
Mandible & maxilla
Benign odontogenic tumors
Adenoid ameloblastoma
Editorial Board Member: Ruta Gupta, M.D.
Deputy Editor-in-Chief: Kelly Magliocca, D.D.S., M.P.H.


Last author update: 1 February 2024
Last staff update: 26 March 2024
Copyright: 2021-2024, PathologyOutlines.com, Inc.
PubMed Search: Adenoid ameloblastoma
Table of Contents
Definition / general | Essential features | Terminology | ICD coding | Epidemiology | Sites | Etiology | Clinical features | Diagnosis | Radiology description | Radiology images | Prognostic factors | Case reports | Treatment | Microscopic (histologic) description | Microscopic (histologic) images | Positive stains | Negative stains | Molecular / cytogenetics description | Sample pathology report | Differential diagnosis | Additional references | Board review style question #1 | Board review style answer #1Cite this page: Goldfaden JS, Bilodeau EA. Adenoid ameloblastoma. PathologyOutlines.com website. https://www.pathologyoutlines.com/topic/mandiblemaxillaadenoidameloblastoma.html. Accessed April 25th, 2024.
Definition / general
- Benign, rare tumor of odontogenic origin
- Cuboidal to columnar ameloblastic epithelium that forms duct-like structures, epithelial whorls and cribriform architecture; dentinoid deposits, clusters of clear cells and ghost cell keratinization may also be present (J Oral Maxillofac Pathol 2012;16:272)
Essential features
- Adenoid ameloblastomas have a predilection for the posterior mandible (Head Neck Pathol 2022;16:344)
- Microscopically, adenoid ameloblastomas consist of epithelium resembling conventional ameloblastoma in addition to duct-like structures, epithelial whorls and cribriform architecture
- Dentinoid deposits, clusters of clear cells and ghost cell keratinization may also be observed (J Oral Maxillofac Pathol 2012;16:272)
- Adenoid ameloblastoma can be a challenging and controversial diagnosis as this tumor has features seen in numerous odontogenic tumors (i.e., ameloblastoma, adenomatoid odontogenic tumor, calcifying odontogenic cyst / dentinogenic ghost cell tumor and odontogenic carcinoma with dentinoid)
Terminology
- Adenoid ameloblastoma with dentinoid was proposed by Brannon of the Armed Forces Institute of Pathology in 1994; this terminology has been deemed acceptable by the World Health Organization (WHO) (Brannon: Adenoid Ameloblastoma With Dentinoid, 1994)
- Described as dentinoameloblastoma by Slabbert et al. in 1992 (J Oral Pathol Med 1992;21:46)
ICD coding
- ICD-O: 9300/0 - adenoid ameloblastoma
- ICD-10
- ICD-11
- 2E83.0 & XH1SV4 - benign osteogenic tumors of bone or articular cartilage of skull or face & ameloblastoma, NOS
- 2E83.1 & XH1SV4 - benign osteogenic tumors of bone or articular cartilage of lower jaw & ameloblastoma, NOS
Epidemiology
- Occurrence peaks in the fourth decade, with a slight male predilection (M:F = 1.3:1) and a wide age range of 15 - 82 years (Head Neck Pathol 2022;16:344)
Sites
- ~64.7% of adenoid ameloblastomas occur in the mandible (Head Neck Pathol 2022;16:344)
- Posterior gnathic bones are most commonly affected (Head Neck Pathol 2023;17:688)
Etiology
- Unknown
Clinical features
- Usually an asymptomatic swelling (unless secondarily infected)
- Tooth displacement may be present
Diagnosis
- Adenoid ameloblastoma may be detected radiographically as an incidental finding or present as a clinical swelling
Radiology description
- 82.4% of adenoid ameloblastomas present exclusively as radiolucent lesions and may be ill defined (Head Neck Pathol 2022;16:344)
- May also appear as mixed density due to the presence of dentinoid
- May be unilocular or multilocular
Radiology images
Images hosted on other servers:

Diffuse periapical radiolucency
Prognostic factors
- 45.4% of adenoid ameloblastomas developed at least 1 recurrence following surgical excision (Head Neck Pathol 2022;16:344)
Case reports
- 39 year old man with a chief concern of painful, mobile teeth in the right posterior maxilla (Oral Surg Oral Med Oral Pathol Oral Radiol 2019;128:E53)
- 54 year old woman with asymptomatic radiolucency of the left posterior maxilla (Oral Maxillofac Surg 2020;24:243)
- 57 year old woman with a well defined, unilocular radiolucency between the roots of the right mandibular premolars without intraoral changes (Oral Surg Oral Med Oral Pathol Oral Radiol 2022;134:E162)
Treatment
- Conventional treatment consists of surgical resection as primary therapy (Oral Surg Oral Med Oral Pathol Oral Radiol 2015;120:368)
- Patients may also receive radiotherapy as adjuvant to prevent recurrence (Oral Surg Oral Med Oral Pathol Oral Radiol 2015;120:368)
Microscopic (histologic) description
- Epithelium resembling conventional ameloblastoma, particularly palisading of cells at peripheries of the tumor nests, with additional duct-like structures and cribriform architecture
- Basophilic areas of cellular condensation or morules may be present
- Dentinoid deposits, clusters of clear cells and ghost cell keratinization may also be observed (J Oral Maxillofac Pathol 2012;16:272)
- Mitotic activity may be increased (Oral Surg Oral Med Oral Pathol Oral Radiol 2019;128:e78, Oral Surg Oral Med Oral Pathol Oral Radiol 2015;120:368)
Microscopic (histologic) images
Contributed by Elizabeth Ann Bilodeau, D.M.D., M.D., M.S.Ed.

Epithelial whorls

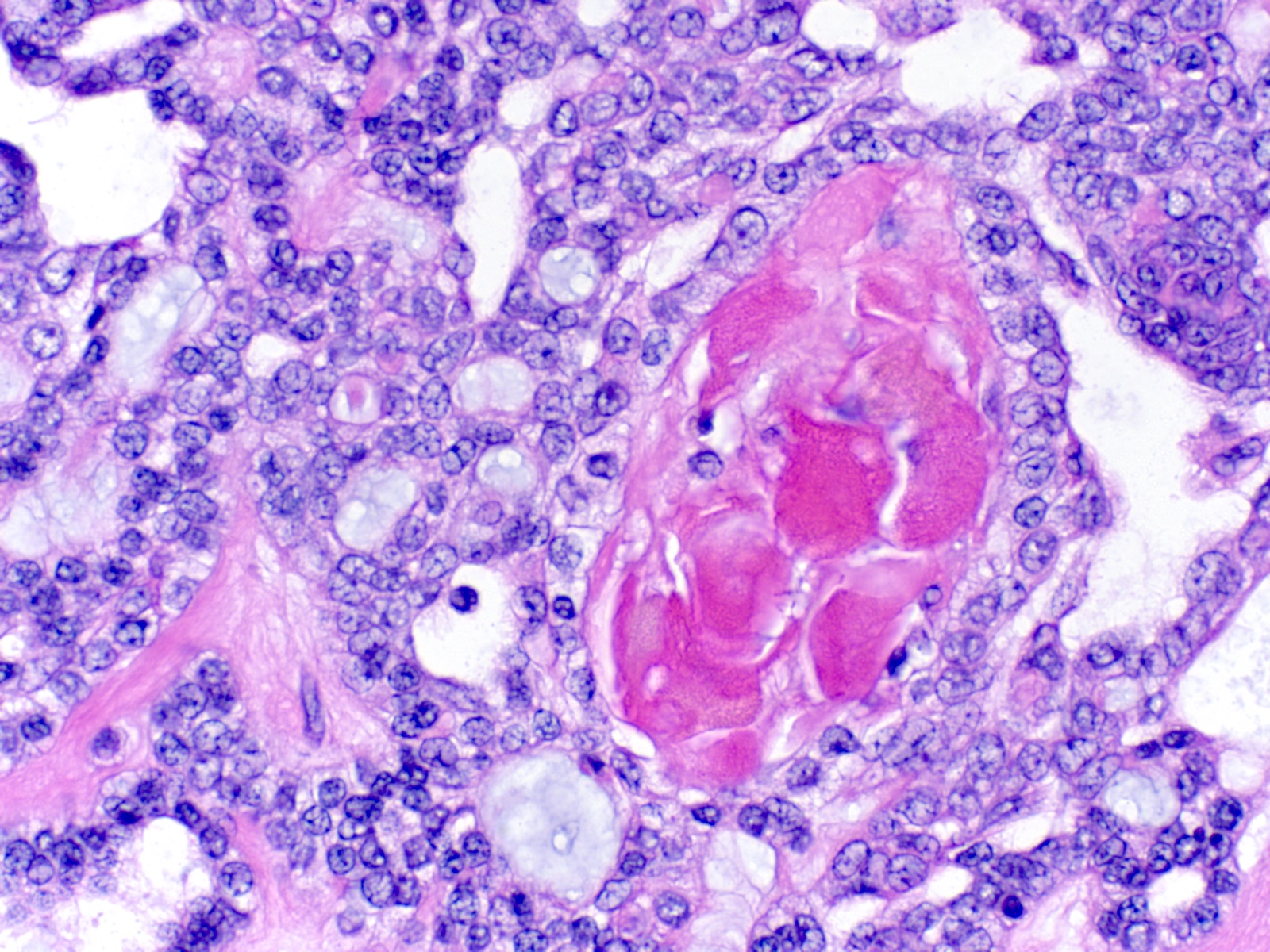
Cribriform architecture and eosinophilic matrix
Focal ghost cell keratinization
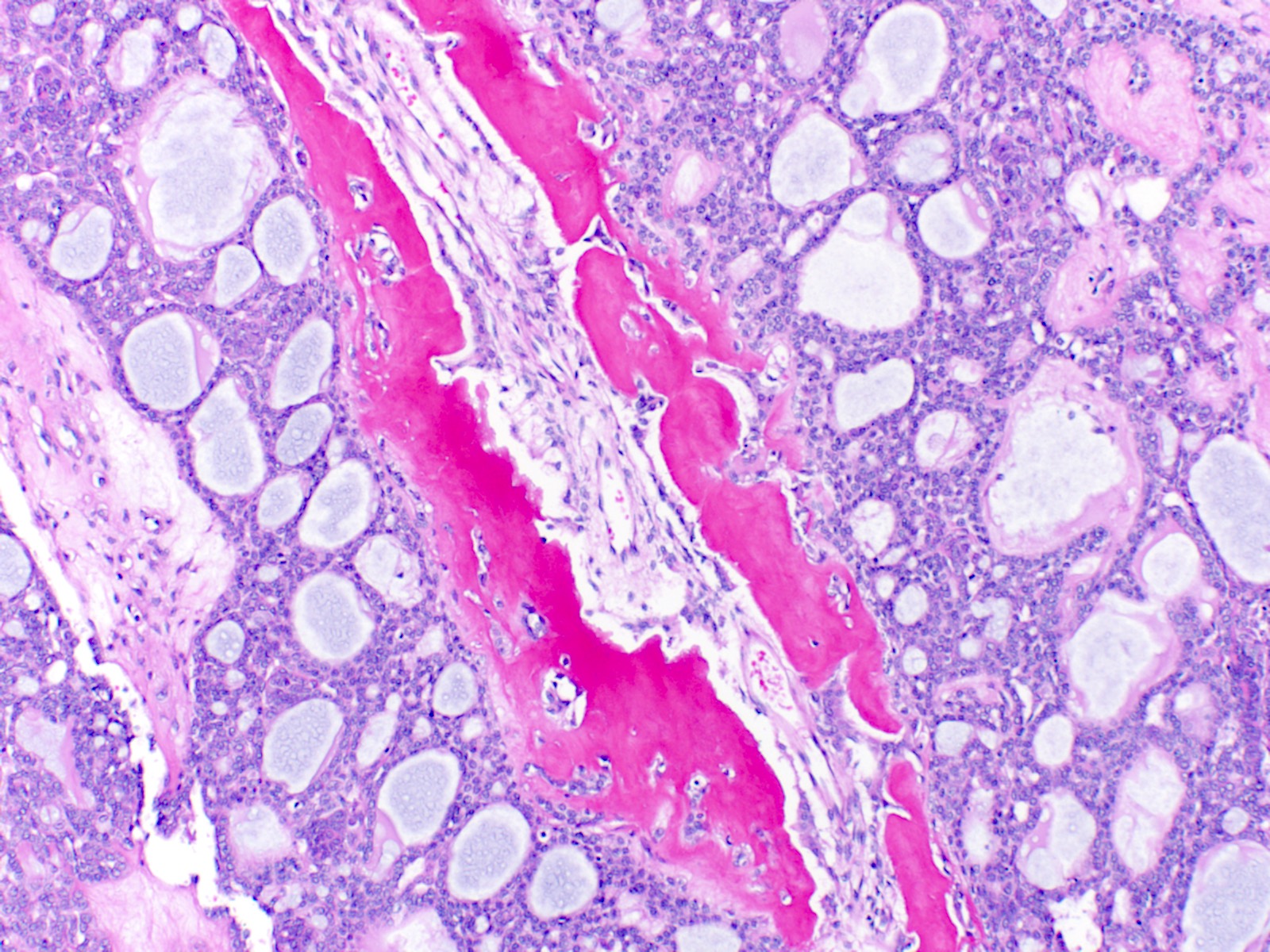
Dentinoid deposits

Increased mitotic activity

Duct-like structures and ghost cell keratinization
Positive stains
- AE1 / AE3 (Oral Surg Oral Med Oral Pathol Oral Radiol 2019;128:e78)
- Beta catenin within morules (Oral Surg Oral Med Oral Pathol Oral Radiol 2019;128:e78)
- CK5/6 (Oral Surg Oral Med Oral Pathol Oral Radiol 2019;128:e78)
- Ki67 may have variable expression, with the upper limit being 72.4 plus or minus 24.9 positive cells per high power field (Oral Surg Oral Med Oral Pathol Oral Radiol 2015;120:368)
- p63 and p40 are positive (Oral Surg Oral Med Oral Pathol Oral Radiol 2019;128:e78)
- p16 is variable (Oral Surg Oral Med Oral Pathol Oral Radiol 2015;120:368, Oral Surg Oral Med Oral Pathol Oral Radiol 2019;128:e78)
Negative stains
Molecular / cytogenetics description
- BRAF p.V600E mutation (which is observed in other ameloblastomas) in addition to KRAS p.G12V and KRAS p.G12R mutations (both of which are typical of adenomatoid odontogenic tumors) are absent in adenoid ameloblastomas (J Oral Pathol Med 2021;50:1067)
- Based on limited data, beta catenin mutations, particularly p.Ser33Cys, p.Gly34Arg and p.Ser37Phe, were observed in 4 of 9 patients (Mod Pathol 2022;35:1562)
Sample pathology report
- Posterior mandible, right, incisional biopsy:
- Adenoid ameloblastoma, 1.5 cm
Differential diagnosis
- Ameloblastoma:
- Columnar cells with palisading, hyperchromatic nuclei of basal cells
- No hard tissue formation is present
- Adenomatoid odontogenic tumor:
- Epithelium may appear nodular, trabecular or cribriform with duct-like structures
- Amyloid deposits may be present
- Enclosed in thick capsule; radiographically often well defined and associated with impacted maxillary canines
- Calcifying cystic odontogenic tumor:
- Ameloblastic epithelium and ghost cells
- Lacks whorls, duct-like structures and cribriform architecture
- Dentinogenic ghost cell tumor:
- Ameloblastic-like areas with palisading of basaloid cells
- Admixed ghost cells: anucleate epithelial cells with pale, cleared cytoplasm
- Lacks whorls, duct-like structures and cribriform architecture
Additional references
Board review style question #1
A 40 year old man presents with a radiolucent lesion of the posterior mandible. Based on the photomicrograph above, what is the lesion?
- Adenoid ameloblastoma
- Adenomatoid odontogenic tumor
- Ameloblastoma
- Calcifying cystic odontogenic tumor
Board review style answer #1
A. Adenoid ameloblastoma. The photomicrograph depicts cribriform areas with duct-like structures and interspersed dentinoid deposits that are associated with clear cells. Answer D is incorrect because calcifying cystic odontogenic tumors lack duct-like structures and cribriform architecture. Answer B is incorrect because adenomatoid odontogenic tumors are well encapsulated and lack mature dentinoid. Answer C is incorrect because conventional solid / multicystic ameloblastomas lack hard tissue formation.
Comment Here
Reference: Adenoid ameloblastoma
Comment Here
Reference: Adenoid ameloblastoma
Back to top
