

Lung
Mesenchymal tumors
Pleuropulmonary blastoma
Author: Erdener Özer, M.D., Ph.D.
Editorial Board Member: Andrey Bychkov, M.D., Ph.D.

Last author update: 1 March 2017
Last staff update: 14 September 2023
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: pleuropulmonary blastoma pathology [TIAB]

Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Radiology description | Prognostic factors | Case reports | Treatment | Gross description | Gross images | Microscopic (histologic) description | Microscopic (histologic) images | Virtual slides | Cytology description | Positive stains | Negative stains | Differential diagnosis | Additional referencesCite this page: Ozer E. Pleuropulmonary blastoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lungtumorPPB.html. Accessed April 20th, 2024.
Definition / general
- Pleuropulmonary blastoma (PPB) is a rare, primitive primary neoplasm of the thorax in young children
- The tumor, which is often but not always associated with cystic lung lesions, may arise in pulmonary parenchyma, the mediastinum and pleura
- It was initially proposed to be a distinct entity in 1988 (Cancer 1988;62:1516)
- An international registry has been established (ppbregistry.org)
Essential features
- Three subtypes of PPB exist (Types I, II and III), and are a continuum from the least to most malignant lesions (Cancer 2015;121:276, Pediatr Dev Pathol 2015;18:504)
- Type I is multicystic; it is now considered the same clinical and pathologic entity as CPAM (congenital pulmonary airway malformation) type IV (Neonatology 2017;111:76)
- Type II shows thickening areas (nodules) within this cystic lesion
- Type III shows solid masses
Terminology
- PPB
- Pneumoblastoma
- Mesenchymal cystic hamartoma
- Cystic mesenchymal hamartoma
- Pulmonary rhabdomyosarcoma
- Rhabdomyosarcoma in lung cyst
- Pediatric pulmonary blastoma
ICD coding
- M8973/3
Epidemiology
- PPB is encountered in childhood, mostly in the first years of life (90% are between 0 - 2 years old)
- Type I may be found in very young children (birth to 2 years of age)
- Types II and III tend to be found after 2 years of age (Pediatr Dev Pathol 2015;18:504)
Sites
- PPB may arise in the lung, mediastinum and pleura
Pathophysiology
- It arises from a primitive mesenchymal cell, likely a stem cell (Am J Surg Pathol 2008;32:282)
Etiology
- PPB is associated with PPB family tumor and dysplasia syndrome in 33% of cases
- Many of these patients have a mutation of the DICER1 gene (Cancer 2015;121:276)
Clinical features
- Children usually present with difficulty breathing or other respiratory problems including persistent pneumonitis, coughing or atelectasis
- 10% may also present with multilocular cystic nephroma and very rarely, Wilms tumor
Diagnosis
- MRI or CT can help diagnose, but biopsy is suggested
Radiology description
- Findings that favor PPB are a right sided, pleural based, peripherally located mass (Cancer Imaging 2009;9:1)
Prognostic factors
- The prognosis of PPB, especially Types II and III is poor because of frequent relapses and distant metastases which are often seen in the brain and bone (Pediatr Pulmonol 2015;50:698)
Case reports
- A neonate with pleuropulmonary blastoma and myelomeningocele (Fetal Diagn Ther 2016;39:234)
- 8 month old infant with difficulty feeding and shortness of breath (Case of the Week #166)
- 2 year old infant that first manifested as recurrent pneumothorax (J Pediatr Hematol Oncol 2012;34:e42)
- 3 year old boy with Type III PPB (Turk Patoloji Derg 2015;31:68)
- 44 month old child with PPB presenting as a solid and cystic mass (Fetal Pediatr Pathol 2014;33:1)
Treatment
- At present, the treatment of PPB is multimodal and includes surgery, chemotherapy or radiation therapy
- The combination depends on the type and aggressiveness of the disease (Pediatr Pulmonol 2015;50:698)
Gross description
- Type I PPB is a peripherally located, multicystic and thin walled structure
- Type II PPB is a mixed solid and cystic tumor characterized by variable thickened or nodule-like areas
- Type III PPB is characterized by a well circumscribed, mucoid, white-tan solid mass attached to the pleura and involves a lobe or entire lung; necrosis and hemorrhage may be present in the friable areas
Gross images
Contributed by Erdener Özer, M.D., Ph.D. and Case #166


Type III PPB
Images hosted on other servers:

Type I PPB has
multiloculated cyst
filled with scanty
clear serous fluid
Microscopic (histologic) description
- Type I PPB is a peripherally located, multicystic and thin walled structure
- Type II PPB is a mixed solid and cystic tumor with variable thickened or nodule-like areas
- Type III PPB is an apparently heterogeneous tumor composed of one or more of the following elements:
- Primitive blastema-like small cells with hyperchromatic nuclei, high nuclear to cytoplasmic ratio and abundant mitoses
- Spindled and ovoid cells embedded in a myxoid stroma
- Nodules of immature or malignant chondroid elements
- Isolated or clusters of large anaplastic cells with pleomorphic nuclei, atypical mitotic figures or eosinophilic hyaline bodies
Microscopic (histologic) images
Contributed by Erdener Özer, M.D., Ph.D., Dr. Roopa Arora and Case #166
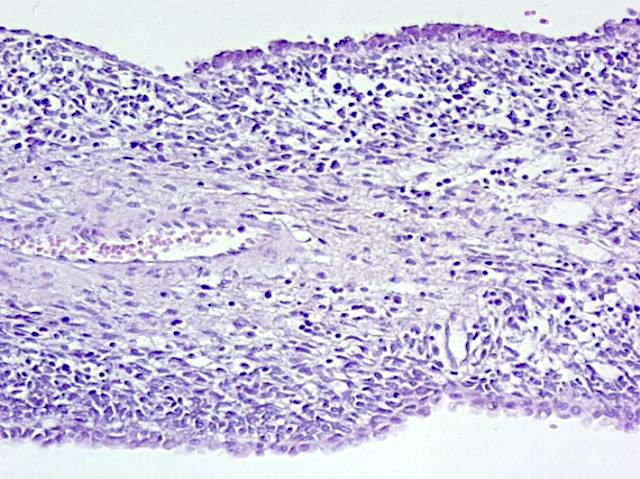
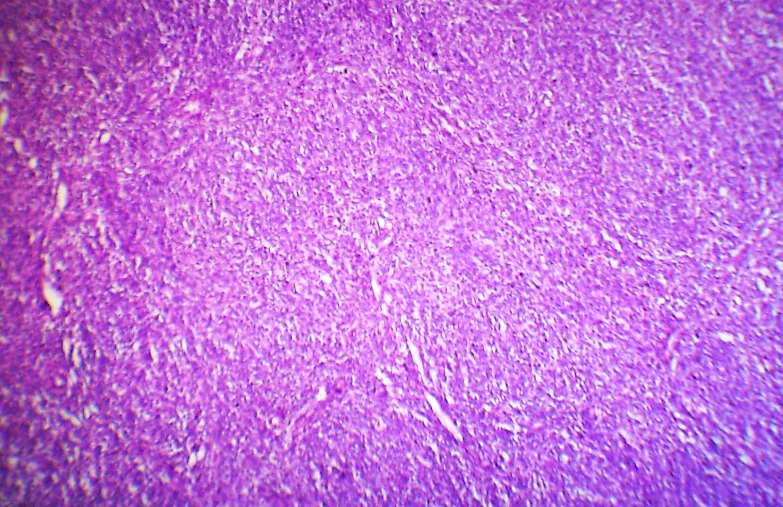
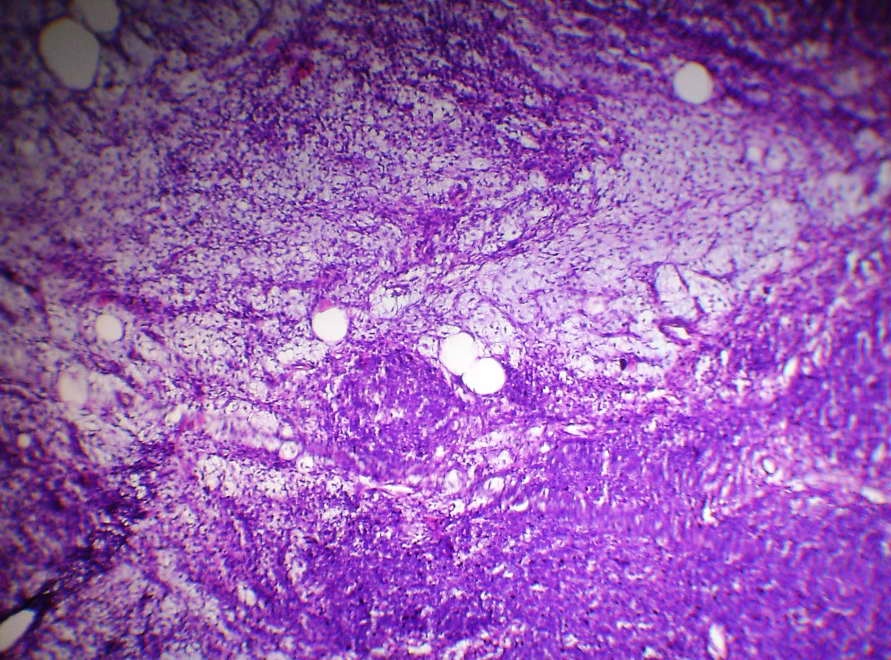
Types I and III PPB
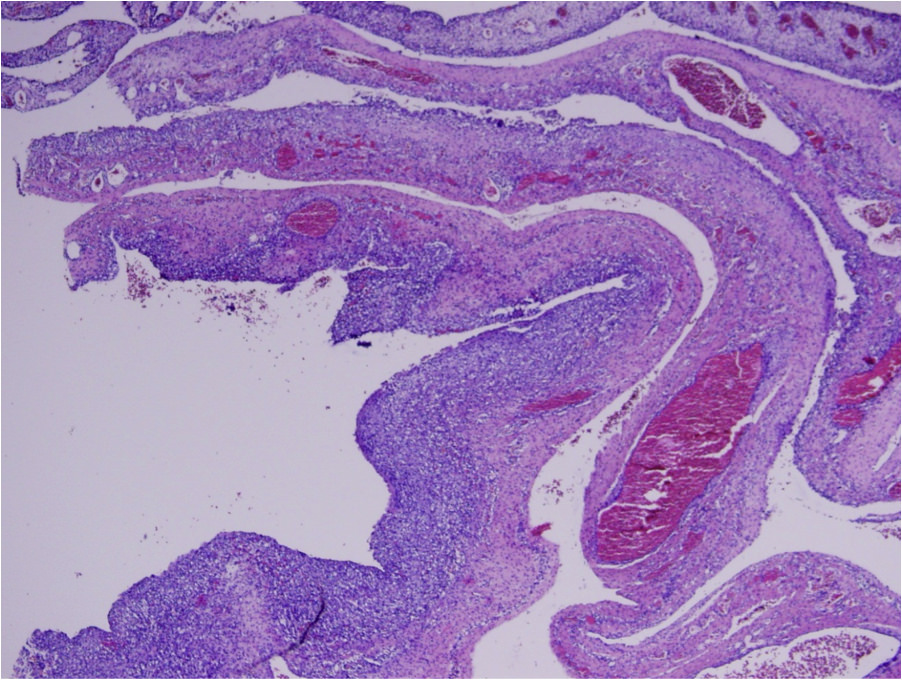
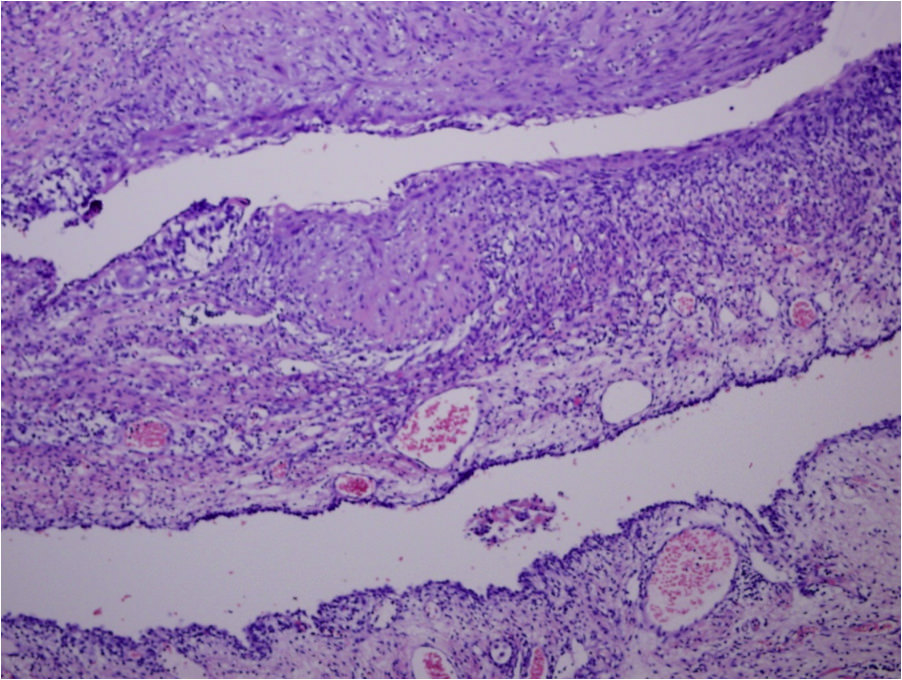
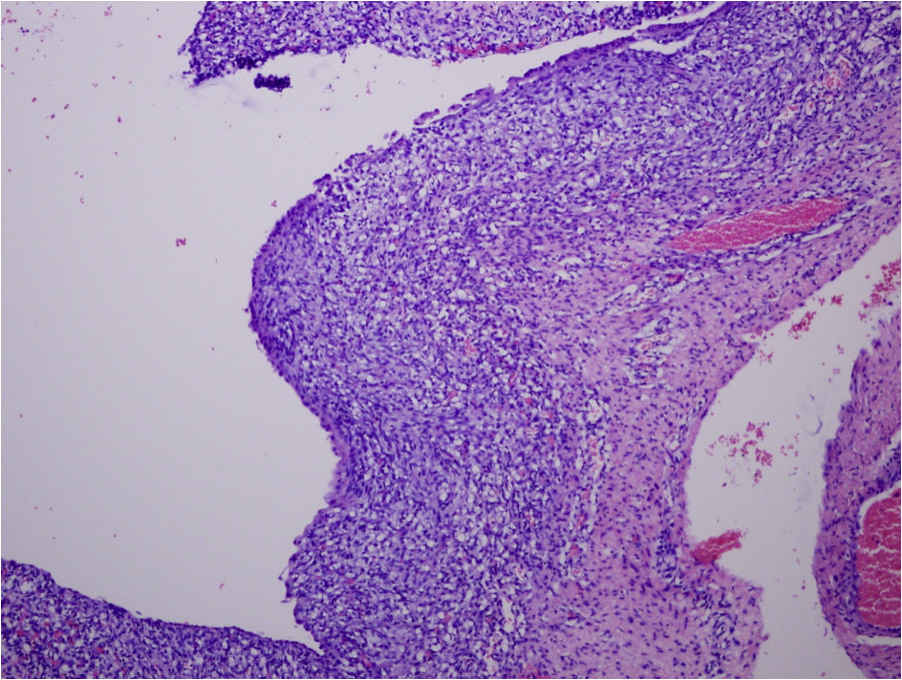
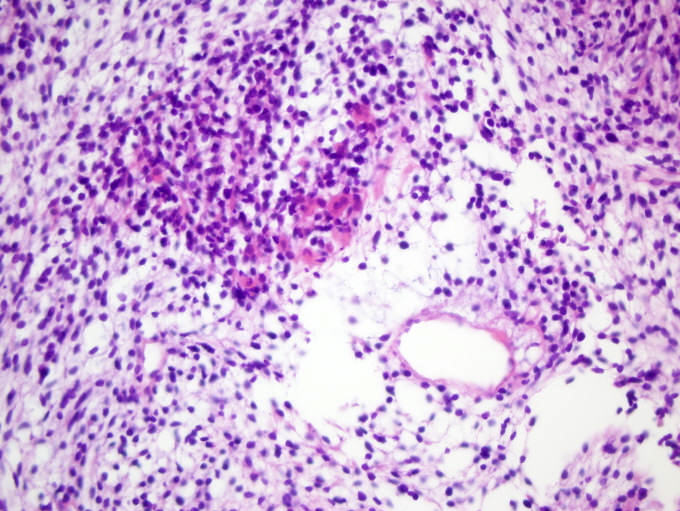
Pleuropulmonary blastoma
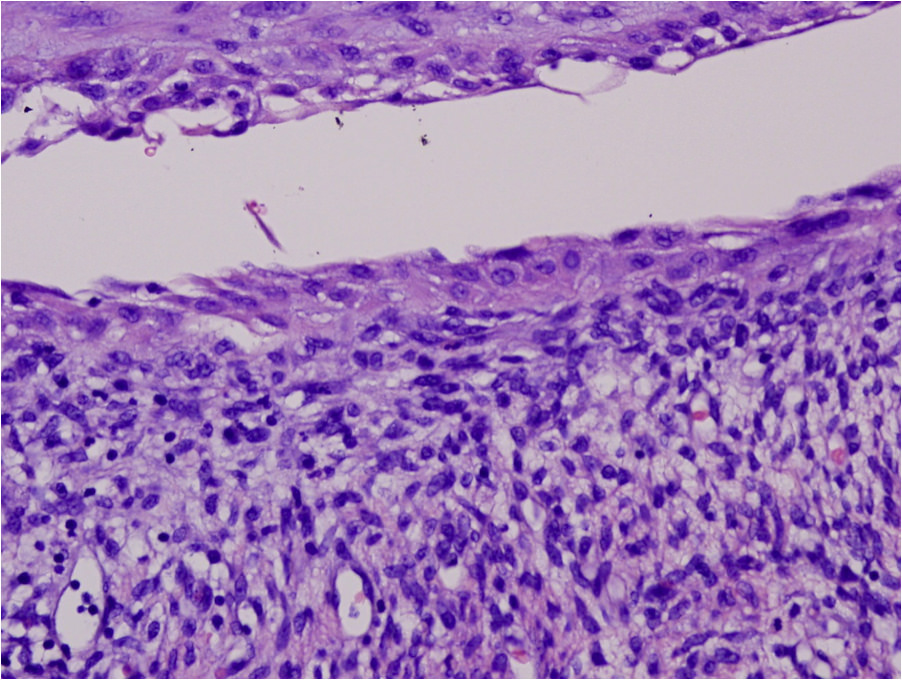
Pleuropulmonary blastoma
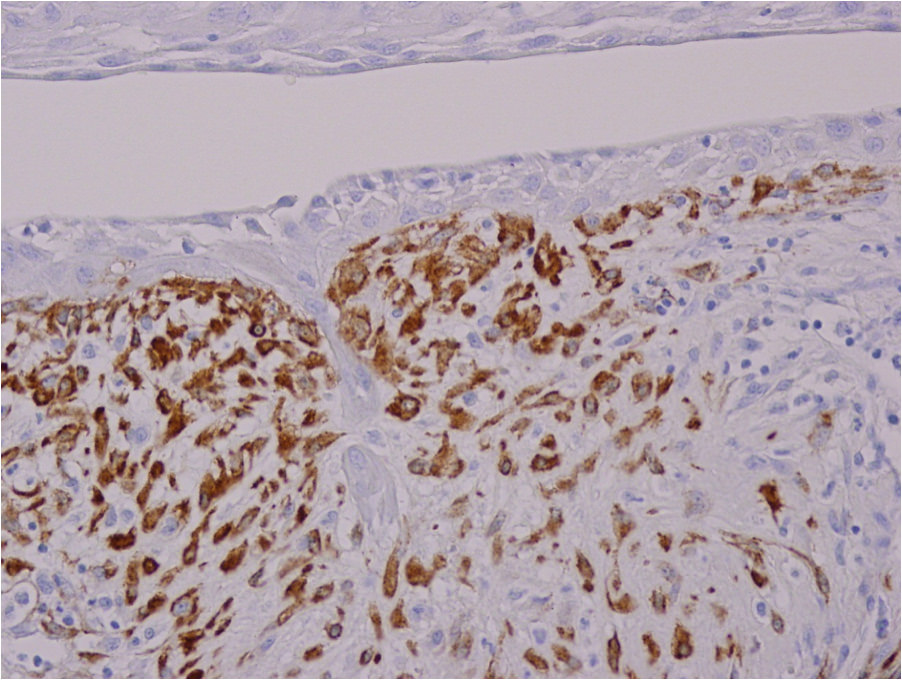
SMA

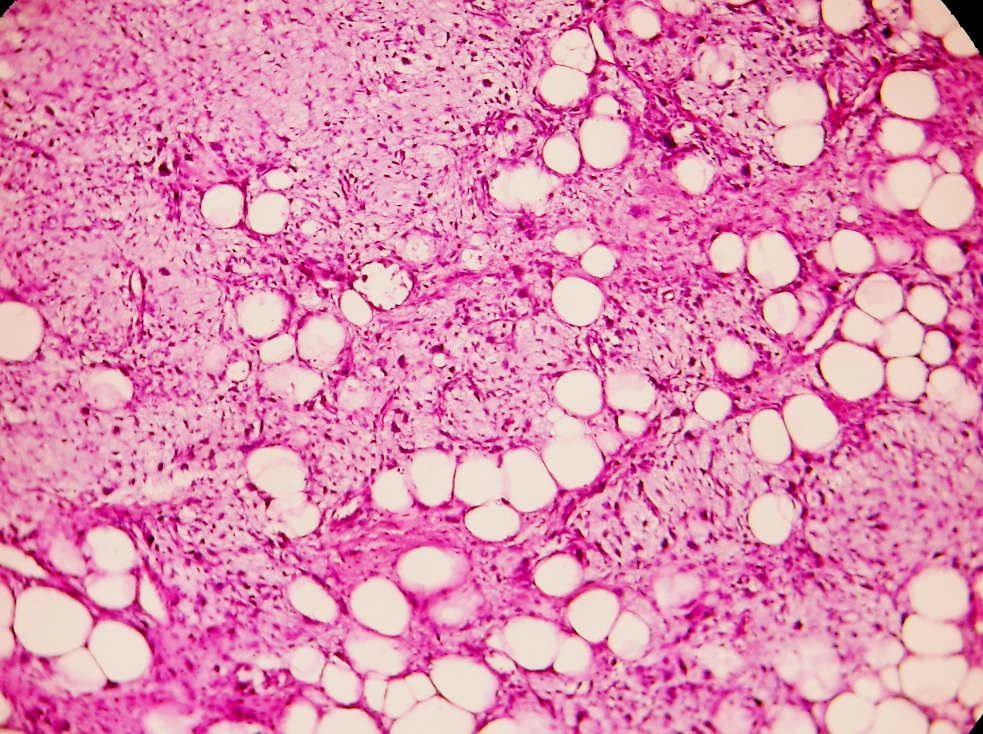
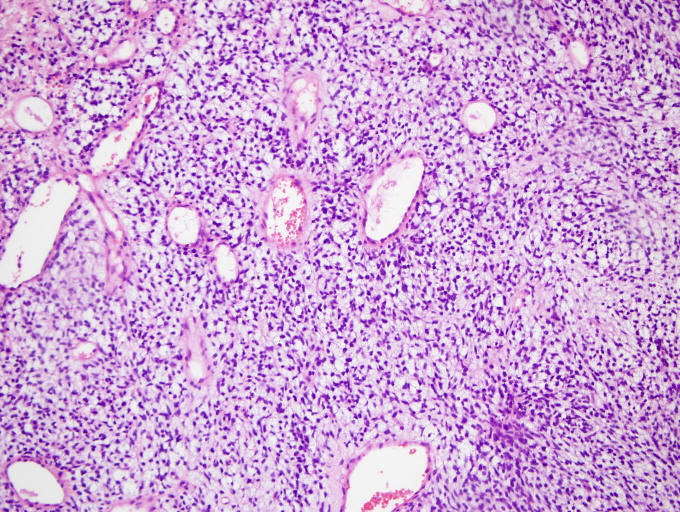
Type III PPB
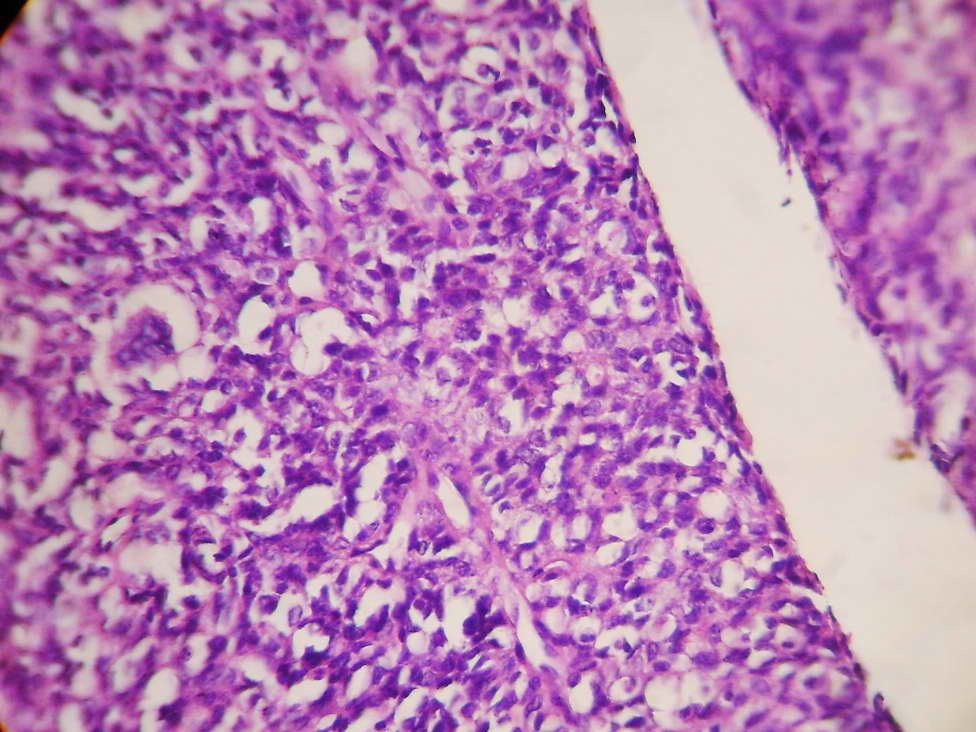
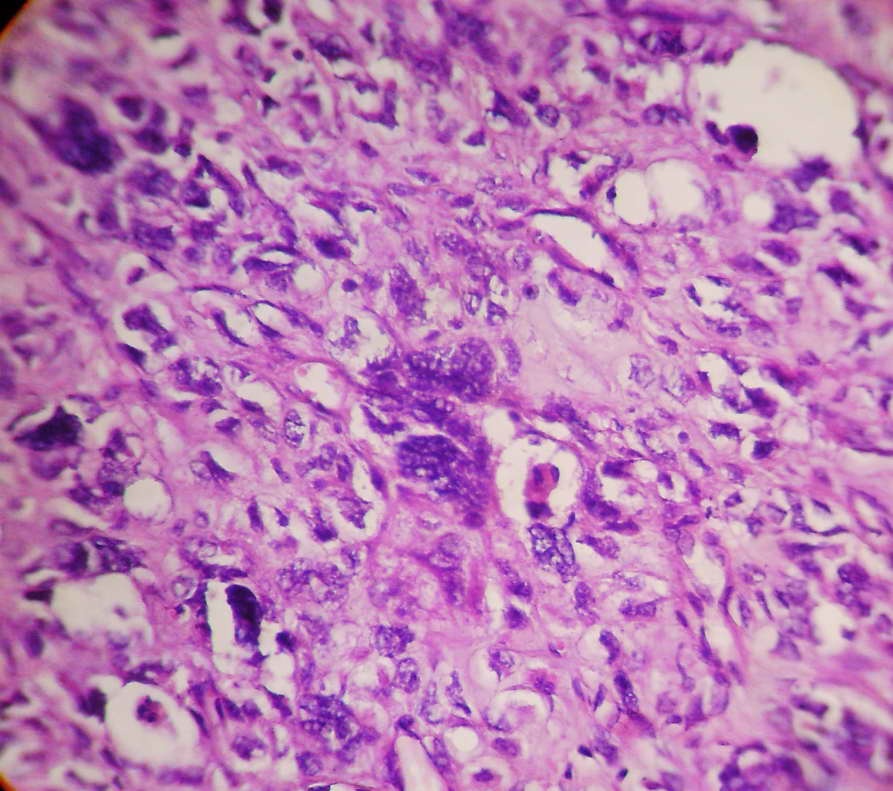

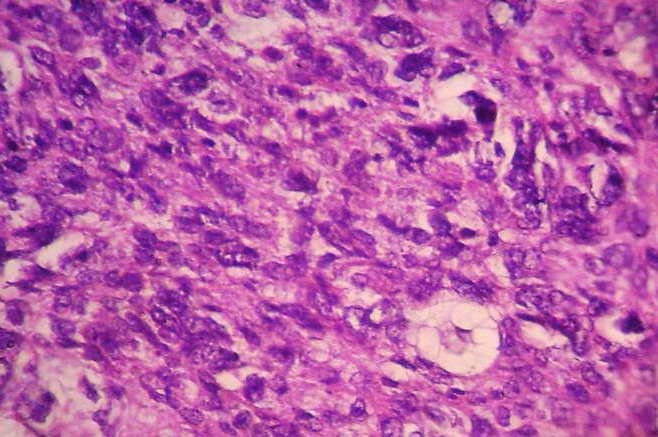
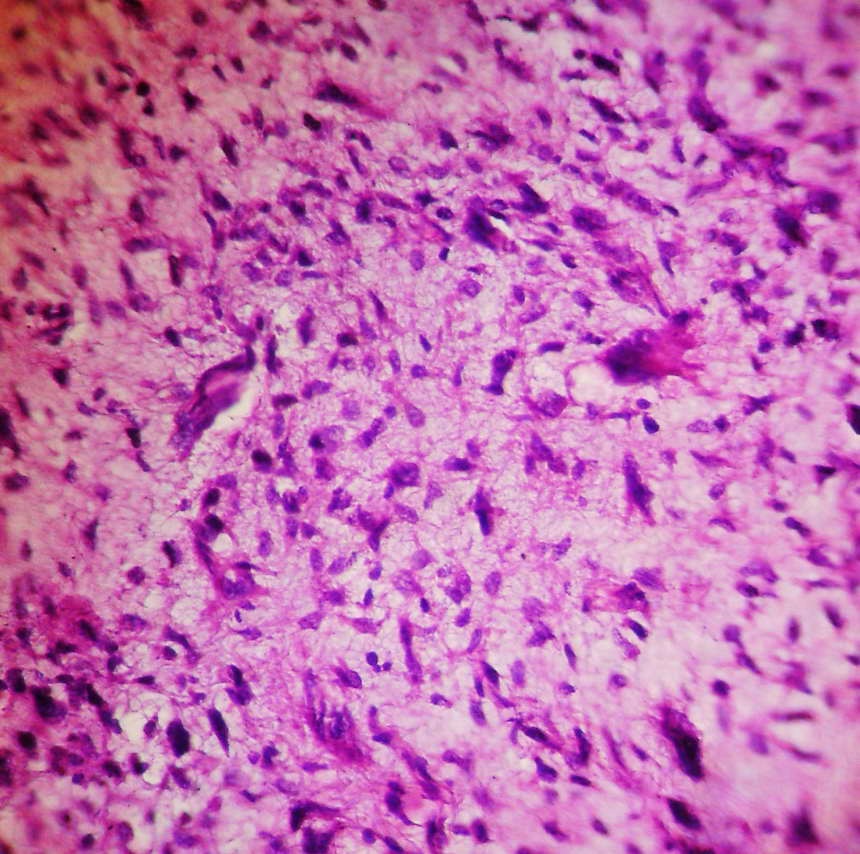
Type III PPB
Virtual slides
Images hosted on other servers:


Cystic pleuropulmonary blastoma
Cytology description
- Cellular smear with both dispersed single cells and cohesive aggregates (Arch Pathol Lab Med 2000;124:416)
- Uniform cells (small round blue cells) may lack cytoplasm, typically display nuclear molding with round or oval nuclei containing darkly stained fine chromatin
- Scattered malignant giant cells have more abundant cytoplasm with indistinct edges and more dispersed chromatin
- Some malignant cells may be spindled with high N/C ratios, eosinophilic cytoplasm and irregular nuclear membranes
- There is no evidence of rosette or glandular formation (Journal of Clinical and Diagnostic Research 2011;5:1656)
Positive stains
- Neoplastic cells: vimentin (diffuse), CD117 (focally), alpha-1-antitrypsin (focally) and CD99 (weakly)
- Surface epithelium: cytokeratin
- Rhabdomyoblasts and primitive cells: muscle specific actin and desmin
Negative stains
Differential diagnosis
- Embryonal rhabdomyosarcoma (for Type III)
- Large bronchogenic cyst / lung cyst (for Type I)
- Other tumors to consider include (for Type III):
- FLIT (fetal lung interstitial tumour)
- Malignant peripheral nerve sheath tumor
- Malignant teratoma
- Mesothelioma
- Monophasic synovial sarcoma
- PNET
- Undifferentiated sarcoma
Additional references
