
Lymphoma & related disorders
Hodgkin lymphoma
CHL lymphocyte depleted
Editorial Board Members: Elizabeth Courville, M.D., Julie Feldstein, M.D.


Last author update: 25 July 2022
Last staff update: 25 July 2022
Copyright: 2002-2024, PathologyOutlines.com, Inc.
PubMed Search: Lymphocyte depleted classic Hodgkin lymphoma
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Pathophysiology | Etiology | Clinical features | Diagnosis | Laboratory | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Cytology description | Positive stains | Negative stains | Flow cytometry description | Electron microscopy description | Electron microscopy images | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1 | Board review style question #2 | Board review style answer #2Cite this page: Owczarczyk AB, Smith L. CHL lymphocyte depleted. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/lymphomanonBlymphocytedepleted.html. Accessed April 19th, 2024.
Definition / general
- Subtype of classic Hodgkin lymphoma (CHL) with numerous Reed-Sternberg cells and scant nonneoplastic background lymphocytes
Essential features
- B cell derived lymphoma with a predominance of malignant Reed-Sternberg cells and depleted inflammatory background
- Rarest of the CHL subtypes, more commonly seen in developing nations
- Associated with HIV infection
- Often EBER positive (in situ hybridization for noncoding RNAs; 50 - 72% of cases)
- References: J Clin Oncol 2011;29:3914, Virchows Arch 2008;453:611, Cancer Epidemiol Biomarkers Prev 2014;23:274, Leuk Lymphoma 2009;50:937, Pathol Res Pract 2013;209:201
Terminology
- Hodgkin lymphoma disease, lymphocyte depletion, NOS
- Classic Hodgkin lymphoma, lymphocyte depletion, NOS
- Hodgkin lymphoma, lymphocyte depletion, diffuse fibrosis
- Hodgkin lymphoma, lymphocyte depletion, reticular
ICD coding
Epidemiology
- Rarest of the CHL subtypes, < 2% of CHL
- More common in developing nations
- Often HIV associated
- Median age 30 - 40 years; male predominance
- References: J Clin Oncol 2011;29:3914, Virchows Arch 2008;453:611, Cancer Epidemiol Biomarkers Prev 2014;23:274
Sites
- Predilection for subdiaphragmatic region (retroperitoneal lymph nodes, abdominal organs) and bone marrow
- Peripheral lymphadenopathy possible
- References: J Clin Oncol 2011;29:3914, Virchows Arch 2008;453:611
Pathophysiology
Etiology
Clinical features
- Often presents with B symptoms (fevers, drenching night sweats, unexplained weight loss) and advanced stage (III - IV) compared with other CHL subtypes (Pathol Res Pract 2013;209:201)
- More aggressive (e.g., higher International Prognostic Score) than other CHL subtypes, including in HIV+ patients (Am J Clin Pathol 2004;121:727, J Clin Oncol 2011;29:3914)
- May be part of a continuum with mixed cellularity subtype (Clin Lymphoma Myeloma 2009;9:206, Cancer J 2009;15:129)
Diagnosis
- Excisional tissue biopsy or resection
- Fine needle aspiration or core biopsy may be difficult to distinguish between CHL subtypes given the significance of tissue architecture and background inflammatory infiltrate for diagnosis
Laboratory
- Nonspecific
- High serum soluble IL2 receptor levels (Pathol Res Pract 2013;209:201)
Radiology description
- Subdiaphragmatic, retroperitoneal lymphadenopathy
- PET CT often shows concurrent bone marrow involvement
- References: J Clin Oncol 2011;29:3914, Virchows Arch 2008;453:611
Radiology images
Images hosted on other servers:

Mesenteric and retroperitoneal lymphadenopathy
Prognostic factors
- Unfavorable prognostic factors (J Clin Oncol 2011;29:3914):
- Advanced disease stage
- Advanced age
- Presence of B symptoms
- ≥ 3 lymph node areas involved
- Large mediastinal mass
- High ESR (erythrocyte sedimentation rate)
- HIV positive
Case reports
- 47 year old man with large periumbilical, mesenteric mass (Int J Gen Med 2019;12:405)
- 60 year old woman with new onset splenomegaly (J Clin Pathol 2015;68:947)
- 76 and 92 year old women with primary extranodal lymphocyte depleted CHL (J Clin Exp Hematop 2021;61:173)
- 88 year old woman with epidural spinal cord compression (BMC Neurol 2012;12:64)
Treatment
- Standard therapy: ABVD (doxorubicin, bleomycin, vinblastine, dacarbazine) with or without localized radiotherapy (J Clin Oncol 2005;23:4574)
- Patients who undergo more intensive chemotherapy tend to do better (J Clin Oncol 2011;29:3914)
Microscopic (histologic) description
- Predominance of Reed-Sternberg cells and scarce background lymphocytes
- Reed-Sternberg cells have multilobated nuclei with prominent eosinophilic inclusion-like nucleoli
- May have coagulative necrosis or sinusoidal invasion
- 2 patterns:
- Diffuse fibrosis:
- Prominent fibroblastic proliferation (nonbirefringent fibrillary stroma) without well formed fibrous bands
- Numerous histiocytes
- Scattered Reed-Sternberg cells
- Scant lymphocytes
- Lack of plasma cells or eosinophils
- Reticular:
- Rich in Reed-Sternberg cells (often sheets) with anaplastic, pleomorphic or sarcomatous features
- Scant background small lymphocytes
- Capsular and perinodal infiltration is common
- Diffuse fibrosis:
- References: Leuk Lymphoma 2009;50:937, Pathol Res Pract 2013;209:201
Microscopic (histologic) images
AFIP images
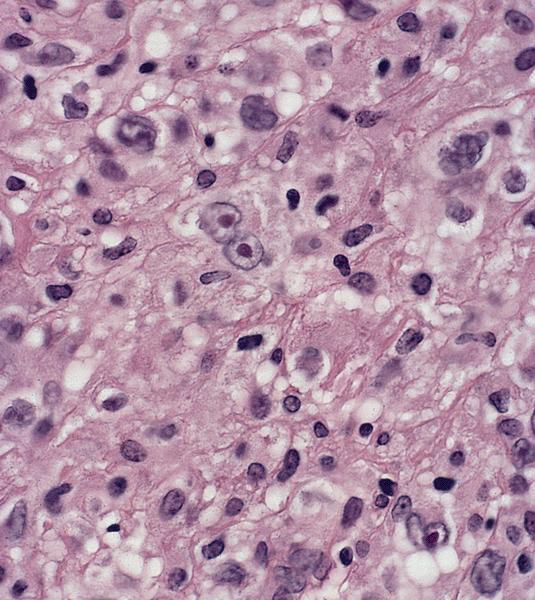
Diffuse fibrosis
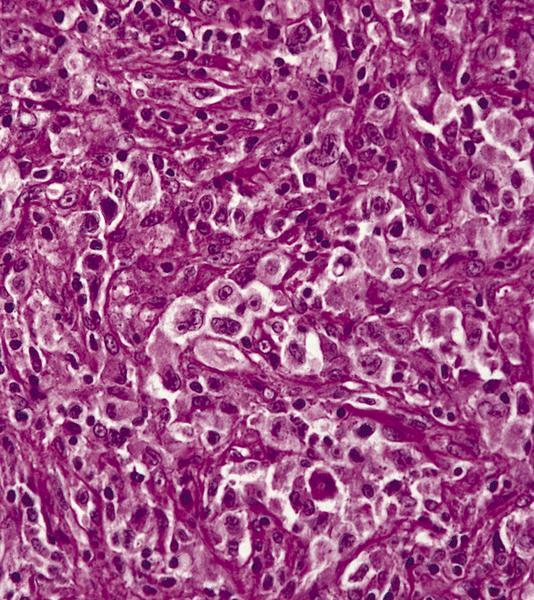
Numerous Hodgkin cells
Cytology description
- Predominantly large, atypical cells with irregular / convoluted nuclear contour, binucleation / multinucleation and frequent mitotic figures
- Rare small lymphocytes
Positive stains
- Reed-Sternberg cells:
- References: Leuk Lymphoma 2009;50:937, Pathol Res Pract 2013;209:201
Negative stains
- Reed-Sternberg cells:
- References: Leuk Lymphoma 2009;50:937, Pathol Res Pract 2013;209:201
Flow cytometry description
- Usually noncontributory as large Hodgkin and Reed-Sternberg cells are delicate and frequently destroyed during flow cytometric processing
Electron microscopy description
Electron microscopy images
Molecular / cytogenetics description
- High rate of IGH gene rearrangements, likely related to the high density of Reed-Sternberg cells relative to nonneoplastic lymphoid cells in the specimen (Leuk Lymphoma 2009;50:937)
Sample pathology report
- Retroperitoneal lymph node, excisional biopsy:
- Classic Hodgkin lymphoma, lymphocyte depleted type (see comment)
- Comment: H&E sections show an effaced lymph node by sheets of large, bizarre cells with irregular, multilobated nuclei, vesicular chromatin, prominent nucleoli and abundant cytoplasm. Rare background small lymphocytes are noted.
- Immunohistochemical stains show that the atypical cells are positive for CD30, CD15 (subset), PAX5 (weak) and EBER (in situ hybridization for EBV encoded RNA). The atypical cells are negative for CD20, CD45, OCT2, BOB1 and ALK1. CD3 highlights rare small T cells.
- Concurrent flow cytometric analysis was negative for monoclonal B cells or aberrant T cells.
Differential diagnosis
- Anaplastic large cell lymphoma (ALCL):
- CHL, nodular sclerosis type:
- Well defined sclerotic, collagenous bands with scattered atypical Reed-Sternberg cells
- Diffuse large B cell lymphoma, NOS:
- No Reed-Sternberg cells
- Usually negative for CD15
- EBV+ diffuse large B cell lymphoma:
Additional references
- Mod Pathol 2003;16:1141 (B cell marker expression), Oncologist 2009;14:739, Hematology Am Soc Hematol Educ Program 2006;2006:266
Board review style question #1
A middle aged HIV+ man presents with abdominal pain and a large retroperitoneal mass is detected on imaging. Core biopsy was performed, showing sheets of bizarre, atypical cells with large nucleoli and frequent binucleation. Scattered background small lymphocytes are present. The atypical cells are positive for CD30, EBER and PAX5 (weak) but negative for CD20. Molecular studies demonstrate immunoglobulin gene rearrangement. What is the most likely diagnosis?
- Anaplastic large cell lymphoma
- Classic Hodgkin lymphoma, lymphocyte depleted
- Classic Hodgkin lymphoma, lymphocyte rich
- Diffuse large B cell lymphoma, NOS
- EBV positive diffuse large cell lymphoma
Board review style answer #1
Board review style question #2
A 35 year old man has extensive subdiaphragmatic lymphadenopathy. Core biopsy of one of the lymph nodes shows an effaced architecture with diffuse, disordered fibrosis and abundant histocytes. Scattered large, binucleated, CD30 positive and EBER positive atypical cells are noted. Plasma cells, eosinophils and small lymphocytes are essentially absent. Which of the following is true about this disease entity?
- Atypical cells are strongly positive for PU.1, BOB1, CD79a and CD20
- Best detected by flow cytometry
- More common in developed nations
- Most likely occurs in female patients
- Often associated with HIV infection
Board review style answer #2
