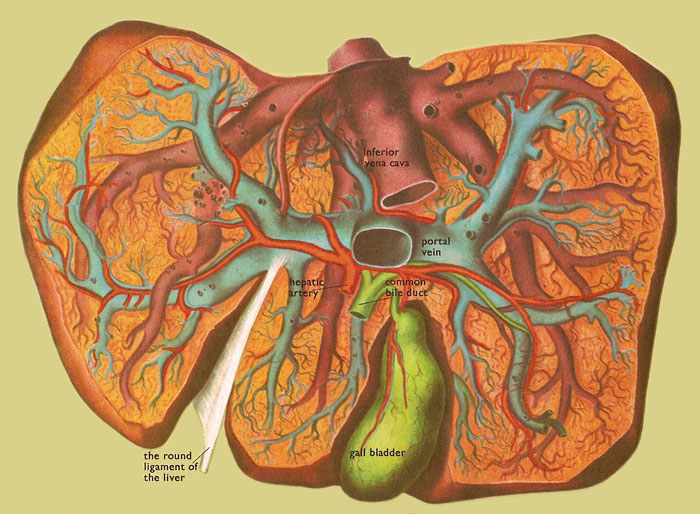
- Dual blood supply (hepatic artery and portal vein) enters at the hilum / porta hepatis on the inferior aspect and exits via the left and right hepatic veins to inferior vena cava
- Peritoneum covers the superior, anterior and lateral surfaces
- External surface is smooth and red-brown
- Cut surface is firm and red-brown, with branches of portal vein, hepatic artery, bile ducts and hepatic vein seen throughout
Contributed by Michelle Wilkinson, B.S., P.A. (ASCP)

Red-brown cut surface
Images hosted on other servers:

Liver at autopsy
- Frozen section may be done to evaluate potential donor livers
- Assess for large and small droplet steatosis, fibrosis and inflammation
- Sinusoids may appear prominent and mimic steatosis
- Submitting tissue sample in saline may introduce water artifact mimicking steatosis
- Reference: J Clin Med Res 2011;3:191
Contributed by Kimberley J. Evason, M.D., Ph.D.
Portal tract
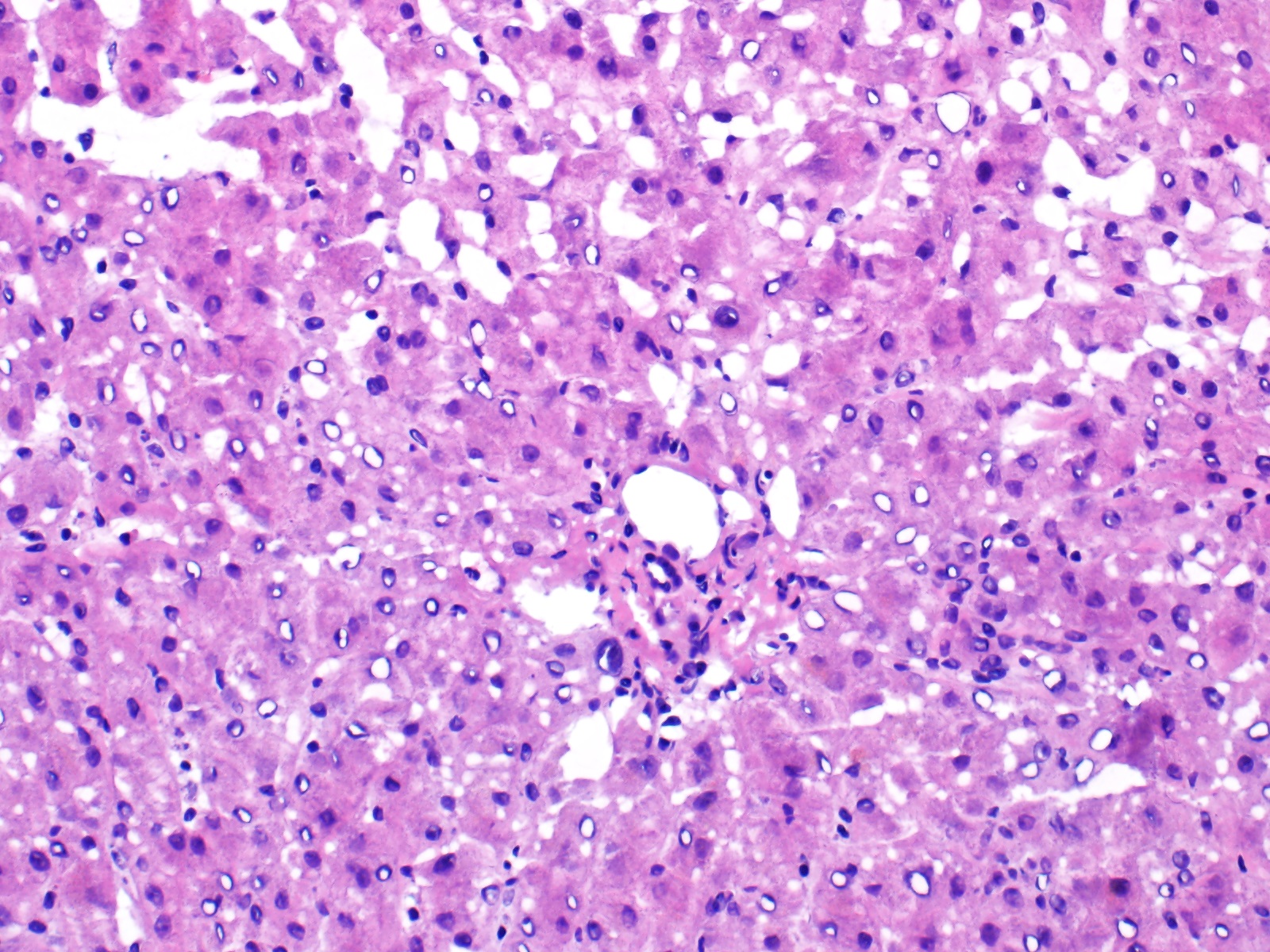
Central zone
- Main liver cell types
- Hepatocytes
- Arranged in plates 1 - 2 cells thick
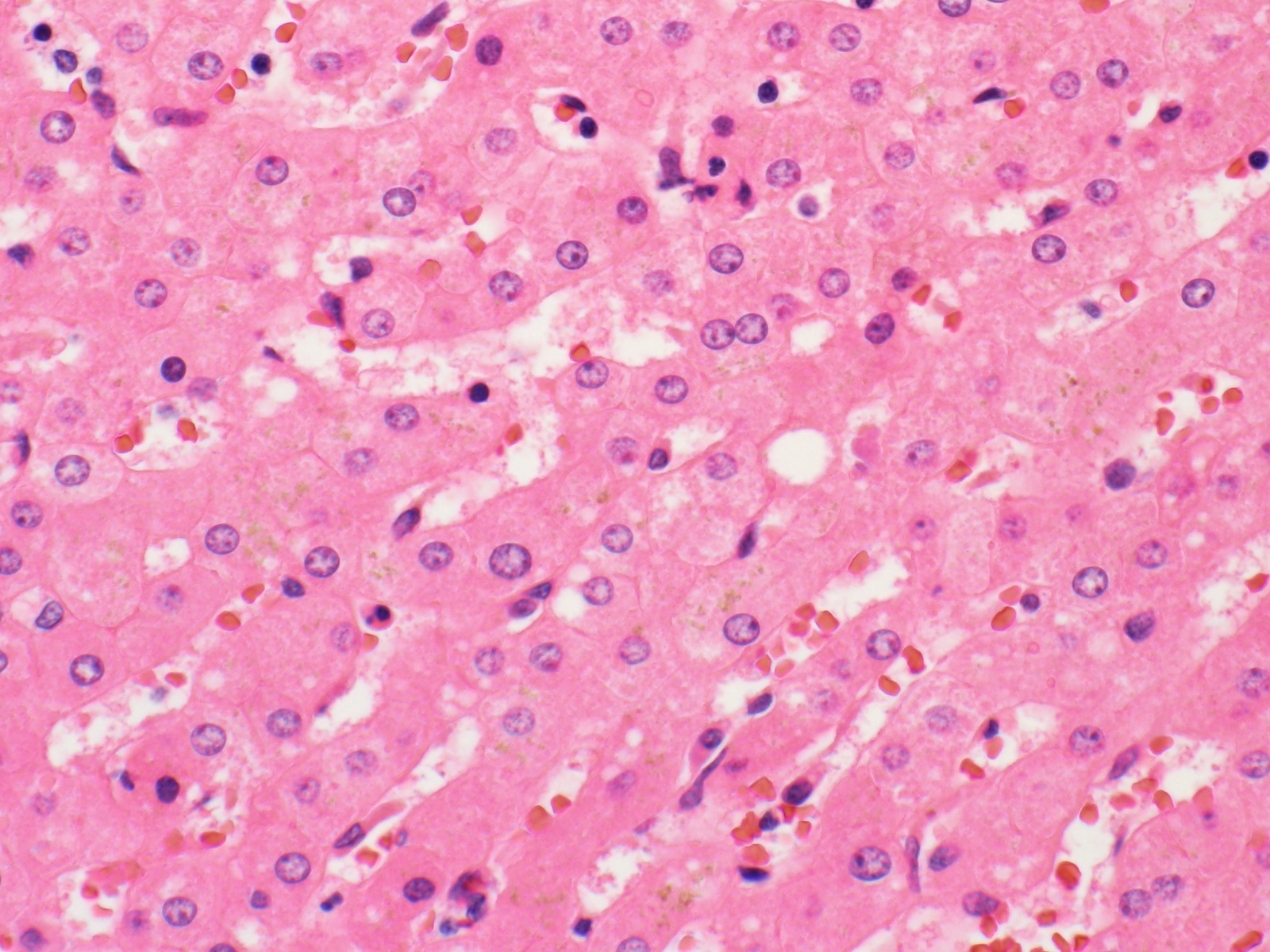
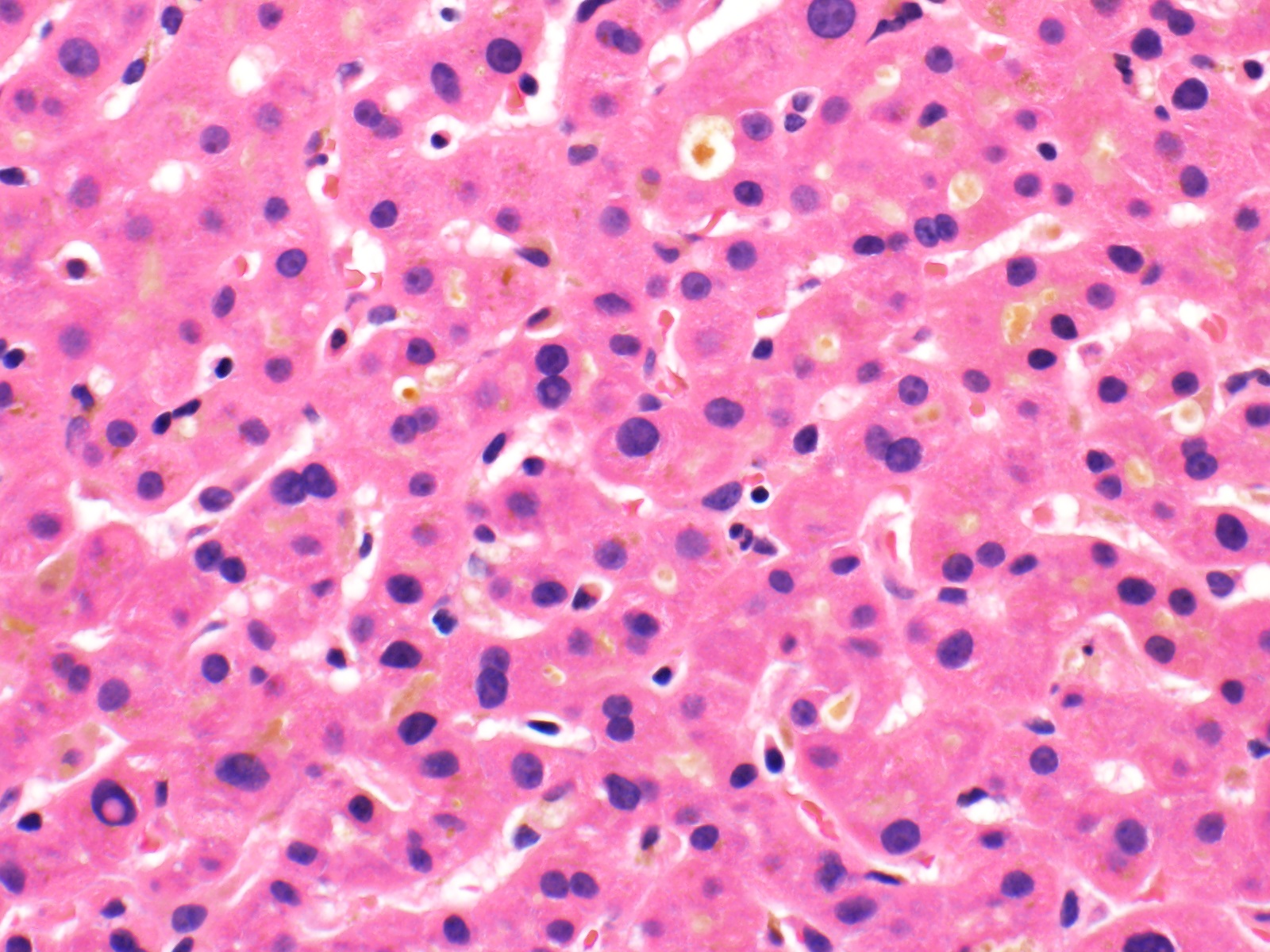
- Polygonal cells with round, centrally located nuclei and abundant eosinophilic cytoplasm with fine basophilic granules; can be pleomorphic and multinucleated
- May contain fat vacuoles, glycogen or lipofuscin pigment
- Cholangiocytes (bile duct epithelial cells)
- Line bile ducts and ductules
- Cuboidal epithelial cells with round, centrally located nuclei
- Kupffer cells
- Located in the sinusoids
- Mononuclear, phagocytic cells (macrophages) that respond to cell injury
- Bean shaped nucleus with abundant cytoplasm and star shaped cytoplasmic extensions
- Stellate cells
- Located in the space of Disse (not normally seen on H&E)
- Become activated in response to cell injury and differentiate into myofibroblasts
- Store fat and vitamin A (Physiol Rev 2008;88:125)
- Endothelial cells
- Line sinusoids as well as blood vessels
- Indistinct cytoplasm and small, elongated nuclei
- Hepatocytes
- Important microscopic features
- Limiting plate: formed by hepatocytes joining together to form a distinct row around portal tracts
- Bile canaliculi: intercellular space formed by adjacent hepatocytes (often not well visualized in normal liver unless distended)
- Sinusoids
- These separate cords of hepatocytes
- Lined by endothelial cells and Kupffer cells
- Space of Disse: space between endothelial cells and hepatocytes (not well visualized on H&E)
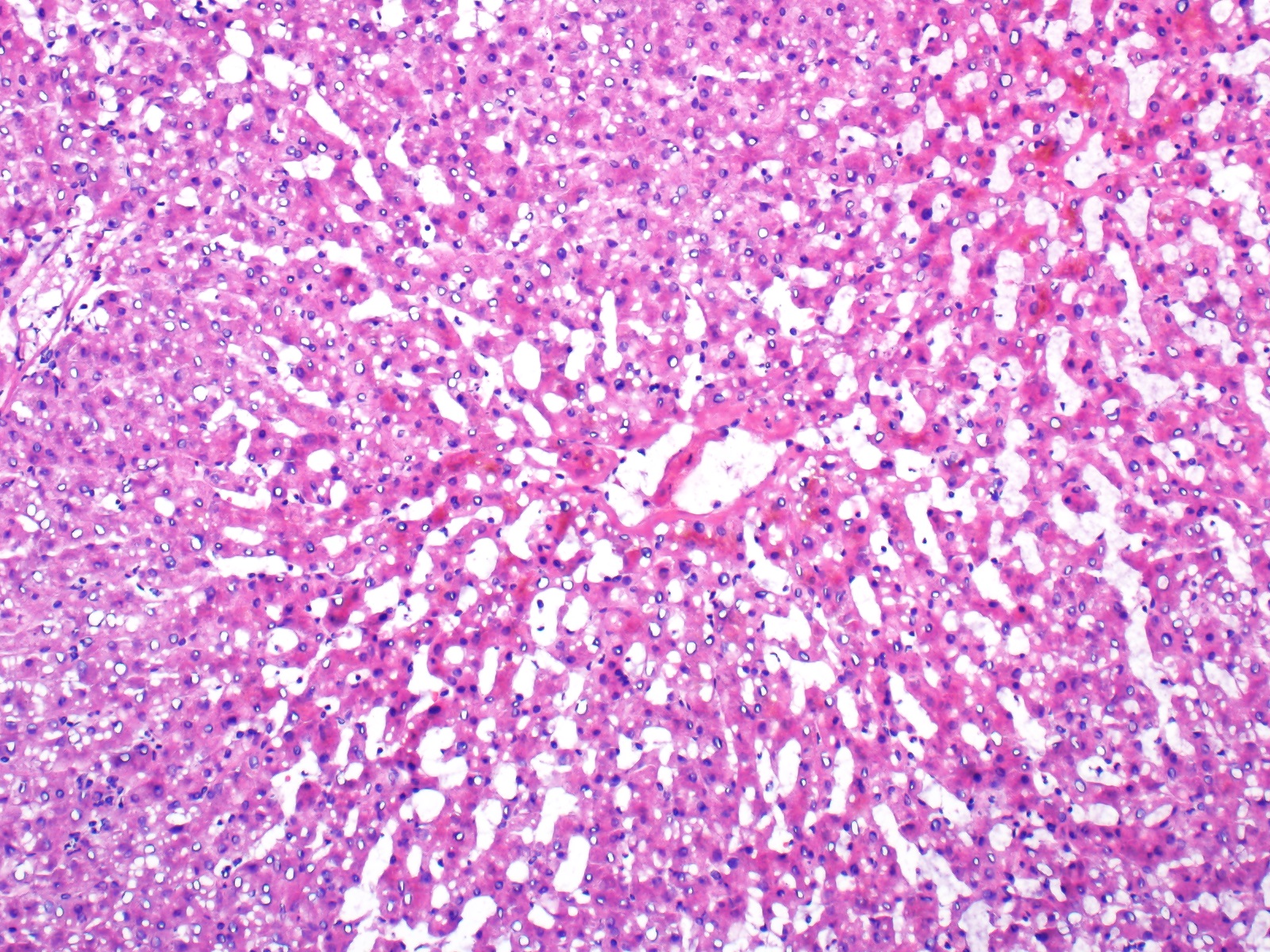
- Central hepatic veins: lined by endothelium; lack valves
- Portal triad / portal tract
- Hepatic artery: lined by endothelium and a thin muscular layer, approximately the same diameter as a bile duct
- Portal vein: lined by endothelium
- Bile duct: lined by cuboidal epithelium, approximately the same diameter as a hepatic artery
- Normal portal tracts will not always show an artery, vein and bile duct; some will show multiple artery or duct faces (Hepatology 1998;28:323)
- Lymphatics: not normally seen on H&E
- May contain few lymphocytes, macrophages, mast cells and eosinophils
- Tend to be more fibrotic in subcapsular zone
- 2 concepts for describing microscopic architecture
- Acinus: functional unit centered around portal triad to include surrounding central veins
- Lobule: functional unit centered around central vein to include surrounding portal triads
- Periportal zone / zone 1
- Higher content of oxygen and nutrients
- Highest metabolic activity
- Least susceptible to ischemia and toxic injury
- Midlobular zone / zone 2
- Centrilobular zone / zone 3
- Most susceptible to ischemia and toxic injury
- Periportal zone / zone 1
Contributed by Kimberley J. Evason, M.D., Ph.D.
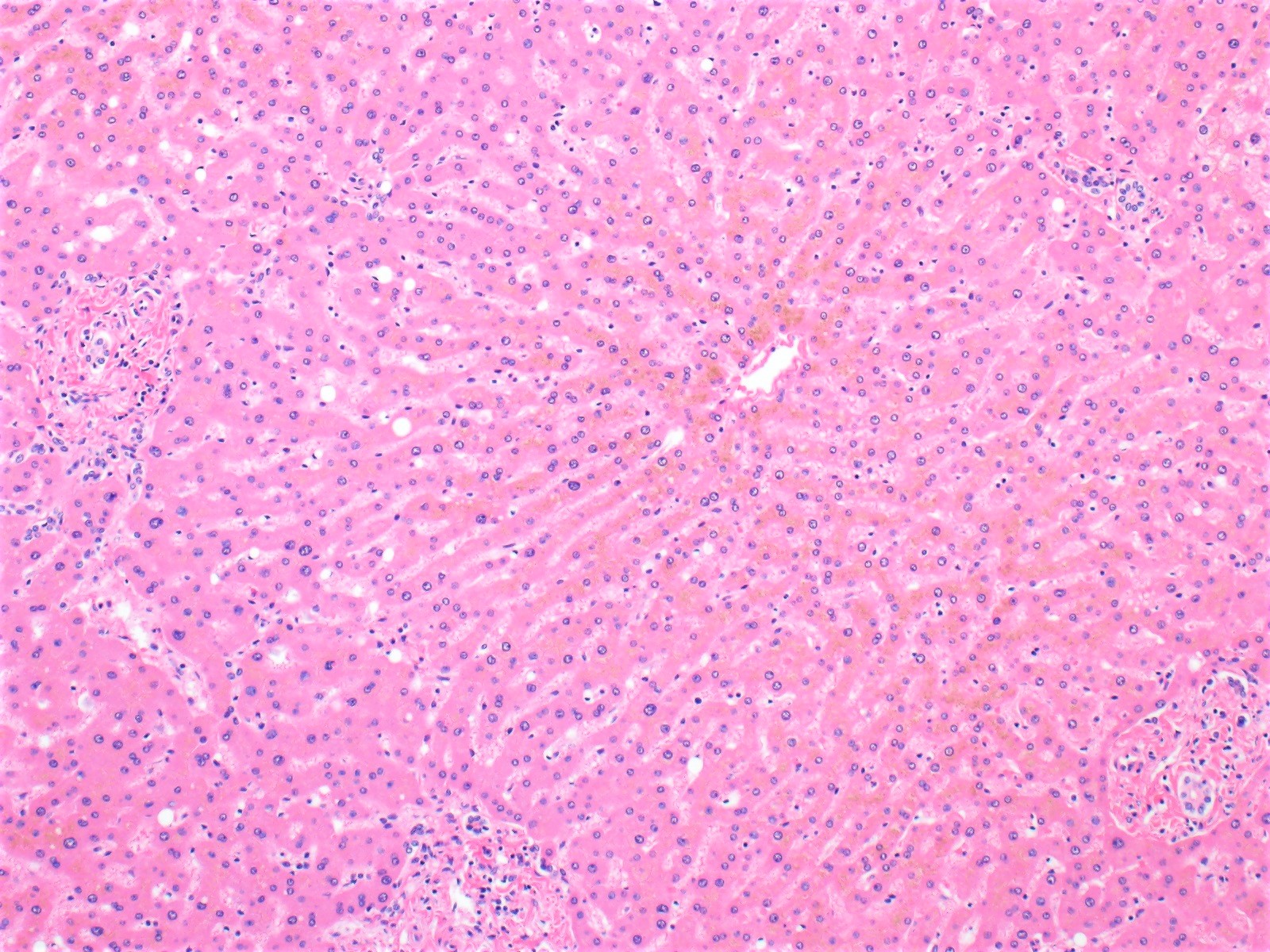
Lobule

Trichrome
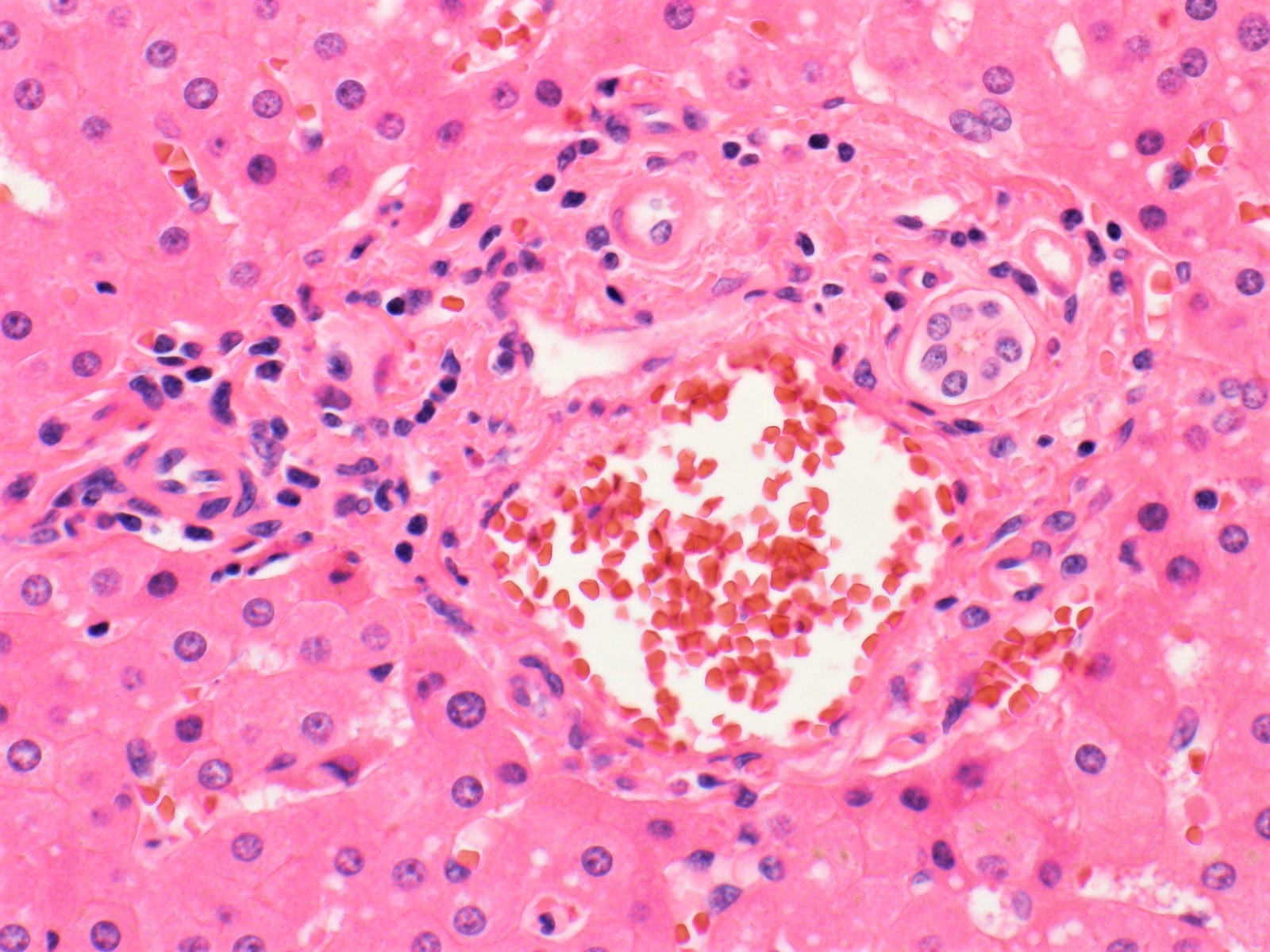
Portal tract
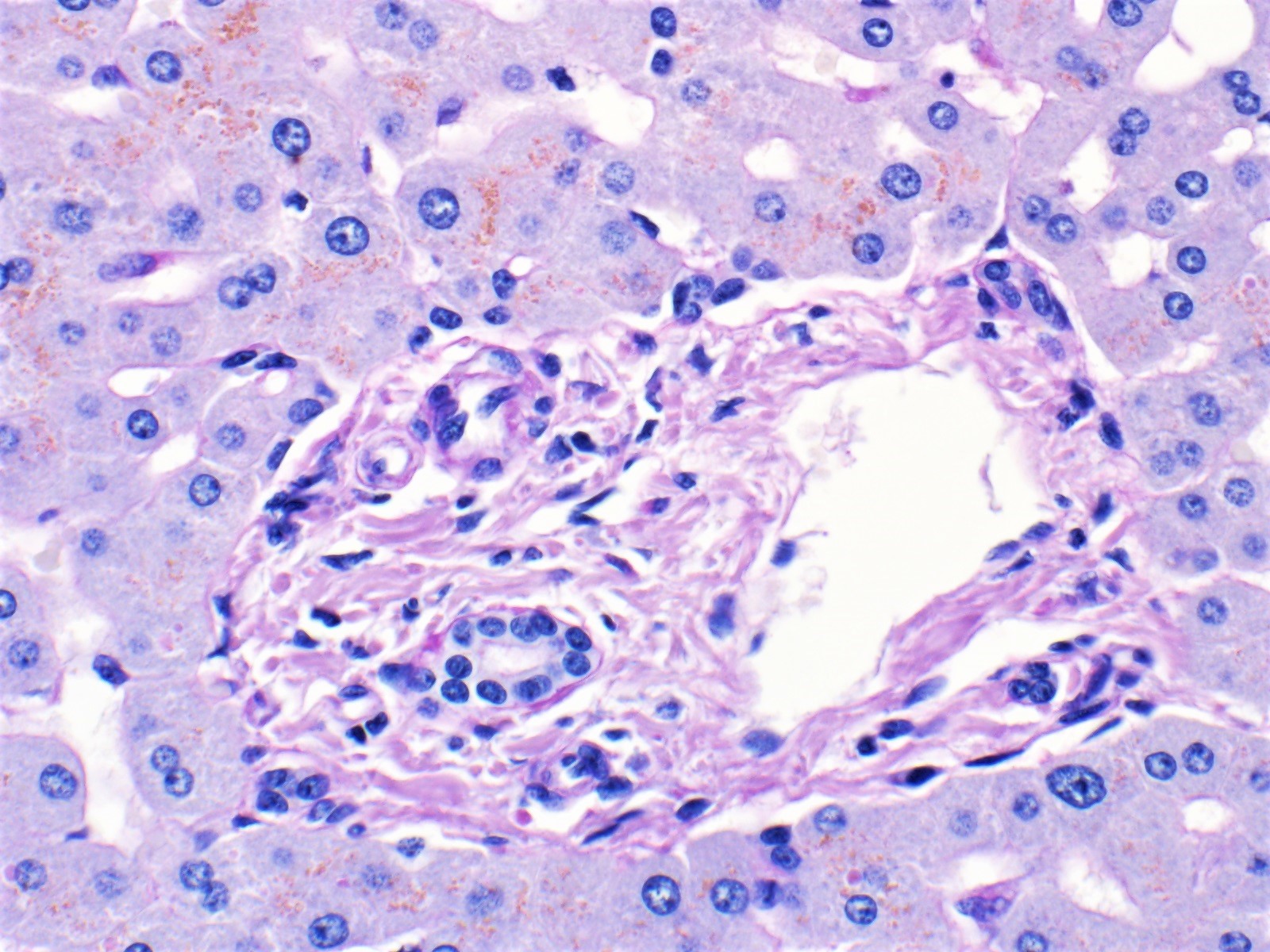
PASD
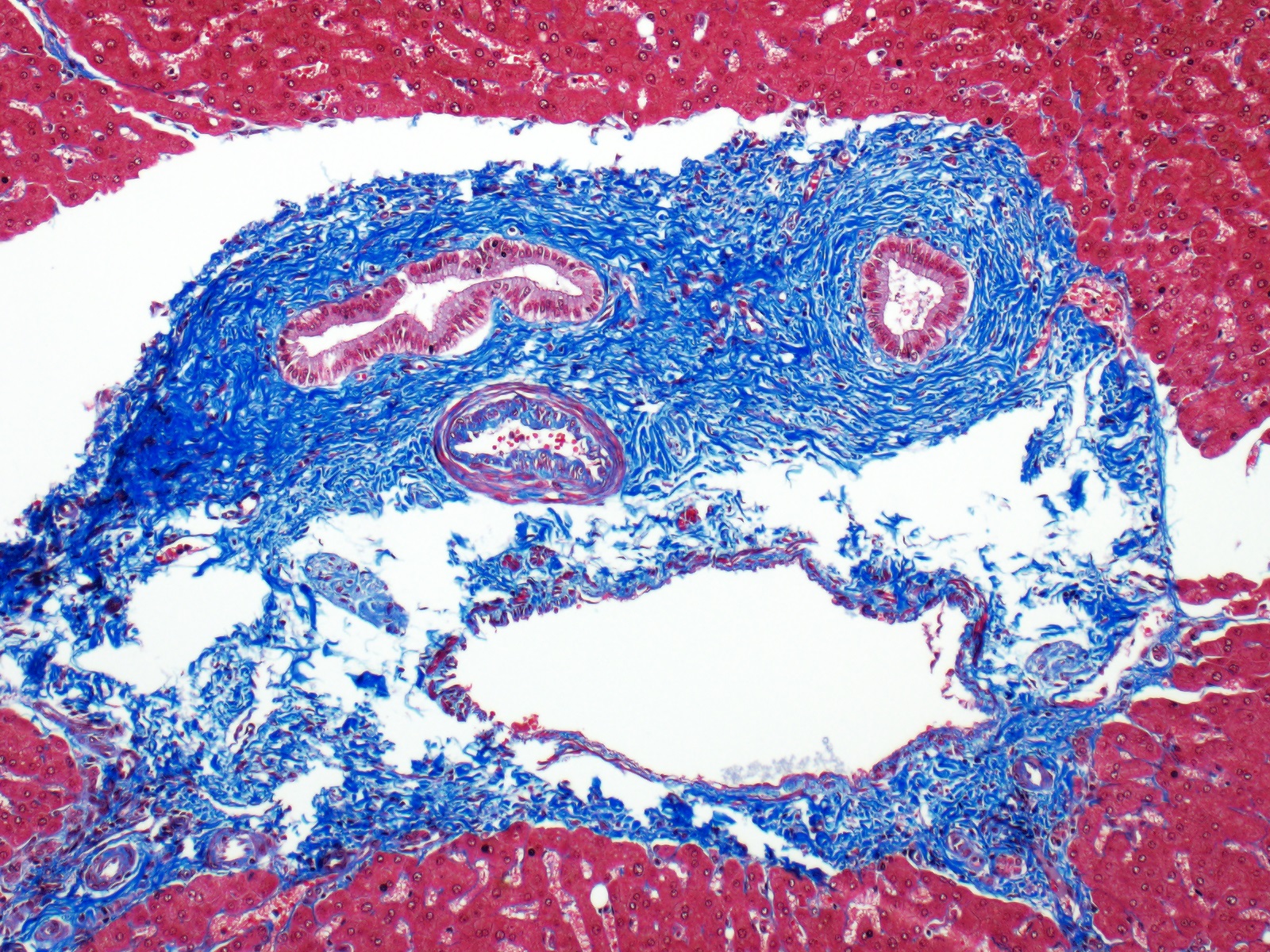
Trichrome large portal tract
Hepatocytes and sinusoids
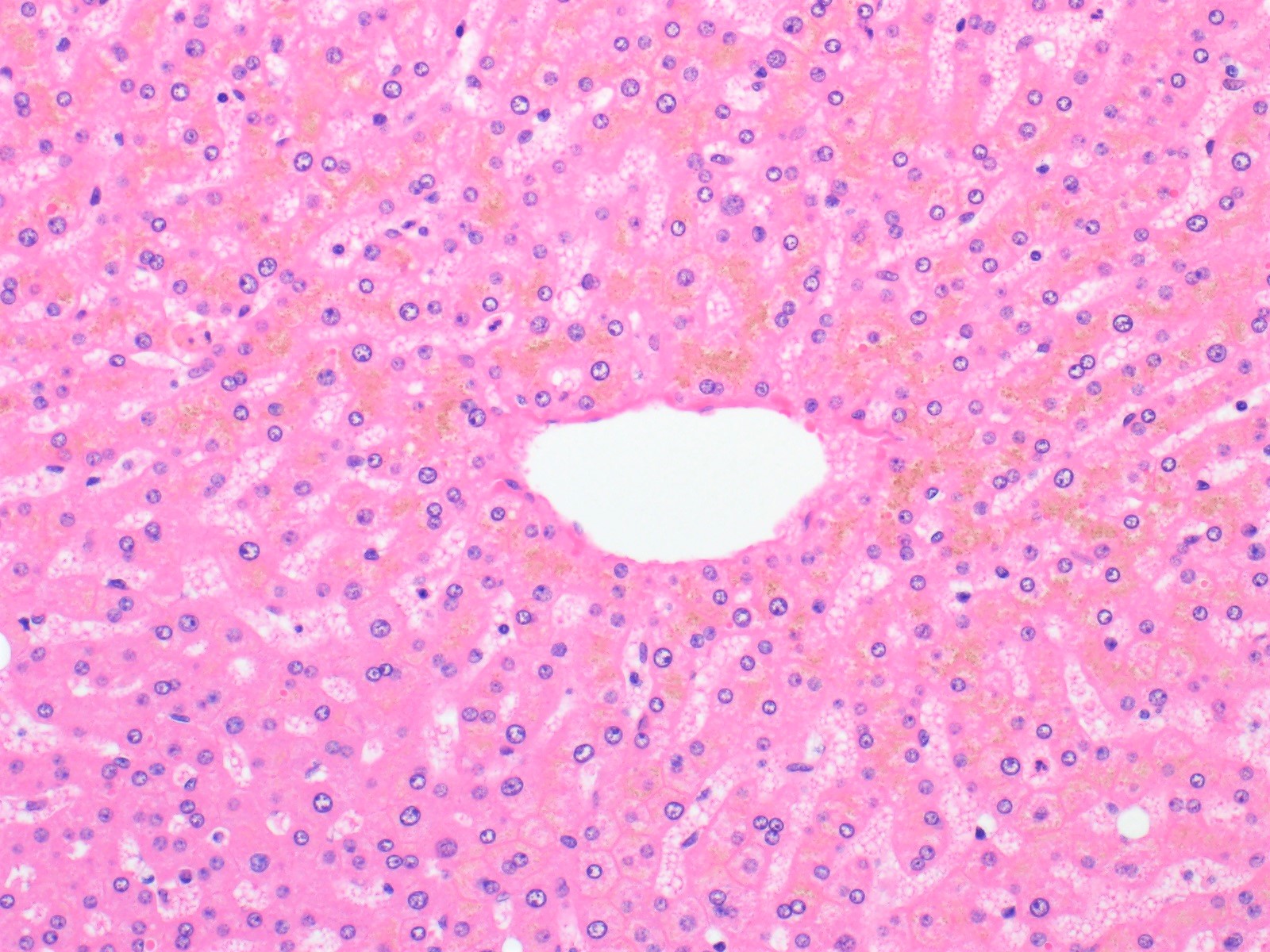
Central vein
Canaliculi
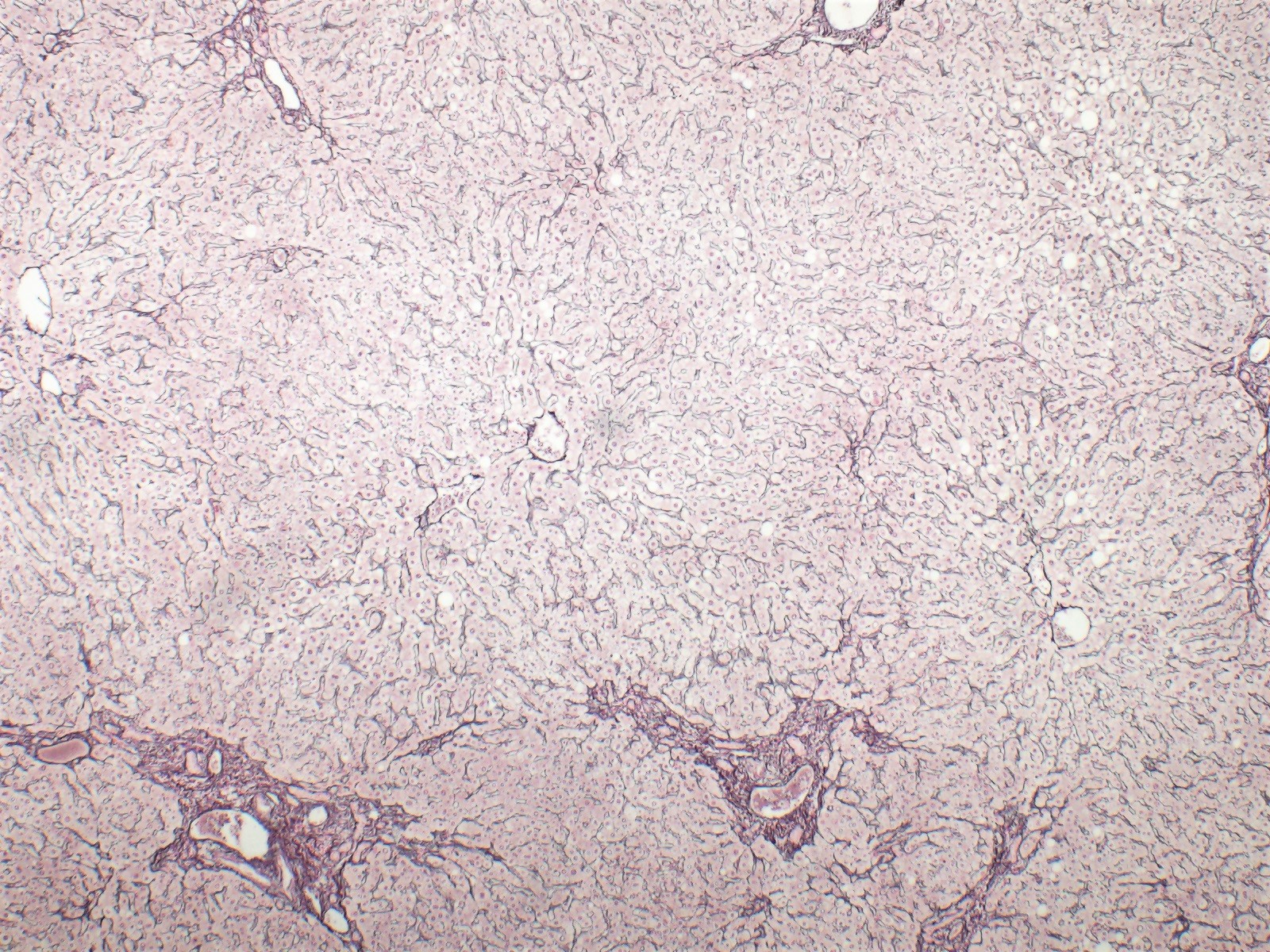
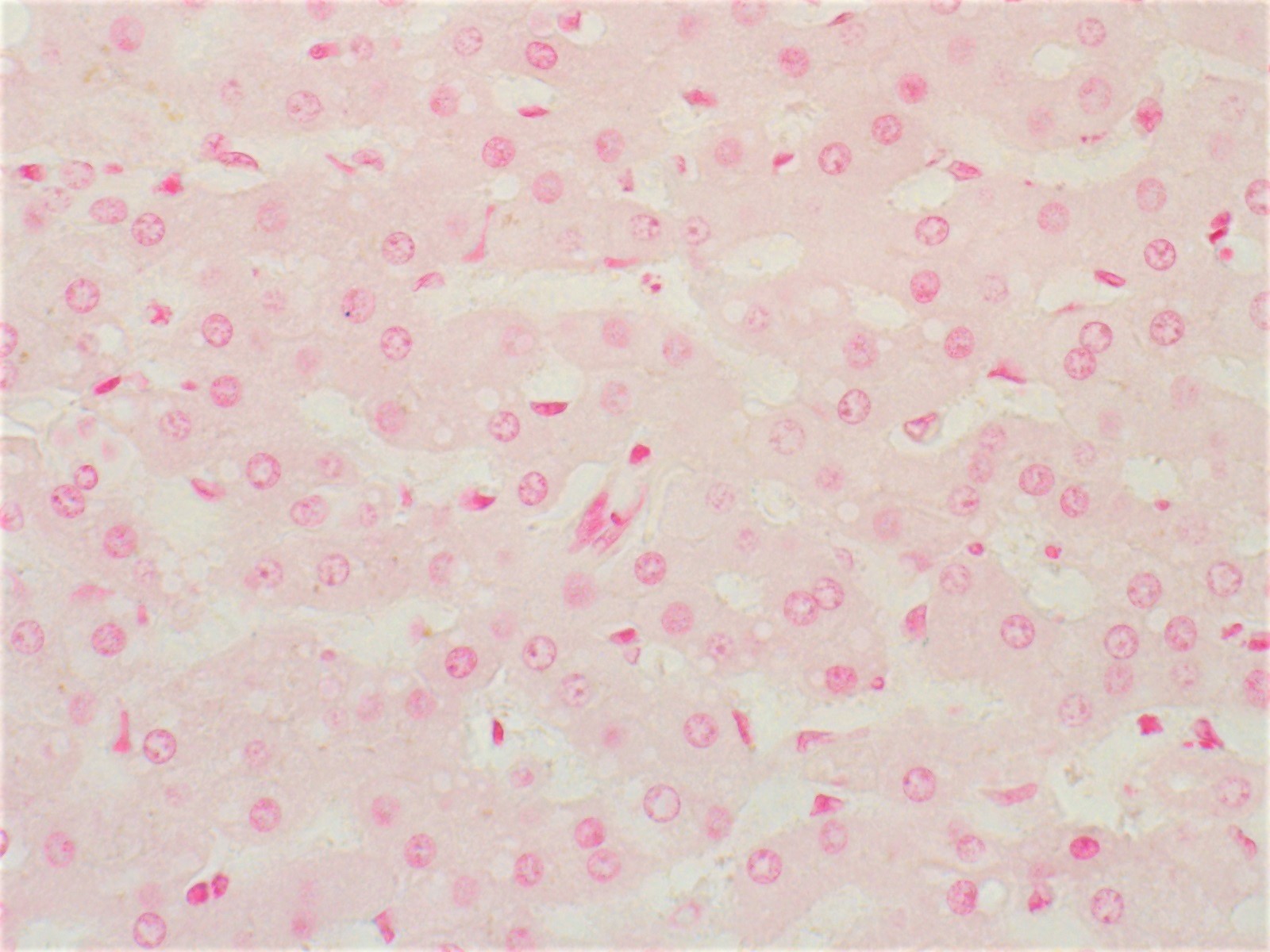
Reticulin
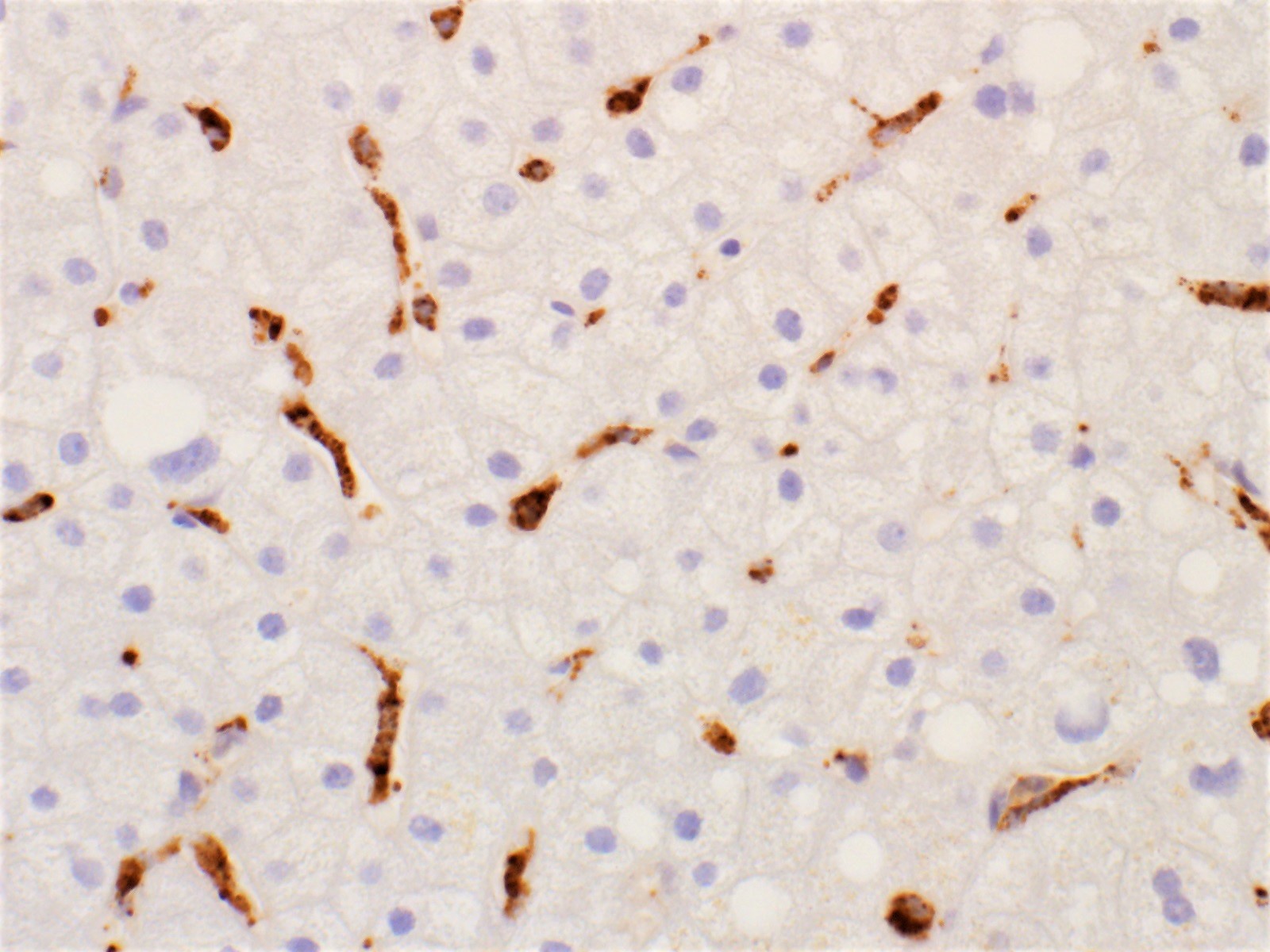
Kupffer cells
Iron
- Hepatocytes
- Polygonal to round cells with abundant dense granular to vacuolated cytoplasm and round, centrally located nuclei with prominent nucleoli
- Arranged singly in 2 dimensional clusters or trabeculae 2 - 3 cell layers thick
- Cholangiocytes (bile duct epithelial cells)
- Cuboidal to columnar cells with scant pale cytoplasm and small, round nuclei with inconspicuous nucleoli
- Arranged in picket fences with nuclear palisading or monolayered honeycomb sheets
- Endothelial cells: rarely seen
- Kupffer cells: rarely seen
- Reference: Cytojournal 2005;2:7
Contributed by Kimberley J. Evason, M.D., Ph.D.
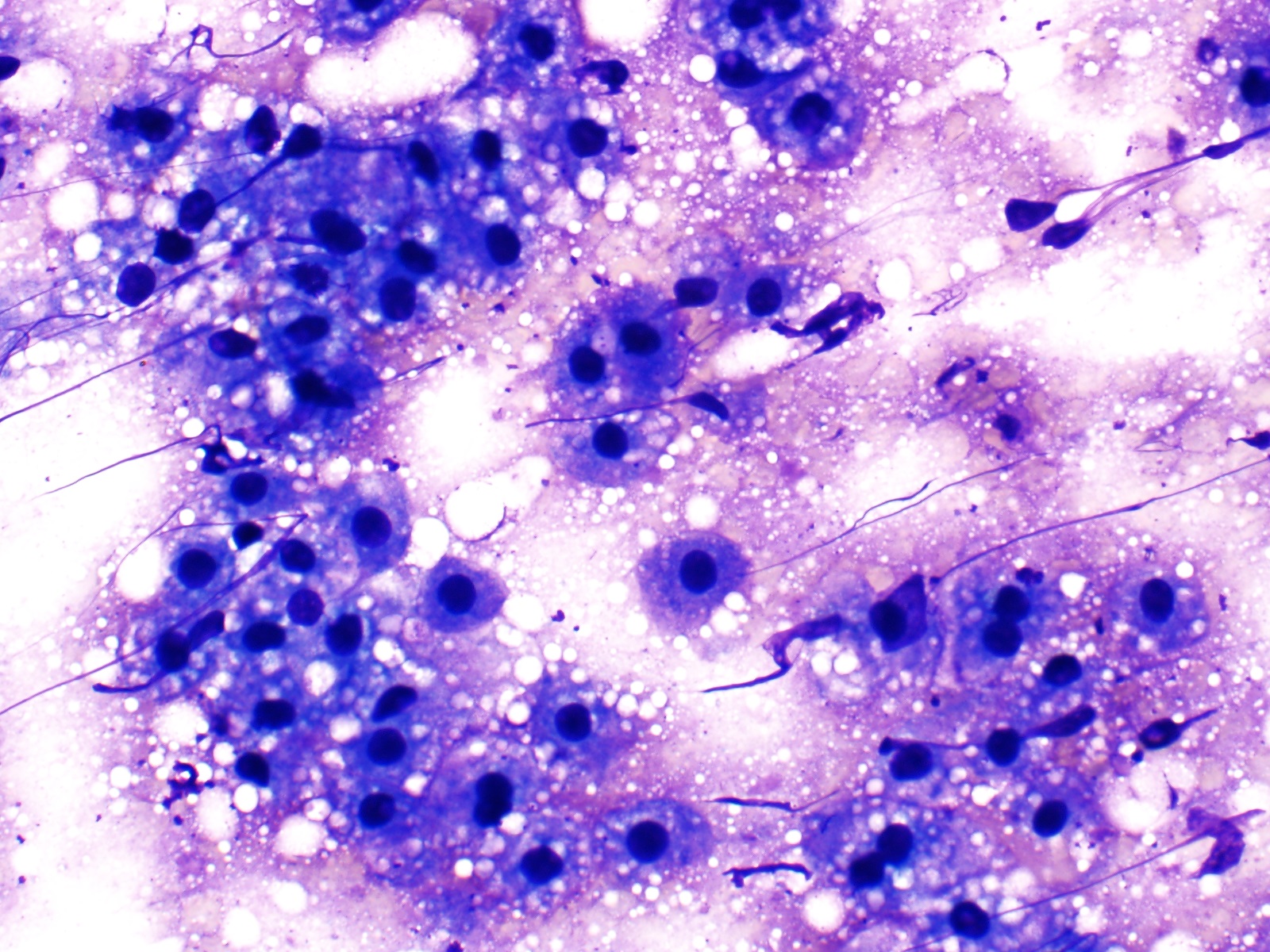
Benign hepatocytes, Diff-Quik
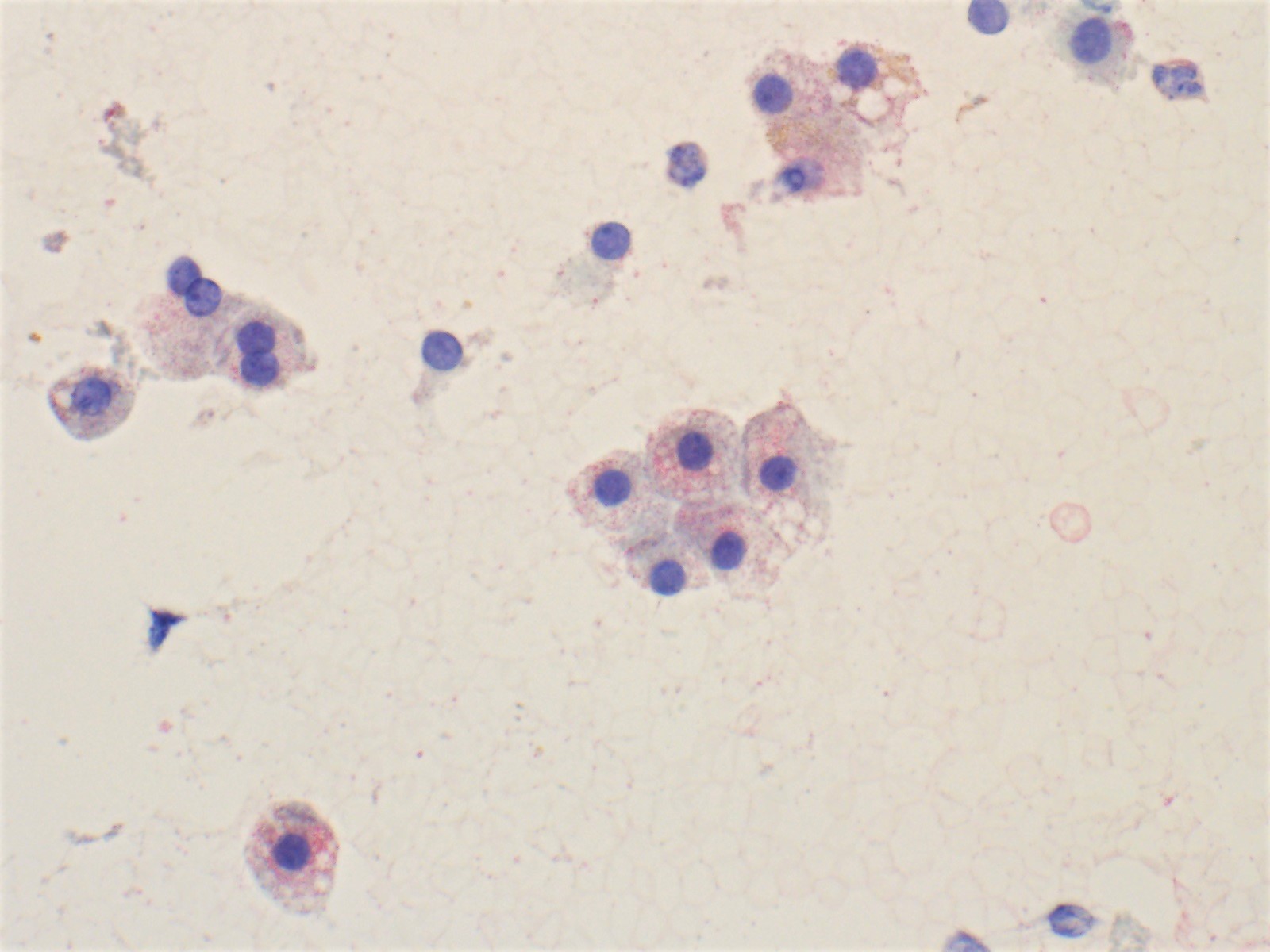
Benign hepatocytes, Pap
- Hepatocytes: HepPar1, CAM5.2, CD10 (bile canaliculi), polyclonal CEA (bile canaliculi) (Manual of Surgical Pathology 2006;71)
- Cholangiocytes: CK7, CK19, AE1 / AE3
- Kupffer cells: CD68
- Routine stains:
- Trichrome: highlights collagen fibers to assess and stage fibrosis
- Reticulin: highlights reticulin fibers to assess hepatic plates for expansion or collapse
- Periodic acid-Schiff (PAS): highlights glycogen
- Periodic acid-Schiff with diastase (PASD):
- Highlights the basement membrane of bile ducts and ductules
- Stains abnormal alpha-1 antitrypsin globules in hepatocytes in the setting of alpha-1 antitrypsin deficiency
- Iron: aids in evaluating iron deposits in hepatocytes and Kupffer cells
- Hepatocytes: CK7, CK19
- Cholangiocytes: HepPar1 (J Hepatobiliary Pancreat Sci 2012;19:289)
- Kupffer cells, endothelial cells, hepatic stellate cells, sinusoids, bile canaliculi, the space of Disse and intracellular components like mitochondria may be visualized with electron microscopy
- Limited use diagnostically except in the evaluation of some metabolic disorders
- References: World J Gastroenterol 2010;16:2851, Compr Physiol 2013;3:1035
Images hosted on other servers:

Endothelium, tangential cut

Bile canaliculus
Development of foregut related to the peritoneum
Liver anatomy (function, topography, external structures, ligaments)
Anatomy of the abdominal viscera: liver, bile ducts and gallbladder
Anatomy dissection of liver
What is the pigment seen in the image above?
- Bile
- Hemosiderin
- Lipofuscin
- Melanin
Comment Here
Reference: Liver - Anatomy & histology
- Albumin
- Alkaline phosphatase
- Aspartate transaminase
- Bilirubin
Comment Here
Reference: Liver - Anatomy & histology
