
Hematology & immune disorders
Primary immunodeficiency disorders
Omenn syndrome
Author: Shamayel Mohammed, M.D.

Last author update: 1 December 2015
Last staff update: 14 June 2022
Copyright: 2003-2024, PathologyOutlines.com, Inc.
PubMed Search: Omenn syndrome [title] lymph nodes
Table of Contents
Definition / general | Pathophysiology | Clinical features | Diagnosis | Case reports | Treatment | Clinical images | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Cytology images | Positive stains | Differential diagnosis | Additional referencesCite this page: Mohammed, S. Omenn syndrome . PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lymphnodesomennssyndrome.html. Accessed April 20th, 2024.
Definition / general
- Rare, autosomal recessive form of severe combined immunodeficiency (SCID) of infancy
- Recurrent infections, early diffuse erythrodermia, failure to thrive, protracted diarrhea, hepatosplenomegaly, elevated serum IgE and eosinophilia, lymphadenopathy, oligoclonal T cell expansions
- Often recombinase activating gene mutations (Clin Immunol 2005;116:246)
Pathophysiology
- Most common genetic alteration is the partial loss of function for recombinase activating genes RAG (RAG1 and RAG2)
- The RAG genes are essential for gene recombination in the T cell receptor and B cell receptor
- This mutation leads to the Inability to productively rearrange VDJ regions in T cell and B cell receptors, which leads to abnormal T cell proliferation and absent B cells
- As a result, the immune system has difficulty recognizing specific pathogens
- An impaired V(D)J recombination process leads to the generation of a few T cells expanding in the periphery, infiltrating target organs such as skin and gut, resulting in the erythroderma and colitis typical of this syndrome
- The disease is characteristically associated with an oligoclonal expansion of Th2 population
Clinical features
- Recurrent infections
- Early diffuse erythrodermia, failure to thrive, protracted diarrhea, hepatosplenomegaly
- Elevated serum IgE and eosinophilia, lymphadenopathy, oligoclonal T cell expansions
- Suppurative lymphadenitis and disseminated sometimes fatal tuberculosis as a reaction to the immunization for Bacille Calmette-Guerin (BCG)
- Lymphoproliferative disorders associated with Primary Immune Disorders (PID) such as SCID
Diagnosis
- WBC count may be normal or elevated with a predominance of lymphocytes
- Eosinophilia is invariably present
- Molecular studies show presence of an oligoclonal set of activated antigen stimulated Th2 cells
- B cells are absent, and NK cells are present
- Immunoglobulin levels show absent immunoglobulin A (IgA) and immunoglobulin M (IgM), elevated IgE levels, and immunoglobulin G (IgG) that is maternal in origin
- IgG antibodies against T dependent antigens, such as tetanus, are nonprotective
- Specific IgM antibodies, such as isohemagglutinins, are absent
Case reports
- Infant with Omenn syndrome and reticular dysgenesis (J Allergy Clin Immunol 2013;131:1227)
Treatment
- Isolation to prevent infection
- Prophylactic treatment with nystatin, antiviral agents (e.g. acyclovir) or antibiotics may be considered
- Immunosuppression with cyclosporine (Arch Dis Child 2002;87:231)
- Bone marrow or other stem cell reconstitution is first line conventional therapy
- Diagnosis at birth may lead to protection from infection and improve transplantation outcome (Blood 2011;117:3243)
Clinical images
Images hosted on other servers:

Pre- and post-treatment

Alopecia and erythroderma
Microscopic (histologic) description
- Total effacement of nodal architecture with no distinct cortex and no follicles
- Also B cell depletion and accumulation of interdigitating reticulum cells (Am J Surg Pathol 1995;19:1082)
- Hassall corpuscles are poorly formed, and lymphocytes are deficient in the thymus
- Paracortical lymphocytes are absent in the spleen
- The spleen, skin and mucosa associated lymphoid tissues contain only a few scattered CD3+ T lymphocytes, and B cells are totally absent (Blood 1999;94:3468)
- Non caseating granulomatous inflammation with BCG / Bacille Calmette-Guerin lymphadenitis (Am J Clin Pathol 2000;113:703)
- Lymphoproliferative disease associated with primary immune disorders:
- EBV is involved in most cases
- Morphology includes reactive lymphoid hyperplasia, polymorphous infiltrate with immunoblast proliferation and overt lymphoma
- Diffuse Large B-cell Lymphoma (DLBCL) is the most common type of lymphoma
- May present as Fatal Infectious Mononucleosis (FIM)
Microscopic (histologic) images
Contributed by Shamayel Mohammed, M.D.
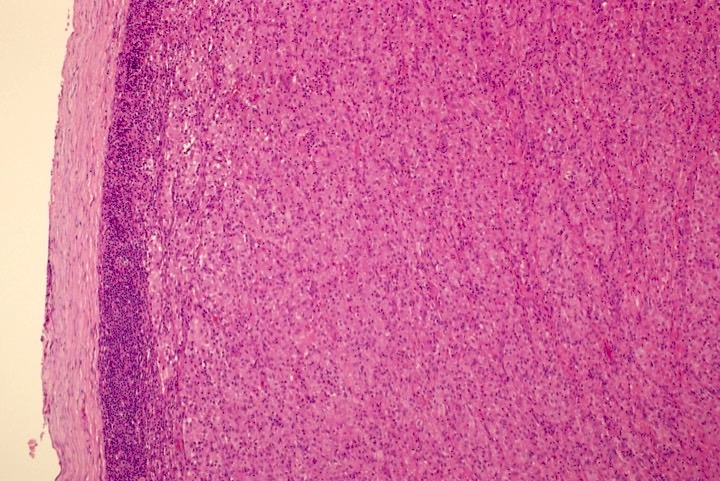
Distinct cortex

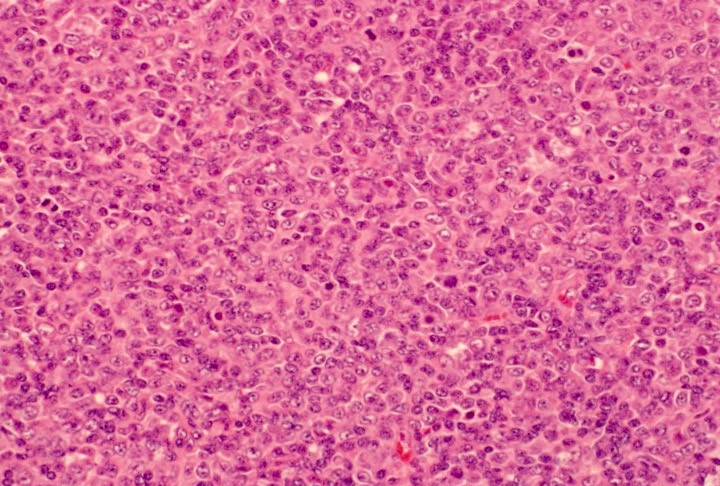
Diffuse histiocytic infiltrate

Patient with SCID
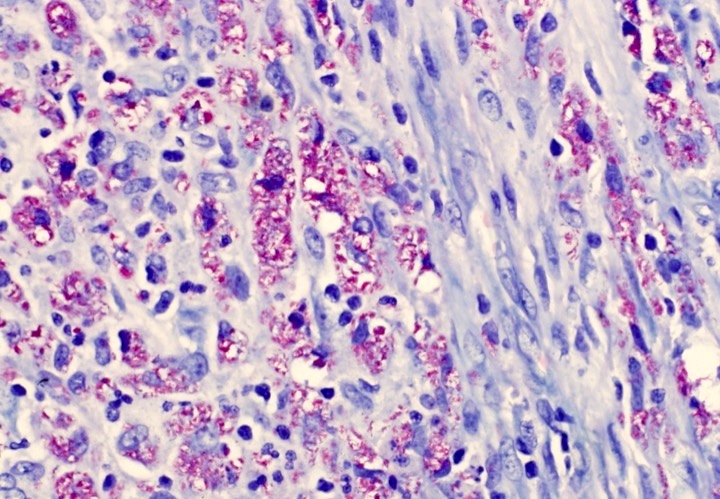
Ziehl Neelsen+
EBV+
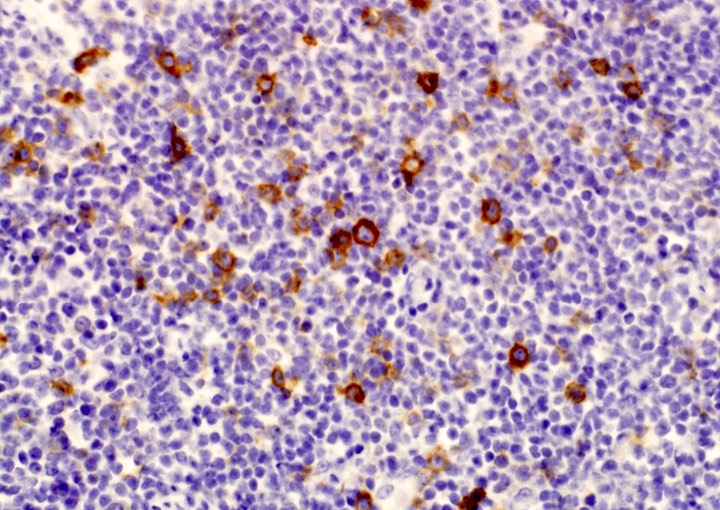
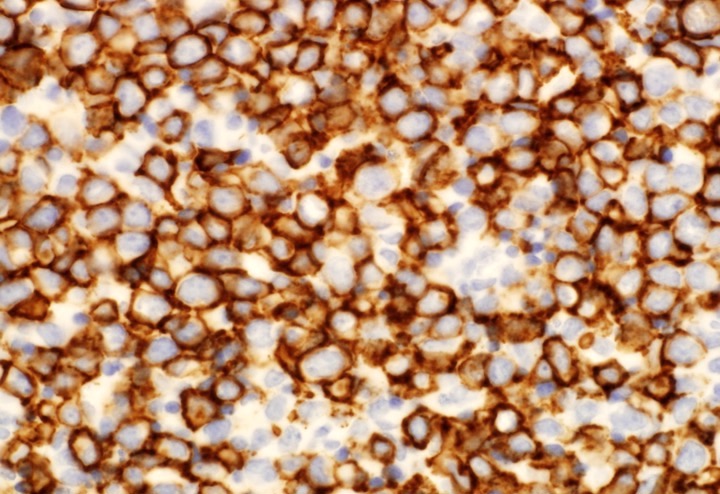
CD30+ immunoblasts
CD20+
Images hosted on other servers:

Parakeratosis and lymphohistocytic infiltrate

H&E, S100

CD30
Cytology description
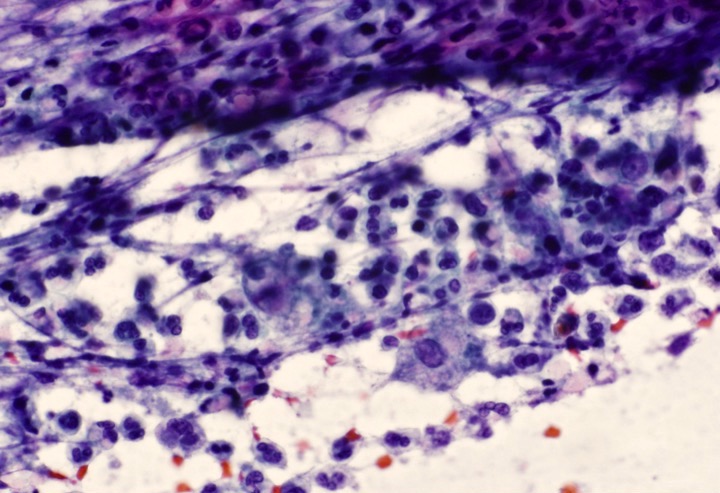
- Large number of histiocytes with abundant streaked cytoplasm
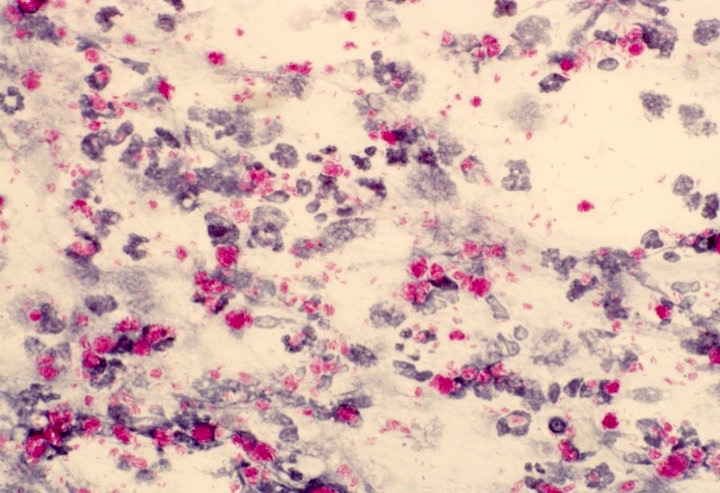
- Ziehl-Neelsen (ZN) stain for acid-fast bacilli positive (Diagn Cytopathol 2001;24:333)
Cytology images
Contributed by Shamayel Mohammed, M.D.
Ziehl-Neelsen+
Histiocytes
Positive stains
- Immunohistochemistry staining show T lymphocyte (CD3+) proliferation
- Majority of the cells express CD30 (Sultan Qaboos Univ Med J 2007;7:133)
- EBV positive in associated lymphoproliferative disorders
Differential diagnosis
- Eczema associated with diarrhea raises the possibility of a food allergy
- Hyperimmunoglobulin E (HIE) syndrome
- T-cell disorders
- Topical dermatitis
